
Abstract
Complex Suicide (CS) is defined as an unusual form of suicide in which several harmful methods are used, simultaneously or in succession, whose purpose is to avoid the possible ineffectiveness of one of the methods used to produce a certain fatal outcome. The study of CS is of great interest and plays a fundamental role in characterizing the knowledge of these rare events. We have retrospectively evaluated all CS cases examined at the Institute of Forensic Medicine of Milan from 1993 to 2022 (n = 75) with the aim of characterizing the deceased who have resorted to it. We also compared the sample of 75 CS cases with a sample of paired 115 “simple” suicides (with a single method). Our analysis revealed that the CS cases were carried out by a “typical” subject identified as an adult male, between 41 and 50 years old, suffering from psychiatric disorders and, in particular, major depressive disorder. The most frequent harmful mode was plastic bag suffocation associated with self-poisoning. CS cases used less violent methods than simple suicide controls. The pathological-forensic approach has brought to light elements that can be useful both for forensic professionals (pathologists and psychiatrists) in correctly classifying these unusual and challenging events and for clinicians working on the front line. Some profiles have been outlined that can be used to identify potentially vulnerable individuals who could benefit from increased health surveillance to treat and prevent suicide.
Introduction
There are some particular suicides defined as “complex” (CS), 1 whose frequency ranges from 1.5% to 5% of all suicides.2,3 They do not result from the use of a single harmful method as is usually the case, 3 but rather from the simultaneous or sequential use of multiple methods.4,5 Since the first reporting and classification of CS in 1974, 6 the literature describes the use of up to six different methods in a single suicide. 7 CS is divided into primary and secondary and planned and unplanned in terms of simultaneous or sequential and programming or non-programming of the suicide methods used.8,9 Some combinations are more frequent,10,11 while some CS are set up with unusual combinations,12–15 and still others with singular means16–19; there are few reports describing the realization of CS based on the type of work activity performed in life. 20 In planned CS, despite the choice of different harmful modalities, the subject determines the order of their application, which can be simultaneous or in temporal sequence, so that in case of failure of the first chosen method, the other pre-planned methods can guarantee a certain death. 21 Conversely, in unplanned CS, if the first chosen suicide method fails 22 or proves too painful or takes too long, 23 the subject resorts to an alternative and improvised method of death using the means in his/her immediate environment. 21 In cases where subjects survive the initial event, these “missed events” represent the escalation that leads them to move from less lethal means to more lethal ones until an effective method of death is achieved. 24 It is generally common among people with a history of severe psychiatric disorders. 8 Indeed, the literature reports that deceased of complex suicides usually suffer from bipolar disorder, schizophrenia, depression, borderline personality disorder, anxiety disorder and antisocial personality disorder.1,25 In these cases, the psychiatric/psychological background of the deceased people plays a major role, as most suicides worldwide are associated with psychiatric disorders, 26 with depression and psychosis described in the literature as major risk factors. 25 Other psychiatric disorders such as anxiety, personality disorders, eating disorders and other mental disorders significantly increase the risk of suicide death compared to the general population.27,28 In this context, Hösükler et al., 28 Demirci et al. 1 and Alexandri et al. 25 reported that in 71.4%, 62.5%, and 50% of complex suicides, respectively, a psychiatric disorder was diagnosed, highlighting the prevalence of this condition in individuals involved in complex suicides.
In this report, we retrospectively evaluated all cases of CS autopsied at the Institute of Forensic Medicine in Milan from 1993 to 2022, with the aim of characterizing the subjects who resorted to this method from both the forensic and psychological/psychiatric point of view. The primary aim of this investigation was a perspective of the specificity of CS as an in-depth descriptive analysis of the phenomenon. To shed more light on the matter, as supplemental to the descriptive insight, we compared the CS aforementioned with “simple” suicides (in which a single harmful method was used), matching for relevant variables (gender, age and lethal suicide method) to adjust for main confounding factors. We present the results and discuss their relevance from psychiatric-psychological and forensic perspectives to provide useful considerations for clinicians working on the front lines of suicide treatment and prevention, as well as forensic professionals, including psychiatrists, to correctly classify these unusual events.
Material and methods
A retrospective cross-sectional study was conducted at the Institute of Forensic Medicine in Milan, one of the largest cities in Italy, where numerous autopsies are routinely performed at the request of judicial or health authorities. Before every autopsy, the forensic pathologist conducts an interview with the family members of the deceased, during which all anamnestic information is collected, such as previous and current illnesses, drug treatments and the use or abuse of psychoactive substances. In the case of deceased suicides, previous suicidal thoughts and/or attempts and the time and manner in which they were carried out are also investigated. To complete the interrogation, it is customary to obtain all medical records from family members, and any additions can be requested directly from the attending physicians or health care facilities where the deceased was treated. At the same time, this information is supplemented by the investigative and circumstantial data provided by the law enforcement authorities who conducted the judicial on-site inspection where the body was found. Any farewell notes (letters, emails, phone messages) left by the deceased are recorded by the officers, as well as all the other investigative elements (e.g., witness statements or video surveillance images) and are copied into the investigation report which is given to the pathologist performing the autopsy. Everything learned is entered by the forensic pathologist into the internal database of the Institute, to which the autopsy report and cause of death are then also added. It should be noted that in all autopsy cases, the final determination of the manner of death - whether suicide, homicide, accident or natural causes - is based on the integration of pathological and forensic findings with circumstantial and investigative data collected and provided by law enforcement officers. In the absence of sufficient evidence, the manner of death may be classified as presumed or undetermined.
For this study, the above mentioned database was retrospectively analyzed to extrapolate all individuals who died by suicide over a period of 30 years (1993–2022). All categorizations of manner of death other than “suicide” were excluded, ensuring to include only those cases that were definitively classified as suicide. Further detailed investigations were then carried out by extrapolating those people who had used at least two different harmful suicide methods (CS). For the specific case of sharp force trauma, the use of different sharp weapons in different parts of the body was considered a different injury modality in accordance with the literature. Self-poisoning with different toxic substances was considered in the same way. 8
For each eligible case, the following parameters were considered: gender and age, suicide methods and means used, medical history, previous suicidal ideation and/or attempts (possibly accompanied by suicide notes), and place of death. Thus, both psychiatric characteristics (psychiatric disorders in the medical history) and psychological characteristics (suicide notes) of the individuals were examined. We would like to point out that the authors of this study have not made any psychiatric diagnoses, but have relied on the diagnoses made by psychiatrists and listed in the latest official medical documentation. In Italy, psychiatric diagnoses are made on the basis of the Diagnostic and Statistical Manual of Mental Disorders. Therefore, for the diagnoses of psychiatric disorders of the individuals selected for this study, it can be stated that the international classification referred to is the DSM (from DSM-III to the DSM-5, according to the versions updated over the years). 29
After the extrapolation, suicide methods were classified by the authors as violent (hanging, stabbing, shooting, jumping from buildings or in front of vehicles, severe intentional car accidents, electrocution, and thermal) or non-violent (fatal poisoning by illegal or prescription drugs, CO poisoning, plastic bag suffocation, and drowning), according to the literature.30,31 Ingestion of corrosive substances, although it is a kind of self-poisoning method of suicide, it has been considered a violent suicide method because of the destructive lesions it causes. 32
Statistical analyses and control group
A descriptive analysis of all complex suicides was carried out. However, in order to investigate and research this phenomenon further, a statistical analysis was also carried out with the selection of a control group. In detail, all CS cases (no = 75) were compared with a sample of simple suicides (no = 115) on socio-demographic, clinical and suicide-related variables. The selection of the cases with a single method of suicide (simple suicides) to match with the CS sample was obtained once again at the Institute of Forensic Medicine in Milan selecting, from all cases of suicide, those in which only one harmful method was used. For each eligible case, the pairing considered the following parameters: gender, age and the lethal suicide method correspondent to the main cause of death for CS, as assessed by the forensic pathologist who performed the autopsy. One case is given as an example: the CS case of a 74-year-old man who died by a gunshot to the head followed by hanging was contrasted with a simple suicide case of a man of the same age who died solely by a gunshot to the head. To improve the comparison, each CS case was compared to one simple case in almost 90% of the sample and with two simple cases in 75% of the sample (namely, out of 75 cases, the selection succeeded in paring 65 single controls and 50 double ones). Gender was equal in all pairings, whereas matching for age was evaluated and it correctly showed no significance in repeated measures t-test (p ≥ .282), comparing cases both from the first and the second matched sample. These results corroborated the mitigation for these confounding factors and allowed us to investigate cases versus controls further.
Statistical analyses were performed with the IBM SPSS Statistics 29 software (IBM Corp., Armonk, NY, USA). The groups were compared with regard to the socio-demographic, clinical, and suicide-related variables with standard tests. We tested the normal distribution of the variables. Since all the continuous variables were not normally distributed, we used nonparametric inference only, while Chi-square test was applied for categorical variables. Statistical significance was set at p ≤ 0.05.
Results
Between January 1, 1993, and December 31, 2022, 75 CS occurred, representing 1.54% of the total 4846 suicides and 0.27% of the total 27400 autopsies during the considered period (Figure 1). In all the selected cases, there were no gaps in the information collected for the study.
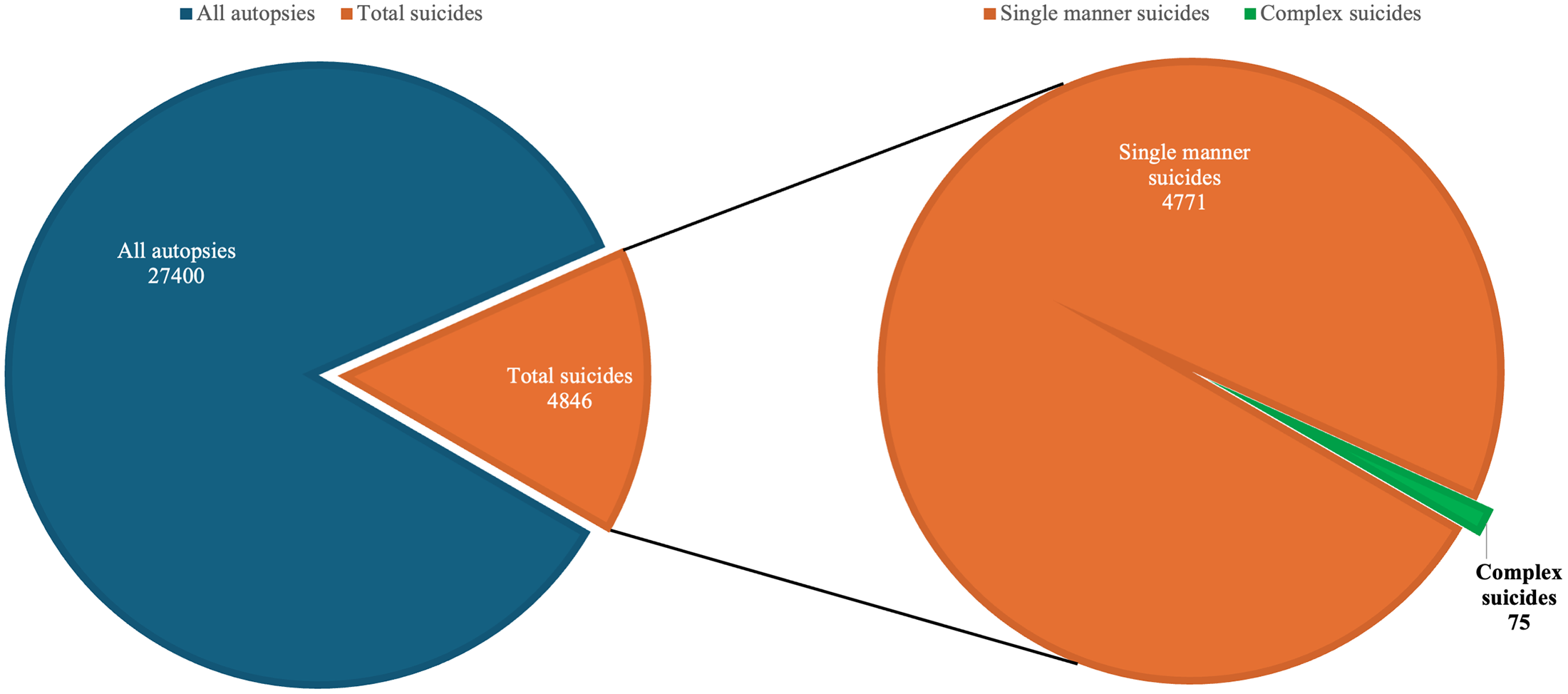
Graphical representation of the total number of suicides, simple and complex, with reference to the total number of autopsies performed in the 30 years considered.
Epidemiological data on cases
The deceased people were all white Europeans: males in 52 cases (69%) and females in 23 (31%), with a ratio of 2,3:1. The age range was between 17 and 86 years, with an average age of 50 years +/- 16.8; the age range of males was between 20 and 86 years with the mean age of 51,19 years +/- 16, while the age range of females was between 17 and 86 years with the mean age of 48.7 years +/- 17.7. Dividing the population into decades of age, it was observed that in the 41–50 age group the majority of deaths occurred, with 23 subjects (16 males and 7 females). All data for this parameter has been shown in Figure 2 (Figure 2).

Graphical representation of CS cases divided by age and gender.
Methods of suicide
In 64 of the 75 total cases (85.3%) two different harmful modes were used, while in 11 (14.7%) three were used. Overall, the most widely used modality was head confinement asphyxiation, i.e., plastic bag suffocation (PBS), observed in 31 cases (41% of the total CS), followed by sharp force trauma in 21 cases (28%) and self-poisoning in 15 cases (20%). These three most common modalities are described below with the details of their different associations.
Plastic bag suffocation
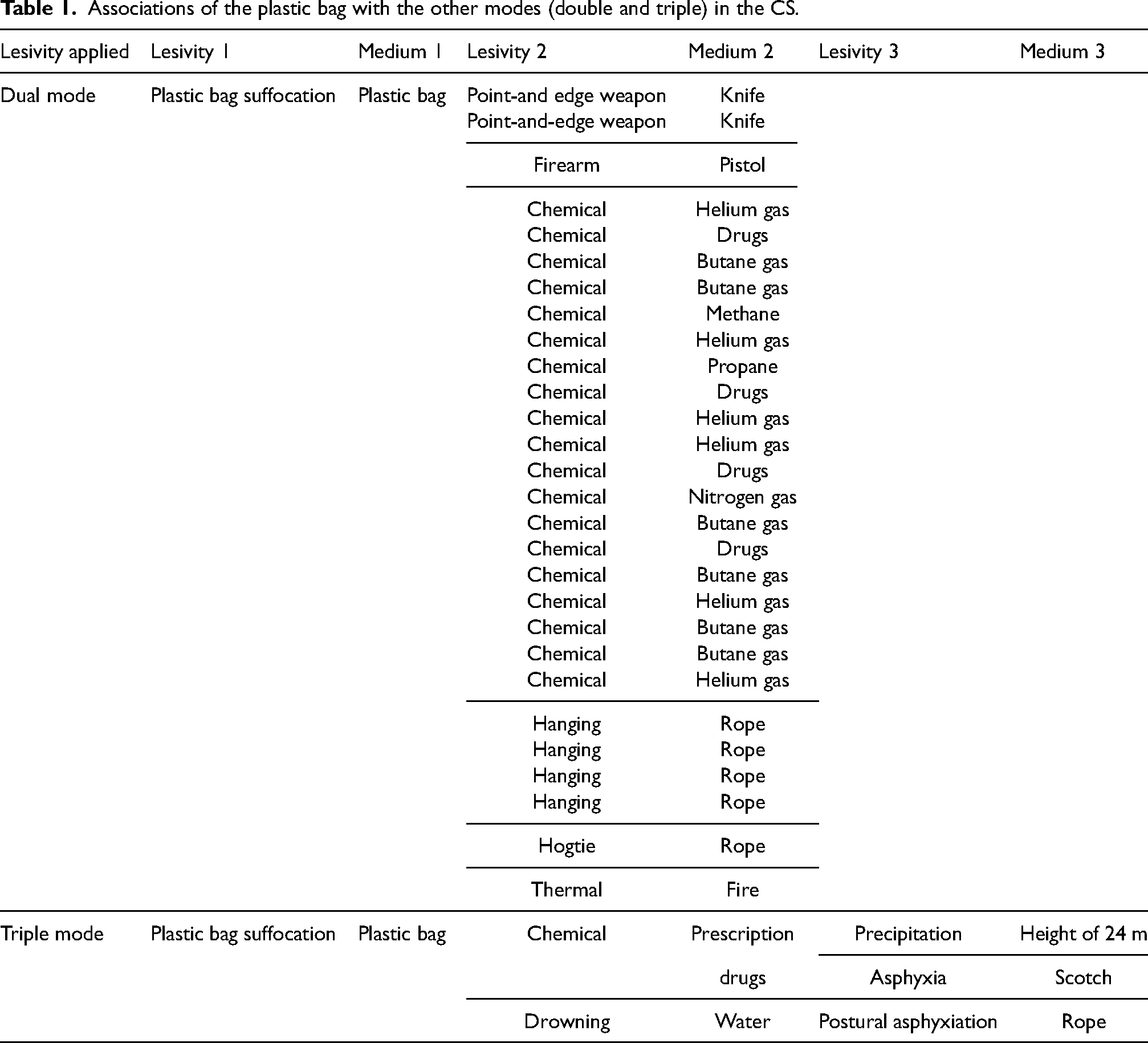
In 28 cases (90%) PBS was associated with only one other modality and specifically with: inhalation of different gases in 15 cases, incongruous drugs intake in 4 cases, hanging in 4 cases, sharp force trauma in 2 cases, and gunshot and self-immolation and hogtie one case for each. Overall, the first harmful mode, to be considered non-violent, was accompanied in 9 cases (33,3%) by a violent suicide mode; in the remaining 19 cases (68%) a coexistence of two different non-violent suicide modes was noted.
In 3 cases (10%) PBS was associated with two other different modalities (Table 1). With regard to the triple associations, in all cases a prevalence of non-violent suicide modes has been documented, and only in one case, the third mode implemented can certainly be considered as violent.
Associations of the plastic bag with the other modes (double and triple) in the CS.
Sharp force trauma
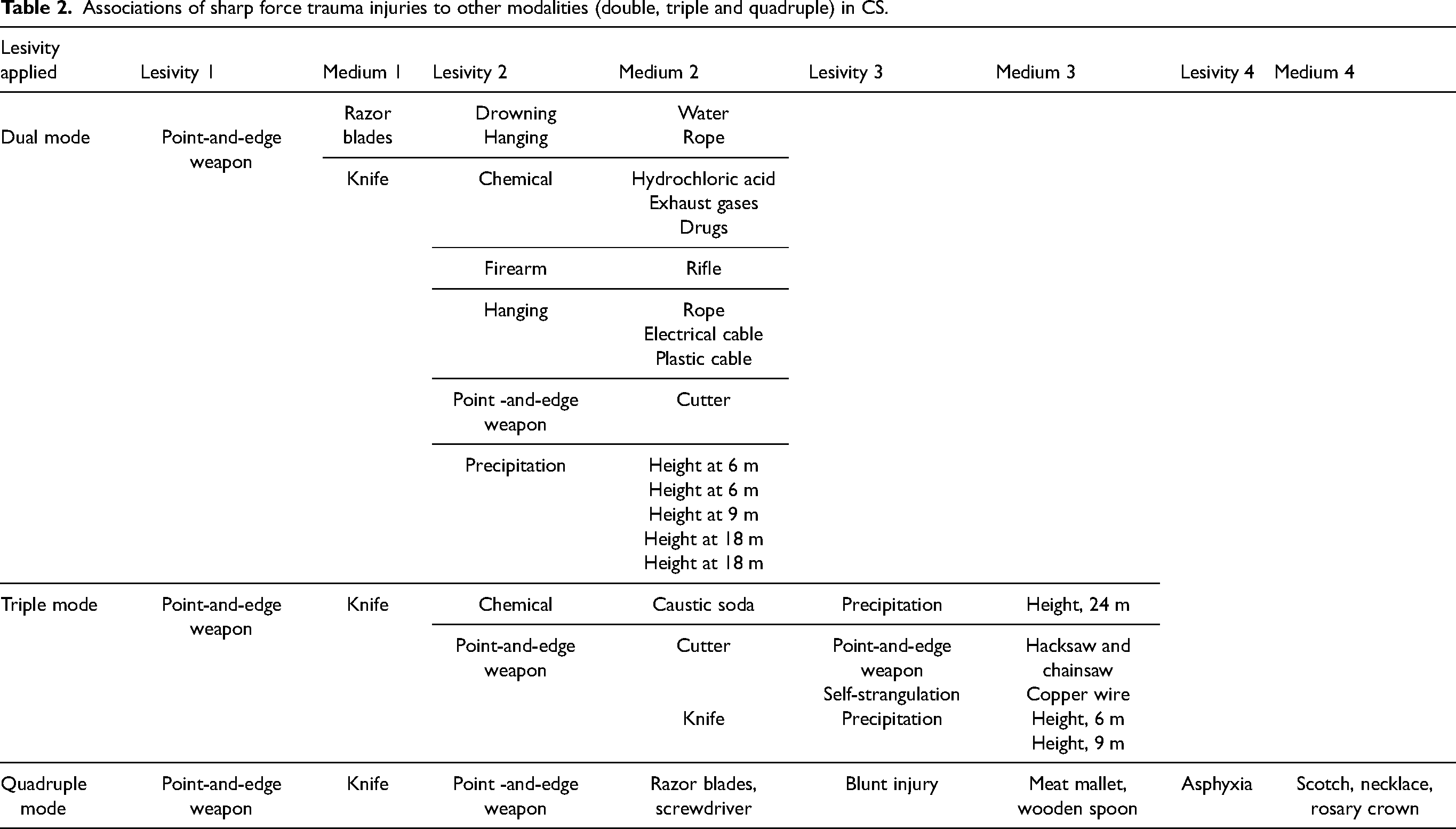
In 15 cases (71%) sharp force injuries were associated with only one other modality and, specifically, with: jumping from height in 5 cases, hanging in 4 cases, self-poisoning in 3 cases, and drowning and gunshot and other point-and-edge injuries (different weapon and body areas) in one case for each. In 5 cases (24%) sharp force trauma was associated with two other different modes and in one case only to three other ones (Table 2). Overall, the first harmful mode, to be considered violent, was almost always followed by a further violent suicide mode (11 cases, 52%). Only in 4 cases (20%), a second non-violent suicide mode was resorted to. In triple and multiple associations (6 cases – 28%) only violent modes have been documented.
Associations of sharp force trauma injuries to other modalities (double, triple and quadruple) in CS.
Self-poisoning
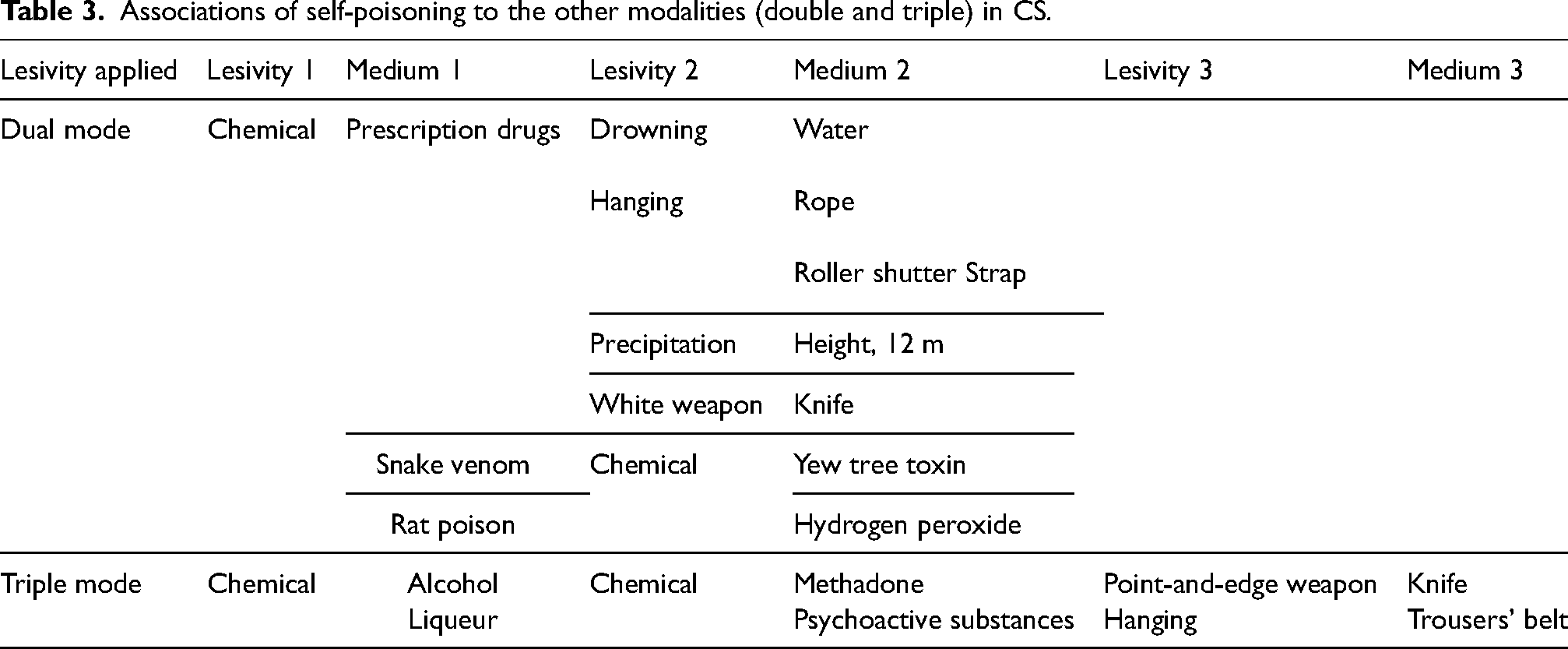
In 13 cases (87%) self-poisoning was associated with only one other modality and, specifically, with: ingestion of different harmful substances in 5 cases, hanging in 4 cases, drowning in 2 cases, and sharp force trauma and fall from height in one case for each. Overall, the first harmful mode, to be considered non-violent, was accompanied in 6 cases (46%) by a violent suicide mode; in the remaining 7 cases (54%), a coexistence of two different non-violent suicide modes was noted. In 2 cases, self-poisoning was associated with two other different modalities (Table 3). With regard to these two triple associations, in all cases a second non-violent harmful mode was documented, in turn followed by a third violent one.
Associations of self-poisoning to the other modalities (double and triple) in CS.
Less frequent suicide mode associations
In 5 cases (7% of the total CS), hanging was associated with gunshot injuries at the head in 3 cases, and sharp force trauma and drowning in 1 case for each.
In 2 cases (2.7%), the association between falling from a bridge with subsequent drowning in a river below was recorded.
Finally in only one case (1.3%) blunt force trauma (car accident) was associated with drowning in a river.
In all these cases, the first harmful mode has always been violent, accompanied in 4 cases by a second violent suicide mode and in 4 cases by a non-violent one, always consisting of drowning.
Overall, in accordance with the circumstantial data provided by the Police, with those of the judicial inspection and with the data obtained from the autopsy examination, 58 suicides (77%) were considered planned CS, while the remaining 17 (23%) as unplanned CS.
Pathological and medical history of CS deceased
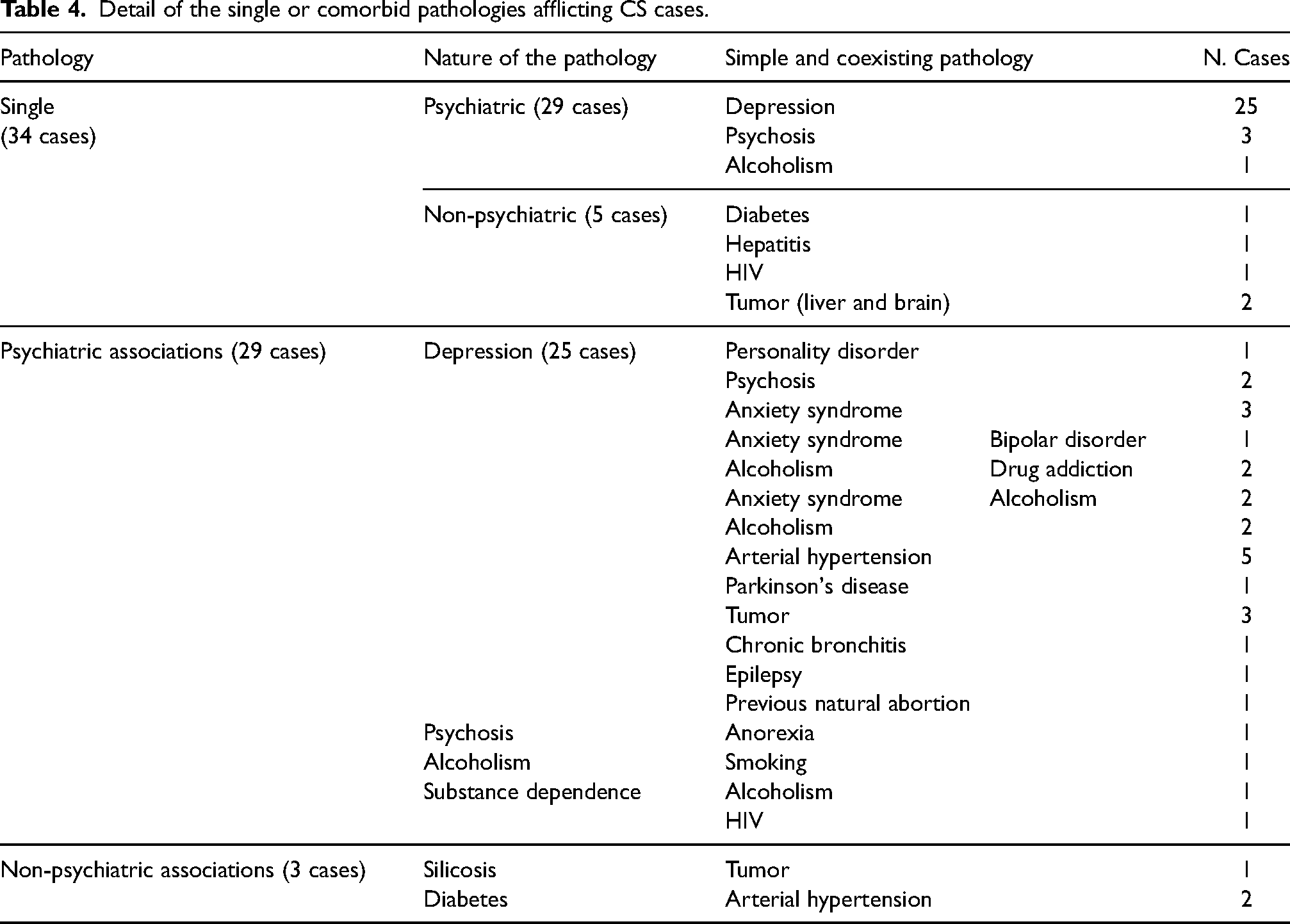
Globally, 66 subjects (88% of the total CS) were suffering from at least one pathology. In detail, 58 individuals (88% of the entire population with pathologies) suffered from psychiatric disorders, 8 (12%) from non-psychiatric pathologies and the remaining 9 had no diagnosis reported in their history. Psychiatric illnesses documented as single morbid forms were depressive disorders, psychosis, and alcoholism. Among all, depressive disorders were prevalent, having affected 74% of the total amount of deceased diagnosed with a pathological condition and 52% of those suffering from at least one psychiatric illness. Depression has been documented as the only morbid form in 25 deceased and as a pathology associated with other non-psychiatric and psychiatric diseases in 24 further deceased. Specifically, depression was found to coexist with chronic non-psychiatric disorders in 13 cases mainly accompanied by arterial hypertension. Depression was also found to coexist with other psychiatric pathologies in 11 cases, with prevalent coexistence with psychosis, alcoholism and substance dependence, as well as with anxiety and personality disorders.
For completeness, non-psychiatric pathologies consisted of single morbid forms in 5 cases (14.7% of all the deceased with a single comorbidity) and associated with each other in 3 cases. The details of the diseases are given in Table 4.
Detail of the single or comorbid pathologies afflicting CS cases.
It was also noted that 43 deceased (57% of the total) were under pharmacological therapy, 8 (19%) of whom were only taking non-psychiatric medication. On the other hand, the remaining 35 deceased (81%) took psychiatric therapy consisting mainly of antidepressants. Psychiatric drugs were administered individually (26 cases) and in combination with other drugs (9 cases). Overall, it emerged that 15 subjects suffering from depression (30% of the total amount of individuals suffering from depressive disorders) were not under psychotropic treatment at the time of death.
Previous suicide ideation and attempts, and farewell notes
Another important investigated aspect concerned previous suicidal ideation and suicide attempt(s): it emerged that 15 deceased (20%) had expressed their intention to kill themselves to friends and family and 19 deceased (25%) had already tried to kill themselves (especially through incongruous ingestion of prescription drugs); out of the total of these 34 subjects, 9 individuals (26%) had both previous suicidal ideation and attempt. In 7 cases family members reported that they were not particularly surprised by the suicidal event of their relative, due to suicidal thoughts recurrent over time, even chronologically recent, and to the suicidal intentions already previously put in place. However, although not entirely unprepared for the eventuality, none of the family members reported that they had perceived signs of an imminent and concrete suicidal action. Despite everything, the majority of the deceased’ people's families, during the interview that preceded autopsy examination, stated that they had no clue that would allow them to believe that their relatives would soon engage in anti-conservative behavior. In detail, 44 subjects had not, to the best of their knowledge, ever expressed suicidal thoughts; as for the remaining 16 individuals (21%), family members reported that the suicidal thoughts expressed by the deceased had been mostly momentary with a fluctuating trend: in some moments they were more intense, while in others they were rarely expressed and, moreover, these intentions were expressed with wide chronological intervals separating them, thus resulting in the suicide act unexpected and surprising for family members. In particular, in 6 cases, an intensification of suicidal thoughts has been reported in recent months, but not accompanied by any previous suicide attempt. Apart from the 19 cases in which a suicide attempt had already taken place, there was no previous attempt in the remaining 56 cases (75) to the best of the family's knowledge.
About the farewell notes, they were found on the scene of 37 (about 49%) CS: to justify the CS the motivations given by the deceased people reported great inner suffering, especially preceding the act. In particular, younger subjects reported relational conflicts in 5 cases (7%) and, in a smaller number, feelings of inadequacy in 2 cases (3%) in adult subjects, financial stress emerged in 10 cases (13%) and rupture of a romantic relationship in 11 cases (15%); elderly deceased reported serious health problems, physical pain and disability as reasons for suicide in 3 cases (4%), as well as loneliness, marital bereavement and social isolation in 6 cases (8%). Among these 37 farewell notes, there are also 6 from deceased who died by suicide during the years of the Covid-19 pandemic. Specifically, 3 CS in 2020, 5 CS in 2021 and 13 in 2022 were recorded. In all the suicide letters, different motives were reported, as mentioned above (suffering for a recent loss in 1 case, financial stress in 2 cases, and social isolation in 2 cases). In one case, the consequences of the Covid-19 pandemic were explicitly cited as the reason for the suicide.
Analysis of the place of occurrence
In prevalence, most of these particular suicides (51 cases - 68%) were carried out by the deceases in their own homes, while the remaining 24 (32%) occurred in outdoor environments. In this context, canals/rivers with 5 subjects, vehicles with 4 cases, followed by hospital and hospitalization facilities for the elderly that recorded 3 cases for each CS; other settings were public parks (3 cases) and prisons (2 cases), an office, an urban street, a barrack, and a cemetery, with 1 case each.
Complex vs. simple suicide
When we compared CS cases to cases with simple suicide (with a single method) on socio-demographic, clinical, and suicide-related variables, we reported two main differences. Firstly, CS seems to record higher previous suicide attempts when compared to controls (chi-square = 39.95, p < .001), even though great cautiousness is required due to the high number of unavailable data for both groups. Furthermore, considering the comparison between violent and nonviolent suicide method, in order to compare CS with the matched single methods, in case the set of methods for the case joined some violent and some nonviolent, we categorized as violent. A binomial test on each separate group showed a prevalence of violent methods among controls (observed proportion equal to 72%, p > .001). Instead, CS distribution seems even between violent and nonviolent (observed proportion equal to 56%, p = .356).
Discussion
The literature has evaluated many aspects of CS from different points of view, but there is no psychiatric-psychological study of the deceased of these unusual self-suppressive forms. For this reason, and to partially fill these information gaps, we have undertaken a retrospective study on all the cases of CS received to the attention of the medico-legal Institute of Milan for the execution of the autopsy, with the aim of characterizing the subjects who die for CS. In addition, some forensic considerations can be useful to professionals in the sector for the correct framing of these unusual and challenging events. For the retrospective study on CS, we relied on the available data and extrapolated those that were relevant. This was information collected during forensic procedures (on-site examination, interviews with relatives, autopsy, laboratory analysis) and carefully recorded in the internal database over the last 30 years, filling in a standardized template. For this reason, no missing epidemiologic-forensic data was recorded for any of the cases, so that a complete and accurate overview of the selected cases could be obtained. In the case of CS, it was therefore possible in all cases to extrapolate the different harmful methods of suicide, as they had to be accurately reported as forensic data of great relevance.
In this general context, the study analysis was able to point out a “typical” prototype of a subject dying of CS, which can be identified in an adult male in the 41–50 age group, suffering from psychiatric disorders. The deceased planned the suicide in his own home, combining in double or triple association the prevailing harmful mode, resulting in PBS. In the dual combinations, PBS was accompanied more by the inhalation of various commercially available gases, in a smaller number of cases by the use of a gun, the ingestion of substances, hanging mechanical asphyxia, gunshot wounds and, very rarely, fire and hogtie (hand and feet are fastened together 33 ). In triple combinations, PBS was mostly associated with substances ingestion and closure of the airways with adhesive tape, precipitation from height with pharmacologically active substances ingestion, and finally drowning and asphyxiation, that is called waterboarding or water torture. 9
The more articulated the associations of the harmful modalities are, the clearer it becomes which component constituted the thinking, considering and/or planning of the suicide: in fact, precisely in the suicide carried out through the application of multiple harmful methods, the strong will of the subjects to end their lives emerges, eliminating any possibility of survival. In fact, the aim of a CS is to obtain a sure fatal outcome and, at the same time, to prevent one of the chosen means from failing, preventing the realization of suicide. 8
In the case series studied, depressive disorder was the most common psychiatric pathology associated with both other psychiatric and non-psychiatric pathologies. With regard to depression, it was found that around 30% of those affected were not receiving psychotropic treatment at the time of suicide. This fact underlines that more attention should be paid to the screening of depressive symptoms and the treatment of this pathology. 34 Among our cases, only one subject was on methadone therapy for opioid dependence. This figure is in contrast to what is reported in literature, especially in countries such as the United States, where the phenomena of opioid addiction and abuse are mainly related to their non-medical use. 35 In Italy, the use of opioid analgesics remains much lower than in Northern Europe and the United States. In addition, numerous efforts have been made to ensure that doctors and pharmacists exercise greater vigilance in prescribing or dispensing opiate drugs to patients. 36 In addition, in 3 cases, subjects were suffering from a neoplastic pathology, a condition of great mental and physical fragility, certainly predisposing to a greater risk of suicide.34,37 It has also been shown that some cases of complex suicide occurred in institutions traditionally considered protected settings, such as hospitals, hospitalization facilities for the elderly and prisons. In particular, with regard to prisons, our data confirm what has already been established in the literature, namely that prisoners are a risk group both for suicide38–40 and for natural mortality at younger ages. 39
To further substantiate this study and the significance of the results, statistical analyses were carried out with a control group of simple suicides with similar epidemiological and forensic characteristics. Comparing CS cases to simple suicides, a higher prevalence of past suicide attempts among CS cases was observed. This result is interesting and can be related to a higher severity of these individuals. The lower percentage among CS cases of violent methods compared to simple suicide controls might suggest a cumulative usage of milder, or so thought, instruments instead of an immediate search for a more aggressive one. However, CS cases’ profiles could be similar to violent attempters’ and serious attempters’ ones. In fact, these subjects, compared with ones whose attempts were neither violent nor serious, were found to be more likely males, older, to have higher severity of depressive symptoms, to have a family history of suicidal behavior, to make repeated suicide attempts, and with higher medical lethality.41,42
In general, CS method and in particular the use of more than one mode in succession may be particularly linked to the concept of acquired capability for suicide of the Interpersonal Theory of Suicide by Thomas Joiner. 43 A subject would acquire the capability for suicide during a period of time by a lower fear of death and an increased pain tolerance and we hypothesize that this condition may result also by the use of more methods in succession.
From a psychological point of view, the discovery of farewell notes has made it possible to investigate the motivations behind the suicide. They were characterized by different prevalence depending on the age group of the cases. Some of the motivations reported in the farewell notes may be related to the other two constructs of the Interpersonal Theory of Suicide: feelings of inadequacy (3%) can be linked to Perceived Burdensomeness (self-hate), while the rupture of a romantic relationship (43%) and loneliness, marital bereavement and social isolation (8%) can be linked to Thwarted Belongingness - to feel disconnected from others. 43 The reasons reported by older adults, i.e., serious health problems, physical pain and disability (4%), can be associated as well to the construct of Perceived Burdensomeness (the feeling of being a burden to anyone) and to the association between physical pain and suicide. 44 It was interesting to note that in one farewell note from an individual who died by complex suicide in the period 2020–2022, the consequences of the Covid-19 pandemic were cited as the reason for the suicide. This suggests that the Covid-19 pandemic certainly had a significant psychological impact on the mental health of certain individuals, although studies have shown that the number of suicides overall did not increase.45,46 Thus, the reasons behind complex suicides, at least in part, may reflect the specific historical circumstances in which they occur. An aspect that has not yet emerged but may become increasingly important in the future is the influence of technology (internet and socials above all) on the mechanism of devising and enacting complex suicides. In addition to a purely psychological approach, suicide notes, together with detailed questioning of the relatives about the state of health of the deceased, particularly from a psychological point of view, and investigations into previous thoughts and/or attempts as part of the so-called psychological autopsy, can make a significant contribution to determining the motives for suicide. 47
At the same time, the correct management of a possible case of CS must not refrain from a strict pathological-forensic approach. Indeed, the circumstances of death could mistakenly point in the first place towards a murderous crime, as CS can be associated with very bloody scenarios and extreme disorder. 8 Regardless of the methods used and the way to self-inflict the injuries, all CS should be meticulously investigated to establish the true nature of the injuries and the reasons behind the gesture. In fact, the probability that the observed lesions were produced by other subjects to simulate a suicide must be carefully evaluated. 8 The diagnosis of CS requires numerous considerations to correctly assess the manner of death, the chronology of events and all the methods involved. In particular, a thorough inspection of the death scene, careful collection of anamnestic data and circumstantial evidence (including witness statements and security camera footage), as well as a full judicial autopsy are essential. If deemed necessary, macroscopic examination can be supplemented by the performance of post-mortem laboratory analysis (histology, toxicology and genetics). Overall, the final diagnosis should be made on the basis of the integration and convergence of multiple elements from different multidisciplinary competences, including psychiatric-psychological ones, which should eventually be combined together as pieces of a single puzzle.
To the best of our knowledge, this is the first study in literature with a remarkable sample size of CS (n = 75: CS is a rare event) and comparing simple suicide cases to CS cases. However, there are the typical limitations of a retrospective study over a large period of time. Although all the investigated categories of information were filled in, we are aware of the possibility that the anamnestic information of the selected cases might not be exhaustive in some parts, especially for older cases. Certainly, we also do not know the degree of physical, social and emotional suffering of the deceased or their feelings about the psychiatric (and other) illnesses from which they suffered. This limitation results from the fact that mainly data relevant for autopsy and forensic purposes are routinely collected. Additionally, the definitions of previous suicidal ideations and attempts from a medico-legal perspective may not align perfectly with the terminology used in suicidology. Despite these limitations, we considered these definitions valid given that the analyzed case histories were derived from retrospective forensic annotations.
Despite these limitations, we believe that this is a study that makes it possible to examine the phenomenon of complex suicides, which even today often remains unrecognized, from a forensic perspective on the basis of autopsies. At the same time, however, it also has a pioneering character because, by specifically examining the psychological and psychiatric sphere of these deceased persons, it allows a view beyond pure forensic pathology into the “world of the living” and into the clinical field for the first time. In this context, some profiles have emerged (age, gender, psychiatric-pathological history and previous suicidal intentions/attempts) that can be helpful in identifying individuals with a potentially higher risk. These are indeed fragile individuals with psychiatric disorders who are likely to be treated in hospitals or psychiatric centres that could be given more attention. For example, it has been noted that many people are not treated for their depressive disorders, so increased health surveillance with more time and economic resources to monitor adherence to drug therapy could have a positive impact. 48 At the same time, increased clinical screening and support for psychiatric disorders could also play an important role in prevention.
In conclusion, this study highlights the usefulness and potential of the interaction between the world of forensic pathology and the clinic as they see the two different sides of CS and only by combining information that comes from both sides and is of equal relevance can it be possible to shed further light on this phenomenon.
Footnotes
Authors’ contributions
ST and GG equally contributed to this work. They devised the project and the main conceptual idea of the article, collected data, drafted the manuscript and performed literature research. MB contributed to the investigation and methodology. FC and RC developed the psychiatric and psychological aspects contributing to the characterization of the cases, performed the statistical analyses and reviewed the manuscript. RZ guarantor of the project and directed the study, devised the main conceptual idea of the article.
Availability of data and material
All the data have been reported in the manuscript.
Code availability
(software application or custom code) Not applicable.
Consent to participate
The author(s) declared that all the investigations were carried out accordingly to the Italian Law.
Consent for publication
All the authors agree for publication
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics approval
All the subjects involved in this study underwent a judicial autopsy at the Institute of Legal Medicine of Milan in order to identify the cause of death. Data collecting, sampling and subsequent forensic analysis were authorized by the inquiring magistrate. In accordance with Italian law, ethical approval is not required in these cases, however the anonymity of the subjects must be guaranteed. Furthermore, this article does not contain any studies with living human participants performed by any of the authors. Finally, this paper follows the guidelines provided by Italian national law, the Italian National Bioethical Committee and the Helsinki Declaration guidelines.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.