
Abstract
This study was conducted to identify processes of coping with COVID-19 and determine their impact on emotional well-being for women of color in the United States. Data were collected from 368 women between May and July 2020 using an online survey guided by the Transactional Model of Stress and Coping, which included an assessment of COVID-19 stressors, Brief Encounter Psychosocial Instrument (BEPSI), 10-item Connor-Davidson Resilience Scale (CD-RISC-10), Ways of Coping Questionnaire (WCQ), and Center for Epidemiologic Studies Depression Scale (CES-D). Over half of the women were depressed (59.0%) and felt ill (69.3%) from the stress of COVID-19. Planful problem solving (M = 4.58, SD = 2.70) was the primary way to cope with COVID-19. A small, positive correlation existed between COVID-19 stressors and depressive symptoms (r = 0.27, p < .001). COVID-19 had a significant impact on the increase of stress (MI = 0.53, p < .001) and depressive symptoms (MI = 5.90, p < .001) as well as the decrease of resilience (MD = 2.17, p < .001) for women of color in the United States. These results can be translated into actionable care plans for clinicians and public health professionals that inform the development of tailored, culturally appropriate, equitable, and gender-specific mental health care for women of color in the age of COVID-19.
Keywords
Introduction
In the United States, the risks faced by women are compounded by being a person of color (POC). By and large, POC have been at a higher risk of contracting and succumbing to COVID-19 due to the increased likelihood of pre-existing chronic disease conditions, multigenerational and close-quarter housing, and improper access to health care and resources due to historic inequities (Bhopal, 2020; Fortin, 2020; Laurencin & McClinton, 2020; Smith & Judd, 2020). Therefore, the intersectionality of being both a woman and POC in the United States is an important concept to examine during COVID-19. The experience of oppression on multiple aspects of identity, both gender and race, invites a unique burden, and together, may compound for a uniquely negative experience (Sanchez-Hucles & Davis, 2010).
The aim of this study was to identify the processes of coping with COVID-19 and to determine the impact on emotional well-being for women of color (WOC) in the United States. Furthermore, this research addressed the mechanisms of resilience using the transactional model of stress and coping (TMSC) (see Figure 1). The TMSC is a classic theoretical framework, which evaluates the process of coping with stressful events (Lazarus & Folkman, 1984). Therefore, the TMSC was used in this study to investigate how WOC in the United States are coping with the stress of COVID-19. The following research questions were developed based on the TMSC: (1) In the wake of COVID-19, what types of coping are predominantly utilized by WOC in the United States? (2) In the wake of COVID-19, what is the relationship between stressors related to COVID-19 and depressive symptoms for WOC in the United States? (3) In the wake of COVID-19, what impact does cognitive appraisal have on coping efforts among WOC in the United States? (4) Does COVID-19 have an impact on stress, resilience, and depressive symptoms for WOC in the United States?
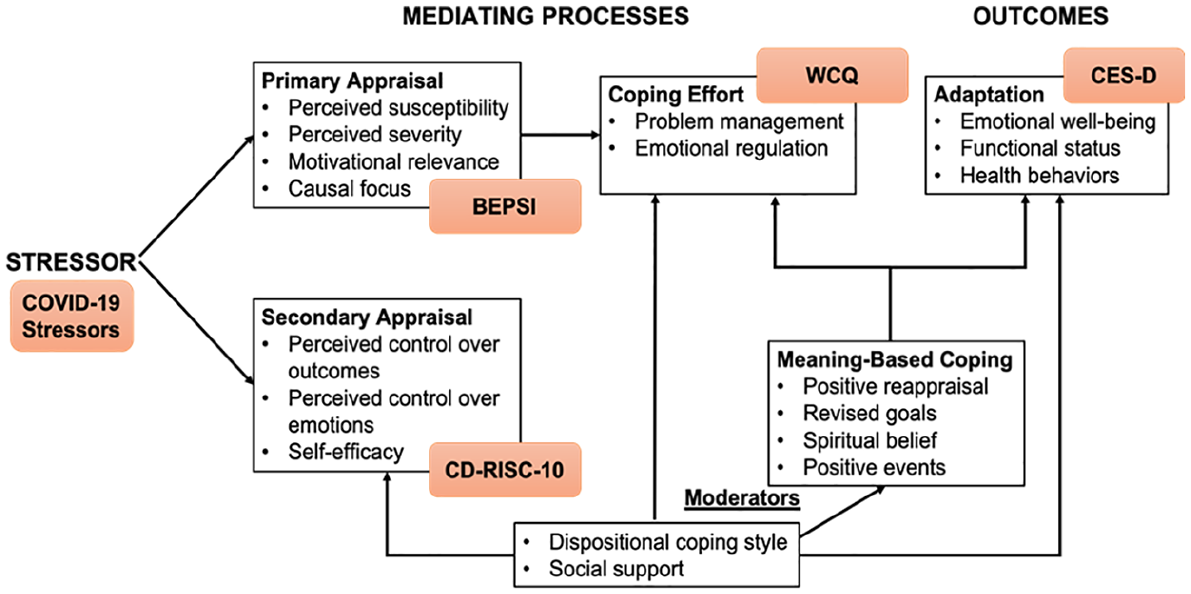
Diagram of the Transactional Model of Stress and Coping.
For decades, issues related to child care at the expense of work opportunities have been a deeply rooted problem for historically excluded and marginalized WOC in the United States. The reality of work and child care are often a source of conflict for WOC (Kamenou, 2008; Michel, 1998). During the height of the COVID-19 pandemic, WOC within the United States were especially burdened by disproportionate responsibilities of family care and are more likely to be essential workers who are unable to work from home while caring for their children (Landau et al., 2020). At the beginning of the COVID-19 pandemic, stay-at-home orders, which were enforced all throughout the United States, resulted in an excessive strain on home life and child care responsibilities. School and day-care closures compounded family care burdens upon women rather than men (Mantovani et al., 2020). In homes where both partners were working remotely during the COVID-19 pandemic, approximately 30% of women reported working less than usual, whereas only 19% of men reported less work (Miller, 2020).
Beyond the domestic nucleus, WOC make up a majority of essential frontline workers, increasing their risk for exposure to COVID-19. Individuals belonging to historically excluded and minoritized groups are more highly represented among essential workers, with 52% being women (Landau et al., 2020; Wenham et al., 2020). Furthermore, women make up about 80% of essential workers in American hospitals, and once the pandemic began, 73% of all health care workers infected with COVID-19 were female (Mantovani et al., 2020; Robertson & Gebeloff, 2020).
Culturally specific coping mechanisms have been shown to be predictive of resilience in some historically excluded and minoritized populations (Clauss-Ehlers et al., 2006). However, minimal literature that characterizes the experiences of WOC during the COVID-19 pandemic is available. In addition, very little information is in the literature addressing how this population manages stress and uses coping processes to survive the adverse effects of the pandemic. Therefore, this study can only begin to address these gaps in the literature by investigating how WOC in the United States are coping with COVID-19.
Materials and Methods
An interdisciplinary research team comprised of members across the United States, including public health faculty and doctoral students, a medical school student, a nursing doctoral student, an early-career faculty member at an osteopathic medical school, and the executive director of a community-based organization, collaborated to develop a cross-sectional online survey guided by the TMSC. This survey was hosted on the Qualtrics platform and disseminated to participants on Facebook, Twitter, and LinkedIn as well as email and text messaging. A diverse group of 368 women responded to the survey. This (n) of women was derived from a study of 891, which was part of a larger online study to examine stress and coping with COVID-19 across the United States. The women were all ages 18 and older, resided in the United States, and self-identified as either Black or African American, American Indian/Alaska Native, Asian, Pacific Islander, or Multiracial.
Prior to data collection, Institutional Review Board (IRB) approvals were received from two institutions (Protocol Numbers 1605172 and 2020-0789). Survey participants responded to emails, text messages, and social media posts between May and July 2020. These messages included a link to the online survey, which was hosted on the Qualtrics (Provo, Utah, USA) platform. Participant online consenting was the first page of the survey and participants could not move forward without consent.
Survey Instrument
The quantitative survey instrument is comprised of five measures designed to evaluate stress and coping with regard to the COVID-19 pandemic for WOC. These measures include: (1) Questions assessing the stressors related to COVID-19, (2) Brief Encounter Psychosocial Instrument (BEPSI), (3) 10-item Connor-Davidson Resilience Scale (CD-RISC-10), (4) Ways of Coping Questionnaire (WCQ), and (5) Center for Epidemiologic Studies Depression Scale (CES-D). Demographic questions were also included to describe the study population.
COVID-19 Stressors
Questions assessing the stressors related to COVID-19 included six items that measured the presence of the stressor in the study. These stressors included financial strain (one item), food insecurity (three items) (Bickel et al., 2000), lack of social support (one item) (Broadhead et al., 1988), and anxiety regarding COVID-19 news reports (one item). These questions were either adapted from validated surveys or developed specifically for this study. Total scores were calculated by adding the sum of responses, where responses were coded from three questions with two answer options (0/1) and three questions with three answer options (0/1/2). Total scores for this measure ranged from 0 to 9, with higher scores indicating more stress related to the COVID-19 pandemic.
Brief Encounter Psychosocial Instrument (BEPSI)
The BEPSI is a 6-item instrument that measures subjective stress and fatigue (Frank & Zyzanski, 1988) and was used to measure primary appraisal in the study. Respondents were asked to complete this instrument at two time points: (1) before COVID-19 and (2) since the COVID-19 pandemic. The first question in the BEPSI assessed the relationship between stress and illness for respondents and was not used for scoring. Scores were calculated by taking the sum of each of the additional five questions that contained a 10-point Likert-type scale and dividing that number by five. Total scores for this instrument ranged from 0 to 10. A participant with a higher final score comparatively experiences more stress (Lee et al., 2015).
10-item Connor-Davidson Resilience Scale (CD-RISC-10)
The CD-RISC-10 provides insight into one’s resilience with health-related stressors. This instrument was used to measure secondary appraisal in the study. Respondents were asked to complete this instrument at two time points: (1) before COVID-19 and (2) since the COVID-19 pandemic. Utilizing a Likert-type scale, 10 items are made up of 10 of the original 25 items from the Connor-Davidson Resilience Scale (Campbell-Sills & Stein, 2007). All of these items were measured by a 0–4 interval-level scale with “0” labeled as “not true at all” and “4” labeled as “true all of the time.” Total scores ranged from 0 to 40. This scale evaluates one’s ability to face adversity and bounce back from stress (Campbell-Sills & Stein, 2007).
Ways of Coping Questionnaire (WCQ)
The WCQ was designed to assess the thoughts and actions individuals use to cope with daily stressful encounters (Folkman et al., 1988) and was used to measure coping in the study. A shortened version of the WCQ (Judge, 1998), which includes 24 items, was used in the survey. The WCQ includes eight subscales. Confrontive coping describes aggressive efforts used to change the situation; distancing describes cognitive efforts to disconnect oneself and minimize the importance of the situation; self-controlling describes efforts to manage one’s feelings and actions; seeking social support describes efforts to seek informational, physical, and emotional support; accepting responsibility recognizes one’s own role in the problem while trying to make things right; escape-avoidance describes wishful thinking and behavioral efforts to avoid the problem; planful problem-solving describes intentional problem-focused efforts to change the situation; positive reappraisal describes efforts to create positive meaning by focusing on personal growth and religion (Folkman et al., 1988).
For this instrument, a paragraph was constructed to focus the respondents on their stressful experiences dealing with the COVID-19 crisis, such as not having enough money to pay bills or buy food, following a stay-at-home order, feeling isolated from friends or family, caring for or losing a loved one, or falling ill because of COVID-19. The sum of the participant’s responses to items for each subscale, which included a Likert-type scale ranging from “0” labeled as “does not apply or not used” to “3” labeled as “used a great deal,” provides a summary of the extent to which each type of coping was used in this stressful encounter. Scores for each subscale ranged from 0 to 9.
Center for Epidemiologic Studies Depression Scale (CES-D)
The CES-D is a short self-report scale designed to measure depressive symptomatology in the general population (Radloff, 1977) and was used to measure emotional well-being, the outcome in the study. Respondents were asked to complete this instrument at two time points: (1) before COVID-19 and (2) since the COVID-19 pandemic. The CES-D was developed to measure the current level of depressive symptomatology experienced by an individual, with a focus on depressed mood. Therefore, the symptoms listed in the scale are among those in which a clinical depression diagnosis is based (Radloff, 1977). The score for the CES-D is the sum of 20 questions. Thus, a possible range for a participant is 0 to 60. A score of 16 points or more is considered at risk for clinical depression (Radloff, 1977).
Data Analysis
Data collected from the online Qualtrics platform was exported into the Statistical Package for the Social Sciences (SPSS, Chicago, IL, USA) version 26 for data analysis. To describe the research participants, descriptive statistics were calculated. Mean scores of the eight coping scales were calculated to identify the three types of coping predominantly utilized by WOC. Pearson correlation was performed to understand the relationship between COVID-19 stressors and depressive symptoms. Multiple regressions were calculated to understand the impact of cognitive appraisal on the eight types of coping. Paired samples t-tests were conducted to evaluate stress, resilience, and depressive symptoms before and since COVID-19.
Results
Description of the Participants
Demographic characteristics of research participants are shown in Table 1. The average age of the 368 women was 42.1 (SD = 14.8) years; and 7% were of Hispanic ethnicity. The race categories represented Black or African American (58.7%), followed by American Indian/Alaska Native (24.2%), Asian (7.1%), Pacific Islander (1.1%), and Multiracial (9.0%). The majority of women had a graduate or professional degree (60.2%) and identified as Christian (51.1%) as well as 38.8% were married. Most women were employed full-time as nonessential workers (44.1%), 24.1% were students, and almost half (48.5%) did not feel comfortable returning to work or school when the stay-at-home-orders due to COVID-19 were lifted. The most frequently reported monthly income before COVID-19 (43.7%) and currently (38.5%) was more than $4,000. However, almost 6% of women currently have no income, and 6% of women are receiving $500 or less a month.
Demographic Characteristics of Research Participants.
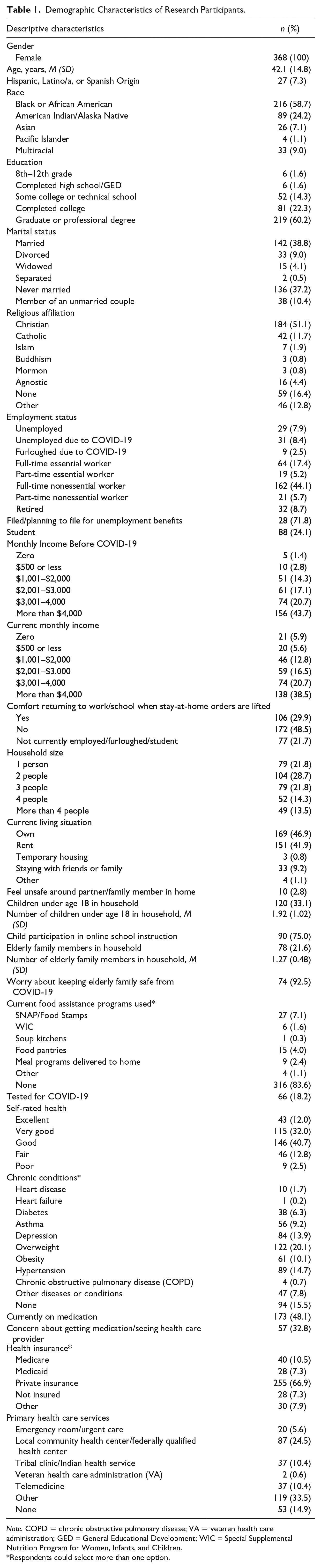
Note. COPD = chronic obstructive pulmonary disease; VA = veteran health care administration; GED = General Educational Development; WIC = Special Supplemental Nutrition Program for Women, Infants, and Children.
Respondents could select more than one option.
Nearly 3% of women indicated they feel unsafe around a partner or family member in their home. About 33% of women have children under the age of 18 living in the household, with an average of 1.92 (SD = 1.02) children. About 75% of these children are participating in online school instruction. Women are primarily utilizing the Supplemental Nutrition Assistance Program (SNAP) as their main source of food assistance during this time. Numerous women were tested for COVID-19 (18.2%), most rated their health as good (40.7%), and almost 14% were diagnosed with depression from a health care provider.
Characteristics of Study Measures
The characteristics of the five study measures included in the survey are displayed in Table 2. The mean score for the assessment of COVID-19 stressors was 4.06 (SD = 1.48), out of a possible range of 1 to 9. The BEPSI, which measured stress, yielded a mean score of 4.67 (SD = 2.68) before COVID-19, and an increased mean score of 5.31 (SD = 2.88) since COVID-19, out of a possible range of 0 to 10. In this instrument, the first question was not used for scoring but was adapted to elicit the current experience with stress and illness for women. This question asked, “Stress can allow us to become more ill (mental health, physical health, lack of sleep). Do you think anything like that is going on for you before COVID-19/since COVID-19?” Before COVID-19, 63.0% of women responded yes. Since COVID-19, this number increased to 69.3% of women who were feeling ill from the stress of COVID-19.
Characteristics of Study Measures.
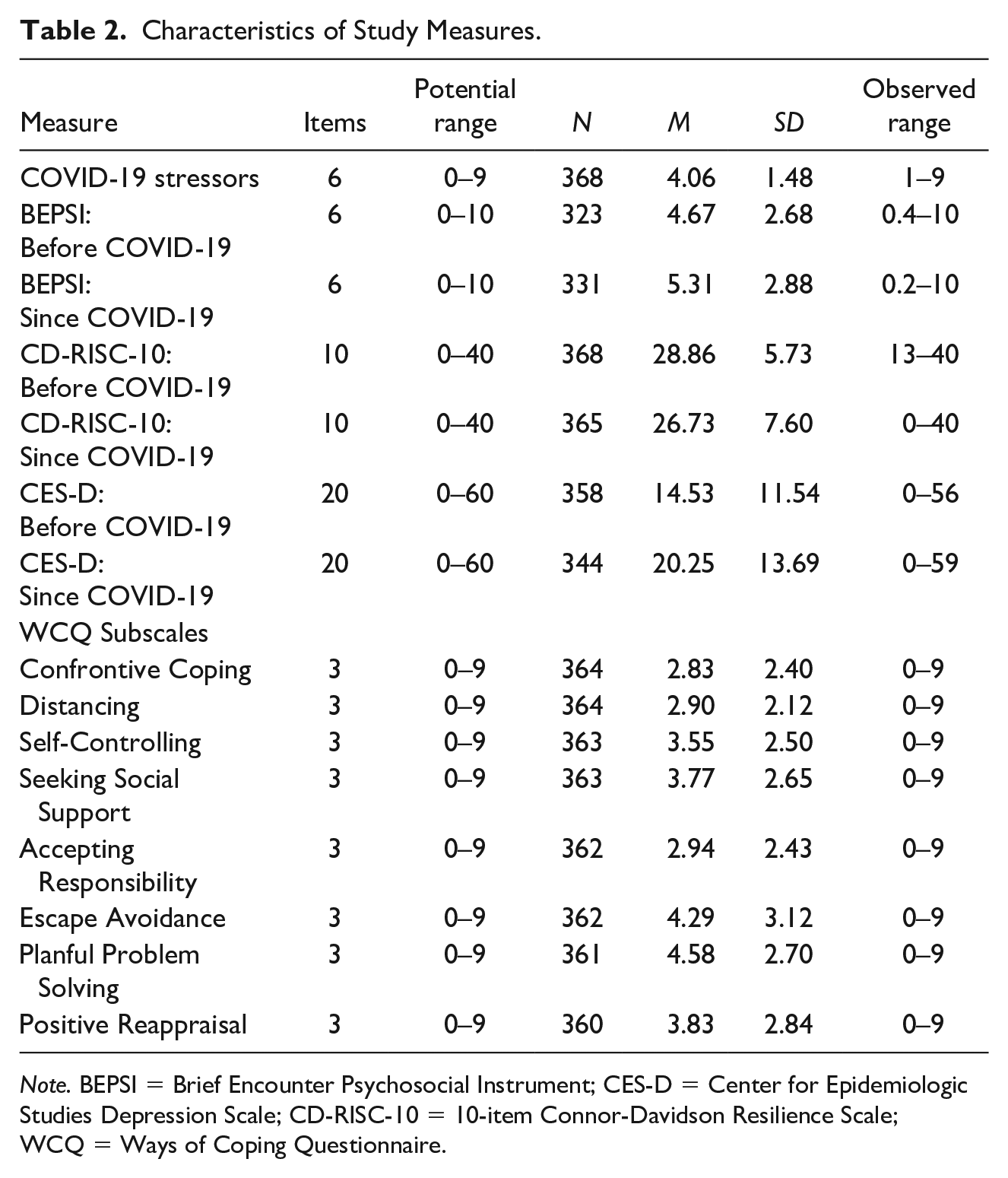
Note. BEPSI = Brief Encounter Psychosocial Instrument; CES-D = Center for Epidemiologic Studies Depression Scale; CD-RISC-10 = 10-item Connor-Davidson Resilience Scale; WCQ = Ways of Coping Questionnaire.
The CD-RISC-10, which measured resilience, generated a mean score of 28.86 (SD = 5.73) before COVID-19, and a decreased mean score of 26.73 (SD = 7.60) since COVID-19, out of a possible range of 0 to 40. The CES-D, which measured depressive symptoms, produced a mean score of 14.53 (SD = 11.54) before COVID-19, out of a possible range of 0 to 60. Since COVID-19, the mean score increased to 20.25 (SD = 13.69), which is indicative of depressive symptoms. Before COVID-19, 38.8% of women were considered depressed. However, with the onset of COVID-19, the number of women considered depressed increased to 59.0%.
Coping With the Stress of COVID-19
The mean scores of the eight WCQ coping scales are reported in Table 2. The three types of coping that were predominantly utilized by WOC to cope with the stress of COVID-19 were: (a) planful problem-solving (M = 4.58, SD = 2.70), (b) escape-avoidance (M = 4.29, SD = 3.12), and (c) positive reappraisal (M = 3.83, SD = 2.84).
Relationship Between COVID-19 Stressors and Depressive Symptoms
Pearson correlation was performed to determine the relationship between stressors related to COVID-19 (financial strain, food insecurity, lack of social support, and anxiety regarding COVID-19 news reports) and depressive symptoms. A small, positive correlation was found between COVID-19 stressors and depressive symptoms (r = 0.27, n = 344, p < .001). COVID-19 stressors help to explain 7.51% of the variance in depressive symptoms for WOC.
The Impact of Cognitive Appraisal on Coping Efforts
Multiple regressions were calculated to explore the impact of cognitive appraisal on the eight types of coping (Table 3). Cognitive appraisal includes primary appraisal, which was measured with stress, and secondary appraisal, which was measured with resilience. Primary appraisal had a significant impact on confrontive coping, B = .255, t(324) = 5.39, p < .001, distancing, B = .120, t(324) = 2.79, p = .006, self-controlling, B = .321, t(323) = 6.75, p < .001, seeking social support, B = .169, t(323) = 3.18, p = .002, accepting responsibility, B = .344, t(322) = 7.46, p < .001, escape-avoidance, B = .469, t(322) = 8.38, p < .001, and planful problem-solving, B = .111, t(321) = 2.10, p = .037. However, secondary appraisal had a significant impact on confrontive coping, B = .061, t(324) = 3.14, p = .002, seeking social support, B = .051, t(323) = 2.34, p = .020, planful problem-solving, B = .076, t(321) = 3.48, p = .001, and positive reappraisal, B = .091, t(321) = 3.94, p < .001.
Multiple Regression Analyses Exploring the Impact of Cognitive Appraisal on the Eight Types of Coping.
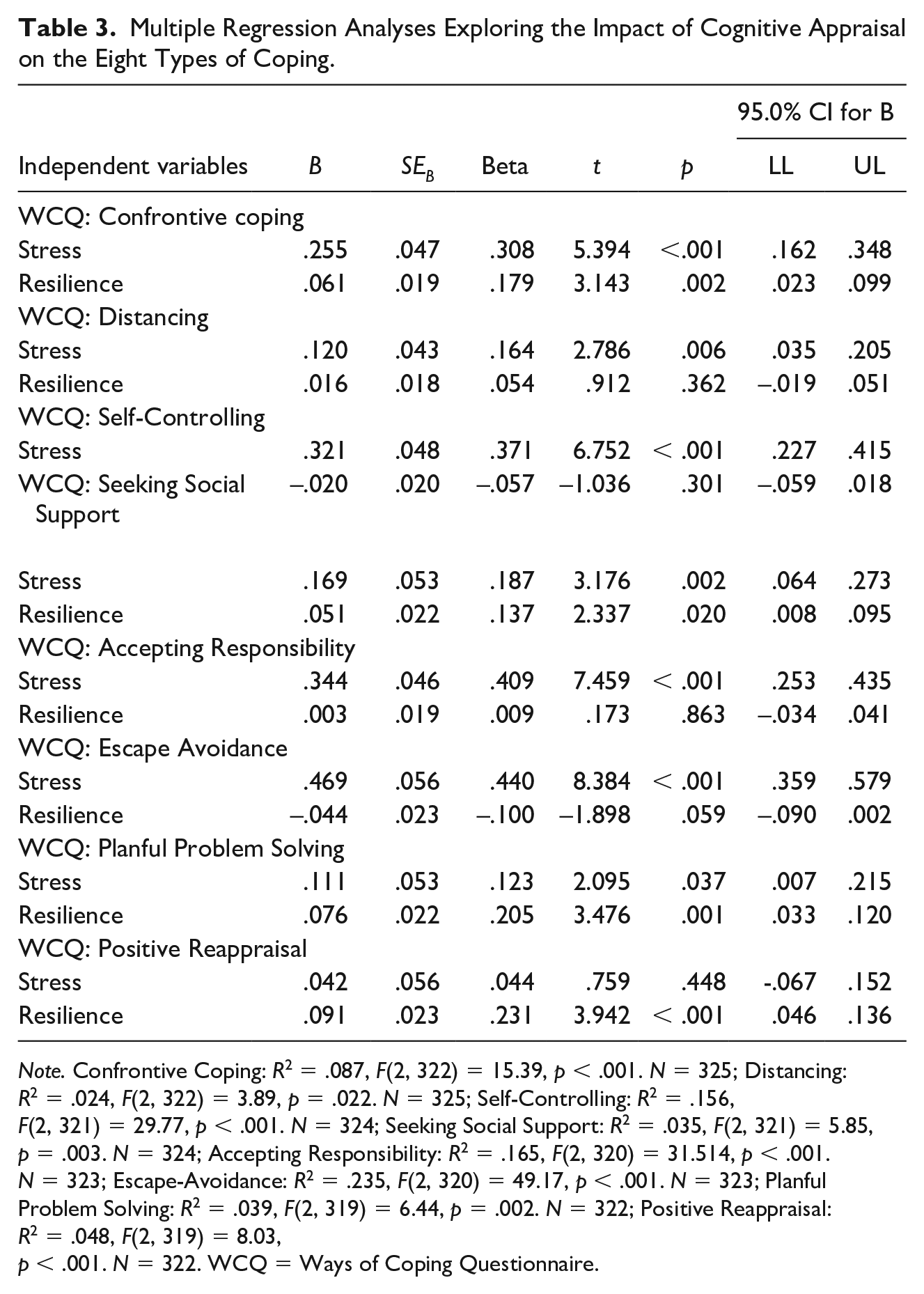
Note. Confrontive Coping: R2 = .087, F(2, 322) = 15.39, p < .001. N = 325; Distancing: R2 = .024, F(2, 322) = 3.89, p = .022. N = 325; Self-Controlling: R2 = .156, F(2, 321) = 29.77, p < .001. N = 324; Seeking Social Support: R2 = .035, F(2, 321) = 5.85, p = .003. N = 324; Accepting Responsibility: R2 = .165, F(2, 320) = 31.514, p < .001. N = 323; Escape-Avoidance: R2 = .235, F(2, 320) = 49.17, p < .001. N = 323; Planful Problem Solving: R2 = .039, F(2, 319) = 6.44, p = .002. N = 322; Positive Reappraisal: R2 = .048, F(2, 319) = 8.03, p < .001. N = 322. WCQ = Ways of Coping Questionnaire.
The Impact of COVID-19 on Stress, Resilience, and Depressive Symptoms
Paired samples t-tests were conducted to evaluate stress, resilience, and depressive symptoms before and since COVID-19. A statistically significant increase was found in BEPSI scores (stress) from before COVID-19 (M = 4.77, SD = 2.63) to since COVID-19 (M = 5.30, SD = 2.86), t (311) = −4.54, p < .001 (two-tailed). The mean increase in BEPSI scores was 0.53 with a 95% CI ranging from −0.76 to −0.30.
A statistically significant decrease was found in CD-RISC-10 scores (resilience) from before COVID-19 (M = 28.90, SD = 5.71) to since COVID-19 (M = 26.73, SD = 7.60), t (364) = 6.85, p < .001 (two-tailed). The mean decrease in CD-RISC-10 scores was 2.17 with a 95% CI ranging from 1.54 to 2.79.
Finally, a statistically significant increase was found in CES-D scores (depressive symptoms) from before COVID-19 (M = 14.28, SD = 11.56) to since COVID-19 (M = 20.18, SD = 13.73), t (340) = −10.14, p < .001 (two-tailed). The mean increase in CES-D scores was 5.90 with a 95% CI ranging from −7.05 to −4.76.
Discussion
The purpose of this study was to identify processes of coping with COVID-19 and determine their impact on emotional well-being for WOC in the United States. In this investigation, we discovered that WOC primarily utilize planful problem solving, which is intentional problem-focused efforts to cope with the stress of COVID-19. This type of coping is reflective of the multiple roles that women endure and juggle, which results in significant physical and mental health demands (Pearson Quinn, 2008) that are exacerbated during the COVID-19 pandemic as a woman of color. The second most used coping process for WOC was escape-avoidance, which consists of wishful thinking and behavioral efforts to avoid the stress of COVID-19. Positive reappraisal, a coping process that creates positive meaning by focusing on personal growth and religion, was the third most used coping process for WOC. Nearly 84% of women in the study identified a religious affiliation, which suggests that they may be using their religion to cope with the stress of COVID-19.
A small, statistically significant relationship between stressors related to COVID-19 and depressive symptoms was determined. COVID-19 stressors, which included financial strain, food insecurity, lack of social support, and anxiety regarding COVID-19 news reports, only explained about 8% of the variance in depressive symptoms for WOC in the United States. This result was observed in the low mean score for COVID-19 stressors, which can be attributed to our highly educated sample, where 60.2% of women attained a graduate or professional degree, and 61.5% were currently employed full-time. Although a small relationship exists, a significant one still exists and may last for years to come. Tracy et al. (2011) found that after large-scale disasters, such as the COVID-19 pandemic, strong correlations were found with worsening mental health conditions both immediately and for many years following.
In alignment with the TMSC, this study explored the impact that cognitive (primary and secondary) appraisal had on coping efforts. Primary appraisal is the woman’s evaluation of the significance of COVID-19 for her well-being. Secondary appraisal is the woman’s assessment of coping resources and options for dealing with COVID-19. Primary and secondary appraisal converged to have a significant impact on confrontive coping, seeking social support, and planful problem-solving. This research discovered that stress as well as resilience influenced aggressive efforts to change the situation; efforts to seek informational, physical, and emotional support; and intentional problem-focused efforts to change the situation. This finding is consistent with Folkman, Lazarus, Dunkel-Schetter, DeLongis, and Gruen (1986), who argue that primary and secondary appraisals converge to determine whether the person-environment transaction is perceived as significant for well-being and in what manner.
The COVID-19 pandemic has had deleterious effects on psychosocial factors such as stress, resilience, and depressive symptoms for WOC in the United States. Stress and depression significantly increased for WOC since COVID-19 occurred. This finding is consistent with Matud (2004), who found that women perceive life events as more stressful and more negative due to a higher level of chronic stress and minor daily stressors that they endure. In addition, resilience, the ability to face adversity and bounce back from stress, significantly decreased for WOC as a result of COVID-19. Similarly, Giarratano et al. (2020) found that pregnant women living in postdisaster communities needed to devise new methods of resilience as a result of increased stress in their lives years after the event.
Although this study is among the early work to illustrate stress and coping experiences with COVID-19 for WOC in the United States, a few limitations should be noted. Since we disseminated our survey instrument online, our results are limited to women with internet access. In addition, the assessment of COVID-19 stressors did not fully capture the stressful experiences with COVID-19 for WOC in this study. Since the majority of women were highly educated and employed, the income-related and social support stressors that we identified did not apply to this group. Finally, we did not have an expansive socioeconomic distribution in the sample, as most of the women were educated and employed, thereby limiting our results to the experiences of WOC with a higher socioeconomic status.
Implications for Practice and/or Policy
These results have implications for clinicians, such as social workers, mental health providers, and physicians, as well as public health professionals. Almost half (48.5%) of the women in the study did not feel comfortable returning to work or school, which adds another layer of complexity to a myriad of informal and formal structures needed to address stress and coping within the COVID-19 pandemic. Furthermore, these results revealed that although these women were highly educated and employed, they still experienced a significant increase in stress and depressive symptoms as well as a decrease in resilience. It appears that racial inequities still persist for WOC with a high socioeconomic status and adversely impacts psychosocial factors in this population. Understanding how WOC are coping with the stress of COVID-19 can help public health professionals and clinicians to provide tailored, culturally appropriate, equitable, and gender-specific care for this population in the United States. These results can inform the current standard of practice, as well as future major crisis response, as many health care delivery systems and social service orgnizations will need to adapt their services to address this increased mental health need due to the pandemic.
Furthermore, the TMSC was an effective theoretical framework to understand how WOC are coping with the stress of COVID-19. This framework provided a snapshot of how these women assessed the stressors related to COVID-19 in their lives, how they evaluated the significance of COVID-19 for their well-being, and how resilient they felt in the face of this pandemic. In addition, the TMSC provided an overview of how this population coped with the stress of COVID-19 as well as how the pandemic impacted their mental health. Therefore, this model can be applied for future pandemic or major crisis response as it reveals an in-depth understanding of an individual’s cognitive and behavioral processes to manage and cope with a stressful event.
Conclusion
This study identified processes of coping with COVID-19 and determined their impact on emotional well-being for WOC in the United States. As a result of this public health crisis, stress and depressive symptoms for this population have significantly increased, and resilience has significantly decreased. In addition, stressors specific to COVID-19 were correlated with depressive symptoms for this population. WOC coped with the stress of the pandemic by utilizing intentional problem-focused efforts to change the situation, wishful thinking and behavioral efforts to avoid the situation, and created positive meaning by focusing on personal growth and religion. The appraisal of stress and resilience also influenced the types of coping that WOC used. These results can be translated into actionable care plans for clinicians that inform the development of tailored, culturally appropriate, and gender-specific mental health care for WOC in the age of COVID-19. In addition, these results provide a foundation for a federal response, such as FEMA, to understand the stressors that people are experiencing during a pandemic and how they are coping with it. This response can then be tailored for targeted communities such as WOC in the United States.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.