
Abstract
This article introduces a new model for the treatment of posttraumatic stress disorder that has the potential to provide clinicians with information that may facilitate improved outcomes. The PACT model emerged during a systematic literature review intended to suggest ways to enhance the efficacy of evidence-based treatments by critically evaluating the potential mechanisms of therapeutic action at work in a novel treatment approach, MDMA (3,4-Methylenedioxymethamphetamine)-assisted psychotherapy, and applying this understanding to existing treatment protocols. The goal of the review was to synthesize the potential therapeutic mechanisms of action that are involved in this approach, and to better understand how they could inform other protocols without the need to administer MDMA. Four elements of MDMA-assisted psychotherapy that do not require the administration of MDMA and could inform our approach to treating patients with trauma form the basis of the PACT model: (1) Presence; (2) Acceptance; (3) Connection; (4) Transcendence. This article highlights how the PACT model reflects the qualities and values of humanistic–existential therapies, explains how it overlaps with and extends common factors in psychotherapy, and suggests how these four elements may signify important avenues of future research for trauma treatments, focusing on enhancing the patient’s experience of safety and posttraumatic growth.
Keywords
Posttraumatic stress disorder (PTSD) is considered a severe and debilitating disorder, with personal and social consequences that can include trouble with day-to-day functioning, interpersonal difficulties, increased irritability and anger, diminished cognitive and psychosocial functioning, increased suicide risk, and substance abuse (Haviland et al., 2016). A majority (70%) of adults worldwide will or have experienced a traumatic event at some point in their lives, and approximately one-third will experience three or more events (Shalev et al., 2017). Following trauma, some individuals will develop PTSD, which co-occurs more than 50% of the time with mood, anxiety, or substance-use disorders, and is associated with serious disability, increased risk for chronic illness and suicide, premature death, and a significantly altered and diminished quality of life in the aftermath of trauma (Shalev et al., 2017).
With many of society’s most vulnerable members presenting with the highest risk of developing PTSD, including women, emergency response personnel, military veterans, and police officers, the search for effective treatments has garnered significant research and public attention. In 2017, the Veterans Health Administration and Department of Defense and the American Psychological Association (APA) each published treatment guidelines for PTSD. Both sets of guidelines strongly recommended the use of three specific evidence-based treatments (EBTs): cognitive behavioral therapy (CBT), cognitive processing therapy (CPT) and prolonged exposure therapy (PE). However, the efficacy of these recommended treatments is mixed, with many studies documenting poor retention and high dropout rates with correspondingly low overall rates of recovery (e.g., Eftekhari et al., 2019; Najavits, 2015). Outcomes appear worse for veterans; for example, one review found that approximately 60% to 70% of military patients retained their PTSD diagnosis even after treatment (Steenkamp et al., 2015).
The purpose of this article is to introduce a new model that has the potential to provide clinicians with information that may facilitate improved outcomes for the treatment of PTSD. The PACT model emerged during a systematic literature review of peer-reviewed, published research (see Larova, 2020). While the model does not necessarily introduce novel therapeutic concepts, it does introduce an emphasis on aspects of treatment that are notably absent from the evidence-based models recommended by the Veterans Affairs (VA). As such, the PACT model is particularly relevant as a proposed adjunctive or integrative model for VA clinicians who are working from these approaches. The purpose of the review was to suggest ways to enhance the efficacy of EBTs by critically evaluating the potential mechanisms of therapeutic action at work in MDMA (3,4-Methylenedioxymethamphetamine)-assisted psychotherapy and applying this understanding to existing treatment protocols. This is a treatment approach where clients receive a course of psychotherapy along with one to three doses of pharmaceutical-grade MDMA (Sessa, 2017a). MDMA-assisted psychotherapy has demonstrated efficacy in six completed Phase 2 clinical trials thus far, as summarized by Mithoefer et al. (2019). The six completed trials enrolled a total of 105 participants, the majority of whom had a history of positive suicidal ideation (86.8%) and/or behavior (30.9%), and who had experienced PTSD for an average duration of 17.9 years. All participants had chronic, treatment-resistant PTSD. The dropout rate across the six studies was 7.6% (8/105). At the conclusion of treatment, 66% of participants in the experimental group no longer met diagnostic criteria for PTSD. Given these positive results, especially in relation to the low dropout rate, the goal of the systematic literature review (Larova, 2020) was to synthesize the potential therapeutic mechanisms of action that are involved in this approach, and to better understand how they could be applied to other protocols without the need to administer MDMA, which remains a controlled, Schedule I substance in the United States at the time of this writing.
MDMA-Assisted Psychotherapy
In the past 15 years, there has been a resurgence of interest in MDMA-assisted psychotherapy to treat PTSD. First adopted in the 1980s and shortly thereafter aborted due to public health concerns (Sessa, 2017b), this treatment is one where clients receive a course of psychotherapy along with MDMA-assisted sessions (Sessa, 2017a). As stated above, the outcomes of clinical trials have been positive. Mithoefer et al. (2010) reported results from the first randomized controlled study testing MDMA-assisted psychotherapy against placebo on 25 subjects with treatment-resistant PTSD. Eighty-five percent of those treated with MDMA-assisted psychotherapy no longer met criteria for the disorder after a single course of treatment (involving taking MDMA three times during a 16-week course of weekly psychotherapy sessions). A long-term follow-up of this cohort showed that, with no further intervention, the results were maintained four years later (Mithoefer et al., 2012). Similar promising results were found in later studies, including six Phase 2 clinical trials (Thal & Lommen, 2018). In addition, there have been promising long-term results in treatment-resistant PTSD patients, defined as those who have tried at least one course of either psychotherapy or pharmacotherapy without relief, with more than two thirds (68%) of those treated by MDMA-assisted psychotherapy no longer meeting diagnostic criteria for PTSD 12 months following treatment (Mithoefer et al., 2019).
However, the current illegal status of MDMA makes direct application of these favorable treatment findings impracticable for clinicians treating individuals with PTSD. Thus, the systematic literature review (see Larova, 2020) was conducted to answer the question: What lessons learned from MDMA-assisted psychotherapy could be applied to EBTs? In answering the overarching research question, a new model emerged.
Research Methodology/Data Collection
When discussing the significance and mixed results of EBTs in the treatment of PTSD, Schnyder et al. (2015) have pointed out that systematic research is particularly useful because it can (1) help identify mechanisms of therapeutic action that have been overlooked by previous studies and may significantly affect treatment outcomes, and (2) reveal effective treatment elements which can inform therapies overall. MDMA-assisted psychotherapy to treat PTSD is a novel therapeutic approach that has consistently demonstrated promising results in successfully treating this disorder, and there is much to be learned from this treatment approach regarding pretreatment factors, structural treatments factors, the neurobiological effects of MDMA, and other areas of importance that could be applied to EBTs for PTSD, whether or not the medicine MDMA is ever utilized. The purpose of the comprehensive review and critical evaluation of treatments for PTSD was to analyze peer-reviewed, published research and increase our understanding of tools for healing injuries to the mind, brain, and body that result in trauma symptoms.
Larova (2020) sought to critically analyze study results in order to formulate research-backed hypotheses to understand why this form of treatment has produced such promising initial outcomes, and whether any of the therapeutic mechanisms involved might be utilized to improve current EBT protocols, without actually needing to administer MDMA. Specifically, Larova (2020) sought to understand the potential therapeutic mechanisms at work in MDMA-assisted psychotherapy to treat PTSD in comparison to EBTs for trauma. To accomplish this task, previously published research on EBTs for trauma was selected for review (and reviewed for selected themes such as participant retention, treatment effectiveness, treatment set-up, roles of the therapist, training of the therapists, and so on), as well as published research on MDMA-assisted psychotherapy for PTSD.
The methodology utilized for this research was Preferred Reporting Items for Systematic Reviews and Meta-Analyses, a systematic review method of data collection that was performed in accordance with the most up to date Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines (Larova, 2020; Liberati et al., 2009). Data in the form of published research was collected for the study pertaining to EBTs for PTSD (CBT, CPT, and PE) as well as MDMA-assisted psychotherapy to treat PTSD. No original data was collected. All research publications selected were carefully examined for their relevance to the stated research questions. Only those articles that could shed light on the specific research questions or offer a useful contribution were included in the study. Reference lists of relevant review articles were manually searched to identify any further studies of interest. A subset of the sources retrieved (55) were identified as the most relevant sources for this study and provided the foundation of the literature review. While older articles were also referenced to provide a background on the historical context of EBTs and MDMA-assisted psychotherapy, or to fill in gaps in recent publications, the majority of articles referenced for the study were published within the past 5 years.
This research was reviewed to critically evaluate the varied effectiveness of these treatments in relation to the healing of PTSD; proposing that there are pre-treatment factors, structural treatment factors, and specific neurobiological effects at work in MDMA-assisted psychotherapy that may be positively influencing PTSD treatment outcomes and could theoretically be applied to enhance existing treatments for PTSD and trauma. The PACT model emerged out of this review.
The PACT Model
Elements of MDMA-assisted psychotherapy that do not require the administration of MDMA and could be used to enhance current EBT protocols form the basis of the PACT model: (1) Presence, (2) Acceptance, (3) Connection, (4) Transcendence (see Figure 1). Each element is discussed below.
The PACT model.
Presence
In the model, presence has a threefold meaning: (1) the therapist’s presence, (2) the therapist’s presentation, and (3) the presence of the setting where therapy takes place. The therapist’s presence reflects the therapist’s attitude and openness to their patient, as well as their capacity to withstand and metabolize their own anxiety when faced with a client’s trauma or symptoms. The therapist’s presentation reflects the therapist’s professionalism and confidence in their treatment approach, meaning a genuine personal conviction that the model they are using is effective. A general rule of thumb is an affirmative answer to: Would you recommend the approach you are using to your loved ones? These form the first two aspects of the concept of presence in the PACT model.
The third aspect refers to the physical setting where therapy takes place. Because MDMA tends to heighten the senses, a quality that the empathogen shares with psychedelics such as psilocybin or lysergic acid diethylamide, the patient frequently becomes acutely sensitive to their environment (Mithoefer, 2017). As such, preparing the physical setting for treatment, ensuring that it is comfortable, aesthetically pleasing, and evokes feelings of nurturance and safety, is uniformly observed as an integral aspect of psychedelic-assisted therapies, and MDMA-assisted psychotherapy in particular (Mithoefer, 2017). While the EBT manuals (CPT and PE) surveyed do underline the importance of the therapist’s attitude and conviction in the treatment method, neither mentions anything about the physical environment or aesthetics of treatment (Foa et al., 2019; Resick et al., 2016). As trauma shares a primary association with one’s sense of safety being violated, it would make sense that a treatment room and environment that are evocative of feelings of safety and comfort would positively influence therapy. A warm and inviting space, that connotes professionalism and comfort, is an essential element of trauma treatment.
The therapeutic setting is naturally assumed to be important across virtually all therapists who work in private practice and tend to arrange and decorate their space in ways that invite trust, reflection and feelings of ease and relaxation in their patients. Similarly, acupuncture clinics, spas, retreats, and other places where people go to restore their spirits, including natural settings such as mountains or parks, have an aesthetic quality to them that is intuitively understood to be of great importance. A biobehavioral explanation includes the understanding of neuroception, a process that occurs without conscious awareness and triggers feelings of safety or danger (Geller & Porges, 2014). Thus, the PACT model highlights the presence of the setting, or where therapy takes place, as constituting an important “therapeutic third” following the dyad of therapist(s) and patient. This aspect of the model suggests that a clinician treating patients with trauma might consider spending time thoughtfully evaluating the setting where therapy will take place, including the furniture, layout, color, light quality, and artwork. In short, this element of the model suggests that a patient’s experience of feeling safe may be supported and enhanced when these elements of presence are attended to.
Acceptance
The therapeutic approach in MDMA-assisted therapy is characterized by the quality of acceptance. Acceptance in this context means practicing a nondirective style of therapy, where therapists allow sessions to flow naturally, accept silence as an important part of treatment, and allow the participant’s experience to guide the sessions (Mithoefer, 2017). A therapeutic team (MDMA-assisted psychotherapy is conducted with two therapists) provides a holding space within which the participant’s own psyche or inner healer can take charge of the treatment, which is especially important as MDMA takes the participant into a heightened state of both connection and vulnerability (Mithoefer, 2017). This approach is reminiscent of supportive therapy, which at least one study of EBTs found to be the preferred treatment of choice in VA providers treating patients with PTSD (Borah et al., 2013), but differs from other approaches that actively target memory “hot spots,” or parts of the patient’s traumatic memory that are especially distressing for them—as PE therapists are instructed to do (Foa et al., 2019). As the VA’s current PTSD treatment guidelines highlight EBTs that put the therapist in a very active and directive role, this aspect of the PACT model is particularly relevant in informing how VA clinicians could enhance purely procedural evidence-based models.
Many clinicians share an understanding that acceptance, rather than force, is a healing agent. Dr. Bruce Perry and Maia Szalavitz (2017), a child psychiatrist whose work has largely focused on traumatized children, writes: Over and over again the research finds that if you use force, if you push people to open up when they aren’t ready, if you require participation in therapy, if you don’t respect individual differences, then your treatment can actually do serious harm. Because safety is critical to recovery and force creates fear, coercive therapies are dangerous and ineffective for victims of trauma. (p. 275)
This element in the model suggests that approaching sessions with a “beginner’s mind” may be very important. In the context of therapy, this means emptying one’s mind of preconceived notions of what the patient’s process will be like, as well as being free from expectations and interpretations of the patient’s process. Applied to EBTs, this could be akin to practicing the discipline of form before freedom, where clinicians become expert in the methods of CBT, CPT, or PE, such that they are able to both flexibly call on them as needed and improvise them to suit different patients. Especially in trauma therapy, patient rapport and feelings of safety are essential—and greatly enhanced when the clinician shows an openness to respond to the patient’s own readiness, perspective, and shifting engagement with the pacing, flow, and direction of therapy.
Connection
Connection between the clinician and patient is paramount in achieving treatment goals, and this is especially true in patients with PTSD who often experience interpersonal difficulties or struggle with achieving trust, reliance, and feelings of safety in relationships (APA, 2017). The therapeutic relationship has been called the sine qua non of effective therapy. An interdivisional APA task force on evidence-based therapy relationships found that the therapy relationship is at least as important as the treatment method, and that therapy relationships make substantial and consistent contributions to psychotherapeutic outcomes, independent of treatment method (Geller & Porges, 2014; Norcross & Lambert, 2018). Interestingly, there appears to be a relatively dismissive view of building the therapeutic relationship in CPT and PE manuals, describing, for example, that “sessions devoted exclusively to trust building are not needed” (Resick et al., 2016, p. 35). The PE manual presents a similar perspective, recommending that no more than two sessions should be aimed at preparing for exposure or building rapport (Foa et al., 2019). These suggestions stand to be questioned, in particular given that the research data consistently shows that such a high number of patients drop out of these treatments early on in treatment (Eftekhari et al., 2019; Watts et al., 2014).
In contrast, the MDMA-assisted psychotherapy treatment manual describes the development of therapeutic alliance and trust as essential to treatment (Mithoefer, 2017). Although there are no sessions geared specifically toward trust building per se, the three initial, 90-minute preparatory sessions that are part of the course of treatment both introduce and follow a nondirective approach that intentionally supports the growth of a strong therapeutic alliance. While it is true that the neurophysiological effects of MDMA (which is known to increase feelings of love, safety, and trust, as well as to enhance empathy for self and others and interpersonal closeness) also likely play a role in connection, a clinician treating individuals with PTSD can work to foster a strong therapeutic relationship without the medicine (Amoroso & Workman, 2016; Bershad et al., 2016).
A solid bond of trust between therapist and client facilitates healing from PTSD. While trauma-focused treatments like TF-CBT, CPT, and PE have been widely disseminated across the VA and found to be somewhat effective for those who complete them—many studies have consistently shown that few veterans do, with several demonstrating completion rates of less than 10% (Mott et al., 2014; Schnyder et al., 2015; Seal et al., 2010; Watts et al., 2014). As such, prioritizing the connection between therapist and patient rather than the pacing of a manualized treatment may be especially relevant for VA clinicians. Trauma-focused EBTs may benefit from adding several initial sessions to support the building a strong therapeutic relationship prior to beginning highly triggering exposure work or cognitive restructuring on traumatic memories, thoughts, and associated feelings, similar to the three 90-minute introductory sessions that are part of MDMA-assisted psychotherapy. Geller and Porges (2014) have investigated how therapeutic presence can be used to facilitate feelings of safety and connection in both therapist and client through activating the ventral vagal system via expressed markers of social engagement such as facial expressions, vocal tone, and gestures that communicate safety and reduce defensiveness. In an effort to enhance connection, therapists may utilize research drawn from polyvagal theory to enhance their initial sessions by helping activate social engagement, reduce defensiveness, and build trust in clients with PTSD.
Transcendence
Transcendence is an evocative word, which can be suggestive of spiritual, mystical, or somehow otherworldly experiences that transcend conscious reality. In the context of the PACT model, the meaning is twofold: (1) inclusion of positive experiences in treatment (allowing space for the patient to experience a transcendence of PTSD symptoms, which can include but is not limited to spiritually transcendent experiences); and (2) posttraumatic growth.
In MDMA-assisted psychotherapy, positive experiences that include mystical, spiritual, or transcendental experiences typically arise naturally, in part as a result of the pharmacological effects of MDMA on the brain (Mithoefer, 2017). During the MDMA-assisted sessions, while therapists are there to support participants in processing their painful experiences and traumatic memories, Mithoefer (2017) points out that: . . . therapists are also there to help explore and validate new perspectives about other life experiences, as well as to join with participants in appreciating joyful or affirming experiences and enjoying moments of beauty, heart opening, and humor. (p. 31)
Experience has shown that early positive experiences can “provide the participant with a platform from which the participant is then later able to approach the emergence of traumatic memories and painful emotions with a greater sense of strength and safety” (Mithoefer, 2017, p. 36).
This is an important point to carry forward to EBTs. While Foa et al. (2019) do point out that in PE, part of the clinician’s role is to act as a cheerleader and source of encouragement for the patient in focusing on their traumatic memories, this is very different from actively facilitating or encouraging positive experiences as part of treatment. Transcendental experiences may include any experience that helps patients have a felt positive experience of what it may be like to live without PTSD. These experiences could take the form of outdoor excursions, the addition of yoga or art classes, meditation, or sessions focusing on posttraumatic growth—all of which have shown benefit in studies evaluating their effects on PTSD (e.g., Campbell et al., 2016; Rhodes et al., 2016).
For example, Campbell et al. (2016) found that when art therapy was combined with CPT to treat veterans with combat-related PTSD it not only improved cognitive processing (compared with those receiving CPT alone), but veterans also reported that they considered it an important part of their treatment. These subjective reports of what works or “feels right” in therapy deserve further attention. Other approaches such as brief eclectic psychotherapy for PTSD, which focuses on creating meaning from one’s traumatic experience, have also shown promising early results in the domain of posttraumatic growth following trauma (Nijdam et al., 2018). Elements of therapy that play an important role in facilitating healing but are not focused exclusively on measurable symptom reduction or elimination, as cognitive and exposure-based therapies tend to be, may represent a significant oversight in existing EBTs.
Posttraumatic growth was defined by Knaevelsrud et al. (2010) as the patient’s subjective experience of positive psychological change following a traumatic event, and Nijdam et al. (2018) found that a decline in PTSD symptoms was significantly related to greater increase in posttraumatic growth. Author and retired therapist Mary Pipher reflects on this phenomenon as “the transcendent response to trauma,” writing: “When something too big for us to handle happens to us, our only healthy response is to grow bigger” (Pipher, 2016, Loc. 198). According to research reviewed by Nijdam et al. (2018), cognitive behavioral and exposure therapies seem to have only a small to moderate impact on posttraumatic growth (Roepke, 2015; Schnyder et al., 2011; Schubert et al., 2015; Wagner et al., 2016). In contrast, in a review of participants who had received MDMA-assisted psychotherapy (n = 60), it was found that treatment resulted in both posttraumatic growth and clinical symptom reductions of large magnitude effect sizes (Gorman et al., 2020). These findings suggest that posttraumatic growth represents an important but understudied mechanism of action in treating PTSD. Trauma-focused EBTs could benefit from including additional interventions that support posttraumatic growth, for example, through encouraging positive developments in self-perception, interpersonal relationships, or philosophy of life, additions which would necessarily stretch existing EBT manualized treatments in length—but potentially also in quality and the ability to effect more significant healing.
The PACT Model and Humanistic–Existential Therapy
In developing the PACT model and drawing theoretical conclusions, it was found that these four elements in many ways reflect central aspects of humanistic or existential therapy to treat PTSD. While many clinicians naturally draw on these aspects in their clinical work, humanistic or existential psychotherapy is not among the strongly recommended EBTs for PTSD by the APA (2017) or the VA/DoD (Veterans Health Administration and Department of Defense, 2017). However, these distinct elements are clearly present in an efficacious treatment for PTSD, MDMA-assisted psychotherapy, and existing research consistently supports the enduring importance of common factors in psychotherapy, such as empathy, collaboration, and positive regard (Norcross & Lambert, 2018).
Vachon et al. (2016) observed that healthy human development throughout childhood is facilitated by a perception of the world as safe, benevolent, and meaningful, and the self as worthy. This correlates with the PACT model as follows: (1) World as safe (Presence), (2) Self as worthy (Acceptance), (3) Others as kind (Connection), and (4) Life as meaningful (Transcendence). These humanistic and existential concerns are further summarized in Figure 2, which shows a comparison of the PACT model with Maslow’s (1970) theory of human motivation and hierarchy of needs pyramid.
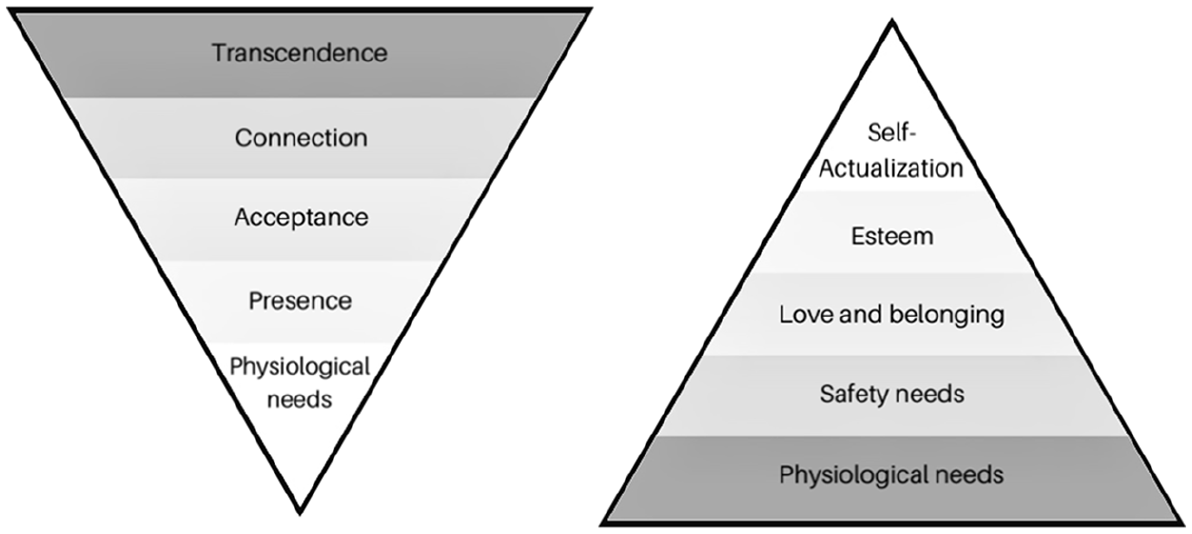
The PACT model versus Maslow’s (1970) hierarchy of needs.
With a common foundation of physiological needs, the four elements of the PACT model roughly reflect an inverted version of Maslow’s hierarchy of needs as follows: (1) Presence, including the physical setup of the room (Maslow’s Safety needs); (2) Acceptance (Maslow’s Love and belonging needs); (3) Connection (Maslow’s Esteem needs); (4) Transcendence (Maslow’s Self-actualization). The inversion of the pyramid is intentional, as it may be significant in visually demonstrating the relative importance of these different aspects in addressing the existential wounds of trauma. While the basic satisfaction of physiological needs is indeed the foundation of all health, including mental health, in healing from the aftershock of psychological trauma—which has shaken an individual psychically rather than physiologically—the relative importance of the higher aspects of the pyramid increase and represent an effort to realign in an existential sense.
Interestingly, prior to his death, Maslow had wanted to add a new pinnacle to his triangle: Self-transcendence, which he defined as follows: Transcendence refers to the very highest and most inclusive or holistic levels of human consciousness, behaving and relating, as ends rather than means, to oneself, to significant others, to human beings in general, to other species, to nature, and to the cosmos. (Maslow, 1970, p. 269)
When faced with trauma, our sense of inhabiting the world in a safe, coherent, and meaningful manner is deeply disturbed (Vachon et al., 2016). The sense of organizing ourselves vis-à-vis reality is disrupted, and transcendental or peak experiences are powerful avenues through which this intangible but incredibly important organizational function can be restored. In another sense, it may be said that when higher order levels of functioning in the world (e.g., a sense of the world as benevolent or one’s life as meaningful) are disrupted, higher order level interventions are needed to restore health. While MDMA-assisted psychotherapy—which facilitates an environment and experience that can accelerate the recovery of a sense of meaning, purpose, and agency in an individual’s life—may be uniquely suited toward supporting recovery from PTSD, there are other, nonpharmacological elements of this approach that could be utilized by EBTs to extend support to the whole-person’s healing from PTSD, which necessarily includes their existential selves. Shattered assumptions and the incapacity to integrate an overwhelming experience form the core of a humanistic–existential understanding of trauma, and the PACT model reflects a therapeutic model that extends our focus beyond symptom reduction to assist in the reparation of the wounded self.
The PACT Model and Common Factors in Psychotherapy
The elements described under the PACT model share some common ground with research from the last decade stemming in part from the APA’s Third Interdivisional Task Force on Evidence-Based Relationships and Responsiveness; however, they also diverge in that these elements arose from evaluating a novel and trauma-specific treatment modality (Mithoefer et al., 2019; Norcross & Lambert, 2018). For instance, the therapist’s capacity for empathy is considered essential across all psychedelic-assisted therapies, and a universally agreed-on quality of a well-trained therapist (Phelps, 2017). While this is not unusual in the realm of all psychotherapy, in MDMA-assisted psychotherapy this qualification is taken a step further and is one of the seven unique therapist skills that Adherence Raters (who view and evaluate video recordings from the therapy sessions) assess to ensure therapists are maintaining fidelity to the treatment model (Phelps, 2017). Common factors in psychotherapy are factors that have been shown to have a demonstrable affect on treatment outcomes irrespective of the therapist’s modality.
Among relationship elements deemed “demonstrably effective” in psychotherapy outcomes, Norcross and Lambert (2018) include the following: alliance in individual psychotherapy, collaboration and goal consensus, empathy, and positive regard and affirmation. These elements show significant overlap with elements of the PACT model, but the PACT model also proposes specific shifts in interventions toward a more nondirective approach, intentional setup of the area where therapy takes place, and purposeful inclusion of transcendental experience—areas of intervention which theoretically bring about the “common factors” deemed effective by Norcross and Lambert (2018). While clinical trials of EBTs do not traditionally assess for the presence or absence of common factors in psychotherapy such as empathy or relative strength of the therapeutic alliance, they also arguably do not explicitly include elements meant to bring them about. Even still, “there is probably no issue more central to clinicians than the evolution of EBTs in psychotherapy,” according to Norcross and Lambert (2018).
A great deal of foundational wisdom and insight came from Carl Rogers’ (1992) seminal article on “necessary and sufficient” conditions for therapeutic change, where he noted his surprise, “at the simplicity of what has emerged” after many years of clinical practice and reflection (p. 95). Of the six tenets highlighted by Rogers (1992), empathy, unconditional positive regard, and acceptance all naturally overlap with aspects of the PACT model and the common factors highlighted by Norcross and Lambert (2018). However, while Rogers (1992) emphasized the universality of his six tenets across diverse patient populations, it is the authors’ view that the wounds of trauma do require particular attentiveness to elements of safety, including setting, the capacity to accept that processing trauma may look different for different patients, and therapist factors (e.g., accepting silence, not forcibly directing therapy). In attending to these aspects, therapists and the therapeutic environment are applying humanistic/existential tenets of trauma therapy and reintroducing the concept and felt experience of a safe, benevolent, and coherent world where the individual’s experience matters greatly (Vachon et al., 2016).
Practical Applications
The PACT model has important practical applications that may be especially useful or applicable in environments such as the VA, where the use of manualized EBTs is both encouraged and the official norm. These practical applications include paying conscious attention to the presence of the physical setting where treatment takes place; therapists being aware of how their presentation comes across to the patient and utilizing greater flexibility in the application of EBT and other treatment protocols, to ensure that a patient’s individual preferences are taken into account and that patients feel heard rather than herded into a standardized form of treatment; allowing more time and attention for building a strong therapeutic relationship at the beginning of treatment, prior to beginning exposure or cognitive therapy; and including opportunities for positive expression, joyful felt experience, creativity, transcendent experience or discussions of meaning surrounding the patient’s trauma to encourage posttraumatic growth, an understudied but potentially highly significant correlate of symptom reduction in PTSD.
Recommendations for Research
Further research on the treatment mechanisms and therapist qualities important to the effective treatment of trauma is needed. As pointed out by Cloitre (2009), a “one size fits all” approach to psychotherapy is inconsistent with what we know about the complexity of trauma, heterogeneity of symptoms, and difficulty with patient engagement, adherence, and outcomes in therapies for PTSD. Additional and controlled research studies addressing the relative importance of various aspects of the PACT model could not only provide critical empirical support and validation of these elements but also highlight which elements deliver the most significant impact, whether in terms of symptom reduction or participant engagement—two equally important aspects.
Due in part to the relatively controversial nature of MDMA-assisted psychotherapy and the need to closely monitor, record, and supervise all related data collection emerging from these studies, there is prospectively a large amount of research that is available for future analysis. Conducting research on elements of the PACT model highlighted by MDMA-assisted psychotherapy could, for example, review and analyze the adherence ratings of sessions along the seven scored dimensions of: communicating safety and support, empathic presence, establishing rapport, verbal communication, eliciting pertinent information, addressing questions and concerns, and nondirective approach (Phelphs, 2017). These dimensions could be collapsed into the four distinct elements of the PACT model, and the thematic areas could be compared with outcome measures specific to PTSD symptomology and/or posttraumatic growth.
Additionally, it would be possible to do a cross-comparison of those patients treated with MDMA-assisted psychotherapy versus control cases who receive an identical course of psychotherapy, absent the MDMA. A thorough analysis could both: (1) compare control and experimental cases on the basis of these aspects in the comparative strength and influence on recovery of elements of PACT model; and (2) separately compare the control cases in outcome rates with those treated by EBTs, where such treatment elements are not assessed at all. This proposed research could demonstrate whether elements of the PACT model are influential and by which degree; the relative importance of different elements of the PACT model; and whether control groups in MDMA-assisted psychotherapy demonstrably improve in comparison with patients treated with EBTs of similar length.
In line with recommendations to further develop personalized treatments for PTSD, more research attention should also be paid to culturally sensitive interventions, particularly in light of the evidence base consistently showing that socioeconomic disparities and racial differences reflect disparate risk factors of developing PTSD, with minorities experiencing higher risk for both experiencing trauma and developing the disorder (e.g., Sibrava et al., 2019).
Conclusion
The purpose of this article was to present a model that emerged from a systematic literature review and identified ways in which the lessons learned from MDMA-assisted psychotherapy could be applied to existing EBT protocols, without the administration of MDMA. The four elements of the PACT model are avenues through which EBT protocols could be enhanced to support increased rates of patient retention, adherence, and, most importantly, recovery, and may be particularly applicable to VA clinicians as one potential avenue through which existing EBTs could be enriched (e.g., Berke et al., 2019; Eftekhari et al., 2019; Watkins et al., 2018). Rather than keeping to a flat diagnostic conceptualization of PTSD as a cluster of symptoms implicated by impaired memory reconsolidation and fear extinction, when the disorder is viewed through a humanistic–existential lens as a disruption in self-cohesion, then treatments must necessarily rise above symptom management to also address these existential and humanistic concerns. The PACT model represents an effort to humanize and enhance existing EBTs along these lines and suggests four ways that this could be done based on the proposed therapeutic mechanisms at work in MDMA-assisted psychotherapy.
The model reflects the qualities and values of humanistic–existential psychotherapies. Importantly, the visual representation of the PACT model reflects the interlinked quality of the four aspects, as well as their symbiotic nature in treatment. The visual inversion of Maslow’s pyramid to reflect the structure of the PACT model intentionally reflects the increased importance given to transcendence, defined by this model as incorporating transcendental or meaning-making experiences as part of the treatment for PTSD. Other elements of this treatment model include building a solid connection with the patient, helping them to feel accepted in the authority of their own experience, and intentionally communicating an ongoing presence in the treatment room through both the environment and treating professional that supports feelings of safety, comfort, and trust.
Additional research on the treatment mechanisms and therapist qualities important to the effective treatment of trauma is needed; the PACT model offers up constructs worthy of further investigation. In treating trauma, we are repairing the fabric of society and so long as available treatments return less than optimal results, the fabric of society will continue to fray. In an effort to weave together a new story of healing, we propose the PACT model to assist with the evolution of trauma treatment.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.