
Abstract
A rare and fatal complication of suction drainage of secondary spontaneous pneumothorax is reported. The patient, likely by a mistake, arbitrarily connected the oxygen supply tube to the thoracic drain. The sharp increase of intrapleural pressure combined with the atmospheric intraalveolar environment caused diffuse lung injury and cardiopulmonary collapse without a direct lung injury. The conflicting interests of patient autonomy and patient safety require further consideration.
Introduction
Pneumothorax is a collection of air in the virtual space between the visceral and parietal pleura. Air that escaped through an injury in the lung surface is trapped intrapleurally causing the collapse of the underlying lung parenchyma. An injured lung surface can create a one-way valve, which can lead to the accumulation of trapped intrapleural air. Once the intrapleural pressure exceeds the atmospheric pressure, tension pneumothorax results. The ipsilateral lung parenchyma collapses under pressure, and if further gas is pumped periodically into the closed space, the mediastinum is displaced toward the contralateral side. Contralateral lung compression and an impaired venous return to the right atrium result in this life-threatening condition. 1
We report a case of a tension pneumothorax caused by a self-inflicted accident. There is no other case of pneumothorax previously reported with a similar mechanism. The case demonstrates that air pressure alone can cause severe lung injury, and also draws attention to the importance of patient safety.
Case report
A 57-year-old male was admitted to the hospital due to increasing shortness of breath and stabbing chest pain that started 2 days ago. Previous medical history included chronic alcoholism and chronic obstructive pulmonary disease as a result of 40 pack-years of smoking. The patient reported no regular prescription medication, his mental status was considered normal, and outward behavior was reported as conventional. The pain intensified on the left side when he coughed. His oxygen saturation in air was 91%, and air intake on the right side was decreased. No functioning lung on the left side and no tracheal shifting were detected. A chest X-ray (CXR) confirmed the total left-side pneumothorax.
Immediate thoracic drainage was performed under local anesthesia. A French gauge 28Ch chest drain was introduced into the sixth intercostal space in the midaxillary line on the left side and the tube was connected to 10 cmH2O of active suction. Immediate relief of symptoms was supported by the control CXR with some remaining atelectasis in the left lower lobe that was accompanied by thin surgical emphysema. A minimal apical pneumothorax was seen on CXR on day 2. Aggressive physiotherapy, incentive spirometry, and pain control all completed the recommended treatment and therapy. The patient was occasionally provided oxygen inhalation via a small caliber, green plastic nasal cannula, which was connected to a central oxygen supply and it was adjusted to 0.25–0.50 FiO2, when needed. A quick recovery and an expanded lung allowed the conversion of active chest suction drainage to a Bülau system (underwater seal) 2 during mobilization. The patient's full compliance and adherence to treatment were noted by the nursing staff, and no mental alterations were noted. The patient was assigned to a four-bed hospital room, in which he was alone, and the room included an operational toilet and sink.
On the night of postoperative day 3, the nurse made her night rounds at 22:00 and reported no abnormalities in the patient's condition. Ten minutes later, she heard a strange noise coming from the ward and discovered the patient in a state of respiratory arrest, accompanied by extremely extensive surgical emphysema. Cardiopulmonary resuscitation (CPR) was immediately initiated. On examining the thoracic tube in situ, it was revealed that, rather than being connected to the sucking device, it now hung freely and the thin green nasal cannula was inserted deeply into the device. The oxygen was adjusted to a 4.5 bar flow. The flow of oxygen was stopped, the chest tube was reconnected to the suction device, and CPR was continued according to the protocol. A second chest drain was introduced because no breathing was detected on the contralateral side. This right-sided pleural drain offered a significant improvement in respiration. Complex resuscitation improved the gas exchange slightly (pCO2: from 69 to 53.4 mmHg; pO2: from 13 to 35.1 mmHg). However, following 45 min of resuscitation, the unsuccessful CPR was terminated, and the patient was declared deceased. During searching the room, an open jackknife was found on the bedside table.
Autopsy findings
The external examination revealed evidence of previous surgical interventions, thoracic drainage, and resuscitation. Extensive surgical emphysema was detected, which was dominantly on the cadaver's left side. Multiple bilateral rib fractures were observed, which likely resulted from chest compressions during resuscitation. Both sides of the chest had a Ch28 drain in situ. Bilateral atelectasis was observed through the parietal pleura before opening the thoracic cavity. After the opening of the thoracic cavity, total collapse of the left, and subtotal collapse of the right lung lobes were observed (Figure 1(a)). Additionally, 150 mL of serous thoracic fluid was found on the left side of the chest, and a few milliliters of blood-tinged serous fluid was located on the right side. On the apical part of the left superior lobe, a collapsed, large emphysematous bulla (3 × 4 cm) was found with a 5-mm long laceration (Figure 1(b)). Two blood-filled, subpleural nodules, which were 5 mm and 4 × 10 mm, were observed on the anterior surface of the superior left lobe (Figure 1(c)), and three emphysematous bullae (1–2 cm) containing air and a 4 × 5 cm bullae containing blood-tinged fluid were found on the diaphragmatic surface of the left inferior lobe. The heart was slightly enlarged (380 g), and the right ventricle was dilated. Other internal organs were congested, and moderate atherosclerosis and hepatic cirrhosis were also observed.

(a) Total collapse of the left and subtotal collapse of the right lung lobes (a). (b) Collapsed emphysematous bulla on the apical part of the left superior lobe (arrow). (c) Blood-filled, subpleural nodule on the anterior surface of the superior left lobe (arrow).
Histological examination of the left lung showed total atelectasis and destruction of the lung structure with extensive fields of emphysematous areas. The alveolar walls were ruptured, and massive intraalveolar, interstitial, and intrabronchial areas of bleeding were seen. The visceral pleura was raised from the lung tissue that was located below it at multiple locations because of subpleural hematomas (Figure 2). Additionally, interstitial scarring and anthracosis were encountered. Scarring exudate that contained fibrin files was also observed on the visceral pleura of this lobe. Histological examination of the right lobes showed subtotal atelectasis, multifocal bleeding, ruptured alveoli, and a destroyed emphysematous lung structure. Some intact alveoli contained edema fluid.
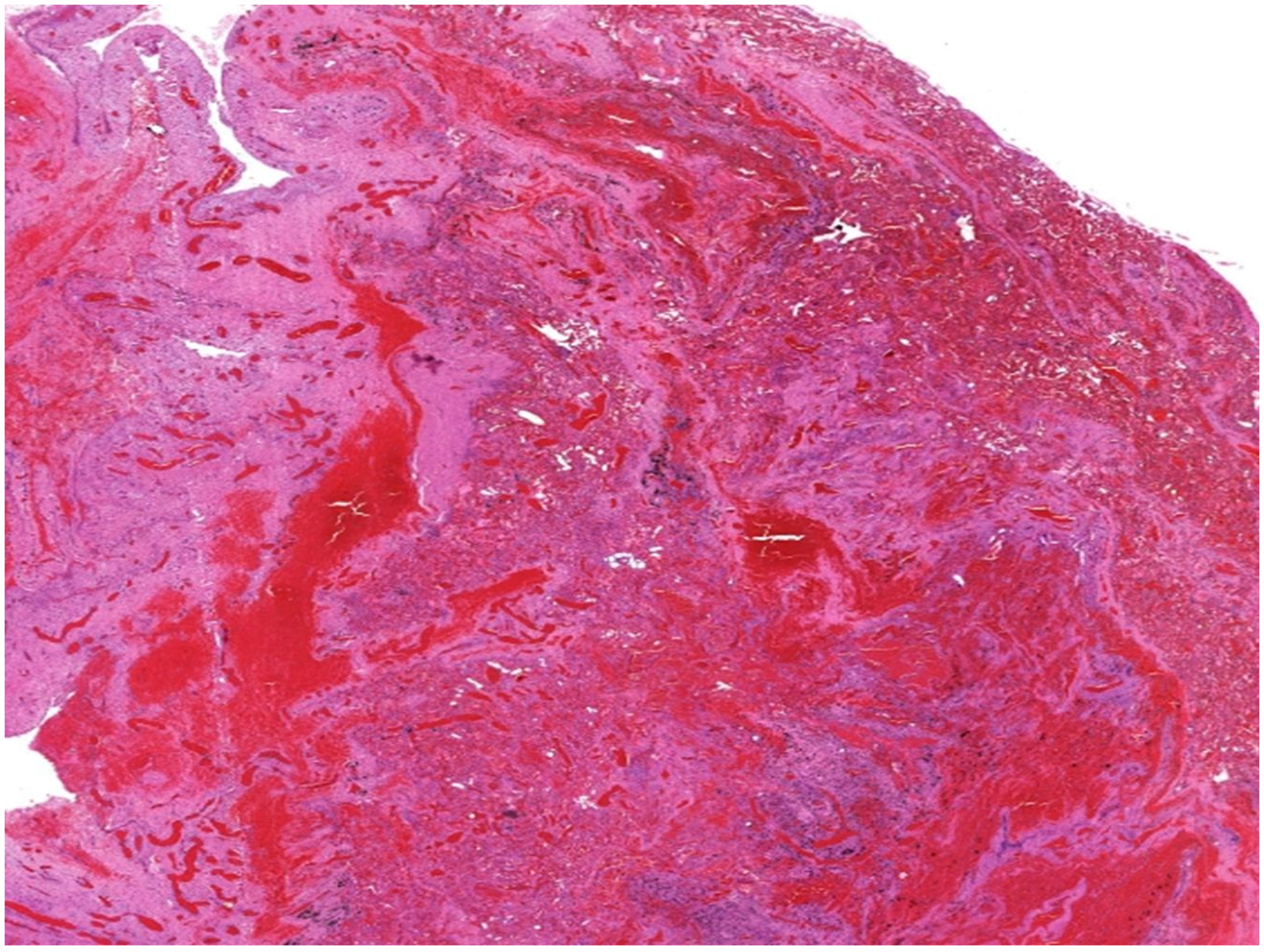
Total atelectasis, destruction of lung structure, and massive bleeding in the lower left lobe (hematoxylin and eosin staining).
Histological examination of the heart revealed mild fatty infiltration, multifocal myocardial fibrosis, and myocardial hypertrophy. The liver tissue showed steato-cirrhosis and alcoholic hepatitis, and the spleen exhibited congestion.
Discussion
Positive end-pressure artificial respiration, especially in prolonged cases and fragile lungs, can result in the rupture of subpleural alveoli and tension pneumothorax. 3 Surgical emphysema, pneumothorax, and pneumomediastinum can also be seen in blast injuries. 4 The pressure wave during high-energy explosions directly compresses the chest wall and increases the intrathoracic pressure. Intrapulmonary pressure is also increased by subjecting the blast wave to the airways. 5 The rapid compression and expansion of gas-filled tissues and the shearing between the tissues of different densities results in stretching and rupture of the alveolar walls, massive intraalveolar bleeding, edema, formation of giant emphysematous spaces filled with blood, epithelial injury, rupture of the visceral pleura and pneumothorax.4,5
An autopsy verified the consequences of left-sided tension pneumothorax, and there was also a severe degree of barotrauma on the right side. The high-pressure oxygen flow from the nasal cannula caused tension pneumothorax in the left thoracic cavity causing complete atelectasis. Dislocation of the mediastinum toward the right, and consequent high intraalveolar pressure offer an explanation for the subtotal right-sided atelectasis. A direct beam of high pressure likely caused severe destruction of the lung tissue, alveolar rupture, and intraalveolar, interstitial, and intrabronchial bleeding. An extreme degree of surgical emphysema was an indicator of the speed and power of the oxygen pressure. Prolonged CPR may also cause lung injuries, but its role in the present is not substantive, since lung injuries caused by CPR are not nearly as severe, and are usually situated in the posterior part of the lungs. 6
The cause of death was acute respiratory failure caused by severe lung destruction and atelectasis. According to the autopsy findings, diffuse bullous emphysema was the origin of the secondary spontaneous pneumothorax.
The chain of events can be reconstructed as follows. The patient disconnected the thoracic suction system at the point of the drain–bottle connection point before using the bathroom. Upon his return to the bed, he noted the two ends of the free tubing: the smaller green one and the slightly larger plastic tube. He confused the two tubes and was unable to connect the nasal piece to the chest tube. Thus, he cut the end of it using his jackknife before inserting it forcefully and deeply into the intercostal segment. While attempting to reconstruct the drainage system, he simply misconnected the oxygen tube to the thoracic drain. The small caliber (6-mm inner French gauge: 18Ch) and green oxygen cannula was inserted deeply into the chest drain (28Ch) so that even the 4.5 bar oxygen pressure was unable to push it out. No supporting evidence of suicide or misconduct was found
The “self-treatment” of a cooperative patient using routine behavior in the presented case serves as a cautionary sign with respect to patient safety. The dangers of the mismanagement of different tubes by the patients can also be illustrated using another case, where the tube for the compressed oxygen was installed into the infusion system by the patient causing a lethal air embolism. 7 Patient safety can be improved in the following ways: using differently sized (not interchangeable) connections; labeling the tubes; using different tube route lines,8–10 or using one-way release valves. 11 Providing information sheets to the patients with an explicit warning about the consequences of self-handling the tubes and catheters is also recommended.
The low energy explosion-like sudden increase of the intrathoracic pressure that resulted from the indwelling oxygen supply cannula with 4.5 bar pressure acted directly on the pleural surface and caused similar, but more severe, diffused lung injury compared to what is typically encountered during blast lung injuries. This case showed that compression of the lung tissue by a sudden and excessive increase of intrapleural pressure, even using physiological intraalveolar pressure, can lead to severe lung injury.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed consent
The case was anonymized, and according to section 40(3) of the Hungarian act of Forensic Experts (2016.XXIX), this data can be utilized freely for scientific and educational purposes without special ethical permission or consent of the relatives of the deceased.