
Abstract
A 55-year-old wheelchair-bound woman with severe cerebral palsy was found at autopsy to have marked distention of the stomach due to a volvulus. The stomach was viable, and filled with air and fluid and had pushed the left dome of the diaphragm upwards causing marked compression of the left lung with a mediastinal shift to the right (including the heart). There was no evidence of gastric perforation, ischaemic necrosis or peritonitis. Removal of the organ block revealed marked kyphoscoliosis. Histology confirmed the viability of the stomach and biochemistry showed no dehydration. Death in cases of acute gastric volvulus usually occurs because of compromise of the gastric blood supply resulting in ischaemic necrosis with distention from swallowed air and fluid resulting in perforation with lethal peritonitis. Hypovolaemic shock may also occur. However, the current case demonstrates an alternative lethal mechanism, that of respiratory compromise due to marked thoracic organ compression.
Introduction
Gastric volvulus refers to rotation of the stomach or part of the stomach by more than 180° creating a closed-loop obstruction. 1 It is a rare entity that may be primary, typically related to abnormalities of the gastric ligaments such as elongation, or secondary, related to abnormalities of gastric function or adjacent organs.2,3 It may also occur in individuals with severe cerebral palsy due to rotation and posterior displacement of the stomach associated with severe kyphoscoliosis. 4 Typically in fatal cases of gastric volvulus, death results from ischaemic necrosis, perforation, peritonitis or hypovolaemic shock, secondary to marked organ rotation.2,5 A case of fatal gastric volvulus in a 55-year-old woman is reported to demonstrate an alternative lethal mechanism.
Case report
A 55-year-old wheelchair-bound woman was admitted to hospital with decreased conscious state and respiratory distress. She had a past history of severe cerebral palsy, intellectual impairment and epilepsy. On examination, her abdomen was tense and distended. Although abdominal X-rays showed intestinal obstruction/volvulus, she was deemed unfit for surgery and did not respond to supportive therapy. Death occurred the following day.
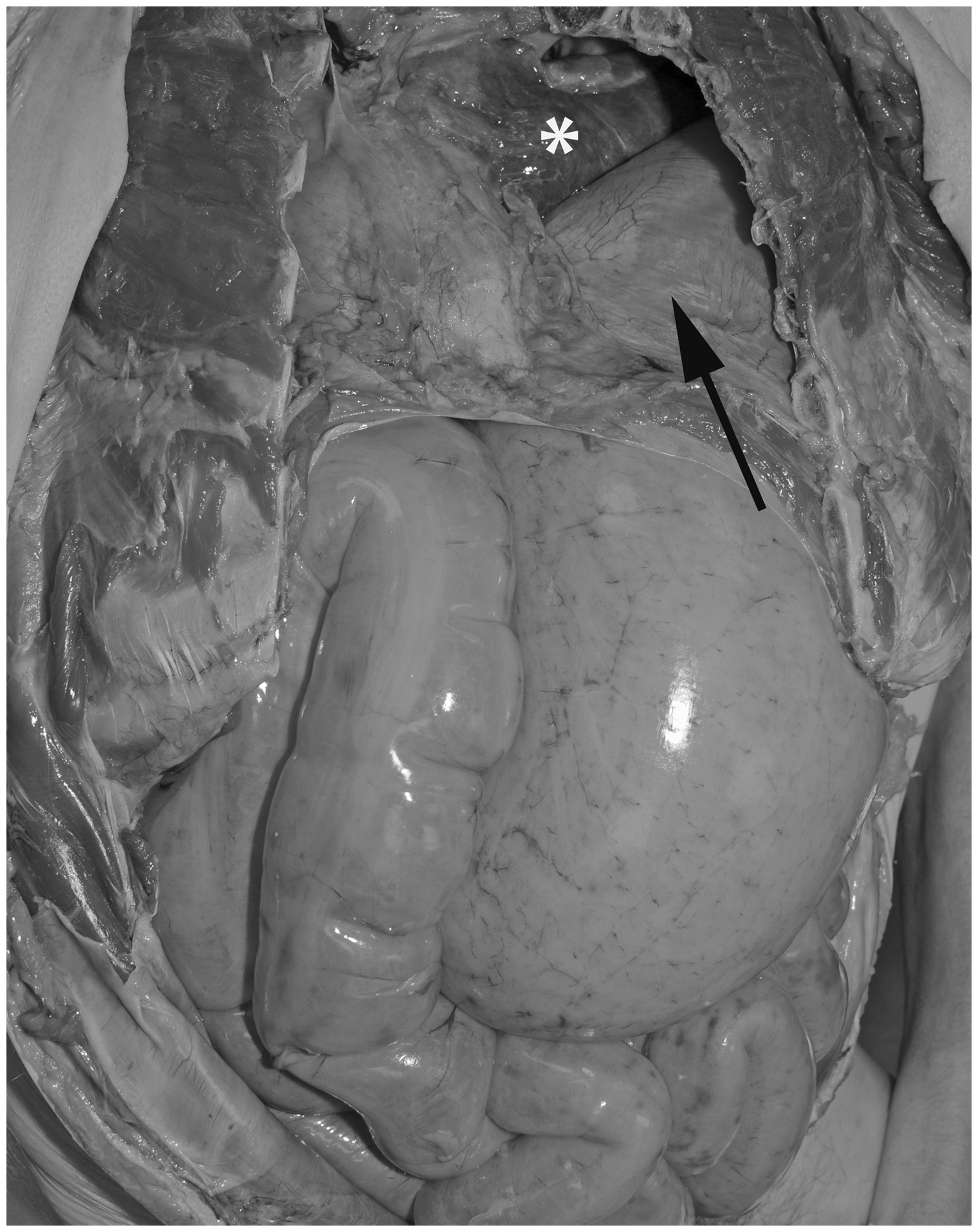
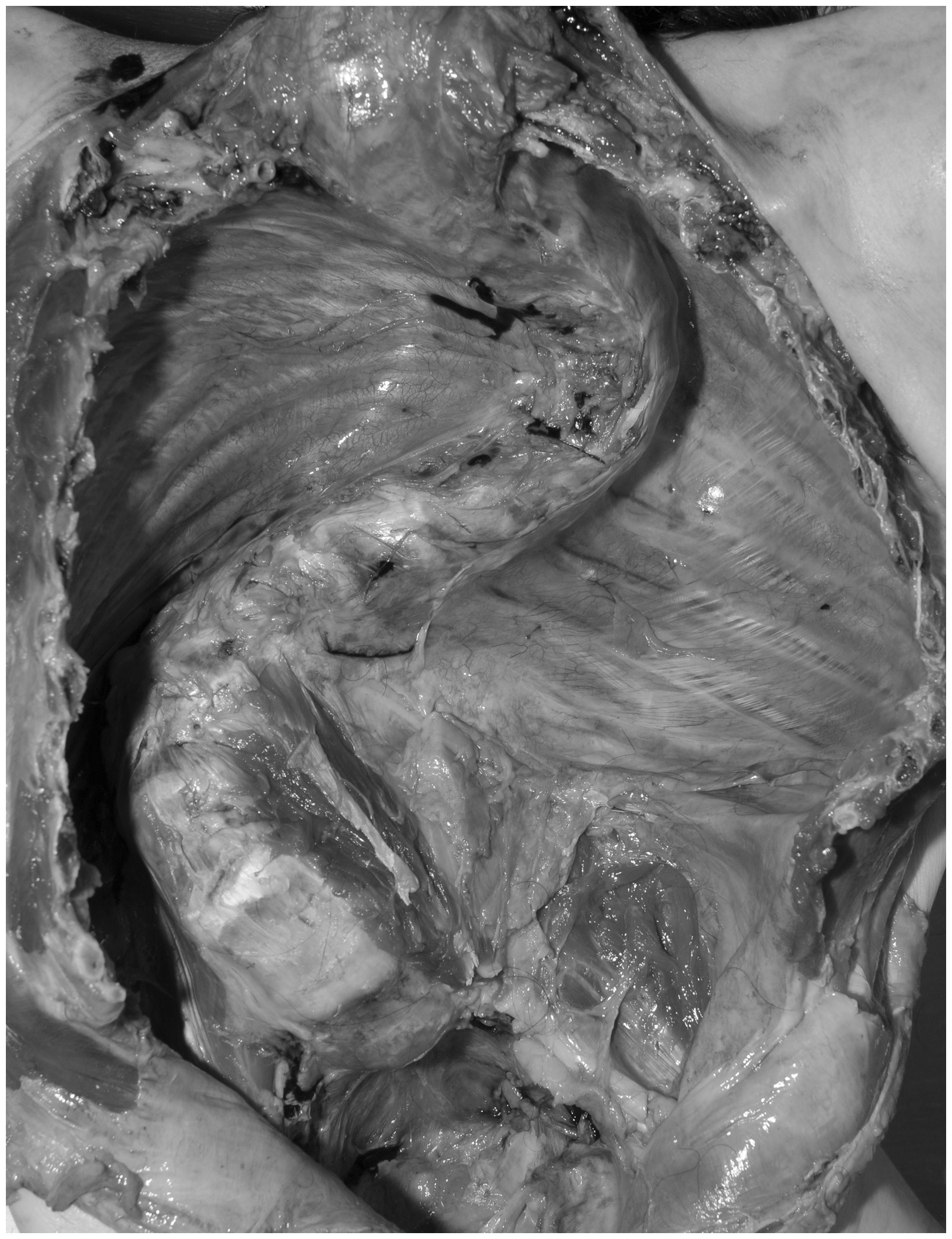
A medicolegal autopsy was undertaken. There was marked kyphoscoliosis with a dysmorphic face, microcephaly and flexion deformities of the feet. The weight was 24 kg and length 122 cm. The most significant finding was marked distention of the stomach due to a volvulus, which had occurred around the pylorus. The stomach was viable, and filled with air and 200 ml of fluid (Figure 1) which had pushed the left dome of the diaphragm upwards, causing marked compression of the left lung with a mediastinal shift to the right (including the heart) (Figure 2). There was no evidence of perforation, ischaemic necrosis or peritonitis. The remainder of the intestinal tract was distended by gas but was unremarkable, with brown faeces in the distal colon and no obstruction. Removal of the organ block revealed the extent of the underlying kyphoscoliosis (Figure 3). Histology confirmed the viability of the stomach, and the vitreous humour sodium level of 137 mmol/l indicated that there was no dehydration. No other underlying organic diseases were present which could have caused or contributed to death, and there was no evidence of trauma. Death was due to respiratory compromise from a gastric volvulus complicating severe cerebral palsy.
Opening of the peritoneal cavity revealed marked distension of the stomach due to a volvulus in a 55-year-old woman with severe cerebral palsy. The stomach appeared quite viable with no ischaemic changes. Removal of the chest plate revealed that the left dome of the diaphragm was markedly elevated having been displaced upwards (arrow) by the markedly distended stomach. This had resulted in considerable mediastinal shift to the right with compression of the left lung (asterisk). Removal of the thoracic and abdominal viscera revealing marked kyphoscoliosis.
Discussion
Acute gastric dilatation may result from mechanical and/or neurogenic factors, and in individuals with marked physical and mental impairment this can include air swallowing and neuromuscular incoordination. Gastric dilatation may also be associated with diabetes mellitus due to autonomic neuropathy, and with eating disorders.4,6 Kyphoscoliosis, as in the present case, can be an additional predisposing factor due to malposition of the stomach with abnormal ligamentous attachments permitting gastric hypermobility.2,7 In veterinary practice Irish setter pups are at similar risk of volvulus because of a high thoracic depth/width ratio. 8
Intestinal volvulus may occur at any age, and in the elderly may be relatively asymptomatic9,10 and so may be an unexpected finding at forensic autopsy. Gastric volvulus most often occurs in the fifth decade of life, although it may occur in childhood,1,4 and is a relatively rare event, as the stomach is usually held in place superiorly by the oesophagus, inferiorly by the duodenum, and is further secured by the gastric ligaments. 5 However, when it does occur, it carries a high mortality rate of 65%. 11 It can be classified based on its axis of rotation or according to presentation, that is, acute or chronic. 1 Organoaxial volvulus is the most common (in approximately 60% of cases), occurring when the stomach rotates around an axis joining the gastro-oesophageal junction and the pylorus, as in the current case.2,5 The second most common is the mesenteroaxial axis of rotation, where the stomach rotates along the line joining the lesser and greater curvatures. The third and rarest type is a combination of the former two. 2
Distinguishing between acute and chronic gastric volvulus clinically is important as the features and consequences differ. 11 Presentations of chronic gastric volvulus are often non-specific, with recurrent postprandial abdominal pain, belching, vomiting and gastric distension. These cases may be amenable to conservative management.5,11 Acute presentations are, however, life threatening, distinguished by Borchardt’s triad of marked epigastric pain and distension, vomiting with retching, and problems introducing a nasogastric tube into the stomach. 12 However, these signs are not always present and may be difficult to interpret, especially in severely mentally or physically impaired individuals who may not be able to verbalise discomfort.2,4,7 Respiratory distress secondary to increased intrathoracic pressure may occur. 11
Causes of death in cases of acute gastric volvulus usually involve compromise of the blood supply to the stomach, resulting in ischaemic necrosis. This, in combination with distention from swallowed air and fluid, may result in perforation with lethal peritonitis.4,6 Hypovolaemic shock may occur secondary to obstruction, and a rare cause of perforation in a case involving kyphoscoliosis was perforation from distention due to a bleeding gastric ulcer. 13 The current case demonstrates yet another rare lethal mechanism that may be encountered at medicolegal autopsy, that of respiratory compromise from elevation of the diaphragm with lung compression and mediastinal shift. This was on a background of already quite severely compromised respiratory function due to restrictive lung disease from marked kyphoscoliosis.
In conclusion, this report presents an unusual case of death due to gastric volvulus that had caused respiratory compromise. Although rare, the possibility of lethal rotation of the stomach should be considered in all cases of severe cerebral palsy with kyphoscoliosis. Intellectual impairment may obscure symptoms, and lethal mechanisms may be quite variable and only elucidated at the time of autopsy.
Footnotes
Declaration of conflicting interests
None declared.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.