
Abstract
Recognizing that spiritual needs often emerge in health care settings, the Joint Commission requires spiritual assessments in numerous organizations frequented by older adults. Given that many gerontological practitioners have received little training in identifying spiritual needs, a qualitative meta-synthesis (N = 9 studies) was conducted to identify and describe older adults’ perceptions of their spiritual needs in health care settings. Five interrelated categories emerged: (a) spiritual practices; (b) relationship with God; (c) hope, meaning, and purpose; (d) interpersonal connection; and (e) professional staff interactions. The implications of the findings are discussed as they inform the spiritual assessment process.
The Joint Commission requires spiritual assessments in hospitals as well as many other health care organizations providing services to older adults, including nursing homes, home care organizations, and agencies providing addiction services (Hodge, 2006; Koenig, 2007). Formerly known as the Joint Commission on Accreditation of Healthcare Organizations, or JCAHO, the Joint Commission is the largest and most influential health care accrediting body in the United States (JCAHO, 2004). The Joint Commission accredits most of the nation’s hospitals, as well as thousands of other health care providers (Hodge, 2006).
Older adults are among the populations most likely to benefit from the Joint Commission’s assessment requirements—a fact implicitly recognized by the Joint Commission’s stipulation of an assessment in settings frequented by individuals in later life. Spirituality and religion (the vehicle through which spirituality is commonly expressed) tend to play more pronounced roles in the lives of adults over 65, relative to the general population (Musick, Traphagan, Koenig, & Larson, 2000; Newport, 2006; Taylor, Chatters, & Jackson, 2007). Similarly, spirituality holds greater importance to women and many racial minorities (Pargament, 1997). For instance, older African Americans and Caribbean Blacks display higher levels of spirituality, religious participation, and religious coping relative to older Whites (Taylor et al., 2007). Thus, while all adults should receive a spiritual assessment as a routine component of care (Koenig, 2007), it may play an even more important role in service provision for older women and people of color (Pargament, 1997; Taylor et al., 2007).
Scholars define spirituality in diverse ways (Clarke, 2009; Ellis & Narayanasamy, 2009; Paley, 2008; Pesut, 2008). Spirituality is a highly contested concept, and a wide variety of definitions appear in the academic literature (Swinton & Pattison, 2010). One prominent conceptualization is offered by Pargament (2007), who defines spirituality as the search for the sacred. The sacred refers to God and other manifestations of the transcendent, but it also encompasses other entities that are perceived to be sacred. Essentially, any entity can be considered sacred by virtue of being embedded in a transcendent narrative (Crisp, 2010). The concept “search” connotes the active, dynamic nature of human interaction with the sacred (Pargament, 2007). Individuals often search for transcendent meaning during times of stress, which are often precipitated by events surrounding the receipt of health care services (Pargament, 1997).
The Joint Commission’s standards reflect an emerging consensus regarding the role that spiritual assessment plays in holistic service provision (Nelson-Becker, Nakashima, & Canda, 2007). Studies have repeatedly found that many practitioners affirm the importance of spiritual assessment (Sheridan, 2009). For example, a national study of gerontological social workers (N = 299) found that 94% thought it was appropriate to gather spiritual information in assessment and had personally conducted such assessments (Murdock, 2005).
The purpose of administering a spiritual assessment is to identify clients’ or patients’ spiritual needs and determine the appropriate steps necessary to address the issues that emerge (JCAHO, 2005). While not every older adult has spiritual needs, many do. These needs are often directly related to service provision, hence the importance of ensuring that they are addressed appropriately (Barusch, 1999; Hodge, 2005a; Nelson-Becker, 2005).
A significant body of quantitative work has documented clients’ existential spiritual needs in health care settings (Jang et al., 2004; Moadel et al., 1999; Okon, 2005; Reed, 1991). More specifically, perceptions of spiritual needs have been examined among individuals receiving services in rehabilitation hospitals (Anderson, Anderson, & Felsenthal, 1993), pediatric units (Feudtner, Haney, & Dimmers, 2003), substance abuse treatment programs (Carroll, McGinley, & Mack, 2000), hospices (Hermann, 2001), and mental health care (Koslander & Arvidsson, 2007). In addition, perceptions have been examined among people dealing with cancer (Astrow, Wexler, Texeira, He, & Sulmasy, 2007), advanced cancer (Balboni et al., 2007; Hampton, Hollis, Lloyd, Taylor, & McMillan, 2007), psychiatric disabilities (D’Souza, 2002; Fitchett, Burton, & Sivan, 1997), and HIV/AIDS (Warner-Robbins & Christiana, 1989).
This body of research also suggests that clients’ spiritual needs are often inadequately addressed in health care settings. For example, Balboni and associates (2007) examined the degree to which clients’ spiritual needs were supported among a sample of individuals with advanced cancer (N = 230) receiving treatment at five different facilities in New England (two), New York City (one), and Texas (two). In all, 88% reported that religion was either very important (67%) or somewhat important (20%). Among these individuals, 72% reported that their spiritual needs were minimally or not at all met by the medical system.
These relatively high levels of unmet needs may be related to practitioner unfamiliarity with common spiritual concerns (Anderson et al., 1993; Cavendish et al., 2006; Davidson, Boyer, Casey, Matzel, & Walden, 2008). Without an awareness of older adults’ needs, it is easy to overlook their existence, even if one is committed to providing holistic services (Sheridan, 2009). It is often hard to identify information external to the paradigm into which one has been socialized (Kuhn, 1970).
Studies indicate that many practitioners have received little, if any, training on spirituality during their educational careers (Sheridan, 2009). For instance, Murdock’s (2005) national study of gerontological social workers (N = 299) found that 70% reported that preparation in school on spirituality occurred rarely or never. Similarly, content analyses of various academic literatures revealed minimal content on spirituality (Cnaan, Wineburg, & Boddie, 1999; Hodge, Baughman, & Cummings, 2006; Tompkins, Larkin, & Rosen, 2006).
Failure to adequately address spiritual needs can impact a number of health-related outcomes, including clients’ satisfaction with their received care (Astrow et al., 2007; Balboni et al., 2007; Hermann, 2007; Koenig, 2007; Koenig, McCullough, & Larson, 2001). Client satisfaction is particularly significant since this outcome is typically viewed as a proxy for quality of care (Jackson, Chamberlin, & Kroenke, 2001; Press, 2002; Shea et al., 2008). Research has linked client satisfaction with reduced likelihood of professional malpractice suits, greater profitability, increased loyalty toward service providers, greater patient follow-through, and better clinical outcomes (Kaldenberg, 2001; Moscato et al., 2007; Press, 2002). In addition, providing quality services that satisfy clients is widely viewed as an ethical imperative (Astrow et al., 2007).
The purpose of this study is to identify and describe older adults’ perceptions of common spiritual needs that emerge in health care settings. Developing a working knowledge of older adults’ common spiritual needs can help practitioners provide better services by heightening their ability to recognize and address such needs (Cavendish et al., 2006; Davidson et al., 2008; Murray, Kendall, Boyd, Worth, & Benton, 2004). Many gerontological practitioners are interested in learning more about spirituality, perhaps because of sensitivity regarding their lack of knowledge, and the potentially adverse effects upon clients (Murdock, 2005). In response to this expressed interest, this study answers the question: What spiritual needs do older adult clients commonly experience in health care settings?
To answer the research question, a qualitative meta-synthesis was conducted to identify and describe older adults’ perceptions of their spiritual needs in health care settings (Padgett, 2008). Although a relatively recent methodological development, interest in synthesizing qualitative findings across studies appears to be growing (Sim & Madden, 2008). Fields in which meta-syntheses have appeared include: nursing (Meadows-Oliver, 2003), medicine (Sim & Madden, 2008), psychotherapy (Timulak, 2007), psychiatry (Cole & Dendukuri, 2003), education (Kasworm, 1990), health (McCormick, Rodney, & Varcoe, 2003), and substance use (Maher & Hudson, 2007). As discussed in the following, this approach is perhaps ideally suited to answer the present research question.
Method
Qualitative methods of inquiry are widely thought to represent the best approach for exploring phenomena that are intrinsically holistic, idiosyncratic, and contextual (Lincoln & Guba, 2003). Spirituality has been cited as an exemplar of this type of phenomena (Slife, Hope, & Nebeker, 1999; Slife, Wiggins, & Graham, 2005). Thus, while a number of quantitative studies have explored perceptions of spiritual needs using various checklist-type formats, qualitative research may represent the best vehicle to equip practitioners with a transferable understanding of older adults’ spiritual needs (Thorne, Jensen, Kearney, Noblit, & Sandelowski, 2004). Studies that give voice to older adults’ phenomenological reality in health care settings can provide a firsthand understanding of common spiritual needs. Developing an awareness of such understandings may help practitioners identify similar voices in the future.
Relative to the understanding provided by a single qualitative study, a qualitative meta-synthesis provides a “more comprehensive representation of investigated phenomena” (Timulak, 2007, p. 305). This general approach of aggregating qualitative findings across studies has been referred to as a qualitative meta-analysis, meta-ethnography, meta-study, meta-summary, and perhaps most commonly as a meta-synthesis (Finlayson & Dixon, 2008). Although variation within this larger “meta-family” of approaches exists, the guiding principle behind the comparative integration of qualitative research is to provide a more complete understanding of the phenomena of interest (Bondas & Hall, 2007; Maher & Hudson, 2007).
A meta-synthesis is related to, but distinct from, a systematic review. The primary aim of a systematic review is to locate and synthesize research that deals with a particular issue (Littell, Corcoran, & Pillai, 2008). A meta-synthesis shares this goal of cataloguing and combining studies, as signified by the term synthesis (Bondas & Hall, 2007). However, as connoted by the term meta, a meta-synthesis moves beyond a synthesis to include an interpretive analytical component (Finlayson & Dixon, 2008). Analysis is conducted across studies to identify meaning beyond and behind individual studies—meaning that transcends isolated research projects. The findings from each study are reinterpreted and synthesized in light of the data and findings obtained in other studies (Bondas & Hall, 2007).
The aim of a meta-synthesis is not reductive. For example, the purpose is not to identify and then count commonalities across studies, a process that often excludes data that appear less frequently (McCormick et al., 2003). Rather, the aim is to retain all information in each study while adding an interpretive dimension. Although not generalizible, the marriage of synthesis and interpretive analysis provides a richer, more comprehensive understanding of a given phenomena (Finlayson & Dixon, 2008). A new integrated and more complete interpretation of the findings is produced. Compared to individual studies, the new meta-synthesis may have more clarity, coherence, cogency, credibility, and pragmatic utility (Bondas & Hall, 2007).
Accordingly, this method is perhaps the ideal choice to identify and describe older adults’ perceptions of their spiritual needs in health care settings. Compared to single qualitative study, it provides a fuller, more nuanced understanding of older adults’ common spiritual needs. By exposing practitioners to a more comprehensive picture of older adults’ perceptions, practitioners are better equipped to recognize and address the needs that may exist.
Selection Criteria
To identify studies pertinent to the present meta-synthesis, a number of inclusion and exclusion criteria were specified. To be included in the present analysis, studies had to be: (a) qualitative, (b) explorations of understandings of older adults’ spiritual needs, (c) in health care settings, (d) featuring primarily older adults’ views (i.e., mean sample age > 60 years). Two exceptions were made to this latter criterion in the case of a study of chronically ill patients receiving care on a medical ward (Narayanasamy, 1995) and a study of women with end-stage renal disease in which the mean age was unreported (Tanyi, Recine, Werner, & Sperstad, 2006).
In addition, inclusion was contingent upon publication in a peer-reviewed journal. Some meta-synthesizers have recommended excluding studies based on their methodological tradition or perceived quality (McCormick et al., 2003). Conversely, others have advocated including all relevant research across traditions, including unpublished works obtained from “gray literature” searches. In this study, qualitative research from all methodological traditions was eligible to be selected and quality was considered to be sufficient for inclusion if the study appeared in a refereed journal. These choices represent common practices among meta-synthesizers (Bondas & Hall, 2007).
A number of exclusion criteria were also employed. Specifically, studies were excluded if they discussed spiritual needs using: (a) quantitative instruments that required older adults to fit their experiences into predetermined categories, (b) brief case studies, (c) conceptual or theoretical frameworks, or (d) perspectives from health care professionals or caregivers about older adults’ spiritual needs. Research on spiritual coping was also excluded, as this construct was held to be conceptually distinct from the related construct of spiritual needs.
Similarly, studies were excluded if they explored perceptions of spiritual needs primarily among non–clinical/patient samples. The broad range of challenges (e.g., emotional, physical, financial, and existential) associated with admission into the health care system often engenders spiritual needs (Nelson-Becker et al., 2007; Pargament, 2007). Since perceptions of spiritual needs may differ upon admission to health or behavioral health systems, the search was restricted to older adults who could directly address the issue of spiritual needs from a client/patient perspective (Balboni et al., 2007; Harrington, 2004; Pargament, 1997).
Search for Studies
To obtain studies that met the aforementioned criteria, a computerized literature search was preformed. More specifically, a keyword search of the following databases was conducted: Social Services Abstracts, Medline, PsycINFO, PsycARTICLES, PsycCRITIQUES, Psychology: A SAGE Full-Text Collection, PILOTS, Health Sciences, Sociological Abstracts, and Sociology: A SAGE Full-Text Collection. The keywords included spiritual needs or religious needs or spiritual concerns or religious concerns. Titles and abstracts were read to assess their relevance to the present analysis. In all, 77 potential studies were obtained and manually reviewed to assess their relevance and locate other potentially germane studies. Three reviews of related topics were obtained and searched for relevant studies (Flannelly, Galek, & Handzo, 2005; Okon, 2005; Sinclair, Pereira, & Raffin, 2006).
Data Analysis
No single data-analytic strategy exists for conducting meta-syntheses (Sandelowski, Barrose, & Voils, 2007; Thorne et al., 2004). The procedures used in this study were primarily based on the strategies outlined by Bondas and Hall (2007), Finlayson and Dixon (2008), and McCormick and colleagues (2003), supplemented by other qualitative meta-studies and our own experience as qualitative researchers. Given the relatively recent development of this approach, the specific data-analytic procedures used in this meta-synthesis are delineated in Table 1
Process Utilized to Analyze and Synthesize Qualitative Data
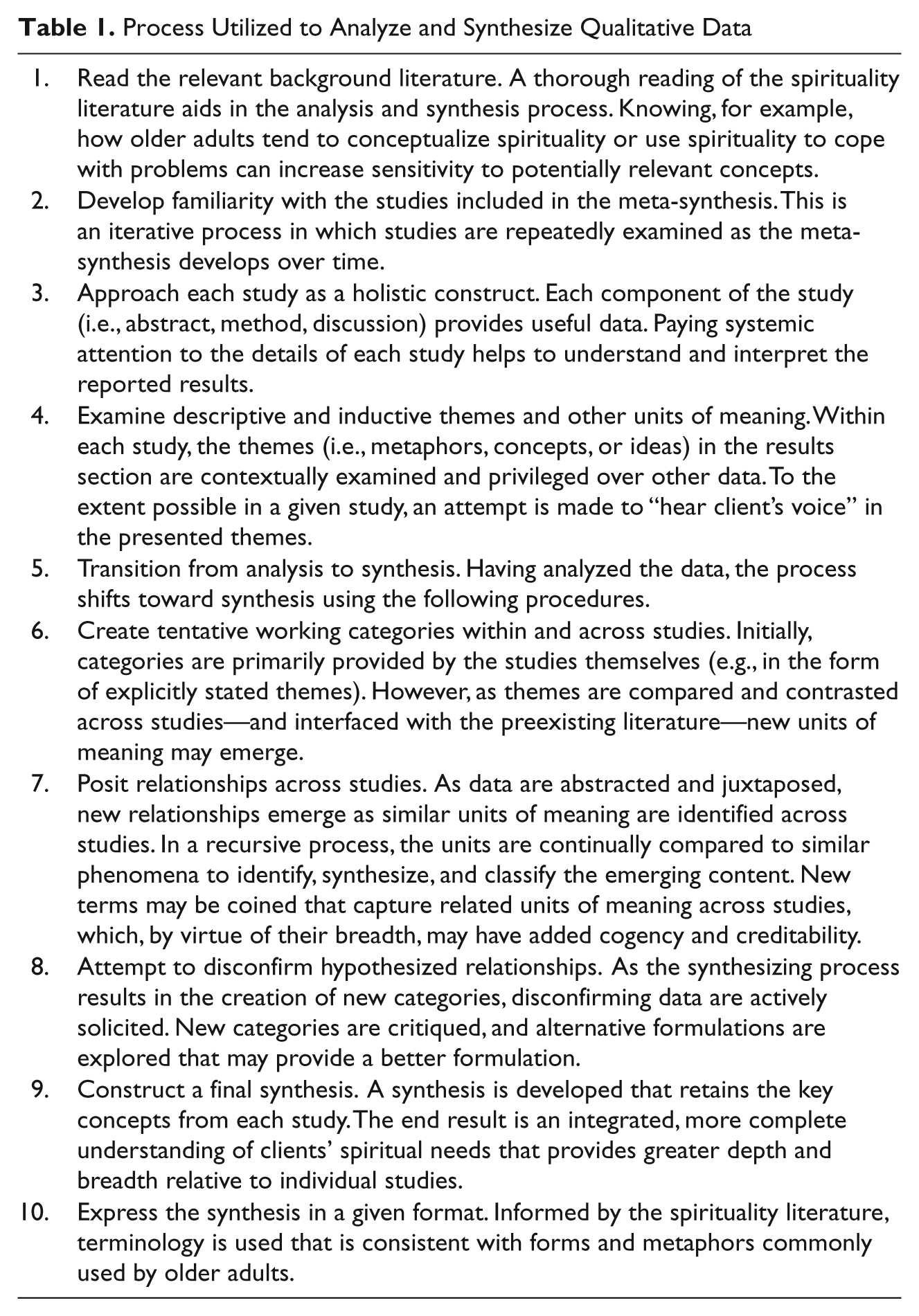
The first author conducted the analysis and synthesis following the 10-step process described in Table 1. Theoretically, the author was guided by what some have called a “weak constructivist” perspective (McCormick et al., 2003). The second author provided peer debriefing (Lietz, Langer, & Furman, 2006). In this capacity, an impartial colleague critically reviewed the implementation of the research methods and provided feedback on the accuracy and completeness of the first author’s implementation of the analytic procedures. This feedback, which helps to minimize the effects of reactivity and bias, enhances the credibility and trustworthiness of the results.
Results
The search produced 9 studies. Some commentators have indicated that approximately 10 to 12 studies represent an ideal number for a meta-synthesis (Bondas & Hall, 2007). Table 2 lists information about each study’s authorship, location, and design. The table also includes a brief description of study participants, including their religious traditions. A relatively wide range of health care settings was represented. Protestant, Catholic, and Jewish affiliations appeared most frequently, which is consistent with the demographics of the United States (Richards & Bergin, 2000).
Older Adults’ Perceptions of their Spiritual Needs in Health Care Settings (N = 9 Studies)

Although the specific questions used to explore clients’ understandings of spirituality and their spiritual needs were not always reported, it appeared that participants used their own definitions of these constructs. For instance, Hermann (2001) reported using semi-structured interviews based on the following questions: “What does the word spiritual mean to you personally?” and “What needs can you identify related to your spirituality as you described it?” (p. 68). Consistent with common practice in qualitative research, none of the studies reported providing participants with a priori definitions of spirituality.
Analysis of the nine studies proceeded in accordance with the procedures described in the previous subsection. The application of the constant comparative approach outlined in Table 1 produced five interrelated categories. These overlapping categories can be summarized as follows: (a) spiritual practices; (b) relationship with God; (c) hope, meaning, and purpose; (d) interpersonal connection; and (e) professional staff interactions.
Spiritual Practices
Spiritual practices emerged as perhaps the most prominent spiritual need. These activities, typically related to the sacred or transcendent, were engaged in on a regular basis. Spiritual practices were perceived to strengthen older adults’ ability to handle the challenges they encountered in the health care system. Spiritual practices listed by older adults as spiritual needs included prayer, reading the Bible or inspirational books on spirituality, meditation, singing worship music, listening to devotional music, receiving the sacraments, listening to sermons, and attending religious services (e.g., church services). Another spiritual practice mentioned involved contemplating the beauty of God’s creation, which included activities such as admiring a sunset, looking out a window, having fresh cut flowers in the room, and being outside in nature.
Older adults reported various structural and physical limitations often hampered their ability to participate in various spiritual practices. For instance, older adults’ ability to pray in hospitals was often hindered by lack of privacy, noisy environments, and disruptive roommates. Similarly, a lack of transportation prohibited attendance at church services. Other respondents reported that reading the Bible was difficult because of vision problems.
Relationship With God
Many older adults indicated that their relationship with God or the transcendent was a central component of their lives. The aforementioned spiritual practices were widely understood to be vehicles for enhancing one’s relationship with God. In other words, spiritual practices addressed the felt need of strengthening one’s existential connection with God.
Cultivating one’s relationship with God was often viewed as a key spiritual need, which helped to handle the stressors associated with receiving treatment or institutionalization. More specifically, admission into the health care system was often perceived as a stressful and isolating event. For many older adults, turning to God was a natural response. Utilizing certain spiritual practices was perceived to nurture a relationship with God. This relationship was an experiential, subjectively felt reality that, when strengthened, enhanced older adults’ ability to deal with the challenges they encountered.
Hope, Meaning, and Purpose
Another family of spiritual needs was related to the concept of hope and meaning. Respondents reported a need to make sense of the situation, to develop a sense of hope, meaning, and purpose in a context often characterized by loss and despair. For example, clients wondered why they were in the health care system, if God had abandoned them, and their place in the afterlife. A number of specific tasks were mentioned that served to address this need. Included among these were asking God and others for forgiveness, engaging in creative activities, caring for or serving others, engaging in rituals, conducting a life review (e.g., looking back over one’s life to see how one’s prayers had been answered), and connecting with significant others.
It is important to emphasize that many older adults expressed feelings of abandonment, isolation, and loneliness in the context of discussing spiritual needs. Uncertainty about the future, guilt about missed opportunities, and despair were also present. Perceptions of one’s self-image were often altered due to disease, ill health, and/or institutionalization. While some older adults derived a sense of meaning, purpose, and hope through their relationship with God, for others, family members and friends helped fill this need.
Interpersonal Connection
Interpersonal interaction with people was also cited as a prominent spiritual need. Older adults often indicated a need to connect with other people as well as a need to process their experiences. This need for interpersonal connection was manifested in a variety of forms. In many cases, clergy played a prominent role in addressing this need. Pastoral visitation was a commonly cited spiritual need. In other cases, respondents indicated a desire to interact with people other than clergy members who, for a variety of reasons, did not always connect appropriately with older adults. For instance, in some situations, older adults perceived clergy as being unwilling to deal frankly with the grim realities clients faced. Consequently, some respondents preferred to discuss their spiritual concerns with others, rather than clergy.
Some older adults cited the importance of regular involvement with others who shared the same belief system, on both collective and individual levels. In addition to attending church services, older adults mentioned Bible studies as an example of forums that addressed this need. Others mentioned the significance of family members and children and noted the importance of regular communication about everyday issues (e.g., the weather, nature, etc.).
Professional Staff Interactions
A final set of spiritual needs related to interactions with the professional staff serving in health care settings. There were expressed needs for increased attention by professional staff to spiritual matters. Specifically, respondents were concerned that professional and nonprofessional staff lacked empathy for, or awareness of, the importance of spiritual needs among older adults. Some respondents—apparently familiar with psychology’s historic antipathy toward religion as represented by Freud (1927/1964) and Ellis (1980)—expressed concern that the helping professions intrinsically demean religious beliefs. Thus, increased staff empathy and knowledge of spiritual and religious matters was reported as a spiritual need.
Some older adults described a felt spiritual need for staff to discuss spiritual issues in a client-centered manner. Toward this end, various respondents suggested the following actions as mechanisms to address clients’ spiritual needs: directly asking clients about their spirituality, talking about God or the sacred, listening to clients’ spiritual issues, and praying with clients. In some cases, older adults had no one with whom to share their spiritual concerns, and staff were perceived to play a key role in meeting clients’ spiritual needs through such mechanisms.
Other respondents felt that professional staff were not best suited to address spiritual needs. While empathy and awareness of clients’ spiritual needs was appreciated, this group of respondents felt that clergy, church members, family, and other individuals were better equipped to address their spiritual concerns. In such cases, staff were often perceived to play an important role in linking clients with the resources older adults needed to ensure that their spiritual needs were appropriately addressed.
Another spiritual need respondents listed was the importance of interacting with older adults in a manner that communicates dignity and respect. For example, interactions characterized by warmth, patience, and kindness can help address spiritual needs. Smiles, friendly facial expressions, and positive interactions with professional staff were cited as helpful.
Similarly, engaging older adults in the decision-making process also meets felt spiritual needs. Practical steps listed in this area included: providing clients with information about treatment decisions, enhancing their control over possible courses of action, and providing information about legal and family matters. Likewise, facilitating older adults’ continuing, active involvement in family matters was also perceived to be a spiritual need.
Discussion
In recognition of the important role spiritual needs often play in service provision, the Joint Commission requires a spiritual assessment in nursing homes, home care settings, hospitals, and other organizations frequented by older adults (Hodge, 2006; Koenig, 2007). Many gerontological practitioners appear to be interested in identifying and addressing their clients’ spiritual needs but have received little training in this area (Murdock, 2005; Sheridan, 2009). The paucity of training is problematic—an inadequate understanding of older adults’ spiritual needs complicates the process of identifying and addressing spiritual needs in busy health care settings (Cavendish et al., 2006; Davidson et al., 2008; Murray et al., 2004).
To address this knowledge gap, a meta-synthesis was conducted to identify and describe older adults’ perceptions of their spiritual needs in health care settings. To the best of the authors’ knowledge, this is the first meta-synthesis on this topic to appear in the academic literature. Analysis revealed that older adults’ spiritual needs fell into five interrelated categories: (a) spiritual practices; (b) relationship with God; (c) hope, meaning, and purpose; (d) interpersonal connection; and (e) professional staff interactions.
The array of needs articulated across these five categories illustrates the diverse manner in which spiritual needs are manifested in the lives of older adults. As implied in the introduction, essentially any entity can be considered spiritual when it is imbued with sacred meaning (Crisp, 2010; Pargament, 2007). Thus, while the spiritual needs that emerged in this study cannot be considered representative, they do help illustrate the diversity of needs older adults experience in health care settings.
Understanding such needs can help practitioners provide better services to older adults. Familiarity with these five larger categories—and common manifestations of specific needs within each category—can help practitioners identify spiritual needs by sensitizing them to their possible presence (Cavendish et al., 2006; Davidson et al., 2008). Developing a working template of common needs better positions practitioners to identify them in practice settings, particularly when conducting a spiritual assessment.
A spiritual assessment can be conceptualized as a two-stage process: a brief preliminary assessment followed, if warranted, by an extensive comprehensive assessment (Pargament & Krumrei, 2009). The purpose of the preliminary assessment is twofold: (a) to determine the relevance of spirituality to service provision and (b) to ascertain whether a comprehensive assessment is needed (Hodge, 2006). In many cases, spirituality plays a limited role in older adults’ lives or is peripheral to service provision. In such instances, a brief assessment may be all that is required (Koenig, 2007; Pargament, 2007).
In other cases, a more comprehensive assessment is warranted (Pargament, 2007). A number of comprehensive assessment tools have been developed to help practitioners identify clients’ spiritual needs, including spiritual histories (Hodge, 2001a), spiritual life maps (Hodge, 2005c), spiritual genograms (Hodge, 2001b), spiritual ecomaps (Hodge, 2000), and spiritual ecograms (Hodge, 2005b). An implicit assessment tool has also been developed for use with clients for whom more traditional spiritual language does not resonate (Pargament, 2007).
Once spiritual needs are identified, gerontological practitioners can take various steps to address these needs. In some cases, practitioners might become personally engaged in directly addressing older adults’ explicit spiritual needs. Some clients may want practitioners to talk with them about God, listen to their spiritual concerns, or pray or meditate with them. Addressing such needs can, from a client’s perspective, play an important role in coping and recovery (Conco, 1995). Furthermore, in some settings, practitioners may be the only helping professionals whom older clients can trust to meet these existentially felt needs (Anderson et al., 1993).
Nevertheless, personally addressing explicit spiritual needs should be carefully considered. A number of professional guidelines have been developed to minimize the risks to clients associated with addressing such a personal topic and should be followed to ensure ethical practice (Hodge, 2006; Koenig, 2007). For example, steps can be taken to ensure that older adults’ spiritual self-determination is respected. Similarly, an adequate level of cultural competence with clients’ spiritual cultures is important. It is also crucial to remain within the parameters of one’s area of professional competence. If these guidelines cannot be satisfied, then alternative strategies should be implemented to ensure older adults’ spiritual needs are appropriately handled.
In many cases, practitioners can meet clients’ needs by linking them to resources (Hermann, 2001). Rather than personally addressing explicit spiritual needs, practitioners may play a more secondary role as facilitators, working with older adults to put in place the necessary resources and assets to ensure their needs are adequately addressed. In this capacity, practitioners might network with an array of clergy members (Ross, 1997). Visits might be arranged with those who share older adults’ spiritual value systems when clients desire such visits. Likewise, practitioners might arrange transportation to religious services or arrange for volunteers to read scripture to older adults who suffer vision impairment (Hermann, 2001).
In addition to linking clients with resources as needs arise on a case-by-case basis, practitioners might proactively implement structural changes to help meet common spiritual needs. For instance, if privacy and noisy environments repeatedly emerge as problems, the possibility of a quiet, dedicated prayer and meditation room might be explored. Practitioners might arrange focus groups to identify ways in which practices might be modified or adapted to better meet common spiritual needs (Davidson et al., 2008).
Similarly, to proactively cultivate empathy and understanding, practitioners might familiarize themselves with commonly encountered spiritual value systems (Anderson et al., 1993). This may be particularly important in light of the lack of training on spirituality many gerontological practitioners appear to have received during their graduate education (Murdock, 2005; Sheridan, 2009). It is not necessary for practitioners to personally agree with older adults’ spiritual values. Rather, the issue is to develop familiarity with, and appreciation for, the underlying value system that provides the context for older adults’ spiritual needs (Hodge, 2006; Koenig, 2007).
Relationships are the milieu in which spiritual needs are addressed (Hermann, 2001; Meert, Thurston, & Briller, 2005). Regardless of whether practitioners personally address spiritual needs or link older adults with the resources to meet their needs, developing traits such as empathy for clients’ spiritual value systems helps lay the foundation for positive helping interactions. Spiritual needs can be very private, personal, and sensitive (Lewis, 2001; Nelson-Becker, 2005). Some older adults may be hesitant to share their spiritual needs due to fear of being ridiculed or otherwise disparaged (Narayanasamy, 1995). Empathy and appreciation for clients’ spiritual value systems helps practitioners transmit the correct verbal and nonverbal cues. Such cues help reassure older adults that practitioners will be receptive to their concerns.
Likewise, it is important to emphasize that basic caring skills—conveying warmth, kindness, patience, and so on—also meet client needs. In one sense, these skills embody basic, professional values. However, when expressed in the context of discussing spirituality, they implicitly transmit important cues and explicitly address clients’ spiritual needs (Hermann, 2001; Meert et al., 2005). For an older adult isolated in an inpatient setting, a warm smile and friendly disposition can meet felt spiritual needs. This finding underscores the importance of self-monitoring to avoid merely “going through the motions.” The result also underlines the powerful impact that seemingly routine interactions can have in the lives of some older adults.
Limitations
In a manner analogous to those conducting meta-analyses (Littell et al., 2008), meta-synthesizers do not usually have access to the original data (Bondas & Hall, 2007). Sources of bias in the original, primary studies can introduce bias into the synthesis (Bondas & Hall, 2007). Similarly, using quotations to illustrate categories—typically a strength of qualitative research—is problematic. While the quotes reported in the original studies are factored into the analytical process, as a study of studies, a meta-synthesis is conducted at a higher level of abstraction. Without access to primary data, it is difficult to include quotes because meta-synthesizers cannot be assured they are representative.
The lack of generalizability associated with this approach should also be reiterated. In addition to the relatively small aggregate sample size, the primary studies did not include many older adults from traditions such as Islam or Hinduism. Therefore, the results may have limited utility with such populations. This is an important consideration in light of the growing diversity among older adults (Berkman, Gardner, Zodikoff, & Harootyan, 2005; Eck, 2001).
The primary studies included a variety of designs that in turn may have influenced the results (Kasworm, 1990). For instance, older adults interviewed at hospitals by professionals may be reluctant to share spiritual needs, which may have been poorly addressed, while receiving care from this same general set of professionals. Alternatively, individuals interviewed subsequent to their hospitalization may fail to completely recall spiritual needs that were acutely felt at the time of hospitalization.
The degree of homogeneity required to combine studies is an issue in any analysis based on aggregated findings, whether quantitative or qualitative (Littell et al., 2008). In meta-analyses, it is not uncommon for substantial heterogeneity to exist. Studies may vary by type of intervention, study design, and outcome measures, depending on the state of the research in a given area, the researchers’ goals, and other variables (Kaplar, Wachholtz, & O’Brien, 2004; Masters, Spielmans, & Goodson, 2006; Smith, Bartz, & Richards, 2007).
In meta-syntheses, it is common practice to aggregate findings if the studies address a similar research question (Bondas & Hall, 2007; Finlayson & Dixon, 2008). As implied in the Method section, this was the basic approach adopted in this synthesis. Within these parameters, some meta-synthesizers support the inclusion of heterogeneous designs as a way to enhance the breadth and depth of the synthesis, while others prefer more heterogeneity among primary studies (McCormick et al., 2003). Researchers who fall into this latter camp may wish to refine the selection criteria used in this study, a practice that becomes more feasible as the number of primary studies on older adults’ spiritual needs increases over time. Meanwhile, the present study fills an important gap in the existing literature by providing a richer, fuller understanding of the spiritual needs older adults may experience in health care settings.
Conclusion
Admission into health or behavioral health care systems often engenders the emergence of spiritual needs (Nelson-Becker et al., 2007). Many older adults want practitioners to address these needs (Flannelly et al., 2005), and research has linked addressing spiritual needs with a number of positive health-related outcomes (Astrow et al., 2007; Balboni et al., 2007). In recognition of this reality, the Joint Commission requires spiritual assessments in a number of health care organizations frequented by older adults (Hodge, 2006; Koenig, 2007).
In practice, however, older adults’ spiritual needs are often overlooked or inadequately addressed, perhaps due to lack of practitioner familiarity with the spiritual needs older adults commonly experience in health care settings (Anderson et al., 1993). This study fills an important knowledge gap in the gerontological literature by identifying common spiritual needs and providing examples of how these various needs are manifested in health care settings. By familiarizing practitioners with the needs older adults commonly experience in health care settings, practitioners are better equipped to meet those needs. In addition, by meeting older adults’ spiritual needs, practitioners provide more holistic, client-centered services that help clients cope, recover, and thrive in the midst of often difficult circumstances.
Footnotes
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article:
Preparation of this article was supported by a grant from the John A. Hartford Foundation.