
Abstract
Background
The number of welfare recipients has steadily increased in Japan during recent years, although the number of homeless persons has decreased. Despite there being many reports regarding medicolegal death among homeless persons, medicolegal death among welfare recipients has not been fully investigated.
Methods
We identified 10,293 individuals who received welfare aid during their lifetime among the 81,867 cases that were examined by the Tokyo Medical Examiner’s Office (2008–2013). We retrospectively compared the proportions of medicolegal death to total population, age, sex, family status, clinical history, and manners/causes of death among non-indigent persons (controls), homeless persons, and welfare recipients.
Results
A higher proportion of medicolegal death to total population was observed among the welfare recipients, compared with the controls. The welfare recipients (65.5 years) were younger than the controls (68.9 years), and the proportions of male sex and living alone were higher among the welfare recipients. Hypertension and circulatory disease were the leading clinical conditions among the welfare recipients. Death due to disease was the leading manner of death, and circulatory disease was the leading cause of death among the welfare recipients. The proportion of individuals with a long period between death and discovery (which made determining the cause of death difficult) was also higher among the welfare recipients.
Conclusion
Welfare recipients have a greater risk of sudden death compared with non-indigent persons. Preventive strategies should target middle-aged to elderly men who live alone, and should address their risks of circulatory diseases and solitary death.
Introduction
Technological and economic advances in developed countries have created a huge gap between the social classes. Furthermore, the increasing number of people with low socioeconomic status is a common problem in many countries, especially during financial crises. In Japan, the number of homeless persons increased during the 1990s (when the bubble economy collapsed), and homelessness became a major social problem at the beginning of the 21st century.1,2 A study during 2000 in Osaka city (the second largest Japanese city) demonstrated that many homeless people died untimely deaths due to preventable causes, such as infectious diseases and starvation, 1 which is similar to the findings from other countries.3–6 Therefore, the Japanese government developed comprehensive measures to address homelessness, including job creation, which resulted in the number of homeless persons steadily decreasing from 25,296 in 2003 7 to 6040 in 2015. 8
However, the number of welfare recipients has steadily increased in Japan, especially after the 2007 global financial crisis, despite the decreasing number of homeless persons. Many Japanese homeless persons can apply for welfare payments based on the Livelihood Protection Law, as indigent persons can receive financial support that is customized to the extent of their poverty, in order to maintain a minimum standard of living (e.g. housing and education). In this system, medical care is provided free of charge to all welfare recipients. The number of welfare recipients increased from 882,229 in 1995 to 2,158,840 in 2014, 9 and many of these individuals require assistance to obtain medical services. According to the 2013 Japanese national survey, 46.1% of all welfare recipients were >65 years old and receiving aid for medical services. In addition, 41.8% of recipients who were <65 years old had some disease or injury that required financial support. 9 These data suggest that medicolegal death, including sudden unexpected death, among welfare recipients may also be a serious problem, although specific data regarding this topic have not been collected. Numerous reports have evaluated medicolegal death among homeless persons,1–6 although it is not clear whether those cases’ demographic characteristics also represent cases among welfare recipients.
In this study, we investigated a large number of medicolegal deaths among welfare recipients in Metropolitan Tokyo, which has a medical examiner system. This study aimed to clarify the demographic characteristics of medicolegal deaths among welfare recipients by comparing them with similar cases among homeless and non-indigent persons. We hope that these data can facilitate effective strategies for preventing sudden unexpected death and improving health among welfare recipients.
Materials and methods
Study sample
All medicolegal deaths in Metropolitan Tokyo are reported to the Tokyo Medical Examiner’s Office. Medical examiners perform postmortem examinations to determine the manner and cause of death for these cases, which can be classified as sudden unexpected death due to disease, non-disease-related causes, or unknown causes. Medical examiners perform autopsies when the cause of death cannot be determined by the deceased individual’s clinical history, course of illness, situational and external investigations, or postmortem radiological investigation.
We retrospectively reviewed the case records for all cases that were examined by the Tokyo Medical Examiner’s Office between 2008 and 2013 (n = 81,867, autopsy rate: 19.2%), and selected cases of individuals who had received welfare aid during their lifetime. We also selected homeless cases, which were defined as individuals “who, for no reason, occupy city parks, rivers, roads, stations, and other facilities as the living space to lead their daily lives,” as defined by the “Law Concerning Special Measures to Support Self-Reliance of the Homeless.” 10 All other cases were defined as controls.
Methods
Age distribution according to group.
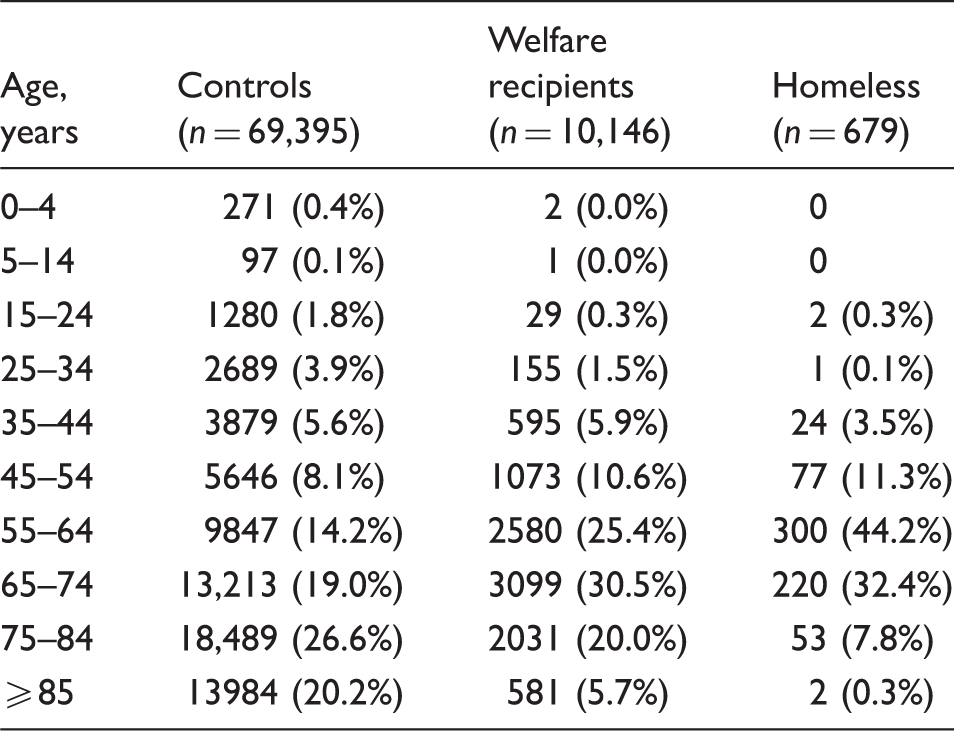
Numbers in parentheses indicate the proportion of cases to the total number in each group.
Data regarding the total number of welfare recipients in Metropolitan Tokyo were obtained from the Bureau of Social Welfare and Public Health, Tokyo Metropolitan Government.11,12 We also obtained data regarding the total number of homeless persons and total population in Metropolitan Tokyo from the census reports of the Ministry of Health, Labour and Welfare.13–20 Causes of death were classified according to International Statistical Classification of Diseases and Related Health Problems, 10th Revision (ICD-10). 21
Cases with unknown age and sex were excluded from the analyses, except as a proportion of the medicolegal deaths among the total population. In addition, cases with suspected criminal involvement or medical malpractice (n = 1647, 2.0% of total cases) were transferred to other facilities (Forensic Department of Medical Faculty of Universities) and were excluded from our analyses, except as a proportion of the medicolegal deaths among the total population, because we could not obtain detailed data (including causes of death) for these cases. Furthermore, we excluded cases that were determined to have involved homicide (n = 7) from the comparisons of the manners/causes of death. The total numbers and autopsy rates for the comparisons of the manners/causes of death were 69,391 controls (autopsy rate: 18.7%), 10,144 welfare recipients (autopsy rate: 22.6%), and 678 homeless persons (autopsy rate: 63.6%).
Statistical analysis
Intergroup comparisons were performed using the χ2 test or t test, as appropriate. Differences with a p-value of < 0.01 were considered statistically significant.
Ethical approval
The Ethics Committee of the Tokyo Medical Examiner’s Office approved the study protocol and use of data.
Results
Demographic characteristics of medicolegal deaths
Proportion of medicolegal death to total population according to group.
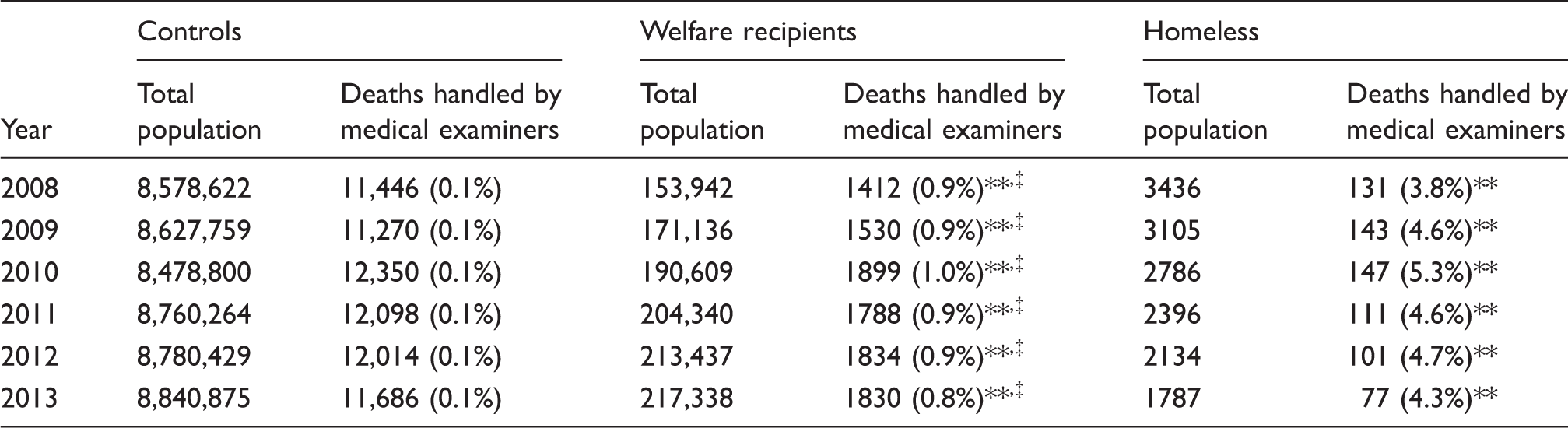
p < 0.001 (compared with controls), ‡p < 0.001 (compared with homeless).
Numbers in parentheses indicate the proportion of cases to total population of each group in each year.
Approximately 80% of the cases were >55 years old for all groups (Table 1). Medicolegal death was most frequently reported among 65–74-year-old welfare recipients, 55–64-year-old homeless persons, and 75–84-year-old controls. The mean ages of the welfare recipients (65.5 years) and homeless persons (62.4 years) were significantly younger than that of the controls (68.9 years) (p < 0.001). The mean age of the welfare recipients was significantly older than that of the homeless persons (p < 0.001).
Sex, family members, and past medical history according to group.
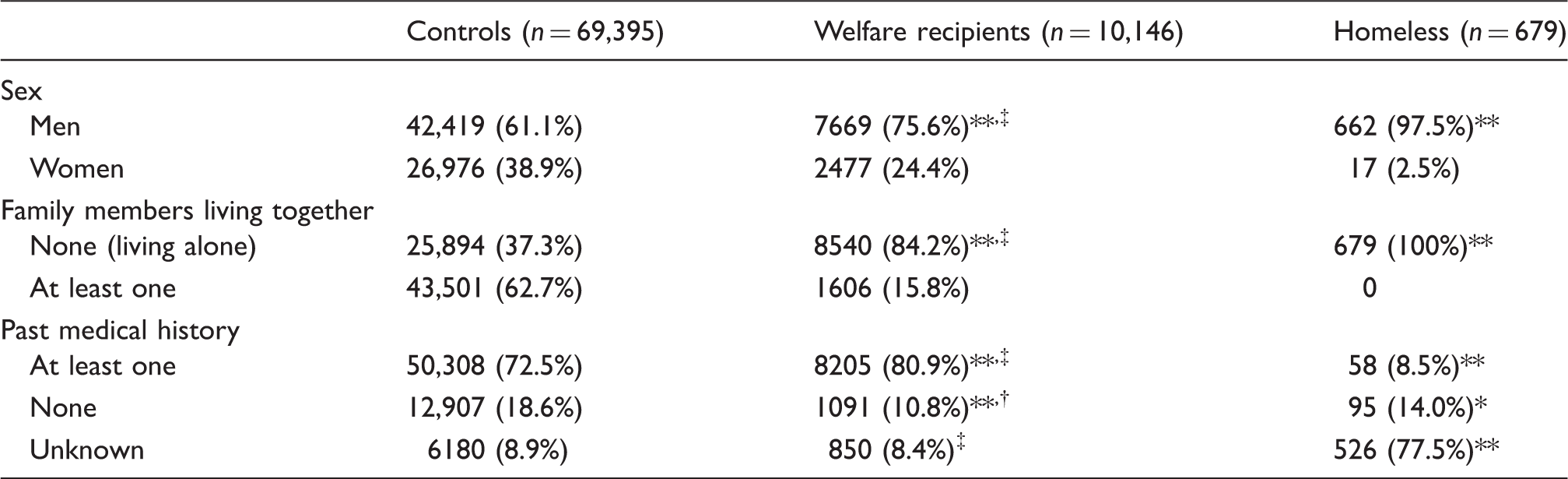
Numbers in parentheses indicate the proportion of cases to the total number in each group.
p < 0.01 (compared with controls), **p < 0.001 (compared with controls), †p < 0.01 (compared with homeless), ‡p < 0.001 (compared with homeless)
Past clinical history
The proportion of individuals with past clinical history was significantly higher among the welfare recipients (n = 8205; 80.9%), compared with that among the controls (n = 50,308; 72.5%) and homeless persons (n = 58; 8.5%; Table 3).
Representative clinical history according to group.
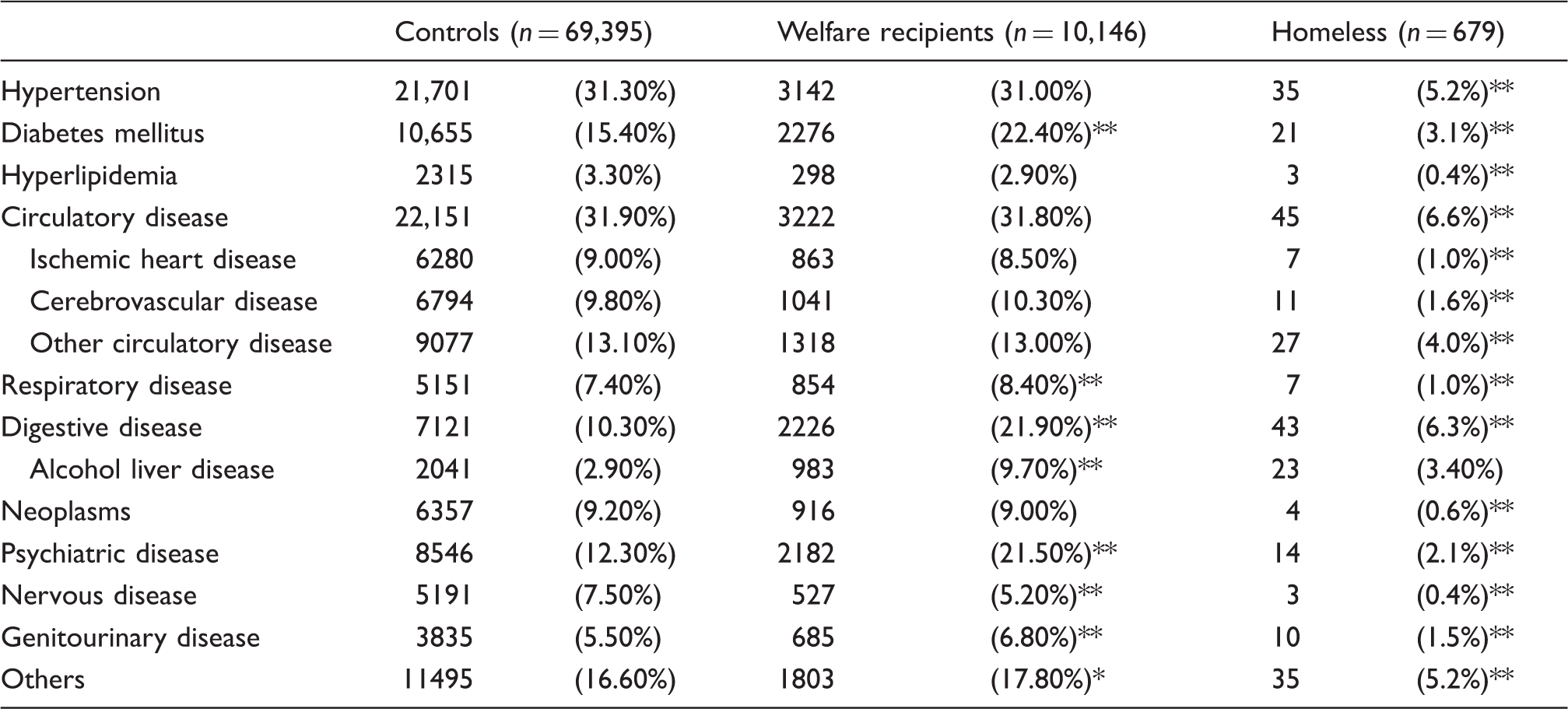
Numbers in parentheses indicate the proportion of cases to the total number in each group.
p < 0.01 (compared with controls), **p < 0.001 (compared with controls)
Comparing the manners of medicolegal death
Death due to disease was the leading manner of death for all groups. The proportion of accidental deaths was higher among homeless persons (22.4%), compared with those among the controls (8.5%) and welfare recipients (7.5%).
Manner of death according to group.
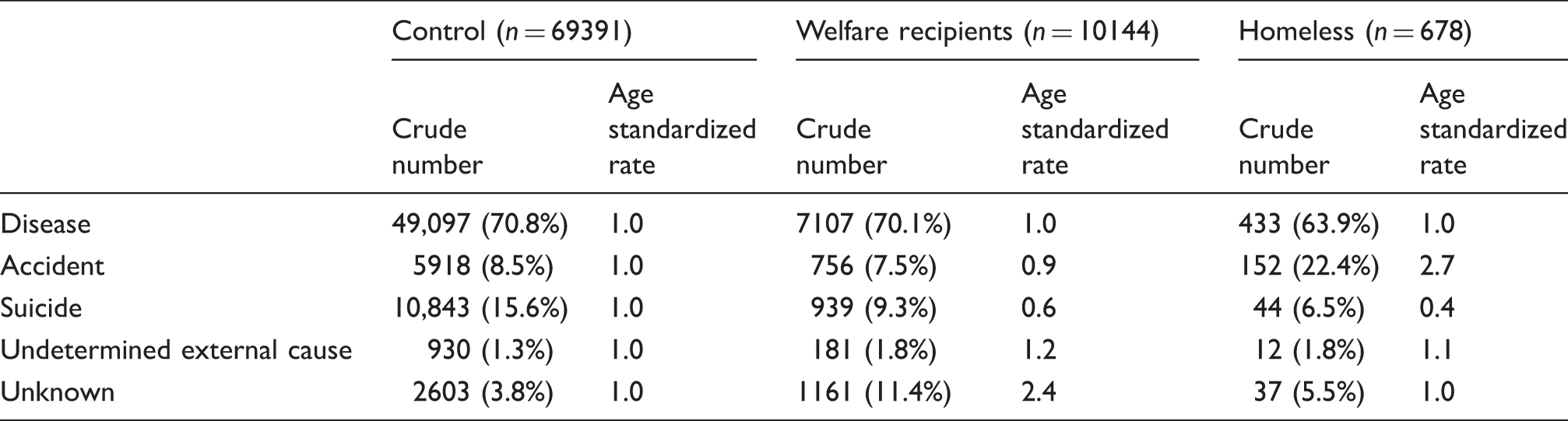
Numbers in parentheses indicate the proportion of cases to the total number in each group.
Comparing the causes of medicolegal death
Regarding death due to disease, circulatory disease was the leading cause of death in all groups, and sub-classification of the circulatory diseases revealed that ischemic heart disease was the most prevalent cause of death. Among the homeless persons, the proportion of circulatory disease (23.0%) was lower than that among the controls (49.0%), whereas the proportions of non-circulatory diseases (e.g. pneumonia, tuberculosis, malnutrition) among the homeless persons were generally higher than those among the controls.
Among the welfare recipients, the proportion of circulatory disease (41.0%) was lower than that among the controls, although the difference was much smaller than the difference between the homeless and control individuals. The proportions of several non-circulatory diseases (e.g. infectious disease, malnutrition) among welfare recipients were midway between those of the homeless and control individuals. After excluding circulatory diseases, digestive disease was the most prevalent cause of death among welfare recipients (11.7%), and the sub-classification of the digestive disease showed that the proportion of alcoholic liver/pancreatic diseases was higher among the welfare recipients (7.2%), compared with those among the controls (2.6%) and homeless persons (4.4%).
Major causes of death according to group.
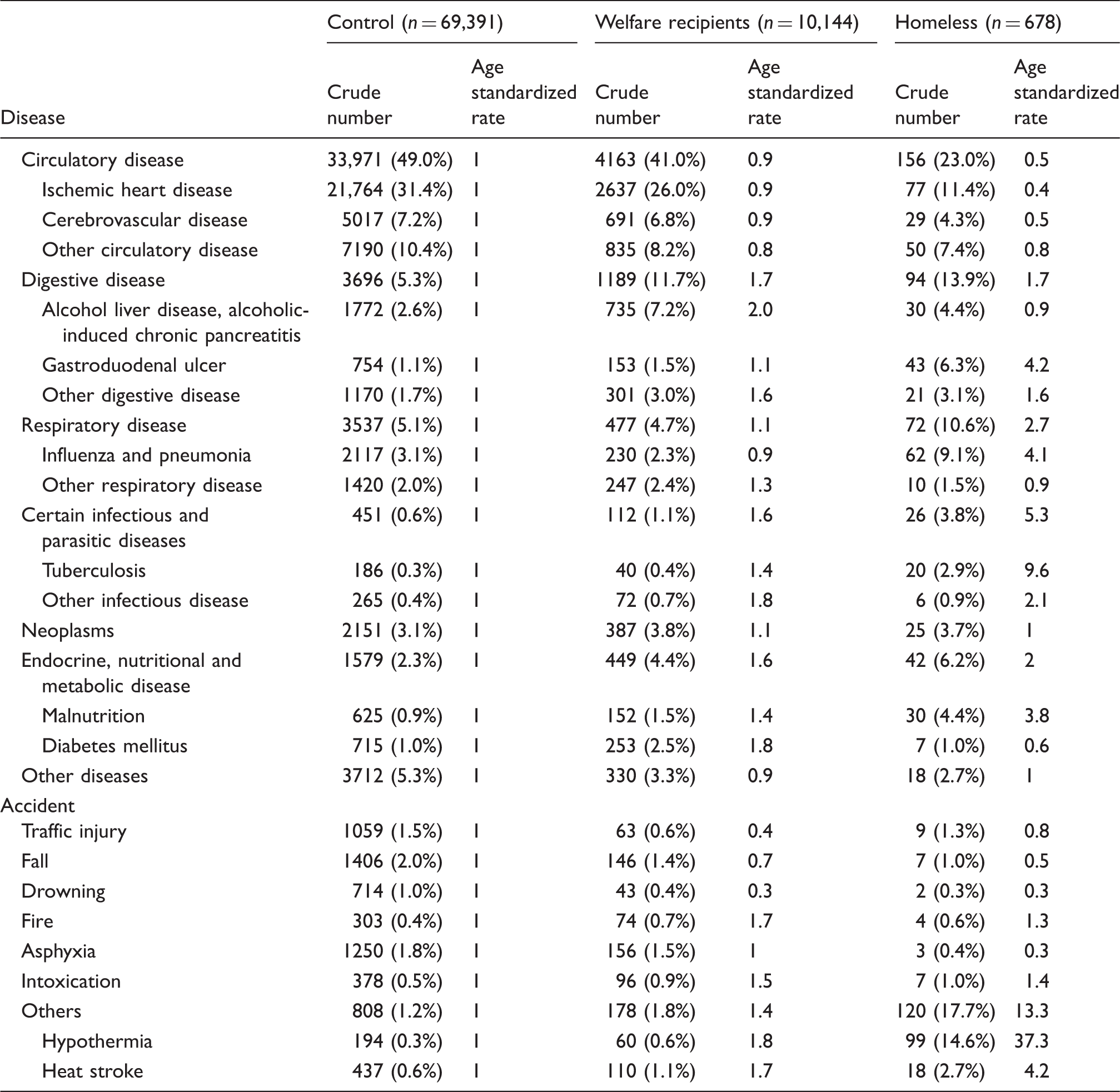
Numbers in parentheses indicate the proportion of cases to the total number in each group.
Discussion
The results of this study clearly demonstrate that welfare recipients had a greater proportion of medicolegal deaths, compared with that among non-indigent persons, although this proportion was less than that among homeless persons. Previous studies have demonstrated that low socioeconomic status is strongly associated with a shorter life expectancy and mortality.22–26 Therefore, our findings of higher proportions of medicolegal deaths and lower ages at death among welfare recipients and homeless persons suggest that medicolegal death may be an important contributor to their shorter life expectancy (vs. that of non-indigent persons). Preventive strategies should focus on middle-aged to elderly men who live alone, as this group accounted for a substantial portion of the medicolegal deaths among welfare recipients.
Death due to disease was the leading manner of medicolegal death among welfare recipients, and our comparisons of several specific causes of death suggest that the causes of death among this group exhibited different characteristics compared with the homeless group. For example, receiving welfare may improve hygiene and nutritional status, which may decrease the numbers of deaths due to pneumonia, tuberculosis, and malnutrition, compared with those among homeless persons. However, increased numbers of death due to circulatory diseases were observed among the welfare recipients. Therefore, measures to address circulatory diseases and lifestyle-related diseases (e.g. hypertension and diabetes) may be important for preventing sudden deaths among welfare recipients, as well as among non-indigent persons. In addition, measures to address alcohol-related diseases may be important, because welfare recipients exhibited higher prevalences of clinical histories and deaths that involved alcohol-related diseases.
The Japanese government covers all medical costs for welfare recipients, which may explain why this population exhibited the highest proportion of having a clinical history. However, it is not clear whether welfare recipients regularly visit a doctor or consistently take their medicine to treat acute or chronic diseases. For example, a study regarding the outcomes of alcoholic liver cirrhosis demonstrated that the treatment dropout rate among patients who were receiving welfare was 35.7%, which was higher than that among the general population. 27 Therefore, welfare service staff should monitor the actual medical consultation status among welfare recipients.
Hypothermia was the leading cause of accidental deaths among homeless persons in the present study, and this finding has also been reported in previous studies.1,2 However, we found that the proportion of hypothermia was significantly lower among welfare recipients, compared with that among homeless persons. Applying for welfare and living indoors may decrease the number of deaths due to hypothermia among welfare recipients, although their proportion of hypothermia was higher than that among non-indigent persons. In addition, the proportion of heatstroke was higher among welfare recipients, compared with that among non-indigent persons. A majority of deaths due to heat stroke occur among elderly persons who remain indoors without a working air conditioner during extreme heat waves. 28 Furthermore, chronic debilitating diseases and social isolation are risk factors for hypothermia and heatstroke,28–31 which might increase the risk of death due to hypothermia and heat stroke among welfare recipients. Therefore, welfare service staff should consider both the physical condition and living environment (e.g. availability of an air conditioner) of welfare recipients, especially during the winter and summer months. Furthermore, anti-psychotic drug use was the major cause of deaths due to intoxication among the welfare recipients. Therefore, psychiatrists and welfare service staff should also consider the risk of overdose and the side effects of the anti-psychotic drugs that welfare recipients are receiving.
We also found that a prolonged period from death to discovery was significantly more common among welfare recipients. As most of the deceased were found indoors at their home, living alone may prolong the discovery period for these cases. Social withdrawal and decreased communication with neighbors were suspected to be causative factors in several cases. A higher prevalence of psychiatric disease in the individuals’ clinical histories might be related to this situation, although further detailed analysis is needed to clarify the reasons for these deaths. Nevertheless, more frequent visits from welfare staff, encouragement to participate in self-help groups, and obtaining regular employment may help decrease the frequency of these solitary deaths.
This study has several limitations. First, the study sample did not include all deaths among welfare recipients, because natural deaths (i.e. death due to disease, as diagnosed by the family physician) are generally not reported to medical examiner’s office. In addition, we excluded homicide cases from the analysis of the manners/causes of death. However, the number of homicide cases is very small in Japan, and their exclusion does not affect our conclusions. Second, we defined non-indigent persons as all individuals who were not included as welfare recipients and homeless persons. Therefore, we cannot exclude the possibility that a small number of indigent persons were included as control cases, because each individual’s economic status could not be fully investigated using the available data. Third, the autopsy rate is not high at our institute, which is likely related to a recent increase in the number of elderly deceased individuals with a clinical history and the use of postmortem radiological investigations at the emergency hospital. In addition, the autopsy rates differed significantly between the groups, which is likely because homeless persons are less likely to have a detailed clinical history. In this context, a previous study revealed that physicians tend to overestimate circulatory disease as a cause of death in non-autopsied cases, and to underestimate other diseases (e.g. digestive disease) and non-disease-related causes (e.g. heat stroke). 32 However, we identified similar trends regarding the causes of death among welfare recipients and the other groups when we only considered autopsied cases (data not shown). Therefore, we believe that this survey provides representative findings regarding many features of sudden death among indigent persons in Japan.
Conclusions
This study revealed a high prevalence of medicolegal deaths among welfare recipients. Middle-aged to elderly men who lived alone accounted for a large proportion of this group, and preventive strategies should include measures to address circulatory diseases and solitary deaths. Furthermore, social support to prevent isolation may be an important method for reducing sudden deaths among welfare recipients.
Footnotes
Contributorship
H Suzuki designed the study, analyzed and interpreted the data and wrote the first draft and subsequent revisions. T Tanifuji and N Abe contributed to the data analysis. T Fukunaga contributed to the data analysis and manuscript review.
Declaration of conflicting interests
None declared.
Funding
The author(s) did not receive any funds or sponsorship of any kind from any individual or organization.