
Abstract
This article uses data from a panel of Australian mature-age women to examine the effects of care roles on workers’ intentions to leave their jobs. We focus on how the employment effects of care roles can be shaped by the economic circumstances of the worker. We find that caring for an ill, frail or disabled family member has significantly lower effects on the turnover intentions of mature-age women with ‘poor’ (as compared to favourable) economic circumstances. We interpret this pattern as reflecting the financial costs associated with the provisioning of these types of family care needs.
Introduction
The need to combine informal care roles with paid work commitments will grow rapidly in the immediate and medium-term future. Population ageing is associated with an increase in the number of people with long-term health conditions and the number of Australians living with dementia will almost treble by 2050 (Australian Institute of Health and Welfare (AIHW), 2012). Similar trends have been documented in other countries (Calvano, 2013; Kotsadam, 2011). These trends are increasing pressure on the formal care sector and, due to shifts from institutional care to community care, also increasing the importance of informal care (Tolhurst, 2001). Women (as wives and daughters of those in need of care) are usually the main source of informal care for people who have a long-term health condition, are frail or aged (Australian Bureau of Statistics (ABS), 2013). Increasingly, these care roles are performed by mid-life women who are active in the paid workforce (ABS, 2009; Calvano, 2013; Carmichael et al., 2010).
The context of population ageing emphasizes the need for research on the effects of informal care roles on the employment decisions of mature-age women. In this study we address the question of whether the economic circumstances of a woman’s household affects her employment decision-making when informal care needs arise. The question has thus far been neglected in the literature on the employment effects of informal care needs. As outlined in the next section, most research on the employment effects of informal care roles has focused on the time demands of informal care roles. This approach has often been guided by a human capital model that focuses on how informal care roles increase the direct and opportunity costs of time spent in paid work and, thus, on how these roles act as a disincentive to participate in paid work (see Schneider et al., 2012). However, this approach tends to neglect the financial costs that can be associated, for example, with the specialized medical services needed for ill, disabled or elderly family members, or the educational needs of children.
1
That is, as Charusheela (2003: 292) notes, the approach has tended to emphasise the contexts that pull rather than push women into paid work. In doing so, it has tended to neglect how labour market experience is shaped by a woman’s class background: … once we recognise that increased dependence on marketised products … may expel workers out of the household and into the marketplace in order to ensure that minimum levels of survival are met, we begin to get a very different image of the experience of work and of labour-market entry for women from different class backgrounds.
In this study we utilize a model of household production to guide an empirical analysis of the effects of informal care roles on employment decision-making using cross-sectional and longitudinal data from the Australian Mature Age Women in Aged Care (MAWAC) survey, conducted in 2011–2012. We use the MAWAC data to examine these relationships by focusing on how mature-age women workers’ intentions about leaving their paid work roles are affected by informal care roles, and how this relationship varies between those living in households characterized by good, as compared to strained, economic circumstances.
The final section of the paper discusses the implications of our findings for policy and research. We highlight how the reliance on the human capital model has tended to neglect the importance of women’s economic situation as a constraint on their ability to reduce their paid work hours in the presence of higher informal care roles. Unfortunately, this has also resulted in a relative neglect of the financial pressures associated with informal care roles. We argue the importance of policy designed to respond to the needs of women who have informal care roles and are struggling to maintain their paid work roles.
Literature review
As Leigh (2010) observes, a substantial body of empirical literature examines the employment effects of informal care roles. Several studies have examined this issue across all demographic groups and have identified a negative relationship between informal care roles (commonly measured by a binary variable) and both workforce participation and the number of paid work hours (see e.g. Carmichael and Charles, 1998; Kotsadam, 2011). A smaller number of studies have focused on the employment effects of informal care roles for mature-age women, but have typically also identified negative employment effects of informal care roles. For example, using data from the Australian Longitudinal Study on Women’s Health for 2001 and 2004, Berecki-Gisolf et al. (2008) found that women aged in their 50 s who took up a role caring for an ill, frail or disabled person between these years had a lower rate of labour force participation than other mature-age Australian women. Probit regression analysis of data from the Housing, Income and Labour Dynamics in Australia (HILDA) survey for 2001 to 2009 by Austen and Ong (2013) revealed that the probability of a mature-age Australian woman retaining employment from one year to the next reduced when her informal care roles (measured by hours involved in caring for a child, or ill or disabled family member) increased. International studies that have focused on mature-age women have reached similar conclusions (Bolin et al., 2008; Hank, 2004; Pavalko and Artis, 1997; Spiess and Schneider, 2003; Wakabayashi and Donato, 2005).
However, the empirical evidence on the employment impacts of informal care roles is not conclusive. In his detailed analysis of a cross-section of Australian workers in the HILDA data between 2001 and 2007, Leigh (2010) found only small effects of informal care roles on labour market outcomes, including employment status, number of weeks worked, and hourly wage rates. Wolf and Soldo (1994) found no effect of elder care on employment or hours worked. A recent Austrian study by Schneider et al. (2012), similar to the current study, used logit regression techniques to examine how informal care roles affect the turnover intentions of workers. It found that increased hours spent in an elder care role reduced the relative risk that a female worker would anticipate a job change. It also found that women who provided care to an older person in need of supervision had a lower relative risk of anticipating labour market exit, which was interpreted as evidence of the respite effect of paid work.
The mixed evidence base on the employment effects of informal care roles creates an important need for further empirical work – to achieve clarity about the nature of the relationship between informal care and paid work roles. However, there are also important theoretical reasons for pursuing this topic. Virtually all the empirical studies outlined so far have focused on the time demands associated with informal care roles, and how this can make the maintenance of paid work roles difficult. It has neglected the financial costs associated with the provisioning of family needs. As such, the existing empirical literature has, implicitly at least, been guided by a human capital model that emphasizes how individual decision-making about paid work roles is affected by the present value of alternative uses of time, such as participation in paid work or involvement in informal care. Informal care needs are typically described as involving time commitments that raise the direct and opportunity costs of paid work and, thus, reduce the attractiveness of this particular alternative (see Schneider et al., 2012). The relationship between informal care needs and paid work is also commonly understood to vary with workplace characteristics. For example, characteristics such as access to flexible working arrangements and/or the ability to take leave for family reasons are expected to reduce the opportunity cost of undertaking a paid work role (see Austen and Ong, 2013).
Whilst this theoretical approach highlights some important elements of the relationship between informal care and paid work roles, it has also resulted in an empirical literature that has neglected other, potentially important aspects of the relationship, including the influence of the economic circumstances of individuals with informal care roles. Previous empirical studies have typically not explored the possibility that the effects of informal care roles on employment decision-making might vary with social class, as well as gender. This is an important gap in the research for two reasons. First, and perhaps most obviously, it is important to acknowledge the diversity of women’s situations and how the effect of similar life events, such as the advent of informal care roles, will vary between groups of women. Knowledge of these differences will be important to the achievement of policies aimed at addressing any inequalities associated with the allocation of informal care roles to women. Second, at the empirical level, variation in the employment effects of informal care roles across socio-demographic groups might help to explain why, when calculated across all groups, the effects are often measured as small or insignificant. That is, if informal care roles are associated with lower rates of involvement in paid work in one group and higher rates of involvement in another, the net measured employment effect of the roles might be small.
Theoretical frame and research hypotheses
Our study responds to current gaps in the literature on the employment effects of informal care roles by utilizing a model of household production that can reflect both the time demands of informal care roles and their association with financial costs. Models of household production (Gronau, 1977) focus on the decisions that households make about provisioning their various needs. Reflecting their neo-classical origins, the models assume that households evaluate the relative availability, cost, and quality of alternative ways of ‘producing’ the goods and services required to provision their needs. These alternatives may be ‘time intensive’, such as when the household members directly provide care for other family members, or ‘market goods intensive’, such as when products or services are purchased to provide for family needs. Household production models, therefore, explicitly consider variables that are largely neglected in human capital models of employment decision-making. They also incorporate an assumption that household members share a common set of preferences relating to the alternatives available to them. A household production model outlined by Bosworth et al. (1996) assumes that individual household members will allocate their time between paid and unpaid roles in order to achieve their household’s agreed needs. Purchased or market goods and services must be funded by income, which can be derived from participation in paid work or alternative sources, such as accumulated savings or government transfers.
This model generates a number of predictions that are relevant to the current study, which focuses on issues relating to the provisioning of family care needs. First, time (as opposed to market-based) alternatives for the provisioning of these needs will be more heavily utilised in household situations where the market alternatives are not readily available, are very costly, or of poor quality, all other things being equal. In these situations, the models predict that family care needs will result in fewer (or zero) paid work hours by household members, as they increase their allocation of time to informal care. The predicted reduction in paid work hours need not be evenly distributed amongst household members. Indeed, women’s lower average earnings lead to the prediction that their time is more likely to be allocated to unpaid roles due to a lower opportunity cost. Agreed household needs therefore lead to particular outcomes for workforce participation by individual household members. Kotsadam (2011) used a similar logic when she related the level of State provision of elder care to the employment rates of women in a range of European countries. In her analysis, low State provision increases the pressure on women to provision this care themselves, with detrimental effects on their involvement in paid work.
A further prediction of the household production model is particularly relevant to the empirical investigation pursued in this paper. The model predicts that, all other things being equal, family care needs that cannot be effectively provisioned through the input of time by household members will increase the importance of paid work by household members without alternative sources of finance. This hypothesis is especially relevant to situations where a dependent family member has an illness or disability that requires relatively expensive medications, equipment, treatment or specialized care. In the absence of alternative sources of income, these expenses will increase the importance of paid work by household members who are able to work. In this scenario, informal care roles may still be relatively high if catering for all of the family member’s needs requires the input of market goods and services and the time of household members. However, in situations where alternative sources of income are available (to meet the cost of medicines, etc.), increased informal care roles may be associated with a reduction in the hours of paid work performed by household members. The models also predict that market (as opposed to time-based) alternatives for the provisioning of family care needs will be more heavily utilised in households with higher wage opportunities, all other things being equal.
Method, data and measures
Econometric specification
This article’s empirical analysis addresses the question of whether, as predicted by the household production models, the effect of informal care roles on employment decision-making varies between women according to their household’s economic circumstances. The analysis focuses on employment decision-making by currently employed workers. We utilize a binomial logit model that relates the probability that a woman is considering leaving her current paid work role to her evaluation of two alternatives: leaving and remaining in her job. Reflecting our theoretical frame, the evaluation of job exit is related to the characteristics of the woman’s current job, including its wage rate, the nature of her family’s care needs (which are likely to influence the availability and cost of market-based care options) and the economic situation of her household.
Following Greene (2002), the formal statement of the binomial logit model is captured by a dependent variable (intention to leave (ITL)) that can take on two possible outcomes (ITL = j, j = 0, 1). The worker may anticipate staying in her current job (ITL = 0); or she expects to leave her current job (ITL = 1). ITL = 0 is regarded as the base outcome. In the first part of our study, we examine differences in ITL in the cross-section where the two outcome values and the defined base outcome generate a binomial logit model formally written as:


An interaction term can capture how the effect of care roles may differ between women with different economic circumstances, with the model defined as:

In the second part of our study we examine temporal differences in ITL between time-periods t1 and t2. In this stage, the dependent variable is increased ITL, which can take on two possible outcomes: lower or constant ITL between t1 and t2 (ΔITL = 0); or increased ITL between the periods (ΔITL = 1). ΔITL = 0 is regarded as the base outcome.
Data
Quantitative studies of the employment effects of family care needs have been hampered by small sample sizes and a lack of detailed information on work characteristics and care requirements (Austen and Ong, 2013; Johnson and Lo Sasso, 2000). In 2010 we designed the Australian MAWAC survey 2 with the aim of providing data relevant to the employment decision-making of Australian mature-age women, including their care roles. Studies of the employment experiences of mature-age women are rare and the group is growing in significance with demographic change and increased rates of workforce participation (Austen and Ong, 2010). The survey focused on the aged care sector because it has a rapidly growing demand for labour, and has a workforce with a median age of 50 and is 95% female. The employment effects of care roles have particular importance in this sector as labour supply may decline if accommodations are not made for workers with high caring responsibilities (Schneider et al., 2012).
By limiting the survey to a single sector it was also possible to reduce heterogeneity in the sample and enhance isolation of the effects on employment decision-making of key variables of interest, such as different care role needs and different economic circumstances.
The initial (‘Wave 1’) MAWAC survey was distributed nationally to aged care providers through their peak industry organization, Aged and Community Services Australia. Eighteen providers identified potential study participants from their personnel data and mailed the survey to 6867 women aged 45 years or over. The survey was completed and returned by 28503 respondents. Approximately 1900 women provided responses to all questions relevant to the current investigation. Approximately one year later, a second MAWAC survey was sent to each of the 6897 women who received the initial survey and 931 responses were received from women who had responded to the initial survey. This gave us complete data for 753 women who responded to the full set of relevant questions in both surveys. This latter set of responses is used in this paper for the longitudinal investigation of the links between changes in family care roles and changing ITL.
Measures
The outcome variable in the cross-sectional analysis is intention to leave the aged care sector (ITL), which was measured by a question in the survey that asked, first, ‘In the past year have you ever thought about leaving the aged care sector?’. A follow-up question asked: ‘How often do you have this thought?’ The possible responses were ‘At least once a year’; ‘At least once a month’; ‘At least once a week’; and ‘Every day’. These responses were grouped into two categories: 1) ‘Low ITL’, where the person had not thought about leaving or had thought about leaving only once in the past year; and 2) ‘High ITL’, where the person had thought about leaving at least once a month, week or day. Approximately one-quarter of the sample reported a high ITL.
While ITL captures only the subjective probability of leaving the current job, empirical evidence demonstrates that turnover intention represents a good proxy for actual turnover (Mobley et al., 1978; Parasuraman, 1989; Schneider et al., 2012). It also has the additional advantage of reducing the problems associated with establishing the chain of causality that arise when actual employment status is linked with care roles. Inverse associations between employment status and care roles revealed through cross-sectional analysis can reflect either a negative relationship between care roles and employment, or a greater tendency amongst non-employed individuals to provide informal care. The use of ITL as the dependent variable reduces the risk of this ambiguity because ITL is unlikely to be causally relevant to care roles.
Our analysis includes measures of care roles relating both to children and to elderly, ill or disabled family members. One variable identifies the number of dependent children living in the worker’s home (27.9% of respondents reported living with at least one dependent child). Another variable identifies the workers who provide more than seven hours of care each week to an ill, disabled or elderly family member, including a partner. This care may be provided to a family member who resides outside the respondent’s household. Seven hours of weekly care equates, on average, to an hour each day spent attending to these needs, and 9.3% of the sample reported this level of care. 4
Interaction terms between the aforementioned care-related variables and a measure of the worker’s economic circumstances are used to test whether the employment effects of care roles vary between workers with different economic circumstances. We distinguish between the women who rate their situation as ‘strained or very strained’ and those who rate it as ‘good, very good or neither good nor bad’.
Job characteristics for the model of ITL were chosen to reflect the extant literature on the determinants of job turnover in the presence of informal care roles (usually based on all age groups and genders). These included occupational differences (Henz, 2004); full-time or part-time status (Drago et al., 2007; Henz, 2004); job flexibility (Scharlach et al., 1991); access to sick leave (Lewis, 1997); and workplace climate and coooperative behaviour of colleagues and supervisors (Schneider et al., 2012). Because our respondents are from within a single industry, there are only four key occupational groups: registered nurses, enrolled nurses, personal care assistants and community care workers. We distinguish between workers who work full-time (35 hours weekly) and part-time hours, and incorporate measures of the respondent’s perception of her ability to determine her working hours, her ability to take leave for family reasons, and whether she is worried about job loss/ability to find another job. Workplace climate is measured by the worker’s perception of the quality of her relationships with higher-level management, supervisors and colleagues.
The selection of personal characteristics for the model also reflects the status of existing literature in the field. This typically highlights how employment rates are negatively related to age and positively related to the employment status of partners (Austen and Ong, 2013). A large number of studies indicate that health status is an important determinant of job turnover (Austen and Ong, 2010; Hasselhorn et al., 2005). Education and labour force experience are commonly linked to job turnover, given their association to wage opportunities and labour market attachment (Austen and Ong, 2013).
We do not require controls for education because our sample is restricted to aged care workers and differences in education are closely tied to differences in occupation. Registered nurses commonly have a university-based qualification, whilst community care workers complete relatively short courses of post-secondary education. Labour force experience is measured by the proportion of time spent in paid work since leaving school. The measure of partner status takes account of whether the woman is married and, if so, whether her partner works full-time hours.
Most studies of the health impacts on turnover rely on workers’ subjective assessment of their health (Austen and Ong, 2013; Schneider et al., 2012). We use the more finely grained Work Ability Index (WAI) score (Tuomi et al., 1991), which is comprised of items that target the workers’ 1) subjective estimation of present work ability compared with lifetime best performance; 2) subjective work ability in relation to both physical and mental demands of the work; 3) number of diagnosed diseases; 4) subjective estimation of working impairment due to ill health; 5) sickness absence during the past year; 6) own prognosis of work ability after two years; and 7) psychological resources (enjoying daily tasks, activity and life spirit, optimistic about the future). The WAI is created by allocating points to each item, producing a summative score that ranges from 7 to 49 points. Our analysis of the links between work ability and ITL is based on a categorization of the WAI according to a transformation of the WAI scores into z-scores. Three categories are identified: ‘Low WAI’ (z ≤ −1); ‘medium WAI’ (−1 ≤ z ≤ 1); and ‘high WAI’ (z ≥ 1).
The second stage of analysis exploits the longitudinal aspects of the MAWAC data to examine how changes in family care needs affect ITL. To isolate these effects the dependent variable measures whether ITL increased between the two waves of the survey or not. 5 We measure whether care roles for children, partners and other family members increased, decreased or remained stable over the previous 12 months. Account is taken of the current level of care. Twenty-seven per cent of the sample reported zero care roles in both waves; 5.7% reported that their care roles had fallen to zero by Wave 2, whilst 7.2% reported lower but still positive care roles. Positive but unchanged care roles were reported by 41.3% of the sample and 18.5% reported higher care roles.
Several control variables in this stage of the analysis are defined in terms of change, rather than levels. Change in ITL is related to experiences of illness or injury in the previous 12 months, and perceived improvement or deterioration in working conditions. Controls are retained for the worker’s perceived outside job opportunities, occupation, age, economic situation and initial work hours.
Results
Sample characteristics.
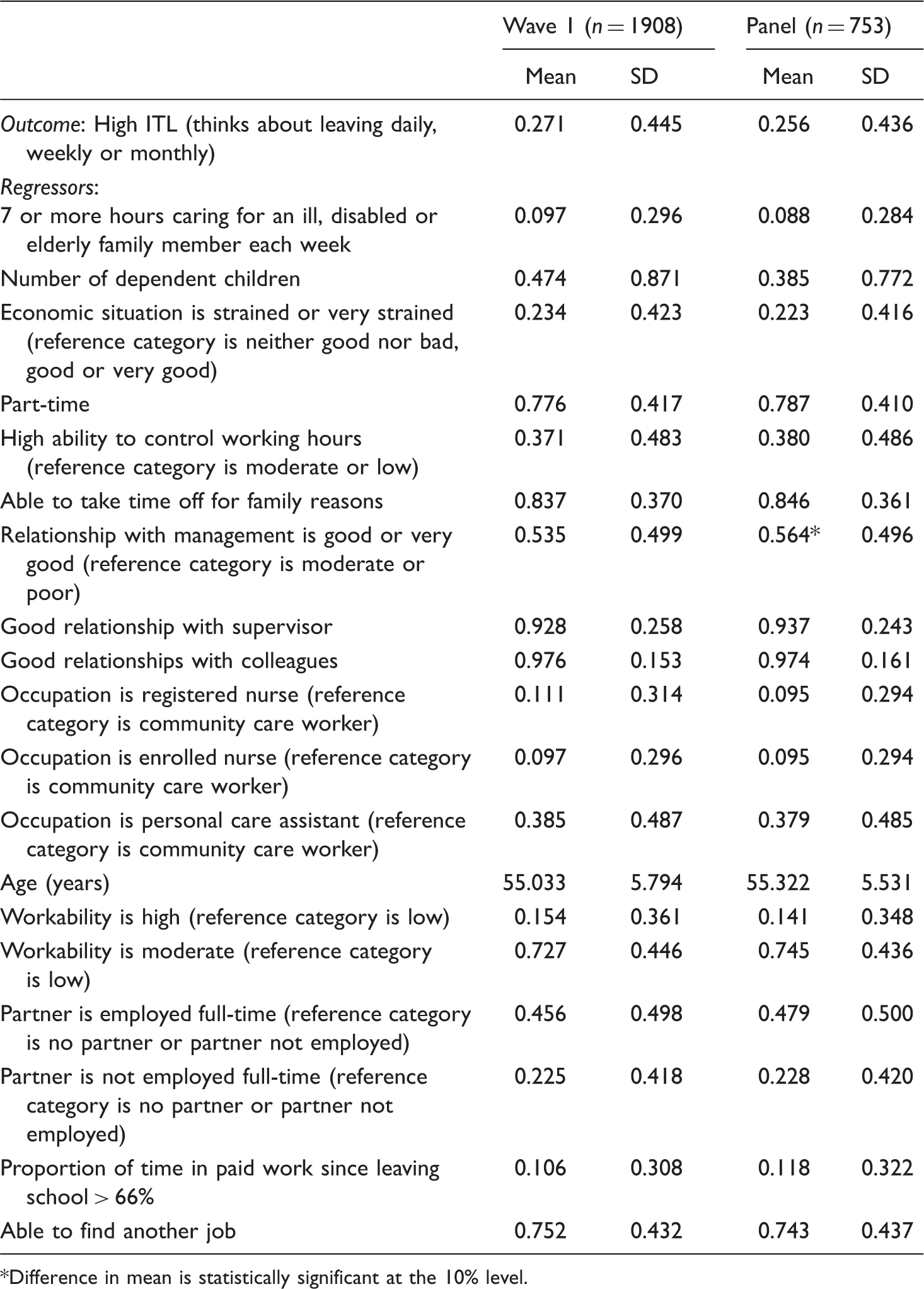
Difference in mean is statistically significant at the 10% level.
Estimation results for the Wave 1 sample.

Number of obs = 1908; log likelihood =−936.35; LR χ 2 (20) = 362.6.
Obtained by using the inteff command in STATA.
Results on the correlates of ITL
When measured across the Wave 1 sample (of mature-age women working in the aged care sector), involvement in care roles relating to ill, frail or disabled family members does not have a statistically significant impact on ITL, and the probability of ITL is negatively associated with an increased number of dependent children. The strongest correlates of high ITL are workability, occupation, characteristics of the work environment, especially the quality of working relationships, and economic situation.
The importance of examining links between the employment impacts of care roles and a woman’s economic situation is highlighted by the results on the interaction term. These indicate that the effect of caring for an ill, frail or disabled family member on the probability of high ITL is significantly lower (by more than 20% points) in households experiencing strained economic circumstances than it is in households with moderate, good or very good circumstances.
Estimation results for the panel.

Number of obs = 753; log likelihood = −394.3; LR χ 2 (15) = 60.
The data in Table 3 confirm the importance of work environment factors in the determination of ITL. The probability of increased ITL is lower for the aged care workers whose work environment improved, compared to those workers whose work environment remained unchanged. The probability of increased ITL is higher for those whose work environment deteriorated (rather than remained unchanged). Part-time work reduced the likelihood of increased ITL, whilst living in a strained economic environment increased this likelihood.
Summary and discussion
Across the sample of mature-age women in Australia’s aged care sector we do not find a significant association between informal care roles and anticipated change in employment. This finding is consistent with results derived by Schneider et al. (2012), from an analysis informed by a human capital model of employment decision-making. As noted earlier, this model emphasises the time demands of informal care roles, but largely neglects the financial resources that may be required to access goods and services that are necessary for providing appropriate informal care. We identify additional, new relationships when we extend our analysis to consider the predictions of a household production model which takes into account the possible need to combine unpaid work with market-based goods and services. Specifically, we find that the employment effects of informal care roles vary with the worker’s economic situation. The association between caring for an ill, frail or disabled family member and ITL is significantly lower for mature-age women with strained or very strained (as compared to good) economic circumstances. This result is only consistent with the predictions of the model of household production, which predicts that, in the absence of other financial resources, the financial costs associated with the provisioning of family care needs can increase the importance of remaining in paid work.
We also find that the presence of dependent children in a woman’s household decreases the probability of high ITL. This contrasts with the findings of most studies on the employment effects of motherhood (see Blau et al., 2010: 98–99). However, it should be kept in mind that our sample is of mature-age women who are likely to have older children. The pattern of our findings could point to the relatively high importance of market goods and services (such as those relating to education) in provisioning the needs of the older child, and/or a relative low ability to substitute home-based production.
These results are important additions to the existing literature on the employment effects of informal care roles and indicate the importance of re-evaluating the type of theory used to guide and interpret empirical analysis of the issue. The existing literature on the employment effects of informal care roles has tended to rely on a human capital model that emphasizes the time demands associated with informal care roles and how these demands increase the incentive to move out of paid work. The results in this paper indicate the relevance of the household production model. This model enables the financial consequences of family care needs that inform the decisions of individuals within households to be reflected in analyses of the individual employment effects of informal care roles. That is, it provides an explanation of differences in these effects across groups of women with access to different economic resources and it helps explain why the ‘average’ employment effect of informal care roles is often found to be small.
The results presented in this paper are consistent with a situation where the financial pressures associated with informal care roles increase the importance of paid work for women living in households with limited economic resources. As such, they highlight the central role that paid work plays in the provisioning of many family care needs. Although this particular finding is not surprising, it is worth emphasizing as it has been neglected in other studies. At a policy level, the finding implies that high priority should be attached to the design and implementation of programmes that enable individuals to sustain their individual paid work roles and respond to family care needs.
This conclusion is reinforced by the pattern of responses to a question to workers with informal care roles in the Wave 2 survey about the effect of these roles on their experiences of paid work. The possible responses were four-fold: the care roles had no effect/required no adjustment in hours or time off (59.6% of respondents with care roles); the roles had some effect but it was possible to cope by taking time off or adjusting hours 6 (26.5%); the roles had some effect but it was possible to cope with the help of family, friends or community organizations (9.6%); and the roles had a large effect and made it difficult to manage (4.3%). These data indicate that, in many cases, informal care roles do not impinge on women’s paid work roles. However, many of the respondents were already working part time hours and, clearly, a substantial number of women find it necessary to create adjustments in their work environment to ‘cope’ with their various paid and unpaid roles. The importance of achieving these accommodations is demonstrated by the rate of high ITL in the (relatively small) group who report that they find it difficult to cope with their paid and unpaid roles (68.2% reported high ITL, as compared to 32.2% of the remainder of the Wave 2 sample). It is also likely that some of the women who were unable to achieve accommodations for their informal care roles left paid work between the waves of data collection and are not represented in our findings.
Several of the other findings of this study on the determinants of ITL support those in the extant literature and, thus, strengthen the evidence base on this issue. In parallel with Schneider et al. (also see Austen and Ong, 2013; Carmichael et al., 2008), we find evidence that flexible working arrangements (specifically, the ability to respond to family care needs) increase the strength of job attachment as measured by ITL. Flexible working arrangements can be important for reconciling the demands of paid work and family care needs.
We also find that good relationships with managers and supervisors increase the strength of job attachment (Schneider et al., 2012, report a strong negative association between workplace climate and ITL for women). Indeed, the intensity of thoughts about leaving the aged care sector appears to be heavily affected by the quality of these relationships – suggesting a significant role can be played by organizations wishing to retain their workforce.
The findings in this paper indicate that workability has a powerful effect on ITL, supporting the findings of Camerino et al. (2006). Workability is a measure of worker health that makes use of finely grained information on the worker’s own assessment of his or health, in addition to information on illness, injury, the ability to meet the physical and mental demands of a job, and psychological resources. It has been used in a large number of studies of worker health over the last quarter-century. The results of the current study highlight the importance of programmes aimed at improving occupational health in maximizing the individuals’ chances of remaining in paid work.
The findings presented in this paper, we believe, represent an important contribution to the evidence base on the employment effects of informal care roles and may assist other researchers to structure their inquiries into the issue. However, there are also some limitations of the current investigation, which future research might be able to address. First, we rely on ITL as a proxy for job exit. European studies provide evidence to support this approach (see Schneider et al., 2012). However, ideally, with the development of larger panels, future studies will be able to utilize more direct measures of employment change.
The fact that our study is based on workers’ experiences in the aged care sector may raise some questions about the ability to generalize its results to other parts of the workforce. The sector features a range of working conditions (especially a very high proportion of part-time and shift work) that may lessen the effect of family care needs on individual employment decision-making. Indeed, qualitative interview data collected as an additional part of the larger MAWAC study indicate that many women choose to work in the aged care sector because its work patterns allow them to more easily accommodate their informal care roles. Future studies of other sectors could contribute important insights into how family care needs influence employment decision-making in different parts of the labour market. Ideally, a single study would canvass a range of sectors. However, a balance must be sought between the greater ability to generalize from data collected from a heterogeneous sample and the greater certainty about relationships measured in data from a more homogeneous sample.
Ideally, future research will also explore the different dimensions of the family care needs that are associated with informal care roles (such as the location, type, cost and frequency of care). Our study utilized a binary indicator to measure care needs relating to ill, disabled or elderly family members. This is an important limitation our data shares with many other large data sets. Furthermore, because our measure was only based on responses to a survey question that asked about the number of hours taken up with these care needs, it is possible that we understate the extent of these needs. As Calvano (2013) notes, if survey respondents do not consider tasks such as driving a parent or spouse to the doctor or helping with finances as ‘care’, then they would not consider themselves ‘caregivers’.
At a theoretical level, there is a need for ongoing research into the elements of household decision-making around the provisioning of family care needs that are not covered by conventional household production models. These elements, which include conflict and cooperation and bargaining amongst/between family members (see Sen, 1990), need to be incorporated to explain why women undertake the majority of unpaid work relating to the care needs of their families. In this paper we utilize a household model to reflect particular aspects of the decision-making environment confronting women (and men) with family care needs. However, more theoretical developments are needed to capture the complexity of household decision making around informal care and work (Agarwal, 1997; Bergmann, 1986; Folbre, 2004). For example, Charusheela (2003) adopts a postcolonial feminist economic perspective to argue that working class women, immigrants and ethnic minority women have always had to work and paid work has been essential ‘for putting food on the table’. Highlighting the importance of the assumptions that are made about choice and power relationships when we theorise about informal work relationships, she emphasizes that women in these situations experience limited power in both the productive and reproductive spheres and can be overworked in both areas.
We conclude by emphasizing that organizations and policy makers will increasingly have to respond to the family care needs of their employees, and that this will demand a sensitivity to the various family and other circumstances of people within the workforce. This is particularly important in a context of increased rates of labour force participation by mature-age women. The evidence compiled in this paper suggests that a supportive work environment and strong working relationships are likely to minimize the employment and other effects of family care needs. The evidence in this paper also suggests that paid work roles are beneficial to many caregivers and this should create an important extra motivation for ensuring this type of assistance is provided where possible.
Footnotes
Declaration of conflict of interest
The author(s) declare that there is no potential conflict of interest with respect to the research, authorship and/or publication of this article.
Funding
The research was supported by an Australian Research Council (ARC) Discovery Project grant (DP110102728).