
Abstract
To determine the cause of death and sociodemographic predictors of dead-on-arrival cases brought for autopsy, a cross-sectional study was conducted. A total of 422 dead-on-arrival cases brought for an autopsy to a tertiary center in Ethiopia were reviewed. Descriptive and analytic analysis were used, and logistic regression analysis was performed to examine the association between sociodemographic variables and the cause of death. The study found that dead-on-arrival cases accounted for 32.5% of all autopsied cases. The mean age was 38.9 ± 15.6 years and ranged from 15 to 90. Approximately two-thirds of the cases were in the 15 to 44 age range. Male victims accounted for more than two-thirds of the cases, and 82.9% of the victims were urban residents. The cause of death could not be determined in 6.6% of cases. Unnatural deaths were the leading causes, followed by communicable diseases and non-communicable diseases. Pneumonia and coronary artery disease were the leading specific causes of death. Residence and age were found to be associated with unnatural deaths. Urban residents had higher odds of dying due to communicable diseases compared to rural residents. Additionally, younger individuals aged 15–29 years had lower odds of dying due to non-communicable diseases compared to those older than 75 years. In conclusion, the high number of brought-in dead cases in Ethiopia, particularly among the younger population, is a concerning issue that requires immediate attention. Unnatural deaths were predominant, highlighting the need for improved safety measures and emergency medical services.
Keywords
Introduction
Dead on arrival (DOA) refers to patients pronounced dead upon arrival or after unsuccessful resuscitation.1,2 Such deaths, especially in apparently healthy individuals, have a profound impact on individuals, families, communities, and society as a whole.3,4 Understanding the causes and factors that contribute to DOA cases is crucial for developing preventive strategies and improving health services, although investigating these cases can be challenging due to limited information.1,5 Autopsy-based studies play a key role in uncovering underlying causes and systemic gaps, offering insights into improving care outcomes.
Investigating DOA cases is vital for identifying healthcare system challenges, particularly in low- and middle-income countries where comprehensive studies are scarce.1,5 The frequency, patterns, and determinants of DOA cases vary globally due to diverse diseases, genetic factors, environmental influences, and healthcare access.1,5
Despite previous studies in Ethiopia focusing on early mortality predictors among emergency department patients, DOA cases have often been excluded, leaving them unexplained until autopsy.6,7 Autopsy-based investigations are crucial for understanding the causes of DOA cases. Currently, there is a lack of specific autopsy-based studies targeting DOA cases in Ethiopia. In Ethiopia, DOA cases are considered medicolegal deaths that require autopsy examination to determine the cause of death (COD). Unfortunately, only a few specialized centers in the country offer postmortem services. The Department of Forensic Medicine and Toxicology at St Paul's Hospital Millennium Medical College is one such center that provides postmortem examination services to cases referred from various regions of Ethiopia.
This study aimed to explore the causes of death and sociodemographic predictors of DOA cases in Ethiopia. By addressing this research gap, it seeks to contribute to public health initiatives, forensic medicine practices, and medical research efforts, offering valuable insights for developing preventive strategies and enhancing healthcare services.
Materials and methods
Study design, setting, and period
A cross-sectional study was conducted at St Paul's Hospital Millennium Medical College (SPHMMC), a tertiary hospital in Addis Ababa, Ethiopia. The Department of Forensic Medicine and Toxicology at SPHMMC provides postmortem services to cases referred from most regions of Ethiopia. Data from medicolegal autopsies conducted from January 1, 2021, to December 31, 2021, were retrospectively reviewed. Data collection occurred from August 1 to September 30, 2022.
Source and study population
The source population included all dead bodies brought for autopsy to SPHMMC. The study population comprised cases aged >14 years declared DOA and brought for autopsy during the study period. Cases with advanced decomposition were excluded.
Sample size determination and sampling procedure
The sample size was calculated using a single population proportion formula with a 95% confidence level, 5% margin of error, and a 10% non-retrieval rate for incomplete or lost records. Assuming a 50% prevalence (due to lack of prior data), the sample size was 384, which increased to 422 after accounting for non-retrieval. To ensure the representativeness of the sample, a simple random sampling technique was used. A total of 982 DOA cases fulfilled the inclusion criteria, and 422 participant records were selected using a simple random sampling technique through computer-generated random numbers.
Data collection procedures
Data were extracted from autopsy logbooks and reports using a pre-designed structured data abstraction template. The tool included sociodemographic factors, circumstances before death, and the outcome variable (cause of death). To maintain data quality, the predesigned data abstraction template was pretested on 40 cases, and amended accordingly. Data collection was conducted by trained medical residents under the supervision of principal investigators. Data completeness and consistency were verified daily.
Definition of variables
(1) Dead on arrival
Dead on arrival or brought in dead (BID) refers to individuals pronounced dead upon arrival or after unsuccessful resuscitation, typically within 15 min of arrival.1,2 Cases that were declared DOA at health facilities and brought for autopsy with a certificate confirming their DOA status were included in our study.
(2) Classification of causes of death
Causes of death (CODs) were classified using the International Disease Classification System (11th version) and the 2006 Global Burden of Diseases classification. CODs were categorized into three groups: communicable diseases (CDs), non-communicable diseases (NCDs), and unnatural deaths. Unnatural deaths included mortality from external incidents, drugs, adverse effects, and medical mishaps. NCDs included circulatory, gastrointestinal, mental, neurological, neoplastic, perinatal, renal, respiratory, and endocrine disorders. CDs included infectious and parasitic diseases.8,9
(3) Classification of residence as urban and rural
According to the urban planning law in Ethiopia, an urban center is defined as a community with ≥ 2000 residents, with ≥ 50% engaged in non-agricultural work. A rural area consists of individuals living in a specific region who are engaged in either agricultural or non-agricultural activities.10,11
Data analysis
Data were entered using Epi infoTM version 7.2.3.1 and analyzed using SPSS version 26. Descriptive statistics such as mean and standard deviation (SD) were used for continuous variables, and frequencies and percentages were performed for categorical variables. Bivariate logistic regression identified relationships between sociodemographic variables and CODs. Variables with P ≤ .2 were included in multivariate logistic regression. A P-value of <.05 was considered significant. The Hosmer-Lemeshow test assessed model fit.
Our study was approved by the SPHMMC Institutional Review Board (Approval number: PM 23/80) on July 27, 2022. This is an IRB-approved retrospective study, all case information was anonymized, and consent was not required.
Results
Sociodemographic characteristics
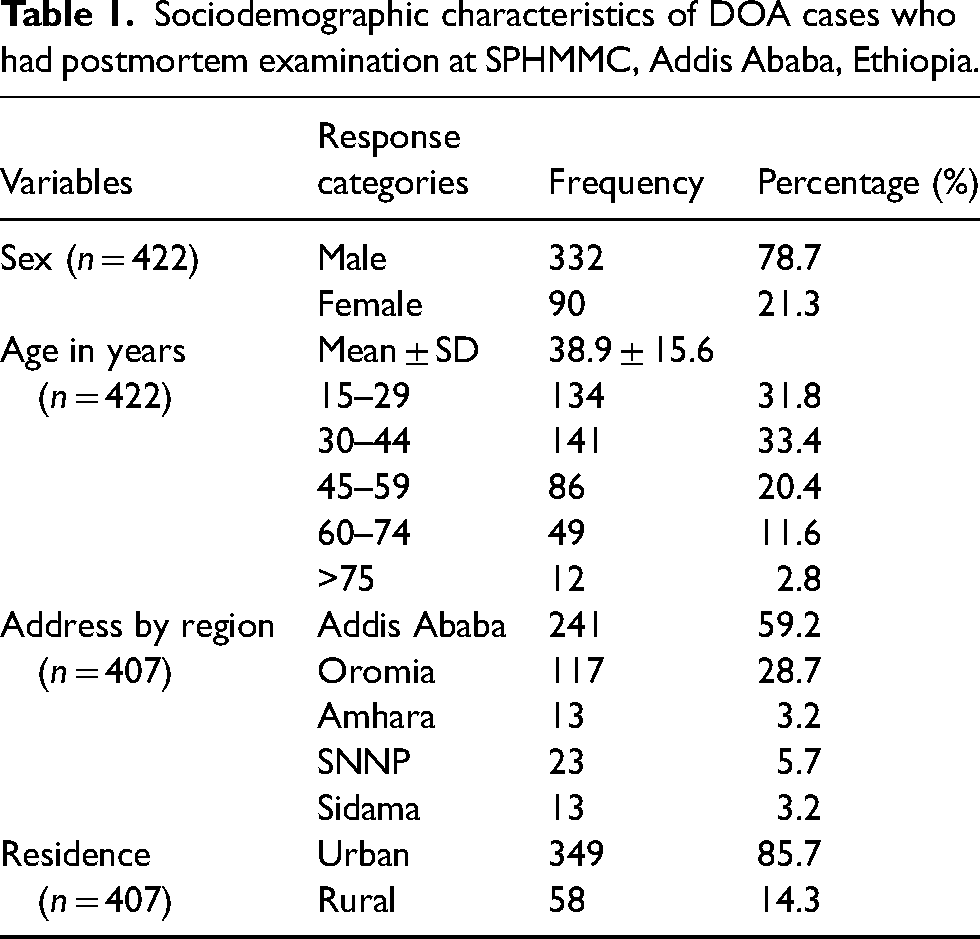
During the study period, 3025 autopsies were conducted at SPHMMC, with 982 cases (32.5%) being BID. In this study, 422 cases were sampled and included in the study (the retrieval rate was 100%). The mean age was 38.9 ± 15.6 years, with two-thirds of cases in the 15–44 age range. Males accounted for 78.7% of cases, and 82.9% were urban residents (Table 1).
Sociodemographic characteristics of DOA cases who had postmortem examination at SPHMMC, Addis Ababa, Ethiopia.
Circumstances related to death
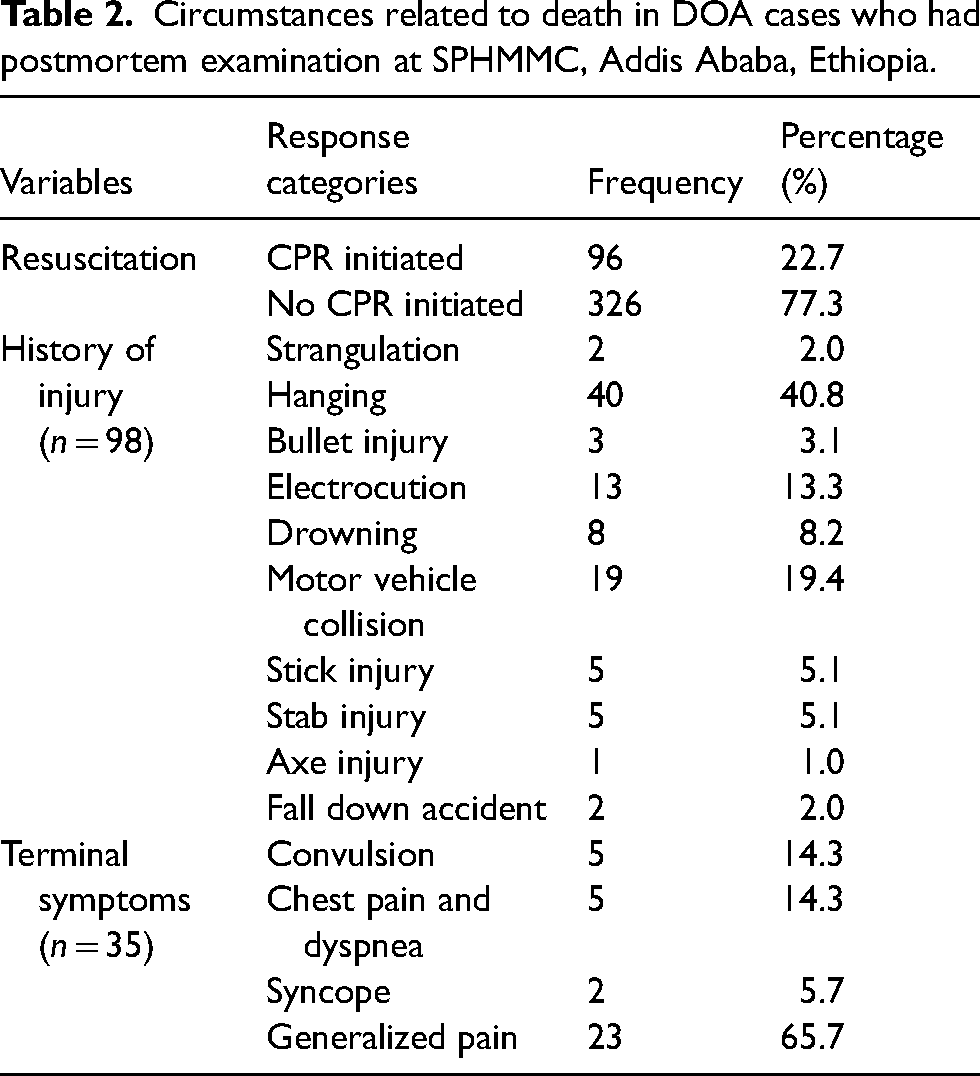
Of the 422 cases, 326 (77.3%) were pronounced dead upon arrival without cardiopulmonary resuscitation (CPR), while 96 (22.7%) died after unsuccessful CPR. Table 2 summarizes the circumstances related to death.
Circumstances related to death in DOA cases who had postmortem examination at SPHMMC, Addis Ababa, Ethiopia.
Causes of death
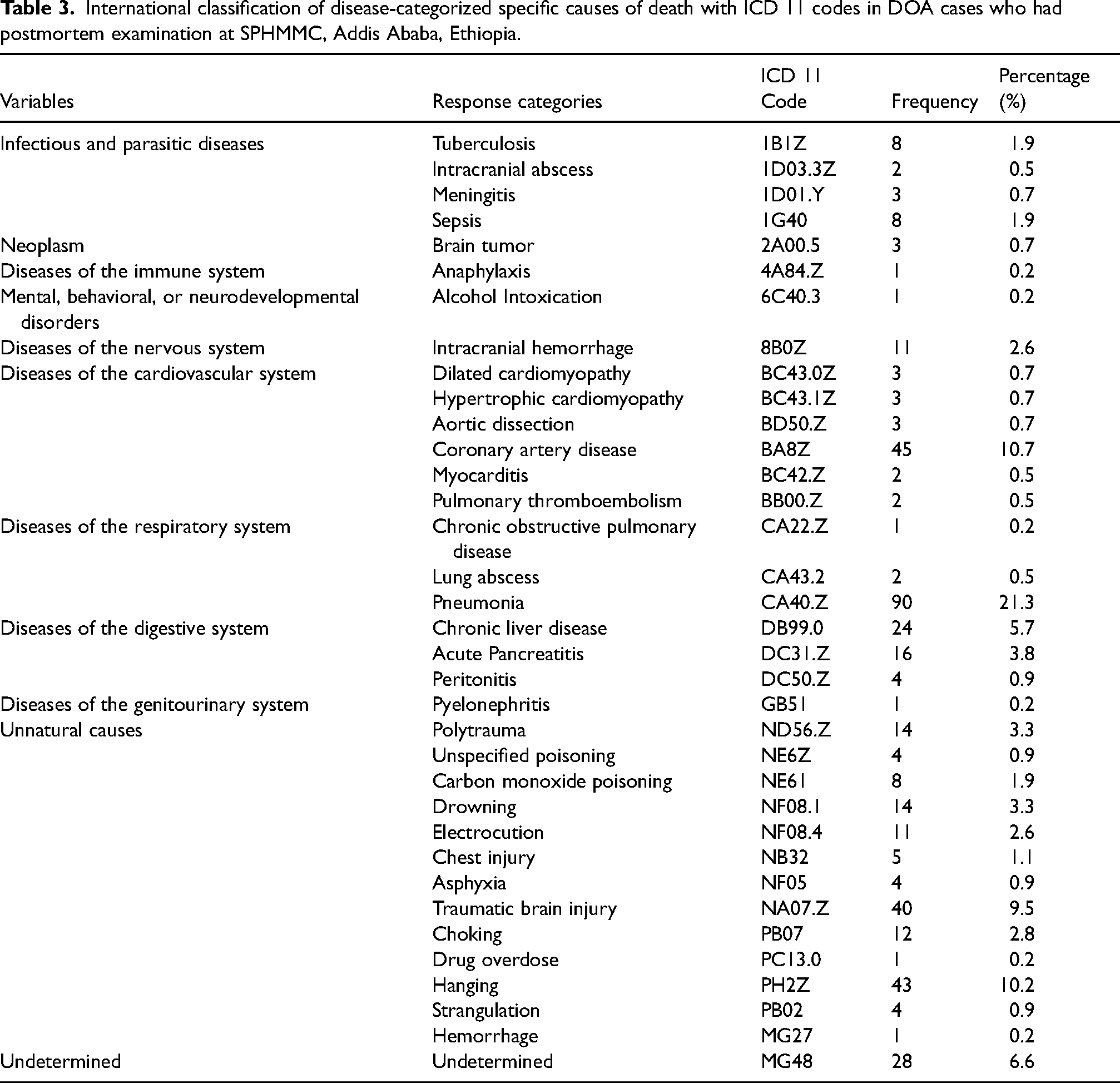
Pneumonia (21.3%) and coronary artery disease (10.7%) were the leading specific CODs. The cause of death remained undetermined in 6.6% of cases. For cases with determined causes, unnatural deaths (41.1%) were the predominant cause, followed by communicable diseases (30.2%) and non-communicable diseases (28.7%) (Table 3).
International classification of disease-categorized specific causes of death with ICD 11 codes in DOA cases who had postmortem examination at SPHMMC, Addis Ababa, Ethiopia.
Associations of sociodemographic variables with communicable, non-communicable, and unnatural causes of death
In the logistic regression model, age, sex, and residence were considered. Bivariate analysis showed residence was associated with CD-related and unnatural deaths. Age was associated with NCD-related and unnatural deaths.
In multivariate analysis, urban residents had 2.9 times (AOR: 2.846 [95% CI: 1.286,6.296]) higher odds of dying due to CD compared with rural residents. The odds of dying due to NCDs among individuals aged 15–29 years decreased by more than 80% (AOR: 0.194 [95% CI: 0.050,0.748]) compared to those older than 75 years (Table 4). The odds of dying due to ECs were five times higher among 15–29 years of age (AOR: 5.091 [95% CI: 1.097,29.628]) compared with those older than 75 years. In addition, urban residents had 71% (AOR: 0.293 [95% CI: 0.154,0.556]) lower odds of dying due to ECS compared with rural residents (Table 4).
Factors associated with communicable diseases, non-communicable diseases and unnatural causes of death in DOA cases who had postmortem examination at SPHMMC, Addis Ababa, Ethiopia.
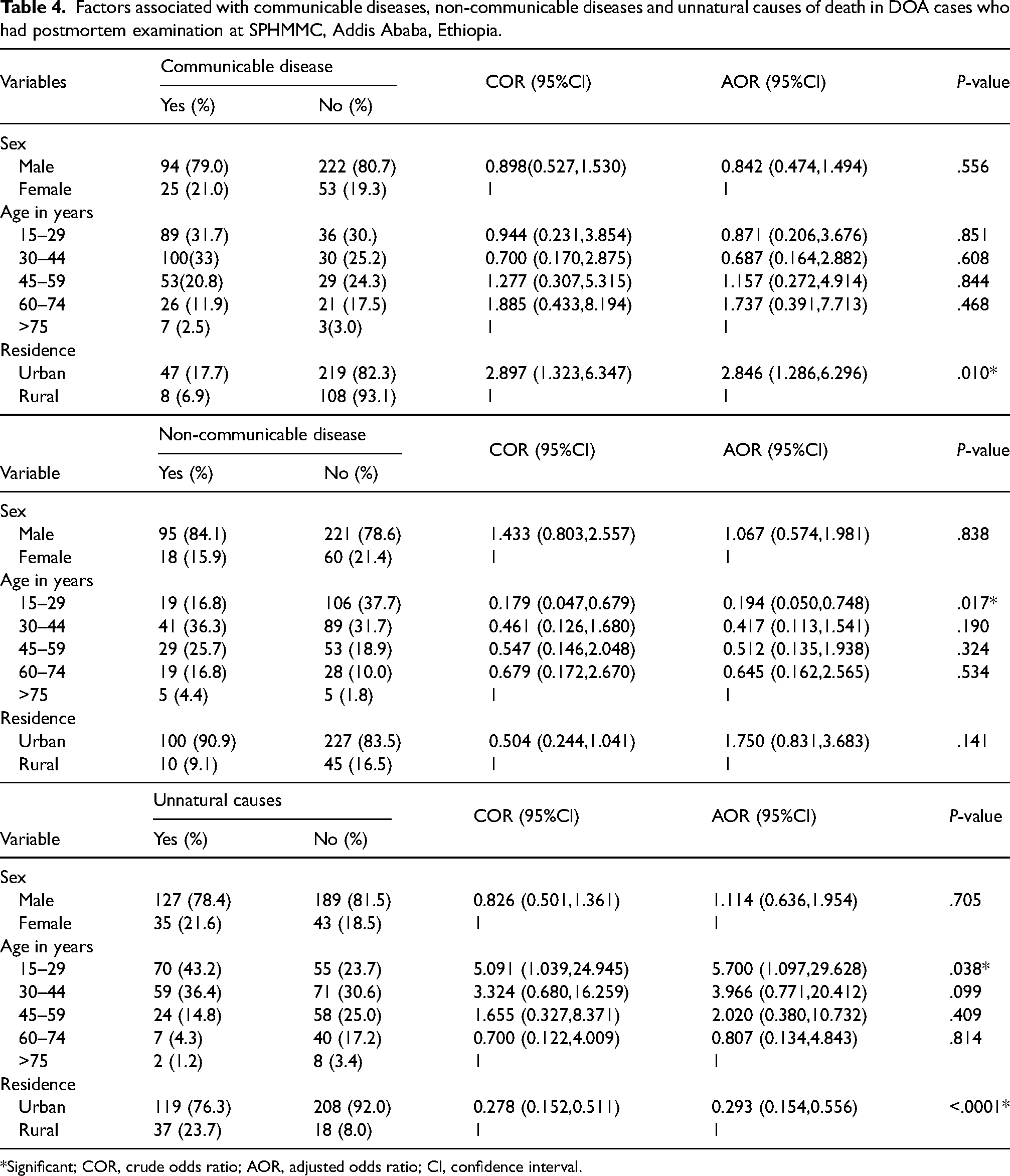
*Significant; COR, crude odds ratio; AOR, adjusted odds ratio; CI, confidence interval.
Discussion
This is the first autopsy-based study on DOA cases in Ethiopia, offering foundational insights into the prevalence, causes, and influencing factors crucial for intervention development. Notably, the study revealed that DOA cases accounted for approximately 32.5% of all autopsies, consistent with findings from Ghana (31.1%) but higher than rates reported in Nigeria (4.2% and 3.5%).12–14 This disparity likely stems from varied study contexts, with SPHMMC serving as a key forensic pathology hub in Addis Ababa catering to cases from most regions of Ethiopia. The higher prevalence of DOA cases hints at underlying issues such as limited healthcare access, deficient transportation services, delayed medical assistance seeking, and cultural beliefs influencing prompt care-seeking behavior. Inadequate prehospital care, particularly in remote or rural areas, exacerbates delays in medical interventions and transport to healthcare facilities, increasing DOA rates. Furthermore, a lack of awareness about the need for urgent medical care in emergencies leads to delayed treatment and more DOA cases, highlighting DOA as a significant public health issue nationwide.
In this study, the leading specific causes included pneumonia (21.3%) and coronary artery disease (10.7%). Unnatural deaths (41.1%) emerged as the predominant contributors to mortality, followed closely by communicable diseases (30.2%) and non-communicable diseases (28.7%). This finding contrasts with studies in northern Ethiopia, where unnatural deaths accounted for 12.3% of deaths, 15 but aligns with previous autopsy-based research in Ethiopia. 16 This discrepancy could be due to differences in the study populations, as the characteristics of DOA cases may differ from those of the general population. The high proportion of unnatural deaths in DOA cases may be linked to accidents, injuries, and violence prevalent in Ethiopia, including road traffic accidents, workplace incidents, interpersonal violence, and self-harm. Factors such as inadequate infrastructure, safety deficiencies, and limited emergency services likely contribute to this trend, emphasizing the need for enhanced safety measures, accident prevention strategies, and violence reduction efforts.
Residence and age were pivotal factors linked to unnatural deaths, with individuals aged 15–29 showing 5.7 times greater odds of mortality due to unnatural causes than those aged >75. This trend aligns with previous research in Ethiopia, reflecting the heightened vulnerability of younger individuals. 15 This vulnerability might be attributed to risky behaviors, a lack of safety awareness, and limited access to protective measures, emphasizing the need for targeted safety education among youth. 17 Rural inhabitants face heightened risks due to deficient infrastructure, sparse emergency response services, and elevated crime rates. Addressing these disparities mandates tailored initiatives promoting safety education, improving rural safety infrastructure, and fortifying emergency response capabilities.
Communicable diseases were the second leading COD (30.2%), consistent with studies in Ethiopia and globally.9,15,18,19 Notably, urban residents exhibited higher CD-related deaths compared to rural counterparts, likely due to urban population density, overcrowded living conditions, inadequate access to clean water and sanitation, and heightened poverty levels. Informal settlements and slums within urban areas, lacking basic infrastructure, further exacerbate disease vulnerability. Targeted interventions in urban areas are imperative, encompassing improved healthcare access, sanitation facilities, hygiene practices, disease surveillance, and health education.
Non-communicable diseases accounted for 28.7% of deaths, highlighting the growing impact of lifestyle-related risk factors such as unhealthy diets, physical inactivity, tobacco use, and excessive alcohol consumption. Addressing NCDs requires comprehensive strategies focusing on promoting healthy lifestyles, early detection, and improving healthcare access.
This study revealed a notable gender discrepancy in DOA cases, with over two-thirds involving males. Possible factors include occupational risks, violence exposure, or variations in healthcare-seeking patterns. Further research is essential to pinpoint causative factors and formulate tailored interventions. Additionally, a significant portion of DOA cases fell within the 15–44 age group, highlighting the profound impact of untimely deaths on the younger population. Premature fatalities in this age group can yield enduring social and economic repercussions for families and communities, warranting focused attention and comprehensive strategies.
However, there are limitations to consider. This study was conducted during the COVID-19 pandemic (2021), a period marked by lockdowns, changes in healthcare access, and other pandemic-related factors that may have influenced mortality patterns and access to medical care. These factors could have affected the characteristics of DOA cases during this time. As the data from this period may differ from pre- and post-pandemic trends, we recommend that these contextual factors be considered when interpreting the findings. Additionally, this study was based on retrospective autopsy data and did not collect detailed information on the underlying factors contributing to DOA cases. Future research could involve comprehensive investigations, such as postmortem examinations, medical record reviews, and interviews with family members or witnesses, to gain a more in-depth understanding of these cases.
In conclusion, the high percentage of BID cases mainly impacting the younger population from both rural and urban communities in Ethiopia is a concerning issue that requires urgent attention. The significant contributions of unnatural deaths highlight the need to focus on improving safety regulations, enforcing traffic laws, promoting workplace safety measures, and implementing violence prevention programs as well as strengthening emergency medical services. Pneumonia and coronary artery disease were the leading specific CODs. This highlights the importance of disease prevention and access to healthcare services in reducing mortality rates. Further research is needed to gain a deeper understanding of the underlying factors contributing to these causes of death and to guide effective interventions.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.