
Abstract
This article uses longitudinal data to measure the effects of ill health and informal care roles on the employment chances of mid-life women, and to examine how these effects are mediated by workplace characteristics. We find that women in jobs with lower skills/status encounter the greatest difficulty in finding accommodations for changes in their health and informal care roles. We identify an important role for paid sick leave and holiday leave in boosting employment retention. However, we find that the positive employment effects of permanent contracts do not extend to women experiencing increased informal care roles. Additionally, we do not identify a positive link between employment retention and flexible working time arrangements. However, we do establish a link between a preference for reduced working hours and employment cessation, suggesting that some women experience problems in achieving flexible working hours and that this causes some of them to leave work altogether. We argue that these findings are relevant to the design of policy initiatives aimed at lifting rates of workforce participation as part of the response to population ageing.
Introduction
Increased workforce participation of mid-life people is a common target for policy on population ageing (Treasury, 2010: xiv). Removing the barriers to the employment of mid-life women is particularly important because this demographic group currently has a relatively low rate of workforce participation. Furthermore, it is a demographic group that will grow at a very fast rate in coming years (Organisation for Economic Co-operation and Development (OECD), 2006). 1 However, until recently, the group has been poorly represented in studies of the workforce participation of mid-life people. As Currie and Madrian (1999: 353) noted in 1999: ‘a glaring limitation of the existing literature is the intense focus on elderly white men, to the virtual exclusion of most other groups’. Hank (2004: 190) made a similar observation in 2004, commenting that ‘we know only relatively little about the work and retirement patterns of mothers in their later years’.
The current article aims to help address the relative invisibility of women in analyses of ‘older’ worker employment by reporting new measures of the effects of ill health and informal care roles on the employment chances of Australian mid-life women (aged 45 to 69). However, the article’s key contribution to the extant literature on mid-life workers is the results it presents on how women’s workplace context and conditions of employment influence the employment impacts of ill health and informal care. We examine how these impacts are mediated by the occupational status of the worker, her access to paid holiday and sick leave, her working hours and shift patterns, and her ability to alter her start and finish times at work each day. The results of the investigation have direct relevance for the design of policy and other initiatives aimed at boosting the workforce participation rates of mid-life women.
The employment impacts of informal care roles and ill health have been a focus of several previous studies of mid-life women’s employment. This reflects, first, the prevalence of informal care work in this demographic group (as noted by Drago et al., 2007) and the group’s relatively high rates of ill health. For example, in Australia in 2009, the median age of informal carers was 53 years old and the rate of ill health (at 18%) was 64% higher among mid-life people than among those aged 25–44. 2
Most studies of the issue indicate that ill health adversely affects the employment chances of mid-life women. For example, Austen and Ong (2010) identified that the employment rate of women aged 40 to 64 was 50% lower among women with ‘poor’ as compared to ‘good to excellent’ health. They also identified that women in this age group whose health declined were more likely than other women to transition out of paid employment. These findings corroborated the results of a European study by Hasselhorn et al. (2005), which identified a ‘healthy worker effect’ on the employment rates of ‘older’ European nurses.
Large measured effects of health on mid-life women’s employment chances have also been reported in a range of studies that did not focus specifically on this demographic group (see e.g. Cai and Kalb, 2006; Jimenez-Martin et al., 2006). Generally, empirical studies of older workers’ employment find that health status is the most important determinant of labour market transitions, with the health effects on employment exceeding the impacts of financial incentives and other factors (Blau and Gilleskie, 2001).
Studies of the impacts of informal care roles also indicate adverse effects on employment chances. Berecki-Gisolf et al. (2008) found that women aged in their 50s who took up a role caring for an ill, frail or disabled person had lower rates of labour force participation than other mid-life Australian women. International studies that have focused on mid-life women have reached similar conclusions (Bolin et al., 2008; Hank, 2004; Pavalko and Artis, 1997; Spiess and Schneider, 2003; Wakabayashi and Donato, 2005), corroborating the results of investigations into the employment effects of informal care across all demographic groups (Carmichael and Charles, 1998; Henz, 2004; Larsen, 2010; Leigh, 2010; McLanahan and Monson, 1990; Mann et al., 2011). However, the employment impacts of care roles have typically been found to be greater in a cross-sectional than longitudinal perspective, 3 and at least one study of the issue (by Wolf and Soldo, 1994) found no effect of informal care on employment or hours worked.
A common recommendation of studies of the employment effects of ill health and informal care is for policy action on work environments. Flexible and/or shorter work hours, access to respite care, and improvements in workers’ ability to take time off from paid work are typical suggestions for lessening the employment impacts of these life events (see Berecki et al., 2007; Carney, 2009; Larsen, 2010).
However, to date, there has been little research on how aspects of the workplace context and conditions of employment influence the employment effects of ill health and informal care roles for mid-life women. Furthermore, across all groups of women, the influence of work environments on the employment effects of ill health and informal care has not been studied in a comprehensive fashion. Rather, different studies have identified possible relationships between these effects and specific employment conditions. For example, Scharlach et al. (1991) identified a link between job flexibility (specifically, the ability to vary work routine) and the impact of informal care roles on paid work participation. Gottlieb et al. (1994) found that carers who were working unusual hours or had variable shifts experienced greater difficulty combining paid work and care roles. Drago et al. (2007) and Henz (2004) both identified full-time workers as experiencing greater difficulties in scaling back their paid work hours than their part-time counterparts. Henz (2004) also found differences in the employment impacts of care roles between low- and high-status occupational groups. Lewis (1997) identified a link between access to sick leave and the employment effects of informal care. Bartley and Owen (1996) and Bradley et al. (2005) also identified occupational differences in relation to the effects of breast cancer on the employment outcomes of women. The findings of a number of studies have indicated an association between education and the employment impacts of health and informal care (Carmichael et al., 2008; Han and Moen, 1999; McDonough and Amick, 2001).
The current study investigates how the employment impacts of both ill health and informal care roles are mediated by specific employment conditions. Using data from nine waves of the Household, Income and Labour Dynamics in Australia (HILDA) survey (spanning 2001 to 2009), data is provided on: the characteristics of mid-life women in paid work; their transitions out of paid work; the impact of changing health and informal care roles on these transitions; and how these impacts are mediated by occupational status, access to paid holiday and sick leave, working hours, shift patterns, and flexible start and finish times.
Data and methods
The conceptual framework for this study is one where workers’ chances of retaining their employment is affected: first, by their accumulated human capital via their education, labour market experience and language skills; second, by possible constraints on their ability and/or willingness to engage in paid work, linked to their health, age and informal care commitments; and third, by current labour market conditions, linked to the business cycle at a particular point in time and location. The framework is one where the relationships between, for example, health and informal care roles and employment retention can vary with workplace context and the conditions of employment. In this study, characteristics such as working time arrangements (including shift patterns), entitlements to sick leave and other forms of leave are of particular interest. By adopting this conceptual framework, we can examine the potential importance of specific employment conditions on the employment decisions of mid-life women who experience changes in their individual health and caring circumstances.
The data have been sourced from the HILDA survey. The HILDA survey began in 2001 with a probability-based sample of Australian households. From 7682 households, 13,969 individuals aged 15 and over were interviewed face to face or via a phone conversation in the first wave of the survey. 4 In this group, there were 2416 mid-life women (aged 45 to 69 5 ). Since its inception, a further eight waves of survey data have been collected, one in each year since 2001. The result is a large longitudinal database that contains information on the labour market characteristics of the survey respondents, including their labour force status in each year, hours of work and, where appropriate, the characteristics of their work environment, such as the nature of work undertaken, the hours of work performed and the type of employment contract used. Also included are data on the respondents’ ages, co-residents (such as partners), human capital (such as education and labour market experience), year and place of residence (to proxy current labour market conditions), health and informal care roles.
HILDA’s data on health and informal care roles come from responses to questions on a self-completion questionnaire. One of these questions asks: ‘In general, would you say your health is excellent, very good, good, fair or poor?’ In our analysis of this data, we distinguish between women who rated their health as excellent, very good or good and those who rated it as fair or poor. 6 We use the responses to another question on the self-completion questionnaire to measure recent changes in health. This question asks whether a health condition had developed in the last year, or if health was worse than a year ago. Informal care roles, other than those associated with child care, are gauged from responses to a question that asks how much time the respondent spends caring for a disabled spouse, disabled adult relative or an elderly parent or parent-in-law. The measure, based as it is on weekly hours of care, can be used to provide an indication of changing care responsibilities. Using a time-based measure has a further advantage of allowing us to examine the impact of low versus high care responsibilities, and of small versus large changes in hours of care over time. We distinguish between women undertaking less than seven hours of informal care work each week (one hour per day) and those undertaking more than seven hours of informal care. We examine changes in informal care roles by identifying women who reported that their care hours had increased by more than five hours per week over the previous 12 months.
The interrogation of the HILDA data follows a number of steps. Initially, we use the cross-section of data relating to the period when the women were first interviewed to compare the education, experience, language, health, care and other characteristics of employed and non-employed mid-life women. A cross-sectional probit regression model is then estimated using this data to generate measures of the correlations between employment probability and ill health and informal care roles, respectively, controlling for the influence of the other factors in our conceptual model. It also performs the important function of generating a variable that corrects for selection bias in the subsequent longitudinal analysis of the data described later.
To take account of the likelihood that the cross-sectional approach will exaggerate the impact of informal care on employment because it relies on a comparison of the employment rates of two different groups, carers and non-carers, the next part of our analysis makes use of the longitudinal dimensions of the HILDA data. We apply a random effects probit regression model applied to pooled data from nine waves of the HILDA data to measure the effect of deteriorating health and increased informal care roles on the probability that a mid-life woman who is in paid work in wave t will retain this involvement through to the next survey period (wave t + 1). 7 The random effects specification enables us to make inferences about the population of mid-life women from which our sample was drawn (Rabe-Hesketh and Skrondal, 2008). The alternative, fixed effects specification is computationally difficult (see Wooldridge, 2002) and, in any case, would have limited our interpretation of findings to within-person effects, with the consequence that we would not have been able to account for the initial conditions (selection) problem noted earlier.
In the final stage of our data analysis, we focus on how the employment effects of ill health and informal care roles vary with the work environments of different mid-life women. To achieve this, we apply random effects probit models to subsamples of mid-life women, defined by their workplace characteristics. The results from this stage of the analysis show how the employment impacts of ill health and informal care are influenced by women’s occupational status, their access to paid sick and holiday leave, their working time patterns, and their ability to alter their start and finishing times.
Comparing the health and care characteristics of mid-life women and their employment transitions
Characteristics of sample: Person observations on mid-life Australian women aged 45–69 years, 2001–2008, by employment transition at initial observation.

The statistics shown in Table 1 indicate partial correlations between employment, employment retention and a mid-life woman’s age, health and informal care roles. For example, the proportion of women reporting good, very good or excellent health was highest (at 90.7%) in the group of women who retained employment and lowest (at 68.8%) in the group of women who were not employed in the study period. Informal care hours were higher for women who stayed out of paid work; 10.7% of this group spent more than seven hours each week on informal care, compared to 4.6% of the group who remained employed.
Estimated marginal effects on initial employment probability: Australian women, aged 45–69 years, 2001–2008.
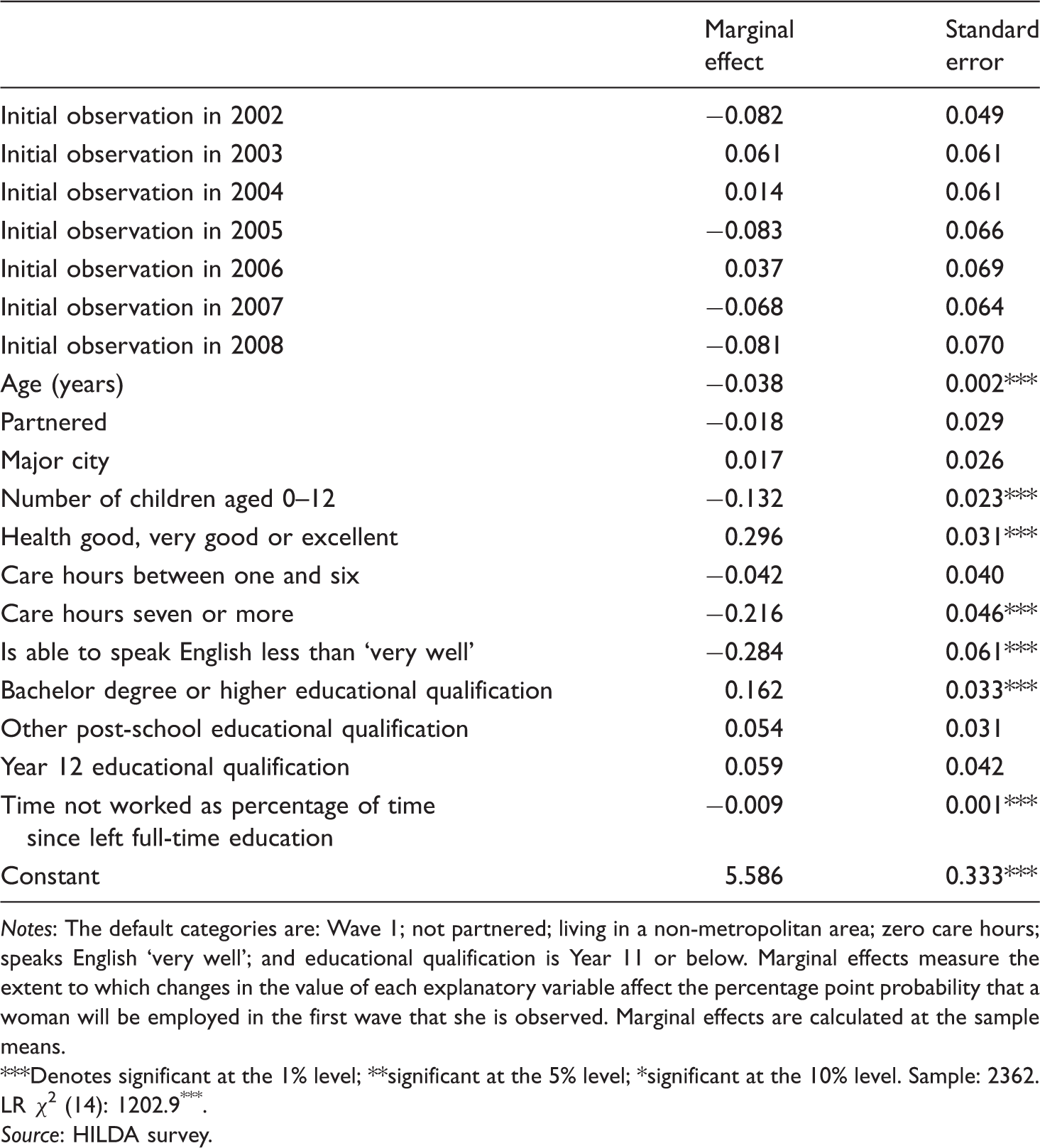
Notes: The default categories are: Wave 1; not partnered; living in a non-metropolitan area; zero care hours; speaks English ‘very well’; and educational qualification is Year 11 or below. Marginal effects measure the extent to which changes in the value of each explanatory variable affect the percentage point probability that a woman will be employed in the first wave that she is observed. Marginal effects are calculated at the sample means. ***Denotes significant at the 1% level; **significant at the 5% level; *significant at the 10% level. Sample: 2362. LR χ2 (14): 1202.9***.
Source: HILDA survey.
Although the data in Tables 1 and 2 are informative of the patterns of employment associated with ill health and informal care work, being based on cross-sectional data they leave open important questions about the nature of the causal relationships. As Carmichael et al. (2008: 8–9) explain, for example, the lower employment rates of informal carers can indicate either that when people undertake care ‘their extra commitments make it more difficult to find or maintain work’ or that ‘people with these labour market characteristics are more likely to undertake care in the first place’. Longitudinal data helps to address these problems by enabling investigation of the relationship between employment retention and prior changes in health and informal care roles. However, the use of longitudinal data creates its own problems. The first is tractable: the women included in the study are already employed, and thus have a set of health, informal care, human capital and other characteristics that set them apart from other mid-life women. If left uncorrected, this sample selection problem will bias the estimated relationships between, for example, changing care roles and employment across the population as a whole. However, as we demonstrate, the problem can be resolved by using the results of the initial probit model (reflected in Table 2) to calculate a generalised residual, which is then included as a regressor in the employment transition model (Heckman, 2000).
The second problem with longitudinal analysis is less easily solved as it derives from the relatively small number of employment transitions available to study even in data sets as large as HILDA. This limits the ability to achieve adequate power in the statistical analysis and, thus, the confidence that can be attached to the nature and magnitude of relationships. Importantly, as we point out later in the article, this data limitation also restricts analysis of complex relationships (such as those involving interactions between variables associated with the employment effects of ill health and informal care).
Estimated marginal effects on the probability of retaining employment: Mid-life Australian women, 2001–2008.

Notes: The log variance is the panel-level variance component. Rho is the proportion of the total variance contributed by the panel-level variance component. The default categories are: Wave 1 (2001); aged 45 to 49; remained single; living in a non-metropolitan area; health remained unchanged; initial care hours zero; care hours changed by less than five hours; speaks English ‘very well’; initial occupation is elementary or labourer; initial working time arrangement is casual, part-time; desired same working hours; and partner remained employed. Marginal effects measure the extent to which changes in the value of each explanatory variable affect the percentage point probability that a woman will retain employment between waves t and t+1. Marginal effects are calculated at the sample means. ***Denotes significant at the 1% level; **significant at the 5% level; *significant at the 10% level.
Source: HILDA survey.
The data in the table indicate that deterioration in health has detrimental effects on a mid-life woman’s chances of retaining employment. Mid-life women who developed a health condition are 4.1 percentage points less likely to remain in paid employment than other women in the following year. The data also indicate that increases in informal care hours of more than five hours per week reduce the chances of employment retention by 6.5 percentage points. Additional comments on the data in the table are made in the following section.
Characteristics of the work environment and the employment retention of mid-life women
The results in Table 3 show that several aspects of the work environment influence the chances of mid-life women being retained in employment. The probability of employment retention is higher – by 2.5 percentage points – for women working in managerial and professional, as compared to elementary clerical or labouring, occupational roles. Women who work full-time and on contracts that give them entitlements to holiday and sick leave are also more likely to retain employment than other women. The probability of employment retention is lowest for women on a casual contract (which typically includes no paid holiday or sick leave entitlements) and working part-time hours. Compared to women on permanent part-time contracts, their employment retention probability is 3.1 percentage points lower. Compared to women on permanent full-time contracts, it is lower by 6.5 percentage points.
The remainder of this section focuses on the relationship between work environment factors and the impact of ill health and increased informal care roles on the employment retention chances of mid-life women. The examination makes use of the same regression model used to generate the results in Table 3. However, we apply this model to different subsamples to identify how the effects of ill health and increased informal care roles vary between women in different working environments. The use of subsamples is necessary due to, as yet, unsolved problems with the incorporation of multiple interaction terms in non-linear regression models (Ai and Norton, 2003; Norton et al., 2004).
Estimated marginal effects of ill health and increased informal care hours on the probability of retaining employment: Subgroups of mid-life Australian women, 2001–2008.

Notes: The data in this table are the marginal effects of ill health and changing care roles as measured in a random effects probit regression model of employment retention, with the full set of controls for year, demographics and so on as set out in Table 3. The default categories are: health remained unchanged; and care hours changed by less than five hours. Marginal effects measure the extent to which changes in the value of each explanatory variable affect the percentage point probability that a woman will be employed when she is first observed in the sample. Marginal effects are calculated at the sample means. ***Denotes significant at the 1% level; **significant at the 5% level; *significant at the 10% level.
Source: HILDA survey.
In accordance with the general pattern identified in Table 3, permanent employment contracts improve the chances of employment retention by women experiencing ill health. In the group of women employed on permanent contracts, deterioration in health is associated with a small magnitude (2.4 percentage point) change in employment retention probability. In contrast, in the group of women employed on casual contracts, worsening health status reduces the probability of employment by a relatively large amount (7.8 percentage points).
However, a different pattern applies in relation to the effects of increased informal care roles. The data in Table 4 show that the effects of these changes are relatively large for mid-life women employed on permanent contracts (reducing the probability of employment retention by 7.8 percentage points). The effect of increased care hours on the employment retention probability of women employed on casual contracts is much smaller in magnitude (2.0 percentage points) and not statistically significant in this group.
The data in Table 4 suggest that working hours arrangements do not have a substantial impact on the employment effects of ill health and increased informal care roles. Within each subgroup, the measured impacts of ill health are similar in magnitude (3.1 percentage points for full-time workers and 4.4 percentage points for part-time workers). Likewise, the magnitude of the employment effect of increased care roles is similar for women working full-time and part-time hours (6.3 and 6.9 percentage points, respectively).
In contrast, the data in Table 4 indicate that higher occupational status reduces the employment effects of ill health and increased informal care roles. In the group of managers and professionals, deterioration in health is associated with a smaller magnitude (3.5 percentage point) change in employment retention probability than is apparent among other women (a 4.2 percentage point impact). The effects of increased informal care hours are also smaller (by 1.5 percentage points) in the group of managers and professionals, as compared to other working women.
Day work is associated with slightly higher employment impacts from ill health (reducing the probability of employment retention by 4.1 percentage points, as compared to 3.4 percentage points for women working night shifts). However, the adverse impacts of increased care roles on employment are of greater magnitude in the group of women who work night shifts (8.5 versus 5.7 percentage points, respectively). The relationships follow a similar pattern when the comparison is between women who have flexible start and finish times at work and those who do not. That is, the magnitude of the impact of ill health is highest in the group who have flexible work conditions (4.8 as compared to 3.5 percentage points, respectively). However, the impact of increased informal care roles is lower for this group (4.8 versus 7.1 percentage points, respectively).
Discussion and conclusion
The results presented in this article contribute new data on workforce participation by mid-life women. They comprise new measures of the employment effects of ill health and informal care roles, derived from a large and comprehensive longitudinal data set. The results also include novel estimates of the mediating effects of different workplace characteristics on the employment impacts of ill health and informal care roles. This information is relevant to the design of policy initiatives aimed at lifting rates of workforce participation as part of the response to population ageing. It provides governments and employers with insights into the types of workplace reforms that are likely to be positive for workforce participation, and which will help reduce the impacts on mid-life women when they experience ill health or undertake informal care responsibilities.
The findings of this article are, first, that both ill health and informal care work impede the workforce participation of affected mid-life women, which is in concordance with the predictions of a conceptual model that emphasises the importance of labour market opportunities and costs to employment retention. We identify these effects both cross-sectionally (comparing employment retention rates of affected and non-affected women) and longitudinally (examining how the experience of ill health or increased informal care work affects the chances of employment retention). As such, our results add to a growing body of evidence showing that ill health and informal care roles are important determinants of mid-life women’s ability to remain engaged in paid work.
Our study also identifies how the retention of mid-life women in employment is influenced by their workplace environment, indicating that these factors are important ‘extensions’ to basic models of employment determination. First, we identify occupational differences in employment retention favouring women in high-status occupations. These are likely to reflect the greater labour market opportunities of highly-skilled workers, linked to the incentive that firms have to retain their highly-skilled workers, as well as the incentive that exists for women in high-skill/-status jobs to extend their paid working life. The results also suggest that skill levels (reflected in occupation) affect the influence of ill health and informal care on employment retention. We find that women in jobs with lower skills/status are least able to find accommodations in their paid work roles for changes in their health and informal care roles. Thus, they are likely to face relatively high penalties for these life circumstances. The implication for policy is that interventions aimed at minimising the employment impacts of ill health and informal care roles should be focused on low-skill/-status jobs.
Second, we find strong evidence of differences in employment retention between mid-life women employed on full-time permanent contracts, as compared to those on casual part-time contracts. Our data generally indicate that access to paid sick leave and holiday leave promotes employment retention, which suggests that extending these entitlements to all workers could boost the rate of workforce participation.
However, our evidence also shows that the relationships between work environment characteristics and employment retention are complex, with implications for ongoing efforts in research and policy on ageing workforces. For example, we find that the positive employment effects of permanent contracts only apply to women experiencing ill health. Women on permanent contracts are more likely to leave paid work following an increase in informal care roles than their counterparts who are casually employed. Thus, while we produce evidence of the positive effects of leave entitlements on workers’ ability to manage ill health (consistent with our conceptual framework), we do not find evidence of similar effects in the case of informal care roles. This could reflect the limited leave entitlements to support informal care roles in permanent contracts. It could also indicate that women on casual contracts have a greater ability to change jobs or their hours of work – to preserve their employment when informal care hours increase – than do their counterparts on permanent contracts. Further research, with access to a larger sample, is required to test this hypothesis.
The complexity of the relationships between work environment characteristics and employment retention is also apparent in our finding that part-time work, per se, does not promote employment retention. We also find little evidence of a general link between employment retention and both day work and flexible start and finish times. At face value, these findings would appear to conflict with the predictions of our conceptual model, which suggests that to the degree that these factors assist workers to manage episodes of ill health and informal care roles, they will promote employment retention. However, it is noteworthy that another of our findings is that women who expressed a preference for fewer hours in the initial survey wave were more likely to leave paid employment than women who were satisfied with their hours. This suggests that some women experience problems in accessing part-time work (or reducing their hours of work in other ways) and that the lack of this type of flexibility can cause them to leave work altogether. For policy, the finding suggests another possible mechanism for positively influencing the employment rates of mid-life women, namely, improving their ability to alter their working hours within the context of their current employment contracts.
Footnotes
Funding
This work was supported by the Australian Research Council Discovery Program (grant DP110102728).
Acknowledgements
This article uses unit record data from the Household, Income and Labour Dynamics in Australia (HILDA) Survey. The HILDA Project was initiated and is funded by the Australian Government Department of Families, Housing, Community Services and Indigenous Affairs (FaHCSIA) and is managed by the Melbourne Institute of Applied Economic and Social Research (MIAESR). The findings and views reported in this article, however, are those of the authors and should not be attributed to either FaHCSIA or the MIAESR.