
Abstract
When analysing bodies recovered from a watery environment, all manners of death, a variety of causes of death and the possibility of body disposal have to be considered. Unclear circumstances of death, unidentified victims and body decomposition may hamper a forensic investigation. The lack of specific and sensitive drowning-related autopsy findings and post-mortem blood alcohol levels (blood alcohol concentrations (BACs)) may also lead to erroneous conclusions. We reviewed the autopsy records for all bodies recovered from water in Friuli, northeastern Italy, over a 28-year period, focusing on death circumstances, autopsy findings and blood alcohol levels. Some unusual cases were examined separately. Among the 69 cases, there were 32 accidents, 13 suicides, 4 homicides, 6 natural and 14 undetermined deaths. Causes of death included 51 drownings, 6 undetermined, 5 cardiac deaths and 7 non-drownings. Six deaths in a bathtub and one diving-related death were also included. Acute alcohol intoxication was ascertained in 22 of 40 victims. Some significant limitations in the approach to water-related deaths have been highlighted: although emphysema aquosum and external foam resulted to be the most reliable indicators, a determination of drowning based exclusively on autopsy findings cannot be ascertained with certainty. Furthermore, it was found that the standard definitions of wet and dry drowning in the literature differ widely from a morphological perspective and this may lead to misleading outcomes. Post-mortem BAC changes have been critically analysed only in bodies found in cold water, and, in the absence of an alternative to blood specimens, the use of pre-set cut-off values is still necessary.
Keywords
Introduction
The forensic investigation of corpses recovered in or near water focuses on victim identification, the evaluation of the post-mortem submersion interval (PMSI) and the determination of the cause and manner of death and therefore relies on close collaboration between the forensic pathologist and other agencies.1,2 The pathologist also has to determine whether the victim was alive on entering the water and why he/she was unable to self-extricate. 3
The morphological diagnosis of drowning is complex, since autopsy findings related to drowning are not specific and many deaths are still prematurely labelled as ‘accidental drowning’, leading to erroneous conclusions.1,4–6
Misleading conclusions in the determination of the cause and manner of death in water-related deaths may also arise from an inaccurate interpretation of alcohol concentrations in the victim's body: ethanol intoxication is one of the leading risk factors in adults for unintentional drowning and it is also frequently reported among suicides and murders by drowning, but detected levels may be altered by post-mortem phenomena.7–10
The aim of this study was to review the records for all the victims of water-related deaths whose corpses underwent autopsy in Friuli, northeastern Italy, in the period 1993–2020. Deaths in bathrooms and diving-related deaths were included. The research focused on the identification of the potential pitfalls at autopsy and in the interpretation of detected blood alcohol levels, which may interfere in the determination of the cause and manner of death. Moreover, four peculiar cases were separately analysed in order to illustrate some distinctive complex scenarios which may be encountered in the approach to bodies recovered from watery environments.
Materials and methods
A retrospective analysis reviewed all the post-mortem records held by the Department of Medicine/Legal Medicine of the University of Udine from 1993 to 2020 (n = 6919). A text word search using 41 terms associated with water-related deaths was carried out and all the records for that type of death were systematically examined. Only cases undergone complete autopsy were included in the study.
Victims were analysed according to the cause and manner of death (accident, suicide, homicide or undetermined), which had been established by the forensic pathologist, since it was specifically requested by the judicial authorities. The circumstances of death, suicide notes and body locations were recorded and the analysis of the individual profiles of the victims included their sex, age, medical and psychiatric history and any previous suicide attempts.
Submersion intervals were classified into three categories: <24 h; from 1 day to 7 days; over 7 days.
Autopsy findings included:
the presence of external foam when the corpse was recovered; typical signs of drowning affecting the respiratory tract and other pathological findings; and the degree of putrefaction when the body was recovered and when the autopsy was performed, and the interval between the two. absent; beginning: incipient green discolouration; proceeded: extensive discolouring and veins visible; high degree: putrefaction gas bloated and adipocere; skeletonization. a peripheral blood alcohol concentration (BAC) >0.2 g/L in the absence of putrefaction or ethanol detected in an alternative source other than blood (vitreous humour or urine, for example); and a peripheral BAC >0.6 g/L in putrefied bodies.
Putrefaction was classified into five stages, in part using the method proposed by Schneppe et al.
11
:
Toxicological data and diatom tests were included if available. Acute ethanol intoxications were determined on the basis of the criteria adopted by Lucas et al.
12
:
Ethanol levels were determined by headspace gas chromatography.
Statistical analyses were performed using the IBM SPSS software platform. Continuous variables (age and alcohol levels) were reported as median and range (minimum–maximum), while categorical variables were summarized as absolute frequencies and percentages. Fisher's exact test was used to investigate associations between categorical variables. Statistical significance was set at p < 0.05.
No ethical approval was required for this retrospective study, because the data were not related to living persons but to decedents (data normally available from autopsy records of our institute).
This retrospective study was conducted as a part of a PhD research thesis at the University of Udine, Department of Medicine, Section of Forensic Medicine, which was approved by the University of Udine on 30 June 2020 (Rectoral Degree 585/2020, protocol number 0036224).
Results
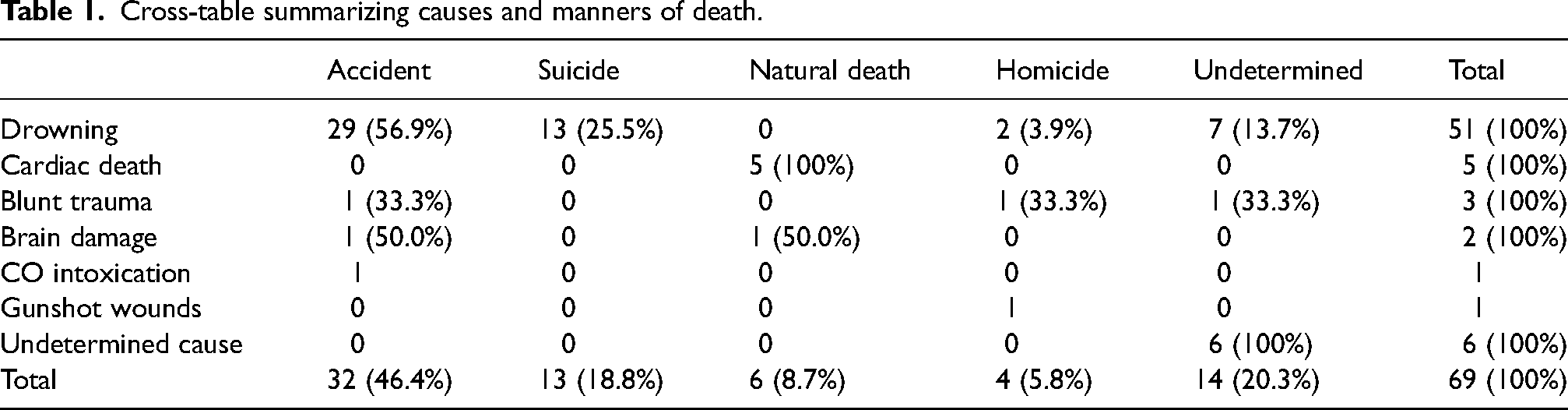
A total of 336 (4.86%) cases of deaths in or near water were identified. Among these, 69 underwent complete autopsy; data concerning causes and manners of death are summarized in detail in Table 1. The cause and the manner of death were not determined in 6 and 20 cases, respectively.
Cross-table summarizing causes and manners of death.
In only one instance could the identity of the victim not be ascertained: this concerned the recovery of the skull of an adult male in 50-cm-deep seawater. All the other victims were visually recognized, with the exception of two who were identified by their dental records.
Victims’ individual profiles and acute intoxication
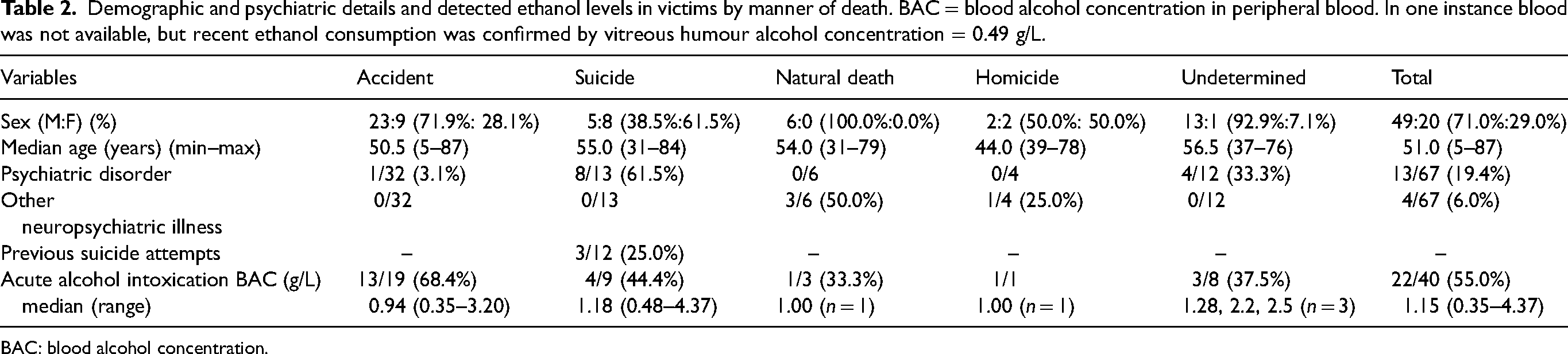
A clear male prevalence was observed and the median age was 51.0 years. The youngest victims were three male children (two aged 5, one aged 6) who drowned at the seaside, but could not be resuscitated.
Thirteen individuals were found to have been affected by psychiatric disorders. An overwhelming prevalence was observed among suicide victims, with five cases in which clinical depression had been diagnosed, whereas 6 victims (4 accidents, 2 undetermined; ratio M/F: 2/1) suffered from chronic alcohol abuse.
Two individuals who died from natural causes were affected by intellectual disability and one had Alzheimer's disease. An elderly woman drowned by her husband was suffering from severe cognitive impairment and was wheelchair-bound. After killing his wife, the man, suffering from depression, in turn, drowned himself. 13
Ethanol was detected in 40 cases, with 22 victims being in a state of acute ethanol intoxication.
The highest blood alcohol concentration (BAC) was detected in a case of complex suicide (see case 2).
Two victims were found to have been under the influence of cocaine: one of these was a 51-year-old man who was the victim of a complex suicide in his boat at sea, due to liquefied petroleum gas inhalation and drowning. 14
Details are summarized in Table 2.
Demographic and psychiatric details and detected ethanol levels in victims by manner of death. BAC = blood alcohol concentration in peripheral blood. In one instance blood was not available, but recent ethanol consumption was confirmed by vitreous humour alcohol concentration = 0.49 g/L.
BAC: blood alcohol concentration.
Circumstances surrounding death
Six suicide victims explained their motives (2 suicide notes, 1 text message and 3 verbal declarations).
Fourteen (20.3%) victims underwent resuscitation, but only in one instance, spontaneous circulation was restored, though the victim (a 50-year-old woman) remained unconscious and died in hospital due to brain damage as a result of hypoxic encephalopathy six days later. In the remaining 13 cases, resuscitation attempts resulted to be unsuccessful.
Six deaths occurred in bathtubs (4 males, 2 females; age range: 29–76 years, median = 36 years) and 4 were attributed to drownings (3 of them accidental). In one instance, toxic HbCO levels were detected in the victim's blood (73%) and in one case the cause of the death was attributed to hypertrophy of the left ventricular myocardium.
Autopsy findings
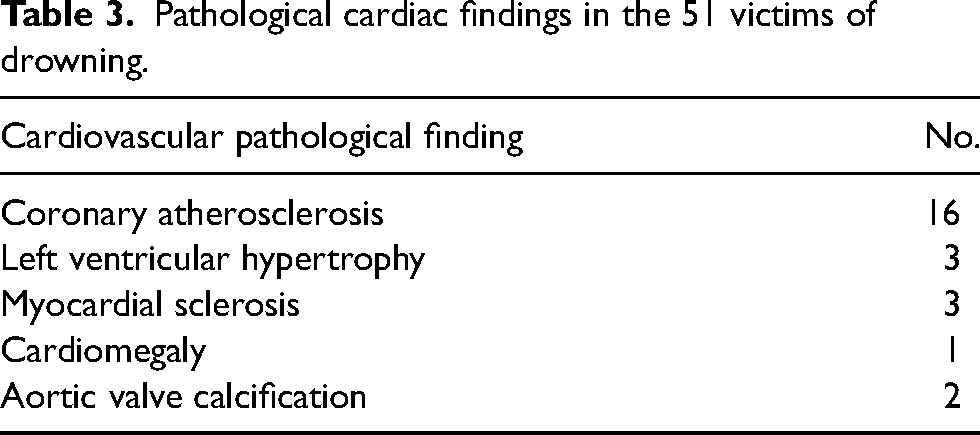
Fifty-one out of 69 cases (73.9%) were classified as drownings. Among them, non-fatal cardiovascular pathologies were observed in 22 instances (details in Table 3).
Pathological cardiac findings in the 51 victims of drowning.
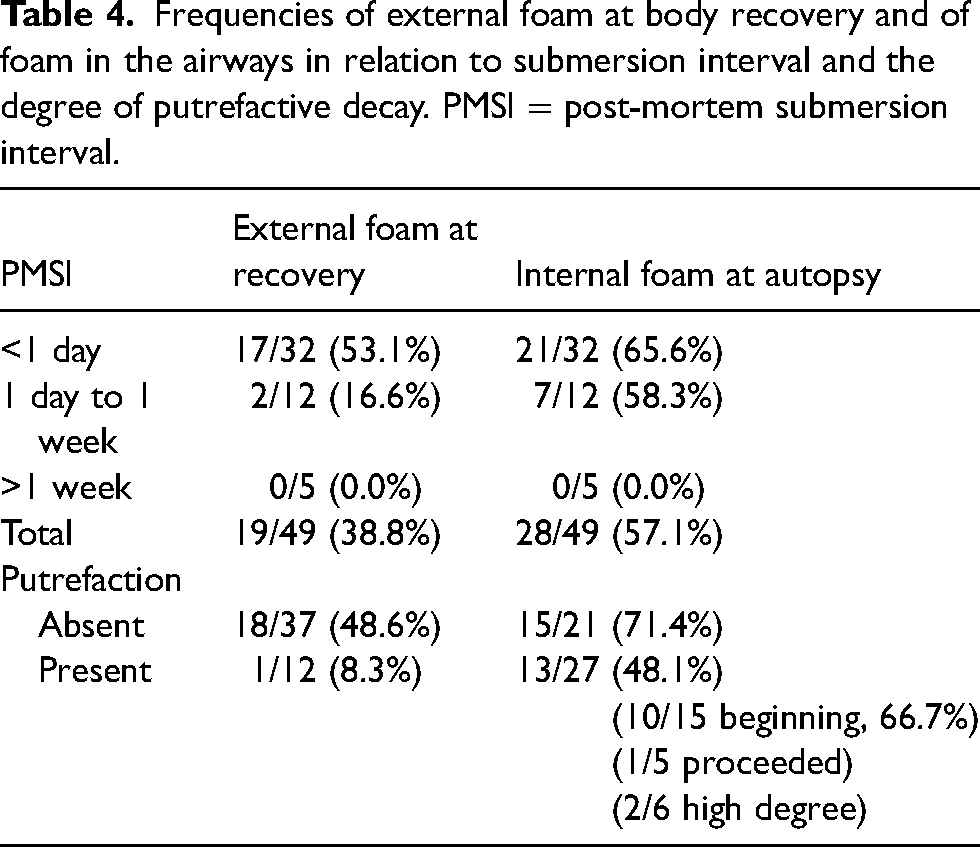
Drowning and non-drowning victims were compared for evidence of external foam when the bodies were recovered and froth in the airways revealed during autopsy. The external foam was noted in 19 of 49 (38.8%) cases of drowning and in 1 of 18 (5.6%) non-drowning cases (p = 0.008), whereas froth in the airways was observed in 28 of 49 drowning victims (57.1%) and in 2 of 15 (13.3%) non-drowning victims (p = 0.003).
These findings were analysed in drowning victims with regard to the submersion interval and the level of putrefactive decay of the body at recovery and at autopsy (Table 4). Twelve of 49 (24.5%) bodies were affected by putrefactive changes on recovery (5 beginning, 3 proceeded, 3 high degree, 1 adipocere, and 1 case of external froth observed in a corpse characterized by high degree putrefaction), and 27 of 49 (55.1%) at autopsy (15 beginning, 5 proceeded, 6 high degree, and 1 adipocere).
Frequencies of external foam at body recovery and of foam in the airways in relation to submersion interval and the degree of putrefactive decay. PMSI = post-mortem submersion interval.
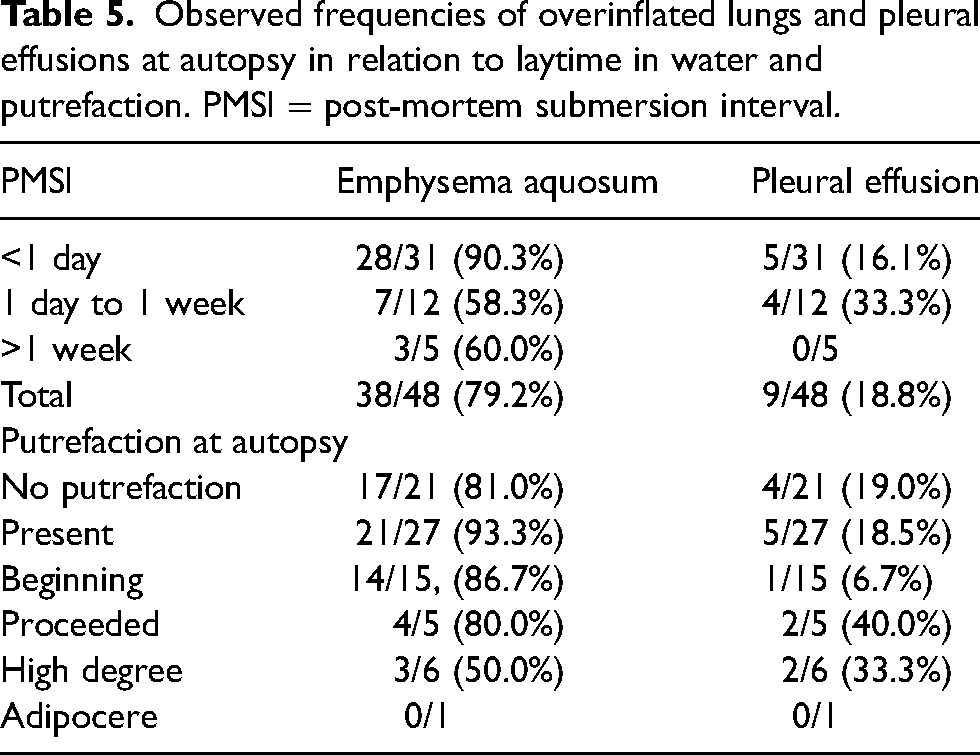
Overinflated lungs and pleural effusion were analysed in 48 drownings and 15 non-drownings: the former was observed in 38 drowning and 2 (13.3%) non-drowning cases (p-value < 0.001), the latter in 9 (18.8%) victims of drowning and in 1 (6.7%) non-drowning victim (p-value = 0.43)
Their frequencies in drowning victims with regard to PMSI and putrefactive decay have been reported in Table 5.
Observed frequencies of overinflated lungs and pleural effusions at autopsy in relation to laytime in water and putrefaction. PMSI = post-mortem submersion interval.
Gastric mucosa lesions were reported in only 4 of 68 cases (5.9%, 2 drownings and 2 non-drownings), and subpleural haemorrhages (Paltauf's spots) in 3 of 51 victims of drowning (5.9%).
Particular cases
Case 1
The non-putrefied naked body of a 43-year-old woman was found in a drainage ditch (water depth = 0.15 m). Minimal abrasions were observed and those did not involve the neck region and were not consistent with signs of struggle. Three rubber objects in the vagina were noted at autopsy. Peripheral BAC was 1.28 g/L, COHb and diatom tests were negative and chronic emphysema was observed in the lungs at histology. The cause and the manner of the death were recorded as undetermined.
Case 2
The non-putrefied body of a 56-year-old diabetic woman was found on a river bank. Insulin pen needles, an empty bottle of whisky and a farewell letter were found at the death scene. At autopsy, froth exuding from the nostrils, mouth and airways and overinflated lungs were noted. Femoral BAC was 4.37 g/L. Circumstantial data and death scene findings suggested a suicide.
Case 3
The severely putrefied body of a 55-year-old woman with a history of suicide attempts by wrist cutting was found submerged in a pond. Stones (5 kg) were found in the victim's stockings and a suicide note was found at the scene. At autopsy, there were no typical signs of drowning but diatoms were detected in the spleen. BAC was 0.48 g/L.
Case 4
A 31-year-old male was found dead in the bathtub. He was affected by pulmonary sarcoidosis, colon cancer with ileostomy and liver metastasis and had refused to undergo chemotherapy. The door of the bathroom was locked from the inside and the man's parents called for help. The victim was in the habit of self-treating with unconventional anticancer therapies, including warm baths (water temperature = 40°C). He had manifested suicidal intentions in the past. There were no external signs of violence and toxicology was negative. The manner of death could not be clearly categorized either as an accident or a suicide.
Discussion
A critical consideration in this study concerns the low number of water-related deaths which underwent complete autopsy and toxicological analysis, because they can only be requested by the judiciary. Since suicide and attempted suicide do not constitute an offence under Italian law, there is little interest in investigating the effective cause of death, once third-party involvement in the death of the victim has been ruled out. This factor has led to a reduced number of analysable cases, with an imbalanced sample size of drowned and not drowned victims.
Drowning represents a relevant cause of death, with more than 300,000 cases in 2015 and a mortality rate in Italy of 0.81 per 100,000 individuals.8,15 However, a wide variety of scenarios may be encountered by the forensic pathologist in cases of corpses found in water. 16
Autopsy findings related to drowning
The frequency of observed external and internal foam, with the highest prevalence in the time interval of <24 h after death was in line with values observed in other studies. Moreover, it was not in accordance with the much higher frequency (90%) of external foam at body recovery observed in a similar Italian study.11,17,18,19
Corpses with a PMSI between 1 day and 1 week did not show a significantly lower presence of frothy fluid in the airways when compared with those with a PMSI shorter than 24 h; moreover, no significant differences were measured comparing bodies affected by ‘beginning’ versus ‘absent’ putrefaction.
These outcomes are in contrast with a recent study which, at autopsy, showed a marked decrease of foam in the airways in bodies with laytime in the water of between one day and one week when compared with those which had been submerged for <24 h. 11
Aqueous emphysema and external foam proved to be the most specific and sensitive markers of drowning. However, prolonged submersion and putrefaction may reduce evidence of aqueous emphysema more than froth in the airways.
Many authors have raised the issue of differential diagnosis between aqueous emphysema and lung changes due to chronic pulmonary disease and those generated by post-mortem penetration of liquid into the lungs of submerged victims dead from causes other than drowning: histological examination may be helpful in distinguishing aqueous emphysema from the former, but is less helpful in distinguishing it from the latter.2,20,21
Pleural effusion is clearly not specific to drowning, nor is it sensitive. Furthermore, its reliability is also affected by post-mortem changes in bodies subjected to prolonged submersion and advanced putrefaction, caused by the trans-thoracic leakage of pleural liquid.22–25
Gastric mucosal tears and subpleural spots were observed in a very low percentage of cases, confirming that they are of little value in investigating alleged drowning victims. 11
Wet and dry drowning: An unclear morphological definition
Another critical issue in the morphological determination of drowning is the classification into ‘wet’ (or typical) and ‘dry’ (atypical) drowning, with the former representing the large majority of cases and the latter accounting for only 10% to 20% of all alleged drowning cases. The definition of dry drowning is clear, being described as ‘a drowning process which has been shortened by water-independent factors’ 11 or ‘drowning without significant aspiration of fluid’ and has been explained by mechanisms such as sudden laryngospasm, vagally-mediated cardiac arrest triggered by the contact of liquid with the airways, with old age and pre-existing cardiac comorbidities being a risk factor.2,4,11,26 The morphological aspects of dry drowning at autopsy refer to the absence of any evidence of fluid aspiration, but the literature shows that the classifications provided by several authors are not concordant. Shkrum 4 defined dry drowning as the absence of signs of wet drowning, such as pulmonary congestion and froth in the respiratory tract; Lunetta and Modell2 equated the concept of ‘dry lungs’ with an absence of signs of aqueous emphysema, whereas according to Saukko and Knight 26 the appearance of the lungs would be ‘normal in all aspects’. On the other hand, Schneppe et al.11 in their recent article reported that external foam at recovery, foam in the airways at autopsy, emphysema aquosum and Paltauf's spots had been observed in 19%, 82%, 97%, and 6% examined cases of dry drowning, respectively. Stephenson et al. 27 raised the question of whether dry drowning could be categorized as death due to upper airway obstruction, since there would be no fluid aspiration, while Van Beeck et al. 8 suggested avoiding the distinction between wet and dry drowning altogether.
Other researchers focused on lung weight to distinguish drowning from non-drowning cases and to distinguish wet from dry drowning, using a cut-off value of 1000 g (combined lung weight) or of 500 g per lung.12,22,28 This approach turned out to be extremely arbitrary and misleading, if only for the fact that lung weight can differ widely between individuals, with some authors pointing out that only a combined lung weight of >2500 g could be significant in differentiating drowning from non-drowning cases.2,4,17,29
To sum up, a clear morphological definition of dry drowning is currently not available, causing a risk of misinterpretations.
The issue of the interpretation of post-mortem alcohol levels in submerged bodies
More than half of the victims were under the influence of ethanol, although the method used to ascertain a condition of acute ethanol intoxication was conservative. Illicit drugs, on the other hand, were detected in significant concentrations in only two bodies. Post-mortem endogenous ethanol production (PMEP) may lead to an overestimation of the real BAC at the time of death in submerged bodies. A correct approach, therefore, should at least include the comparison of BAC, urine and vitreous humour alcohol concentrations when possible. 30 In the absence of an alternative to blood specimens, cut-off times between death and sampling for alcohol analysis and exclusions of cases with low BACs (e.g., lower than 0.5 g/L) have been suggested to avoid false-positive results.31,32
A recent study showed that the impact of PMEP on epidemiological research on drowning and alcohol is limited and that the use of over-rigorous cut-off criteria may exclude a considerable number of alcohol-positive drownings. However, this study was carried out in Finland and its authors suggested that similar research be carried out in other settings with a higher ambient temperature and protracted post-mortem submersion times. 30
Our results were not in contrast with the current literature, confirming that alcohol is a leading risk factor for water-related fatalities.7,12,33
Considerations on the peculiar cases
Case 1 was consistent with body concealment. The disposal method was ranked as grade 1 (simple abandonment in an isolated area), likely to prevent retrieval of the corpse (‘defensive behaviour’) and the manner and the cause of the death of the deceased could not be clearly identified.34,35
On the other hand, the detection of the rubber objects in the vagina of a naked body suggested a sexual motive, one of the most frequent motives behind homicides with subsequent concealment of the corpse. 35 Non-lethal concentrations of ethanol, as frequently observed in this type of incident, were identified and they were suggestive of a condition of euphoria and diminished attention span, judgement and control. 36
The manner of death in case 2 was consistent with a complex suicide. The role of ethanol and drugs in these types of fatalities has widely been the object of debate, with many authors affirming that they are often taken to avoid pain and suffering and not for self-killing.37,38 Another crucial point was the history of diabetes mellitus of the victim, since high glucose blood levels can promote PMEP in a decomposed body. 39
However, BAC higher than 3.5 g/L can turn out to be lethal, but it has been rarely encountered in cases due exclusively to PMEP. Furthermore, the victim had been seen alive <24 h before the recovery of the body and changes due to body decomposition were not noted, making the hypothesis of PMEP unlikely.40–43
The cause of death was attributed to drowning, but the possible role of injected insulin as a third suicide method could not be ruled out, although it could not be confirmed by toxicological analysis.
With regard to case 3, the recovery of weights in submerged bodies requires differentiation between suicide, homicide and/or body disposal: it is necessary to ascertain whether the victim might have attached weight or ropes alone and to look out for other signs of violence on the body, but these could have been concealed by advanced decomposition.1,2,44,45
On other hand, a diatom test is still not regarded as standard practice in an investigation of water-related deaths and it is still not accepted in a court of law as a way of providing a diagnosis of drowning. It can only support the forensic pathologist in case of an inconclusive autopsy.1,2,46,47
Although a history of previous suicide attempts should not rule out homicide or accident death, the finding of a suicide letter and the circumstantial evidence were strongly suggestive of suicide. 48
The reason for using weights in suicidal drowning is to maximize the chances of death: this technique should be differentiated from complex suicide, since only one self-suppressive method is involved. 44
In the approach to deaths in a bathtub (case 4), the possibility of other causes of death other than drowning, all manners of death and the possibility of body disposal must be considered.49,50
It is important to check the presence of electrical devices and of signs suggestive of CO poisoning, as well as to measure ambient and water temperature: hot water might be involved in torture by scalding and cold water might be indicative of a delayed rescue attempt. 1 Moreover, bathing in hot water may account for a sudden decrease in blood pressure, which may bring about cardiopulmonary arrest, or may be responsible for the development of fatal arrhythmias, such as ventricular tachycardia or extra-systole, especially in elderly people or in subjects affected by hypertension. 51
Checking whether the victim's clothes and the floor surface near the suspected water are dry or wet can provide further important information.1,52
It is important to underline that crucial factors contributing to drowning in a bathtub include alcohol or drug intoxication, pre-existing cardiovascular disease and a history of epileptic seizures, with lip contusions and bite tongues representing possible evidence of seizures.4,53
The presence of signs of violence must be looked for, whereas it must be considered that foam in the airways may be noted in deaths due to causes other than drowning. Moreover, small amounts of water may be aspirated during the terminal phase, with emphysema aquosum being the most frequent finding in some reports.54–56
In the presented case, considering the personal history of the victim, the hypothesis of suicide could not be ruled out.
A similar case, in which a 55-year-old woman affected by nasopharyngeal carcinoma and liver metastasis died in her bathtub with evidence of drowning, was reported by Okuda et al. 53
Concluding remarks
In this paper, all the cases of water-related deaths in Friuli over a 28-year-period were reviewed.
Typical autopsy findings observed in the respiratory tract which are suggestive of drowning turned out not to be completely reliable when determining the cause of death in that they were affected by putrefaction and prolonged submersion. Emphysema aquosum and external foam proved to be the most reliable indicators, but its differentiation from other post-mortem changes due to submersion must still be ascertained.
The concept of ‘dry’ (or atypical) drowning has proved to be another significant source of misinterpretation, since there are conflicting definitions reported in the literature.
The interpretation of BAC levels has turned out to be another critical point in the approach to submerged bodies, on account of potential alterations induced by PMEP and the important role of ethanol in water-related deaths: although this topic has been widely analysed in cold water, the lack of specific studies in temperate climates forces us to keep taking a conservative approach in cases of bodies found at higher ambient temperatures.
Analysis of the case history demonstrated the broad spectrum of scenarios which can be encountered by the forensic pathologist and showed that a considerable number of water-related deaths remain undetermined.
Finally, we still need to improve our knowledge of water-related deaths where autopsy, alcohol levels interpretation and death scene investigation are concerned, even though the issue of drowning has been so extensively analysed in forensic pathology.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article