
Abstract
Introduction
Defining extreme temperatures as the cause of death remains challenging. It is mostly based on circumstantial, macroscopic and microscopic features.
Methods
We retrospectively compared groups of cases of fatal hypothermia, fatal hyperthermia and non-extreme temperature-related deaths. We analysed specific histological findings, focusing on samples from the liver, pancreas and kidney.
Results
Between 1 January 2013 and 31 December 2016, 15 autopsies were performed for deaths related to extreme temperatures. They included 11 cases of fatal hypothermia (group A), four cases of fatal hyperthermia (group B) and eight controls (group C). Perinuclear hepatocyte vacuolisation was observed in seven cases of hypothermia, one case of hyperthermia and four controls. Pancreatic cytoarchitecture was well preserved in two cases of hypothermia, one case of hyperthermia and two controls. No particular microscopic feature was found in pancreatic samples. Renal epithelial tubular cell vacuolisation was observed in seven cases of hypothermia and one case of hyperthermia, while it was absent in all controls. Chromogranin A (CgA) was markedly positive in the pancreatic tissue of five cases of fatal hypothermia and one control, and mildly positive in one case of fatal hyperthermia. No significant p-values were observed for any comparisons (p > 0.05), except when hypothermia cases group were compared to the control group for the Armanni–Ebstein phenomenon test (p = 0.0078).
Conclusions
Although our study did not find a specific microscopic marker, hepatocyte vacuolisation, the Armanni–Ebstein phenomenon and pancreatic CgA positivity, taken together, may be useful tools to confirm hypo- and hyperthermia-related deaths, in addition to circumstantial and macroscopic findings.
Keywords
Introduction
Post-mortem diagnosis of deaths related to extreme temperatures is still challenging. Information available in the medical literature suggests that circumstantial, macroscopic, microscopic, biochemical, biological and immunohistochemical features can allow fatal hypothermia to be diagnosed, as listed in Table 1.
Major and minor morphological details in hypothermia and hyperthermia.

Regulation of the temperature of a human body and its maintenance at an average level of 37°C depend on an equilibrium between heat dispersal and generation. Hypothermia is defined as a core body temperature <35°C caused by a bodily loss of heat in excess of its ability to generate more. Post-mortem diagnosis of hypothermia-induced death is mostly based on non-specific features, including time of exposure, medication intake and phenomena such as ‘paradoxical undressing’ 1 and ‘hide-and-die syndrome’. 2
The phenomenon ‘frost erythema’, 3 which is a reddish-brown decolouration of exposed skin areas, particularly involving the extensor surfaces of large joints, as a result of dermal hyperaemia and oedema without red blood cell extravasation, supports a diagnosis of fatal hypothermia. ‘Wischnewski spots’ 4 are diffuse haemorrhagic spots that are variable in size and quantity. They are usually 1–2 mm wide, visible on gastric mucosa and, less frequently, on lower gastrointestinal tracts, and they are inconstant but pathognomonic findings of fatal hypothermia. Other macroscopic features include bloody discolouration of synovial fluid and skeletal muscle haemorrhages, particularly involving large muscles such as the iliopsoas.
Histological analysis supports the cause of death. Pancreatic cells necrosis with white blood cell infiltration, hepatocytes, adrenal gland cells, pancreatic cells, pituitary gland cells and renal cell vacuolisation, hypoxic cardiac changes and fatty degeneration of myocardiocytes and hepatocytes have been described in cases of fatal hypothermia. Fatty degeneration and vacuolisation of renal tubular cells as a result of hypoxia and fatty acid oxidative metabolism alteration – which is called the Armanni–Ebstein phenomenon –are strongly correlated with fatal hypothermia.5,6 Moreover, microscopic tissue infarction, secondary to small blood vessel occlusion, may be found, caused by red blood cells for haemoconcentration and increased levels of cold haemagglutinin. 7
Many research groups have performed immunohistochemical investigations, pointing out some findings which may also be helpful in supporting the diagnosis of fatal hypothermia. In hypothalamic neurons, for example, a reduced expression of chromogranin A (CgA) by immunohistochemistry was found compared to subjects who died from hyperthermia. 8 On the other hand, the adrenal medullary cells and pancreatic islets were markedly positive to CgA. 9 Other immunohistochemical findings included increased HSP-70 expression in renal tubular epithelium and in glomerular podocytes and increased cerebral cortex positivity to basic fibroblast growth factor (bFGF) and S100β detection.10,11 However, immunohistochemical tests have not been found be reliable diagnostic tools for the post-mortem diagnosis of hypothermia. Finally, biochemistry is a further useful tool for the diagnosis of fatal hypothermia. Increased blood levels of catecholamine and cortisol were found to be related to the stress caused by low temperature exposure. 12 However, catecholamine metabolite levels in urine, particularly metanephrine levels, were found to be more promising compared to serum levels because of the possibility of a post-mortem release of catecholamines by the adrenal glands. 13 Another hypothermia-related metabolic change is the enhanced secretion of insulin antagonist hormones, inducing an increase in fat catabolism and acetoacetate/β-hydroxybutyrate production. 14 Low blood and cerebrospinal fluid thyrotropin levels and increased blood free fatty acids and blood CgA levels have also been associated with fatal hypothermia.8,15
Hyperthermia is defined when the core body temperature rises > 40°C, without intrinsic inflammatory phenomena causing its increase. The post-mortem diagnosis of fatal hyperthermia is also based on non-specific phenomena, and it is mostly driven by time of exposure. The main findings on external examination are extensive hypostasis, early rigor mortis, delayed algor mortis and accelerated putrefactive phenomena. If death occurs rapidly, skin petechiae and visceral haemorrhagic spots are the most common macroscopic findings. If the subject dies more slowly, macroscopic findings include pulmonary and cerebral oedema associated with diffuse neuronal damage, subarachnoid and subdural haemorrhages and petechial haemorrhages, mostly in periventricular areas. 16 Moreover, polyvisceral congestion, especially involving the lungs and brain, can be found. On histology, brain involvement is represented by focal degenerative lesions in the cerebral cortex, basal ganglia and brain stem. Initial and diffuse alveolar damage in the lungs, without hyaline membrane or air embolism, is also a common finding in fatal hyperthermia. 17 In brain, lung and myocardial small vessels, the accumulation of neutrophilic white blood cells may also be observed. Other microscopic signs, which may suggest the diagnosis of hyperthermia-related death, are acute pancreatitis, focal liver necrosis, mostly centrilobular, associated with massive cholestasis. A peculiar feature of fatal hyperthermia is contraction band necrosis of myocardial cells, which is microscopically evident as thick and intensely eosinophilic bands that span the short axis of the myocardial cells.
In cases of fatal hyperthermia, immunohistochemistry has revealed a reduced expression of glial fibrillary acid protein in glial cells. Similarly, expression of S100β in white brain matter has been demonstrated to be reduced in this particular setting. On the other hand, S100β expression in the cerebral cortex has been shown to increase, together with neuronal single-stranded-DNA (ssDNA) and bFGF levels. CgA has also been shown to be more expressed in hypothalamic neural cells in case of fatal hyperthermia. 9 Research groups performing biochemical analysis in cases of hyperthermia-related deaths have revealed increased urinary levels of norepinephrine, increased dopamine levels in cardiac and peripheral blood, increased serum CgA and higher levels of epinephrine and norepinephrine in peripheral blood.
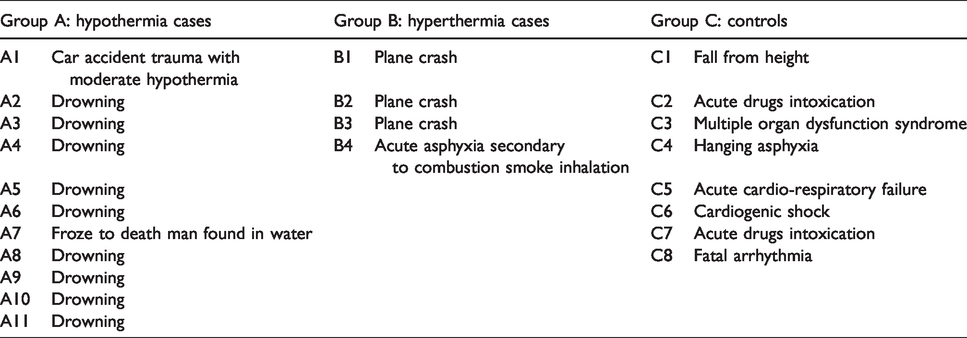
We present data regarding a retrospective study of 15 deaths related to extreme temperatures that were autopsied between 1 January 2013 and 31 December 2016. Subjects were divided into three groups: group A included 11 cases of fatal hypothermia, group B included four cases of fatal hyperthermia and group C comprised eight controls. Causes of death are shown in Table 2. The aims of this retrospective study were to compare the groups of cases of fatal hypothermia and fatal hyperthermia with the control subjects, who died for different reasons, and to correlate the cause of death with specific histological findings, focusing on samples from the liver, pancreas and kidney.
Groups and causes of death in the study population.
Methods
All cases of death related to extreme temperatures between 1 January 2013 and 31 December 2016 were retrospectively collected from the autopsy database of the Departmental Section of Forensic Medicine of the Università Politecnica delle Marche of Ancona, Italy. Based upon the particular mode of death, cases were assigned to three groups: group A – subjects who died from hypothermia; group B –subjects who died from hyperthermia; and group C – controls (Table 2). In the control group, subjects who died from different causes were included in order to help identify and interpret any histological and immunohistochemical differences between groups.
Tissue samples were fixed in formalin, dried, clarified, paraffin embedded and cut with a microtome in order to obtain sections 4–8 µm thick. Histological sections were stained with hematoxylin and eosin. Immunohistochemical stains were done with automatic tools (Autostainer Link48; Dako, Glostrup, Denmark), following the manufacturer’s data-sheet indications (Chromogranin A; 12200). Finally, the slides were observed with an optical microscope.
Fisher’s exact test was performed to assess the statistical significance of differences between the study series, relating to perinuclear hepatocyte vacuolisation, vacuolisation of pancreas gland cells and the Armanni–Ebstein phenomenon.
Results
The liver, pancreas and kidneys of subjects who died from hypothermia were well preserved. Liver samples showed a preserved microscopic structure in all cases of fatal hypothermia. Well-recognisable polyhedral hepatocytes with round nuclei were organised in cords around the centrilobular vein. On the other hand, in hyperthermia-related cases, organs were hardly recognisable because of diffuse autolytic phenomena. In particular, B1, B2 and B3 cases showed extensive hepatocyte autolysis, with markedly altered cellular structure.
Perinuclear hepatocyte vacuolisation was observed in seven (70%) cases of hypothermia, one (25%) case of hyperthermia and four (50%) controls (Table 3). Liver samples were not available in case A5.
Perinuclear hepatocytes vacuolisation.

Pancreatic cytoarchitecture was well preserved in two (33%) cases of hypothermia, one (100%) case of hyperthermia and two (100%) controls (Table 4). Pancreatic samples were not available in cases A2, A6, A7, A9, A11, B1, B3, B4, C1, C3, C4, C5, C6 and C8. Pancreatic samples in hypothermia-related deaths did not show any peculiar morphological features. Microscopic and cellular structures were preserved, with regular organisation of acinar cells around the lumen and well-recognisable islets of Langerhans. On the other hand, in samples collected in cases of fatal hyperthermia, cell architecture was markedly impaired for diffuse regressive and autolytic phenomena. In general, no particular microscopic feature was found in pancreatic samples.
Vacuolisation of pancreas gland cells.

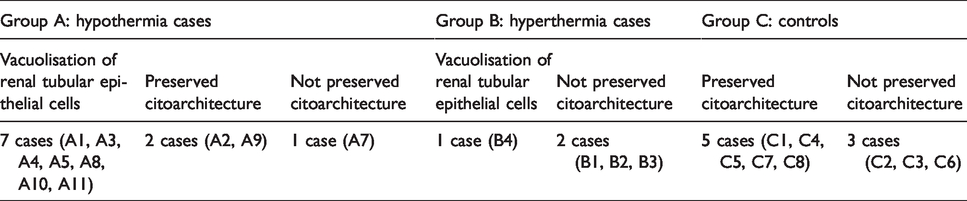
Renal samples collected in cases of fatal hypothermia showed a well-preserved cellular structure, with well-defined cortex and medullary areas. Renal epithelial tubular cell vacuolisation was observed in seven (70%) cases of hypothermia, and it was more evident in drowning-related deaths. Renal samples in cases of fatal hyperthermia showed extensive autolysis, particularly in death related to aeroplane accidents. Renal samples collected in controls were mostly well preserved, apart from three cases (C2, C3 and C6). One (33%) case (B4) of hyperthermia showed renal epithelial tubular cell vacuolisation as well, while it was absent in all controls (Table 5). In A6 and B3, the kidneys were not available.
Armanni–Ebstein phenomenon.
As regards immunohistochemical results, CgA was markedly positive in the pancreatic tissue of five (83%) cases of fatal hypothermia (see Table 6). In detail, all samples collected in drowning-related deaths showed the intense positivity of the islets of Langerhans to CgA, and the islets appeared clearly distinguishable. Mild positivity to CgA, with a diffuse spotty pattern in one (100%) case of fatal hyperthermia (B2), was also found. However, pancreatic microscopic structure was markedly altered and a well-defined demarcation of the islets of Langerhans was missing compared to samples collected in fatal hypothermia. CgA was also positive in one (50%) control (C7).
Chromogranin A (CgA) expression in pancreas gland cells.

Investigations show that our histological samples tested for analysis have a good correlation with hypothermia. No significant p-values were observed for any comparisons (p > 0.05), except when hypothermia cases were compared to controls for the Armanni–Ebstein phenomenon test (p = 0.0078).
Discussion
Despite the development of new tools and techniques and the constant research of novel markers by different study groups, the post-mortem diagnosis of fatal hypo- and hyperthermia remains challenging. Over time, several circumstantial, macroscopic and microscopic markers have been proposed and studied in extensive ways, but their accuracy and reliability have frequently been disappointing.
In detail, hepatocyte vacuolisation is a histological finding that has previously been described in the literature, particularly in fatal hypothermia. 18 Our experience strongly confirms these data. However, it seems to be a non-specific marker. In fact, this microscopic feature was also found in controls, in which exposure to low temperature as a cause of death was definitively excluded. Hepatocyte vacuolisation was also evident in one case of fatal hyperthermia and in drowning-related deaths. In our opinion, in these cases, low water temperature may explain the cellular modification, even although it was not the primary cause of death. Therefore, hepatocyte vacuolisation may be considered an additional element which has to be integrated with other circumstantial, macroscopic and microscopic features. In fact, hepatocyte vacuolisation may also be observed as a common form of steatosis (i.e. macro- and/or micro-vesicular pattern in alcoholic liver disease) in patients affected by liver disease.
Pancreatic changes have been described in association with hypothermia: focal or diffuse pancreatitis, haemorrhagic pancreatitis, patches of fat necrosis over the surface of the organ, haemorrhages and focal or diffuse interstitial infiltration of leucocytes. Further, for pancreatic samples, our data confirm what has already been shown in other studies because no specific histological marker was seen.19,20 Therefore, post-mortem artefacts (necrosis), visible in the pancreatic parenchyma, may be observed after non-forensic autopsies due to lytic enzymes rather than hypo- or hyperthermia.
Our renal samples also confirmed how important the Armanni–Ebstein phenomenon is in fatal hypothermia. As previously explained in other works,1,6,21 lipidic vacuolisation in the renal epithelium may be explained by hypoxia and altered fat acid oxidative metabolism. 22 Since this feature was absent in all controls, the Armanni–Ebstein phenomenon seems to be a useful marker to confirm post-mortem diagnosis of fatal hypothermia, but not to exclude it.
Immunohistochemical analyses focused on searching for positive CgA in pancreatic samples. A surprising finding was an intense positivity to CgA in all drowning-related deaths. CgA expression previously created a strong interest in the forensic science community.9,23 However, we are not aware of published data correlating CgA expression to drowning deaths. This phenomenon may be explained by a marked neuroendocrine stress response to cold water and might therefore also be related to fatal hypothermia, playing an important role in determining the cause of death. The only case in which CgA expression was absent involved death related to a car accident in which mild hypothermia occurred following death from other causes.
In cases in which death occurred secondary to aeroplane accidents, the quality of pancreatic samples was compromised. Therefore, extremely limited considerations can be made relative to fatal hyperthermia, as positivity to CgA may be considered an incidental finding. However, stress-related neuroendocrine system activation cannot be completely excluded. An important issue is the accelerated autolytic and putrefactive phenomena due to exposure to high temperature which compromised the reliability of most immunohistochemical analysis. However, the stress-related aetiology of the neuroendocrine response makes CgA positivity non-specific, since any potential pre-mortem cause of stress may result in increased pancreatic expression of CgA.
In conclusion, even although no specific microscopic marker was found in our study, hepatocyte vacuolisation, the Armanni–Ebstein phenomena and pancreatic CgA positivity may together be useful tools to confirm hypo- and hyperthermia-related deaths, in addition to circumstantial and macroscopic findings. In our opinion, the key may be to focus on other stress-related markers, such as catecholamines, urine and blood cortisol, ketones and CgA in cerebrospinal fluid. This phenomenon should be further studied with larger samples in order to help improve diagnostic accuracy and confirm results.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.