
Abstract
Introduction
This study investigated variables associated with methamphetamine-related deaths in Thailand.
Methods
This study used data obtained from methamphetamine-related autopsy cases over a six-year period from 2011 to 2016. From the data available during this period, considered variables included: demographic, toxicological and histopathological profiles. Methamphetamine blood concentration calculations and myoglobin immunostainings in kidney samples were also carried out. Statistical analysis and tests of significance were conducted using a paired-sample t-test, adopting a p-value of 0.05.
Results
A total of 61 methamphetamine-related cases were reviewed. Of several pathological findings, cardiovascular pathological findings were the most common. Cases were divided into a non-trauma group (n = 19; 31.15%) and a trauma group (n = 42; 68.85%), and it was found that methamphetamine blood concentrations of non-trauma cases were largely in therapeutic ranges. The differences between methamphetamine concentrations of trauma and non-trauma groups were not statistically significant (p > 0.05). Immunostainings for myoglobin in kidney samples were positive in two non-trauma cases, which is suggestive of methamphetamine-induced rhabdomyolysis.
Conclusions
Methamphetamine intoxication causes cardiac toxicity and can cause death. However, methamphetamine quantitation, autopsy findings and scene investigations are considered altogether in determination of cause of death due to many factors such as drug tolerances. Myoglobin immunostaining was found to be a useful tool in determining cause of death.
Introduction
From reports on drug-related deaths between 2008 and 2012 in Thailand, 81% of the deaths were attributed to methamphetamine use.1,2 This large percentage of methamphetamine-related deaths reflects the high prevalence of methamphetamine addictions and users in Thailand. Thus, further research of its affect as a cause of death are warranted.
Methamphetamine stimulates the central nervous and cardiovascular systems, which can cause various symptoms and pathologies resulting in death, for example acute myocardial infarction, cardiac arrhythmia, pulmonary oedema, intracerebral haemorrhage 3 and renal failure due to rhabdomyolysis. 4 Moreover, prolonged and continued use of methamphetamines has been seen to cause several pathologies, which may result in eventual death, including coronary atherosclerosis, left ventricular hypertrophy and cardiomyopathy. 3
The prevalence of methamphetamine-related deaths is high. Yet, there is a lack of research concerning methamphetamine deaths, especially in conjugation with methamphetamine blood concentrations. Hence, this study aimed to analyse autopsy data in cases where methamphetamine was found in the blood during autopsy. The results obtained from this study will be used to interpret the pathology related to methamphetamine abuse, as well as methamphetamine blood concentrations which may be considered in determination of a cause death. Moreover, this is the first study on this topic in Southeast Asian countries, which have one of the highest methamphetamine user rates in the world.
Methods
This analysis compiled medico-legal full autopsy report data from the Forensic Laboratory of the Faculty of Medicine, Ramathibodi Hospital, Mahidol University for the period 2011–2016. In all considered autopsies, tissue samples from the brain, aorta, heart, lung, liver, spleen, pancreas, adrenal glands and kidneys were examined grossly and histologically. Three main coronary arteries and the left main branch were serially sliced at a thickness of 5 mm and were examined for atherosclerosis. Both ventricular walls were also serially sliced at a thickness of 5 mm and were grossly and histologically examined for infarction and other diseases. At least two sections of the left ventricle and one section of the right ventricle were histologically examined. Femoral blood alcohol tests, as well as comprehensive drug screenings for 1700 drugs in femoral blood, including amphetamines, opioids, and cocaine, were performed in a laboratory which has received ISO/IEC 17025:2005 certification. The screenings made use of liquid chromatography (Bruker)-quadrupole time-of-flight mass spectrometry (Dionex Ultimate 3000), where the limit of detection (LOD) was 0.001–0.1 mg/L, depending on the type of drug. The blood alcohol concentrations were measured through use of an Agilent Technologies 7890 B Headspace gas chromatography/flame ionisation detector. Ethanol determination was performed using linear calibration with 10, 20, 50, 100, 200, 300, 400 and 500 mg% of aqueous ethanol solutions.
This analysis selected cases where methamphetamine was found in the blood. The used data included:
Demographic data and general information: sex, age, place of death, weight, height, cause of death, manner of death and circumstance of death; Pathological findings: coronary atherosclerosis, left ventricular hypertrophy, myocardial infarction, pulmonary oedema and liver pathologies such as fatty liver; and Presence of drugs and other substances in the blood.
The pathological findings were confirmed through histological examination. Coronary atherosclerosis was separated into three degrees of occlusion: mild (≥25% occlusion), moderate (≥50% occlusion) and severe (≥75% occlusion). Left ventricular hypertrophy was confirmed through the presence of hypertrophy myocytes. Myocardial infarction included acute and old infarction, while acute myocardial infarction was diagnosed if karyolysis was found with or without contraction band necrosis.
Cases with previous amphetamine or methamphetamine prescriptions were excluded from this study.
Between January 2015 and August 2016, upon positive detection of methamphetamine, methamphetamine quantitations were carried out using liquid chromatography–tandem mass spectrometry where blood concentration levels were divided into the following categories: therapeutic level (<0.1 mg/L), toxic level (0.1–2 mg/L) and lethal level ( > 2 mg/L). 5
Lastly, kidney tissues were collected from 18 cadavers to test for the presence of myoglobin casts in renal tubules using hematoxylin and eosin stains. Upon initial observation of cast presence, confirmations of myoglobin cast were carried out using myoglobin immunohistochemical staining. These were interpreted by an anatomical pathologist.
Statistical values were analysed using SPSS v22.0 (IBM Corp.) in order to obtain percentages, averages and standard deviations. A paired-sample t-test was used to determine the relationships of the data sets, with statistical significance held at p<0.05.
Results
A total of 61/2384 (2.56%) total autopsied cases tested positive for methamphetamine. Their ages ranged between two months and 69 years, with an average (excluding a two-month-old child) of 34.95 ± 9.65 years. With regards to sex, male cases totalled 47 (77.50%), with an average age of 35.4±10.4 years, while female cases totalled 14 (22.95%), with an average age of 33.4±6.2 years. No statistically significant difference was observed in average ages between male and female considered cases. The most frequently observed age range was 31–40 years, which constituted 47.54% of total cases. This was followed by the 21–30 years group, which accounted for 24.59% of total cases. Body mass indices were found to lie between 15.22 and 41.51 kg/m2, with an average value of 23.07±4.27 kg/m2, thus indicating values falling within the normal to overweight range. 6 The most frequent places of death were found to be the ‘place of residence’ (29 deaths; 47.55%) and ‘death on arrival or in hospital’ (19 death; 31.15%).
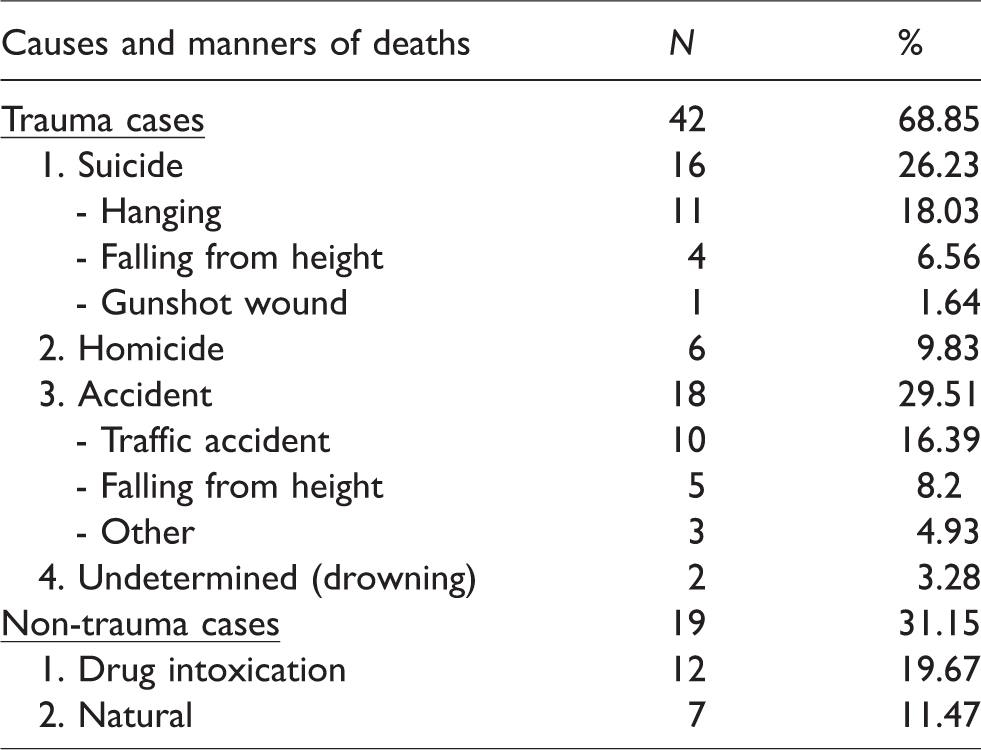
Causes and manners of death were divided into two categories based on the presence of trauma: the trauma group, comprising 42 (68.85%) cases, and the non-trauma group, comprising 19 (31.14%) cases. In one instance in the non-trauma group, sudden death was observed in a two-month-old child who tested positive for methamphetamine. Here, it is assumed that methamphetamine was ingested through breastfeeding, leading to intoxication, because the mother admitted that she had used methamphetamine before breastfeeding.
The causes/manners of deaths and corresponding quantity of each category are displayed in Table 1.
Causes and manners of deaths in methamphetamine-related deaths.
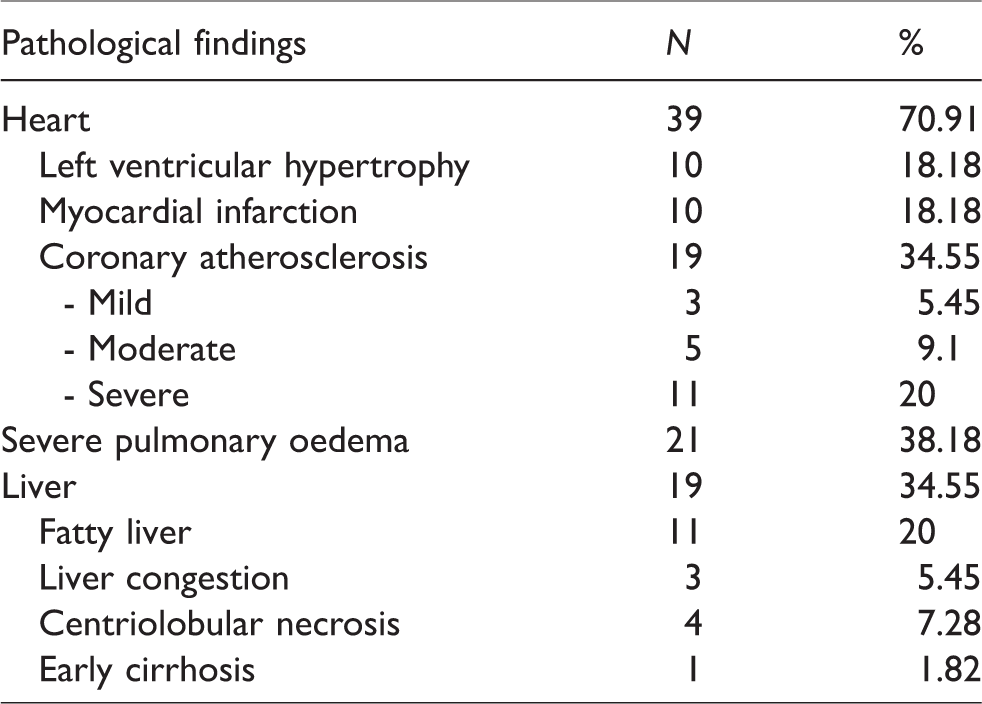
Pathological findings of the 55 applicable cases (not including cases of decomposition and the two-month-old child) can be found in Table 2.
Pathological findings in methamphetamine-related deaths.
No other substances were identified in the blood of 19 cases, while in the majority of cases (n = 42; 68.85%), other substances were present in the blood. Of these 42 cases, the most common substances present in the blood were found to be amphetamine (25 cases; 57.14%), ethanol (15 cases; 35.71%), tramadol (5 cases; 11.90%), benzodiazepines (5 cases; 11.90%), mitragynine (Kratom; 5 cases; 11.90%) and heroin metabolites (3 cases; 7.14%).
In all 15 instances where alcohol was found in the blood, blood alcohol concentrations ranged between 19 and 283 mg%. The majority of these cases (46.67%) were found to have concentrations in the 150–250 mg% range, which is a level of intoxication marked by the occurrence of anxiety, dizziness, confusion, impaired motor skills, nausea and vomiting.
Methamphetamine quantitation was conducted on 22 cases, 14 cases from the trauma group and eight from the non-trauma group. In the 14 trauma-group cases, methamphetamine blood concentrations ranged between 0.001 and 0.670 mg/L. In six of these cases, methamphetamine blood concentrations were found to be at toxic levels. In the non-trauma group, methamphetamine blood concentrations ranged between 0.013 and 0.570 mg/L, and seven of eight cases were found to be at therapeutic levels. Across both groups, no instances of lethal levels were found. Figure 1 shows the number of cases found to be at therapeutic levels (<0.02 mg/L) and toxic levels (0.1–2 mg/L).
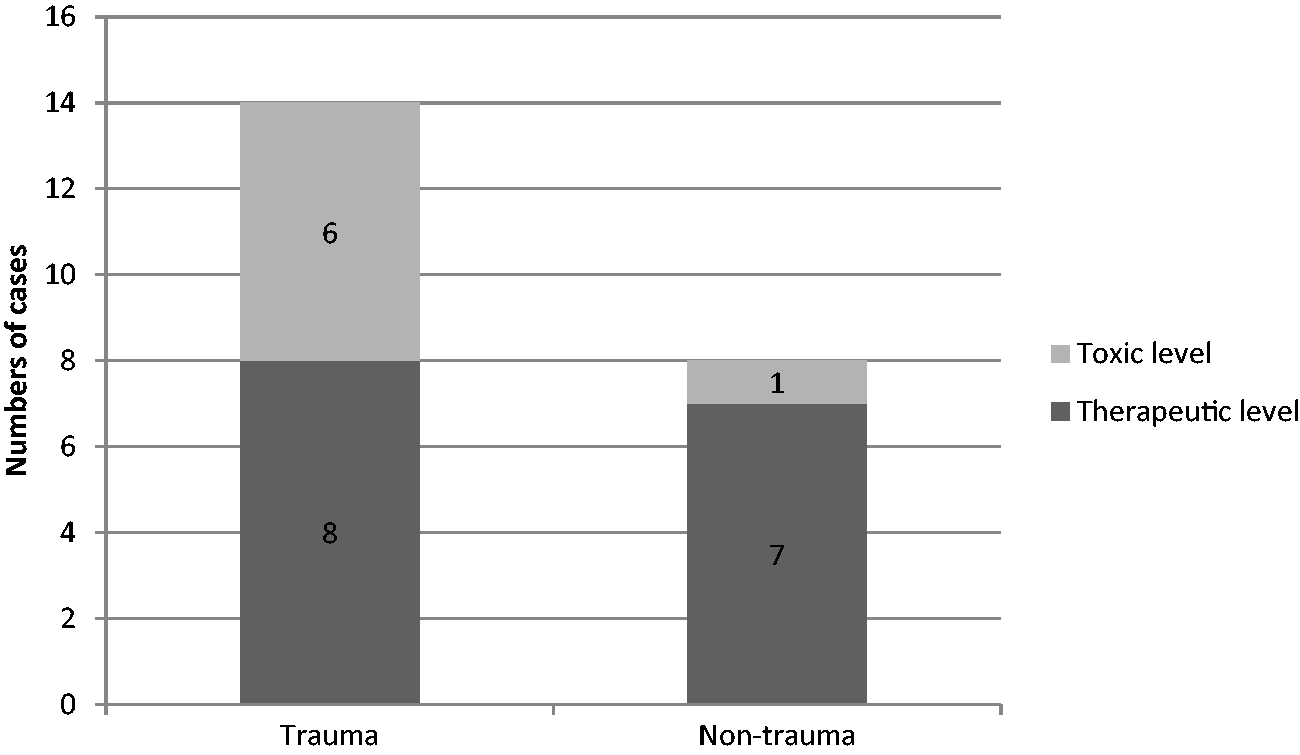
Numbers of cases in each concentration range.
These data, when analysed using a paired-sample t-test, revealed no statistically significant differences between the trauma and non-trauma categories (p > 0.05).
Investigation of myoglobin casts in 18 cases revealed two (11.11%) strongly positive identifications, as well as three (16.67%) positive identifications. The data of each case are shown in Table 3.
Data of each myoglobin-positive case.
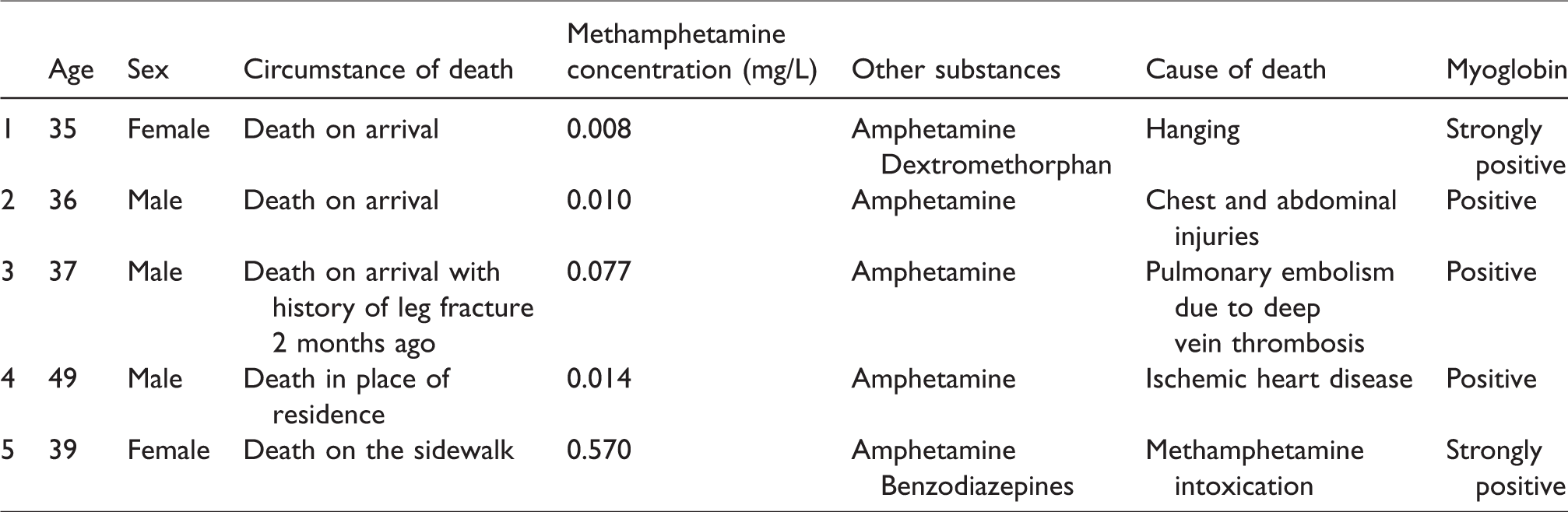
As can be seen in Table 3, cases 1–3 died on arrival, thus indicating that resuscitation was administered before death. The methamphetamine concentrations of these five cases were found to be between 0.008 and 0.570 mg/L.
Discussion
This study made use of cases in Ramathibodi Hospital laboratory, which services one part of the greater metropolitan area. This serviceable area comprises both low- and high-income areas, including government districts, commercial/market areas, residential areas and nightclub areas, which may represent common capital city or urban areas.
In reviewing causes and manners of death, it was found that traumatic accidents were the leading cause/manner of death, followed by accidental overdoses of methamphetamine. This trend has been confirmed in prior research, 7 which found that traumatic injuries in conjugation with methamphetamine use are more frequently found to be causes of death than intoxication or overdose. Moreover, it was found that suicide by hanging was one of the most common cause of death, which may be directly influenced by the hallucinogenic effects of methamphetamine and potential to prompt thoughts of suicide. Indirectly, this may be due to the fact that users contemplated suicide prior to consumption and were prompted to act on such contemplations by the stimulating effects of methamphetamine.
Cardiovascular pathologies were found to be most frequent, and this is in line with previous research,3,8 which showed that both short- and long-term use of methamphetamine were directly linked to the development of various cardiovascular pathologies. The occurrence of such pathologies is attributed to methamphetamine-induced sympathetic stimulation of the cardiovascular system. Here, the most prevalent cardiovascular pathology observed was coronary atherosclerosis where in one exceptional case, coronary atherosclerosis was observed in a 20-year-old. Coronary atherosclerosis is unusual in healthy and young populations, which may indicate that drug testing for young patients with coronary atherosclerosis should be done.
The second most common finding was severe pulmonary oedema. While the mechanism through which this occurs remains unclear, recent research has suggested that smoking toxic substances has been linked with greater microvascular permeability, 9 in turn leading to susceptibility to pulmonary oedema. As corroborated by previous research, 10 the most frequently observed pathology of the liver was fatty liver disease. The mechanism through which this occurs may be related to ethanol use, as ethanol was found in the blood of 15 (35%) cases.
In this study, methamphetamine was commonly used with other substances (68.85%), where amphetamine and ethanol were the most common substances found in the blood. This indicates that the use of addictive substances in conjugation with methamphetamine both directly and indirectly increases the likelihood of death. 3 The occurrence of users consuming more than one substance may be related to increased tolerance levels of users, who require increasing amounts of substances in order to sustain desired feelings.
Amphetamine was the most common substance because it is a metabolite of methamphetamine and/or it may be used in conjugation with methamphetamine to increase stimulant effects. It has been reported that methamphetamine is frequently sold in a mixed form with amphetamine. 11
Ethanol, when used in conjugation with methamphetamine, has been reported to cause tachycardia, as well as excessive oxygen consumption. These can lead to an increased risk of cardiac arrhythmia or other pathologies when compared to the use of methamphetamine alone. 12
Other common substances were found in the blood such as like benzodiazepines, which are reported to be used to counteract the effects of methamphetamine comedowns, often including manic behaviour, insomnia and/or hallucination. In doing so, users may engage in a stimulant–depressant cycle, which has been shown to increase harm greatly.11,13
Methamphetamine in conjugation with opioids (tramadol, mitragynine and heroin) can cause various effects, which largely depend on the amounts of each substance. Reports indicate that combinations of opioids and methamphetamine lead to greater amounts of stimulation than consumption of methamphetamine alone. 14 For example, it has been reported that mitragynine consumption in small quantities increases stimulation of the nervous system, while consumption in larger quantities causes opioid effects. 15 Thus, mitragynine consumption in small quantities in conjugation with methamphetamine may greatly increase stimulation, leading to death.
The methamphetamine concentrations found in both the trauma and non-trauma groups were very broad in distribution. However, the concentration levels of either group did exhibit overlap and consistency, as also reported in prior research. 3 In both groups, the exact level of toxicity was unidentifiable. This variability is observable in the trauma group where one case was able to operate a vehicle with blood concentration levels of 0.67 mg/L, while in the non-trauma group, an individual died with methamphetamine blood concentrations of 0.57 mg/L. While it is assumed that these differences stem from a difference in substance tolerance, 8 it is important to note that post-mortem blood may influence testing results due to drug redistribution affects, which, after death, can cause unequal quantities of drugs throughout the body.
In the non-trauma group, specifically cases with pre-existing heart conditions, previous research has found that the use of even small quantities of methamphetamine (within therapeutic levels) has been shown to be a contributing cause of death. 3 Such was the case in one particular instance in this study, where the methamphetamine blood concentration was found to be in the therapeutic range, with moderate coronary atherosclerosis in two arteries. In this instance, death may be directly attributed to methamphetamine use.
Within the trauma group, methamphetamine blood levels were largely found to be toxic, which means that methamphetamine at toxic levels may be an indirect or contributing factor of death, as reported in prior research. 7
Myoglobin analysis of kidney tissue was carried out to probe for the presence of rhabdomyolysis, which has been linked with methamphetamine use in previous research, purporting stimulation of sympathetic overactivity. This overactivity leads to muscle tissue breakdown and the development of non-traumatic rhabdomyolysis, which in turn leads to renal failure.16,17
In this study, myoglobin casts were positively identified in five cases, where, in three of five cases, resuscitation had been administered prior to death. This is an important consideration, as previous research has indicated that longer survival time is directly linked to the development of rhabdomyolysis, that is, through hypoxia, secondary muscle damage occurs, thus resulting in rhabdomyolysis. 18
Analyses of the causes of death in each positive myoglobin case are as follows:
Case 1: The subject committed suicide via hanging and thus experienced prolonged hypoxia. This coupled with the resuscitation survival time resulted in strongly positive myoglobin identification. Case 2: The subject died in a traffic accident, and it is assumed that rhabdomyolysis was sustained through direct muscle damage from the collision. It has been reported that the leading causes of death with indication of traumatic rhabdomyolysis are electrocution, trauma from a blunt object and trauma from sharp objects in order of prevalence.
18
Thus, sustained trauma coupled with resuscitation survival time resulted in positive myoglobin identification. Case 3: The subject died of venous thrombosis which dislodged in the leg and further thrombosed in the lungs. Past research has found that rhabdomyolysis is a complication which rarely happens due to venous thrombosis.
19
In addition to this, methamphetamine blood concentration levels were within therapeutic ranges, which may be sufficient to cause rhabdomyolysis. These indicate that this subject is assumed to have developed myoglobin casts due to the use of methamphetamine coupled with resuscitation survival time. Case 4: The subject died of myocardial infarction. It has been reported that striated muscle tissue cells can cause myoglobin casts in the kidneys and lead to renal failure and death.
18
In this subject, the heart muscle was infarct which is also striated muscle, so this can cause myoglobin casts. However, there was no report that this striated muscle tissue can cause myoglobin casts. Here, positive myoglobin cast identification is attributed to methamphetamine use. Case 5: This subject exhibited highly positive myoglobin. This individual’s blood contained toxic levels of methamphetamine, and the cause of death was reported to be methamphetamine intoxication. It is assumed that this individual died from methamphetamine use which stimulated the development of rhabdomyolysis. This instance was a key indication that immunohistochemical myoglobin staining is an instrumental method in analysing causes of death.
From the above, it can be concluded that myoglobin immunostaining was not a useful screening method for methamphetamine-induced rhabdomyolysis in instances involving resuscitation (cases 1–3), as the resuscitation survival times may cause rhabdomyolysis independent of methamphetamine use. Importantly, it was useful in non-trauma cases 4 and 5 in order to confirm that methamphetamine use/intoxication may contribute to the cause of death.
Conclusions
This research found that the majority of subjects who died with methamphetamine present in the blood were young fit male adults. Deaths were often related to cardiovascular pathologies, where such pathologies help to confirm the cardiac toxicity of methamphetamine, which can be used in current knowledge campaigns aiming at decreasing abuse incidence rates. In light of the fact that it is no easy task to determine the exact quantity of methamphetamine which is lethal, as there are many conflating factors, in determining the causes of death, one should not consider quantities of methamphetamine alone, given that autopsy reports and scene investigation can also provide important information. In addition to this, myoglobin immunohistochemical staining may be used in determining causes of death and identifying rhabdomyolysis as a cause of renal failure.
This research was limited by the number of considered cases, which resulted in a lack of statistical significance. In addition, it is also limited in identifying potential risk factors related to coronary atherosclerosis, for example whether the individual smoked, had hyperlipidaemia and so on. These will be areas of critical importance for future research.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.