
Abstract
An abandoned fetus with suspicious skin injuries was found dead, lying on the grass of a garden, near a private house. Suspecting infanticide, the prosecutor ordered a medico-legal autopsy. The cause of death was identified as a congenital malformation of the central nervous system such as hydranencephaly, and infanticide was excluded.
Introduction
Forensic investigation of fetuses, stillbirths and newborns and their differential diagnosis often present many difficulties. These bodies are often left in open-air places, and it is not always possible to identify their mother. Sometimes the medico-legal investigation is even more complex because of the putrefaction decay and post-mortem micro- and macro-fauna action. We report the case of fetal remains where the presence of maceration and post-mortem artefacts, as well as an unusual abnormality of the central nervous system, resulted in a difficult diagnosis. To our knowledge, this is the second case report in forensic literature. 1
Case report
A body of an abandoned male baby was found lying on the grass of a garden, near a private house. The body was completely naked, with its umbilical cord lacerated at its placental end; the placenta was missing. Suspecting infanticide, the prosecutor ordered a medico-legal autopsy.
Autopsy findings
Grass and small leaves were seen on the body (Figures 1 and 2). The abdominal wall was diffusely green stained due to initial putrefaction. No congenital anomalies or deformities were observed. Anthropometric data were: length 44.5 cm; weight 1355 g; crown-rump length (CRL) 30 cm; head circumference 29 cm; bisacromial diameter 7 cm; bitrochanteric diameter 5 cm; foot length 5.6 cm. The testicles were not palpable in the scrotum. Nails of the fingers and toes were visible. The head was diffusely covered by black hair about 0.5 cm long; no abnormal masses were visible or palpable at the anterior and posterior fontanelles. The umbilical cord was 4 cm long, still anchored to the abdominal wall, untied and with its free end irregularly jagged and disrupted.
The fetus: frontal view. The fetus: back view.

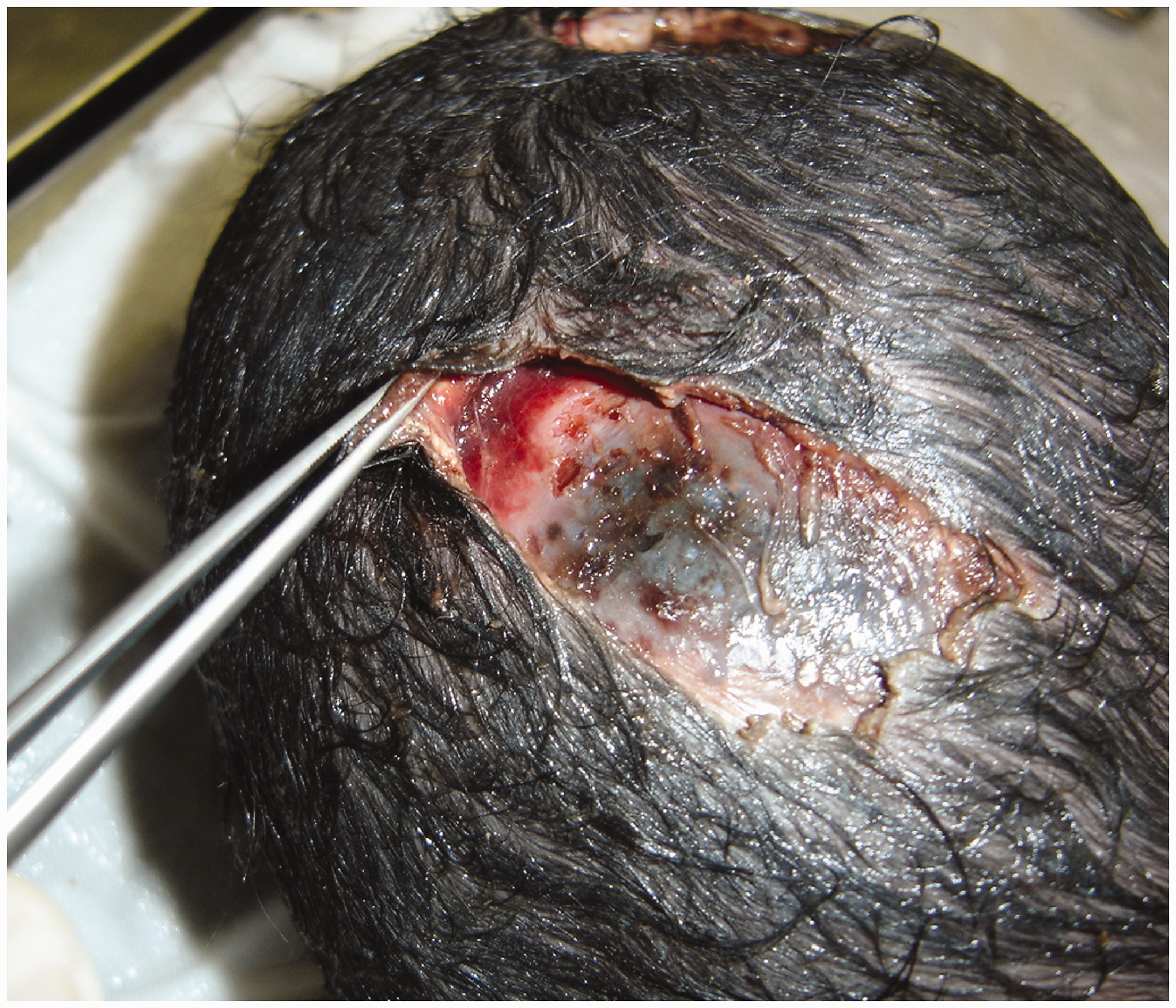
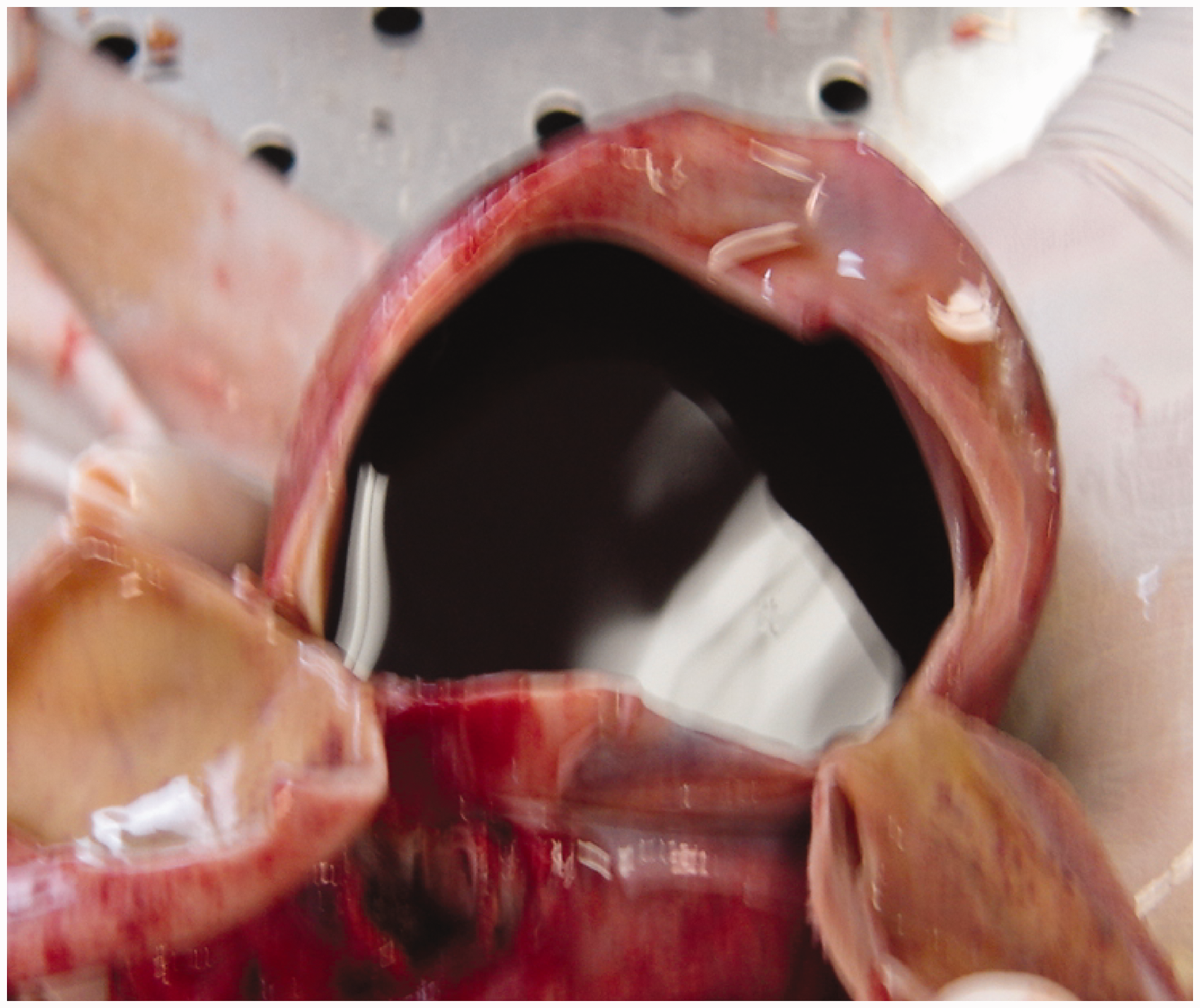
On external examination, many areas of maceration were visible to the face, anterior surface of the chest and abdomen and upper and lower limbs (Figure 3). The left parietal bone was visible through an irregular scalp defect, showing small notches on the osteocartilagineal surface (Figure 4). The external surface of the skull was intact; the anterior and posterior fontanelles were 4 × 4 cm and 3 × 3 cm respectively. Once the cranium was opened, there was only abundant brown-coloured liquid, of water-like consistency, and a very small amount of pultaceus material at the cranial base; no tentoriuos cerebelli was identifiable (Figures 5 and 6). Cerebral arteries and the Willis’ Circle could not be found, although internal and external carotid arteries were found in the neck. No other abnormalities were found; organs were all present and macroscopically intact, although very soft and easily dispersed due to maceration (thymus 9 g; heart 10 g; right lung 12 g; left lung 11 g; liver 58 g; right kidney 5 g; left kidney 6 g). The testicles were correctly positioned in the abdomen cavity. The lungs were dark-red coloured, and solid in consistency. Once the distal epiphysis of the right femur was cut, no ossification centres were found.
The face: post-mortem injuries. The scalp: small notches on the osteocartilagineal surface probably due to the action of teeth or nails of small animals. Abundant brown-coloured liquid, of water-like consistency, in the cranium. The empty cranium: a small amount of pultaceus material in the sub-tentorial region.

Histological findings
The lungs were in the saccular developmental stage. The walls of respiratory bronchioles, alveolar ducts and alveoli were collapsed, without air inside. A very low staining for surfactant at alveoli levels was found through immunohistochemical staining. Skin samples were analysed, showing mostly maceration areas. No haemorrhage, leukocytes or expression of inflammatory molecules (P-Selectin) was seen. Some samples (from the forehead and occipital region where the skin was intact) showed a little haemorrhagic infiltration and a high P-Selectin expression. In samples from the skull corresponding to scalp lesions, subperiosteal haemorrhagic infiltration without P-Selectin expression was noted. At the umbilical cord, a reduced haemorrhagic infiltration with a very intensive P-Selectin expression was found. Other organs showed no pathological findings.
Discussion
The macroscopic features of the lungs, in particular their extremely compact appearance, indicate that, once out of the womb, the fetus did not breathe independently. Furthermore, histological investigations highlighted the compactness of the bronchi, the respiratory cavity collapse and the thickening of alveolar septa: all these elements indicate that there was not air in the lungs. The biometric collected data (length, bisacromial diameter, bitrochanteric diameter, and foot length), the absence of ossification centres and the weight of the organs suggest that the fetus was around 30 weeks gestation. This is in agreement with the fact that the testicles were undescended.
Some suspicious skin injuries, all characterized by the absence of macroscopic and histological signs of haemorrhagic infiltration, were due to maceration, while others were consistent with both the frictional forces due to contact of the skin surface of the fetus with the ground and with the action of the micro- and macro-fauna. In this regard, it should be noted that the small notches on the osteocartilagineal surface of one lesion on the scalp in the left parietal region (Figure 4) are consistent with the action of teeth or nails of small animals such as rats, cats, small dogs, and so on.
The only exceptions were the histological pattern characterizing fragments of intact skin sampled from the occipital region and the forehead (Figure 3), where the haemorrhagic infiltration of subcutaneous adipose tissue was accompanied by an initial fibrinous reticular and some white cells. However, these elements are consistent with a ‘caput succedaneum’, a condition involving a serosanguinous, subcutaneous, extraperiosteal fluid collection with poorly defined margins caused by the pressure of the presenting part of the scalp against the dilating cervix during delivery.
To explain the death of the fetus, given the absence of signs of ante-mortem traumatic lesions, it is necessary to consider the findings inside the skull: abundant brown-coloured liquid, of water-like consistency, and a small amount of pultaceus material in the sub-tentorial region. It must be assumed that the post-mortem decay can hardly justify the pathological findings in the case under discussion. In fact, even considering that the brain is particularly vulnerable to post-mortem decay, even in the later stages of this transformation, it tends to take on a “creamy” consistency and not the “watery” one found in this case. In any case, the good state of preservation of all other organs makes it even more difficult to attribute the state of the brain to the simple post-mortem transformation.
However, the almost complete replacement of the brain by abundant liquid of water-like consistency suggests that the fetus had hydranencephaly. Moreover, the enlarged head circumference (almost 1 cm above that expected for 30 weeks gestational age) supports this hypothesis.
Hydranencephaly is a very rare congenital condition characterised by the complete, or almost complete, absence of the cerebral hemispheres during intrauterine development, and their replacement by a cystic cavity with liquid content. 2 The hallmark is the extensive reduction in brain matter that has been replaced with cerebrospinal fluid. Infants with hydranencephaly have a reduced life expectancy, being either stillborn (more often) or dying within a few hours or weeks after birth, although McAbee et al. reported two cases with 24 and 66 months survival respectively, 3 Bae et al. a case of a 22-year-old female, 4 and Cecchetto et al. a 32-year-old Caucasian male. 2
The aetiology of this malformation is unknown, and in some cases it is a complication of infections contracted by the mother during pregnancy, especially toxoplasma or cytomegalovirus, while according to other authors, it is due to an abnormal development of the fetal arteries (particularly carotid arteries) spraying the brain.5–10
It is still debated when this malformation occurs, although it is generally accepted from the 12th to 26th gestational week, because any later than this and there would be multicystic encephalomalacia instead of hydranencephaly.11–15
The elements now reported suggest that the fetus was suffering from hydranencephaly, that a preterm birth occurred, and that, once extracted from the womb, the fetus did not breathe independently. Moreover, the presence of a disrupted and untied umbilical cord suggests that the delivery was unassisted.
Although very rare, hydranencephaly should be kept in mind by forensic pathologists dealing with fetuses or newborns, above all because these cases often concern women living in economic and social difficulties, with a high chance of being exposed to pathogens and poor antenatal care including ultrasound examinations during pregnancy that could discover this (or other) congenital malformation.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.