
Abstract
The Department of Health has completed its consultation on the nature of the new medical examiner system and supporting regulations. This article considers whether the regulations for death notification to coroners are fit for purpose in the light of the medical literature on unnatural deaths and the experience of a coroner in a jurisdiction with a heavy workload from specialist hospital referrals. It concludes that they are to be welcomed, but that they should not rely on natural/unnatural death as a criterion for notification of deaths during the course of medical treatment, or refer to ‘neglect’. Furthermore, they should ensure that sudden-death syndromes, which may be considered by doctors as natural, are still notified. Relying on these changes to reduce coronial investigations would be unwise. If that is the intention, other reforms may be necessary.
Introduction
A doctor facing the death of a patient, whom he or she has treated in the last illness, has the choice of either providing a medical certificate of the cause of death for the Registrar of Deaths or reporting the death to the coroner. Doctors have no statutory duty to report deaths to coroners: that lies with the Registrar of Deaths. However, it is undesirable and inhumane for a bereaved person, having received the certificate of death and seeking registration, to be told they cannot proceed with the burial or cremation because the death is being referred to the coroner. Thus, the practice has arisen that doctors in the first instance report appropriate deaths to the coroner that they cannot certify. The current guidance for doctors in the completion of these certificates is to be found in the Notes for Doctors in the front of the Medical Certificates of Death book and the Office for National Statistics (ONS) guidance. 1
The death notification or reporting rate has been shown to vary widely across coroner jurisdictions, from 12% to 87%.2,3 Mclean studied a subgroup of 10 similar-sized jurisdictions and found that the range was from 34% to 62%. 4 He found no association between affluence and notification rate. The reporting rate itself may vary due to variations in judgements of doctors about what is not natural and what requires investigation, and with the degree of risk of operative procedures. Thus, one might expect higher reporting rates in jurisdictions with tertiary referral centres.
The inconsistency in reporting rates has been widely criticised and suggests that, even allowing for case mix and variations in local coroner guidance, the issuing of which has been rightly disapproved by the Chief Coroner, 5 doctors have difficulty in interpreting the guidance.
The first report into health care at Mid Staffordshire NHS Foundation Trust 6 highlighted that there appeared to be between 400 and 1200 avoidable deaths, with emergency-care mortality rates being 27–45% higher than expected. It concluded that even if half were due to coding errors, there was a problem that needed investigating. It is interesting to note that during the period of study (2005–2009), the number of death reports to the relevant coroner actually fell, 7 and continued to fall until 2012. 8 The inquest rate remained stable until 2012, at the national average of 12–13%, as did proportion of natural-death conclusions. Whilst these figures are total of all reports, not just for the NHS, and there may be some natural variance, the scale of excess deaths would be expected to increase reporting rates. A rise of about 5% some four years later would be consistent with the suggestion that there are significant cultural factors in organisations that may influence rates of death reporting, and they take some time to change. The Final Report 9 included Recommendation 273 on the need for guidance to health-care providers to oblige Trusts to provide all relevant information to coroners, and Recommendation 274 on the need for unequivocal guidance to Trusts for a priority of openness in disclosure of information to coroners and families. Thus, organisational as well as individual factors play a part in variation of notifications.
The Shipman Inquiry concluded that the system of certification and its scrutiny were confusing and unsafe. 10 It is the anecdotal experience of this coroner that where a death report is made by a medical practitioner to the coroner, the completion of the Medical Certificate of Death (MCCD) often does not respect these rules and may be omitted altogether. Events such as aspiration are inserted with no underlying cause to assess whether the death is unnatural; often the chain of causation is reversed or ignored. Frequently entries are erroneously made in II that clearly directly relate to matters in I. Medical students do not seem to be trained in death certification. The need for scrutiny of death certification was clearly spelt out in the Shipman Inquiry. Improving standards of death certification is one of the potential aims of the medical examiner –as is GMC guidance Good Medical Practice. 11
The section of the Coroners and Justice Act 2009 on notification and certification of deaths has yet to come into force. 12 The proposed new process envisages that the medical examiner will scrutinise death certificates of those deaths not referred to the coroner. It is understood that models have been considered in which the medical examiner is consulted on only some deaths, but it is suggested that scrutiny of all is essential. The Department of Health consultation (section 2.2) 13 states that all deaths that do not need to be investigated by a coroner will be ‘confirmed by a medical examiner before a MCCD is issued or will be established by a medical examiner’. This is an opportunity to ensure that International Certification of Diseases (ICD) codes are properly used and that referrals to the coroner are accurate and appropriate.
It is envisaged that the examiner may discuss with and get signed assent from the bereaved family an agreement to accept the death certification and non-referral to the coroner, or refer to the coroner. The current medical reporting of deaths to a coroner, under guidance, to avoid later referral by the Registrar of Deaths, is to be replaced by a statutory duty of doctors to notify deaths in prescribed circumstances. This would appear to provide a mechanism for raising standards of certification and replacement of the exploratory discussions of prima facie natural deaths and between doctor and coroners officer with peer supervision and is likely to be widely welcomed in principle (although there are many concerns about implementation). It is envisaged that ordinary reporting of deaths directly from doctors to coroners will continue and that medical examiners will speak to coroner’s officers in cases when there is an ‘unusual interplay of circumstances and medical factors’.
This paper considers one aspect of these reforms, namely the adequacy of the proposed new regulations requiring notification to a coroner of a death.
Methods
The Department of Health proposals and ONS guidance were studied, and their sources and relevant law analysed. A Medline and Embase literature search was conducted up to 2017, using the search terms ‘natural’ and ‘unnatural death’. There were very few relevant articles on the question of criteria for notification. The viewpoint reflects the experience of a busy full-time coroner, who has dual qualifications in medicine and law. The weaknesses of the paper are that there is no systematic review of international death notification systems, but there is reference to some that have been the subject of publication. In addition, the view has not been subject to peer debate.
The current guidance
Current guidance 14 is not in the form of regulation and comes from the ONS rather than the Departments of Health or Justice. There appears to be a difference in discretion of whether to notify or report a death in Scotland compared with England and Wales for no apparent reason. a The threshold is low – that certain matters may have caused or contributed to the death. It includes consideration of whether the death is unnatural, specifically identifies causes during operation and anaesthesia and includes deaths with unknown causes.
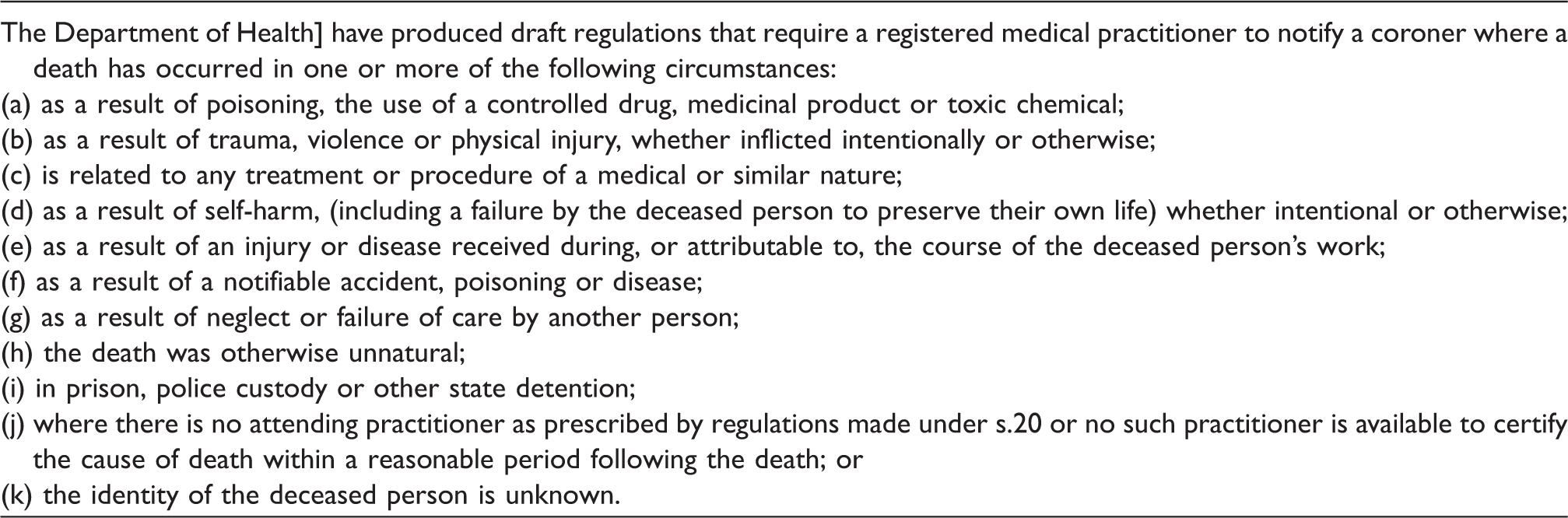
The proposed new regulations
Extract from Notification of Deaths to Coroner’s Regulations, Annex B, Introduction of Medical Examiners and Reforms to Death Certification in England & Wales: Consultation, Department of Health, March 2016.
Analysis
First, it is to be welcomed that guidance is to be replaced by regulation, which will hopefully promote clarity and consistency. There is an odd emphasis on poisoning in (a) and (f) as a separate category, which has Agatha Christie overtones, and must be extremely rare, whereas any substance that creates intoxication and thereby death will be reportable to a coroner. The category ‘notifiable disease’ may need clarification. Reporting deaths to the coroner are to be called ‘notifications’. This may be confusing to doctors, as the term is reserved for diseases notifiable to public-health officials. It presumably is meant to encompass occupational diseases but not tuberculosis and syphilis.
The clauses relevant to medical deaths in the existing ONS guidance advise reporting when:
the death may be due to neglect; the death occurs during an operation/anaesthetic; the death may be due to adverse effects of treatment or standards of care, or about which there is a complaint; or the cause of death is unknown.
The new formulation is that there is a duty to report deaths that have occurred in the following circumstances (selected for relevance to medical deaths):
as a result of neglect or failure of care by another person; related to any treatment or procedure of medical or similar nature; as a result of poisoning, the use of a controlled drug, medicinal product or toxic chemical; or the death was otherwise unnatural.
On first glance, it would appear that the threshold for referral has been raised from a possibility (‘may be due to’) to a probability (‘where death has occurred in the following circumstances … as a result of …’ etc.). Presumably, a doctor not being confident that something has caused death would be left not knowing the cause, and thus would report for that reason. With the guidance currently being advisory to report and the new process being a statutory duty to notify, it is suggested that its principal effect will be to prevent deaths that should be reported now but are not from escaping coronial scrutiny in the future.
With regard to operation and anaesthetic, the regulations seem to have sensibly extended notification to a range of medical interventions. The requirement to dispense with ‘being the subject of complaint for adverse effects of treatment’ would seem entirely sensible with the purpose of the coronial investigation, namely being to focus on causation, and not dependent on having a next of kin voicing concern. Coroners have a duty to consider the submissions of interested persons, which include the next of kin in every case. The phrase ‘related to any treatment or procedure’ would seem to be no less narrow and perhaps broader than ‘adverse effects’. It reflects a continuing realisation that procedures and interventions may be an appropriate subject of coronial consideration or investigation.
The inclusion of ‘neglect’ in the ONS guidance and proposed new regulations is ill conceived, as it cannot be sensible to ask doctors to notify deaths on the basis of applying a legal term of art, established in case-law,
b
which usually requires an expert opinion. It is not the same as neglect in ordinary English usage, nor has it any relation with negligence and is ill understood by doctors. The proposed wording also fails to recognise the inclusion of procurement from the legal definition and the range of other requirements. It would be better to create an easily understood criterion for notification, and leave it to the lawyers to hear submissions from interested persons and decide whether there is reason to suspect neglect. The suggested criterion is: deaths that may be due to a delay, omission or failure to procure or provide care by another person.
However, with the threshold of proof being raised from possibility (may have caused death) to probability (has caused death), this is not a satisfactory way of catching notifiable deaths that are ‘probably’ prima facie natural but require investigation. For example, take a cot death or sudden death in epilepsy or schizophrenia. A sudden unexpected death in infancy could be a murder, or from co-sleeping, or from an identifiable medical disease, but statistically is probably natural. Sudden unexpected death in schizophrenia treated with antipsychotics could be considered to be in category requiring notification and investigation, but if the doctor considers it only may rather than probably was related to antipsychotics, it might not be notified, whilst the public interest in pathological investigation is greater.
These unexpected deaths are routinely notified as possibly unnatural or as deaths unknown, and the new regulations should be strengthened to ensure they all continue to be reported. Either the word ‘may’ in the existing regulations needs to restored or perhaps a new criterion created: where a sudden death was unexpected and the diagnosis is uncertain due to the absence of a diagnostic test, or there is a possibility that the death could be unnatural, the death must be notified.
In cases of an elderly person falling and fracturing her hip and then dying of pneumonia after surgery, there would seem to be no more clarity in the new arrangements than the old. If a ‘but-for test’ is applied, many would be referred, as had it not been for the accident, the operation and complication of pneumonia would not have occurred. However, if only the immediate cause of death is considered, doctors might consider the death natural. The sharing of knowledge between medical examiner and coroner would be useful here. Many of these deaths might reasonably be given an underlying cause of death in 1c of Old Age Frailty, which arguably would mean that the death was natural in law.
The Department of Health consultation erroneously posits at 8.7 that ‘unnatural’ ‘is not defined … but is a term widely understood by those in both coronial and medical worlds to include any deaths that have not resulted from natural causes’.
A review of unnatural deaths 15 has clearly shown the complexity and difficulty in applying the scientific definition of ‘unnatural’ and underlying reasons for the differences between medical and legal meanings and between prima facie and final conclusions, having applied the law.
In Taiwan, 16 adverse effects of medical treatment were expected to be notified, regardless of whether there was malpractice, but a hospital record linkage study showed only 57% of unnatural deaths were reported. Doctors underreported complications of medical treatment. In Japan, 17 the inclusion of complications of medical treatment in reporting requirements of unnatural deaths was resisted when it became clear it might lead to police prosecution. Anecdotally, in England and Wales, there is a respectable body of opinion that regards death from complications of properly conducted treatment for disease as a natural death. It appears that these conclusions relate to the implications of notification rather than scientific classification.
The Japanese review reported that in Finland and Los Angeles, deaths from medical causes, whether related to malpractice or not, are notified for investigation. The proposals in England and Wales appear to continue the national and international trend of notifying all deaths where there is causation and then leaving it to the coroner to determine what requires investigation. It is interesting that in Victoria, 18 Australia, deaths following a medical intervention are only reportable and investigated if the death would not have been reasonably expected immediately before the procedure was undertaken. However, this is not the law in England and Wales.
In conclusion, it is not helpful to require doctors to use natural/unnatural as a criterion for notification. It is often impossible to say, as many deaths have multifactorial causation. Furthermore, some medically prima facie natural deaths may be found by a coroner to be unnatural in certain contexts, and vice versa. However, it is very useful to coroners for doctors to explain to the coroner whether the causes they certify are regarded scientifically as natural. This is especially so, since a medical qualification is no longer an eligibility criterion for coronial appointments, so that medical understanding in coroner’s offices may be scarce.
A notable omission from the list of statutory duties is that, in future, not knowing the cause of death, which is presumed natural, is not to become a duty to notify the coroner. Para 2.8 explains that if the doctor is unable to establish the cause of death, he or she will contact the coroner’s office. Medical examiners will be able to provide advice to a doctor in preparing an MCCD.
Conclusions
It is submitted that medical examiners will not replace the need for coroners to determine whether a notified death is unnatural, but coroners may have before them much better evidence, both clinical and pathological, before making the decision. In the future, with clear criteria for notification and guidance of death certification, concerns about the poor level of completion of MCCDs would hopefully be met by the national medical examiner scheme. It is hoped that doctors will then be assisted professionally to make greater use of the ICD coding and indicate the category in which the death occurs, whether signing a certificate or notifying the coroner. Fewer notifications to a coroner will be made where there is a prima facie natural death, but more may be reported which are adverse effects of treatment. The guidance available and the medical literature suggest that deaths that may involve an external agent as a cause of death should be reported to the coroner to determine if the death is unnatural, and it seems that is preserved in the new arrangements, subject to effective working between coroners and medical examiners. It is beyond the scope of this review to consider the logistical, resourcing, training, independence or other issues concerning implementation of the medical examiner scheme. Nor can this article discuss the key issue of the need for consistent and competent autopsy pathology. An effective and efficient service for those bereaved, where the death is notified to the coroner, requires much more than sensible notification criteria.
However, regulations about notification and the expertise of medical examiners should take cognisance of the difficulties found internationally in using whether the death is natural or unnatural as a criterion, being mindful of the very different meanings and applications of the term in the medical and scientific literature from those in the law.
Neither now nor in the future is there a need to equate the medical and legal understanding of what constitutes an unnatural cause of death. Doctors’ expertise is in understanding what is a prima facie natural death, not in what may be determined as an unnatural death by lawyers.
It is necessary to determine what needs to be reported or notified. If deaths relate to complications of treatment in current law, they need to be notified to the coroner, irrespective of whether they are judged as being natural. Doctors should continue to use the scientific understanding of what is a natural death, and where there are no other criteria to refer or notify, they should seek to certify. Especially in those cases, where causation is not fully understood scientifically, doctors should seek to achieve consensus in notifying the coroner of scientific understanding and possible causes, a process enhanced by the establishment of the medical examiner scheme. Where there is doubt about whether a cause of death can be certified as it is uncertain, it should be referred as unknown. How the coroner applies the law in determining whether the death is unnatural is a matter of legal judgment and requires assessment and/or investigation.
Whether there is current underreporting and whether the introduction of medical examiners will increase notification to coroners and how coroners decide which cases require investigation is beyond the scope of this article. However, it is clear that science, the law and national policy need to be considered as a whole in order to ensure that professionals can meet their statutory duties within available resources. It would be unwise to rely on these revised regulations and medical examiners to reduce the number of coronial investigations: it would be better to consider changes in coronial law such as the specified criteria for investigation of medical deaths in Victoria, if that were the goal.
Criteria for notification of deaths being laid down in regulations are to be welcomed as creating better consistency, avoiding unnecessary notification and greater certainty for doctors of their duties. However, they must be carefully crafted to recognise the complexities of language and definitions in medical and legal literature, not require doctors to perform legal tests and avoid relying on unnatural or natural as being the litmus test of notification.
Footnotes
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The author conducted the research and is the guarantor.
Funding
The author received no financial support for the research, authorship and/or publication of this article.