
Abstract
Sudden deaths may result from many conditions which are either not apparent at autopsy or might be missed and such cases can be tricky as there is no definite cause of death. One such entity is Intracranial colloid cysts, they are congenital neuroepithelial cysts which might be missed or might rupture at the time of dissection. They typically arise within the third ventricle of the brain and can pose a significant risk of sudden death if left undiagnosed or untreated. These are rare entity and on cut-section, these cysts contain mucoid and gelatinous material. In this paper, we have discussed in depth about five cases of colloid cysts, most of which were brought dead to the hospital and were discovered during autopsy without any prior history suggesting the same.
Introduction
The relationship between a forensic pathologist and sudden death is indispensable, and many neuropathological abnormalities are seen while dissecting the brain. However, some cystic lesions, like colloid cysts, are relatively rare entities. Colloid cysts are congenital neuroepithelial cysts or can also be termed as benign supratentorial lesions. If left undiagnosed or untreated, they pose a significant risk of sudden death.
Colloid cysts typically develop slowly, with symptoms appearing in individuals between 20 and 50 years old. 1 They constitute approximately 0.2% to 2% of all brain tumors and about 15% to 20% of masses found within the brain's ventricles. 2 Symptoms of colloid cysts can include headaches, difficulty walking, and memory loss (short term). Certain patients also experience intermittent symptoms as a result of periodic blockage/obstruction at the foramen of Monroe.3,4 In case of sudden obstruction at the level of ventricles, there is rapid increase in intracranial pressure (ICP) which can cause herniation and potentially lead to sudden death. 3
The mechanism associated with sudden decompensation and death is still controversial, however, various theories have been suggested. Some of the theories are; (a) The sudden worsening of symptoms may be linked to the movement of the cyst over its surroundings (the cysts attachment to the tela choroidea) thereby causing intermittent obstruction of the foramen of Monro and sudden intracranial hypertension and herniation.1,5 (b) Sudden bleeding within the cyst can lead to its rapid enlargement, and subsequent obstruction of the foramen could also be the culprit. 6 (c) Another hypothesis is the pressure of the cyst on the hypothalamus, which results in hypothalamic-mediated autonomic cardiac reflex control disruption leading to acute cardiac arrest, with or without pre-existing cardiac disease.7,8
The origin of colloid cysts remains uncertain, the origin is hypothesised with theories of a neuroepithelial origin from choroid plexus, ependymal, or paraphyseal epithelium origins. 9
In this paper, we present five cases of colloid cysts that were discovered only during autopsy. Most of the patients were pronounced dead on arrival or expired within minutes after being brought to the emergency room of the hospital. We shall present their prior symptoms, lab diagnosis if any and autopsy findings of the brain & other organs.
Cases
Case-1
A 32-year-old male was brought to the emergency room of the hospital at 12:08 am with an alleged history of shortness of breath and headache. He was pronounced dead within some minutes of hospitalization, and hence, a diagnosis was not made. On post-mortem examination, the brain was edematous and congested. On further sectioning, there was a solitary cyst inside the third ventricle that measured 2.5 cm in diameter and contained thick brownish gelatinous and mucoid fluid suggestive of a colloid cyst (Figure 1). The lateral ventricles were dilated. Both lungs were congested and edematous. All the other organ systems showed no abnormalities.
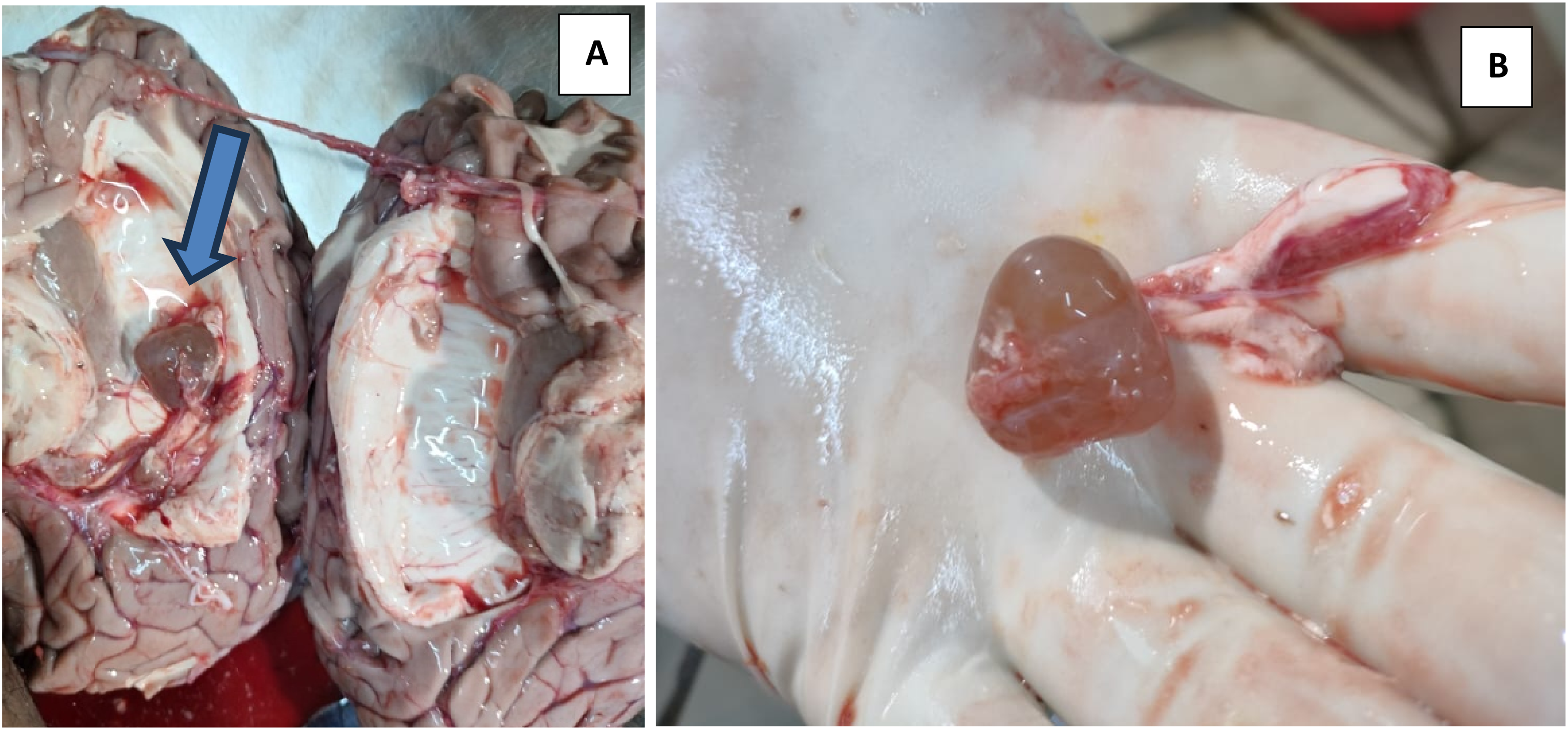
(A) 2.5 cm diameter colloid cyst (blue arrow) in the third ventricle with dilated lateral ventricle. (B) The colloid cyst is brown in color, containing gelatinous and mucoid fluid.
Case-2
A 28-year-old female with an alleged history of intermittent fever, headache, dizziness, abnormal body movements/shaking/involuntary throwing of body parts, crying spells and low mood for the last six months was brought dead to the emergency room of the hospital at 9:30am. Lab investigations conducted two days prior to her death revealed a bulky uterus and minimal free fluid in Pouch of Douglas suggestive of Pelvic Inflammatory Disease on ultrasonography. Results were negative for Malaria Serology (P. Falciparum and P. Vivax), Typhi dot (IgM IgG & IgM), and NS-1 Antigen. On post-mortem examination, the brain was edematous and congested. On cut section: A circular solitary cyst of size 0.5 cm diameter containing brownish gelatinous fluid was present in the third ventricle near the thalamic region of the brain, suggestive of a colloid cyst (Figure 2). The lateral ventricles were dilated. Both lungs were congested. All the other organ systems were congested and showed no other abnormalities.
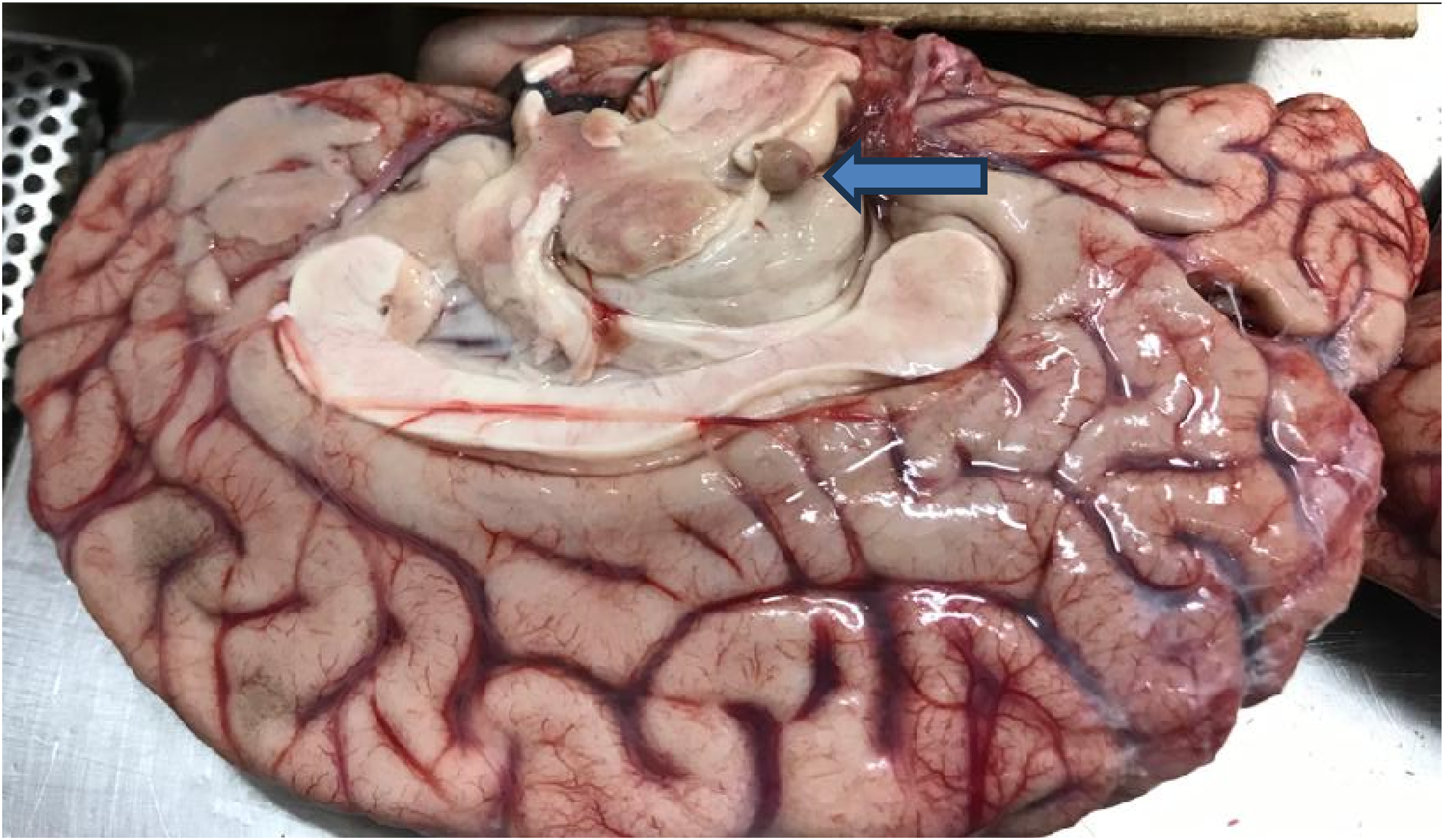
A 0.5 cm diameter, brown color colloid cyst (blue arrow) near the thalamic region.
Case-3
A 56-year-old male was brought to the emergency room of the hospital in a gasping state at 8:40 am. An NCCT head was done, which showed an ill-defined hypodensity in the bilateral medial thalamus and a diagnosis of? Infarct was made. He was managed conservatively. However, he expired at 09:40 am. No prior relevant history is present. On post-mortem examination, the brain was edematous and congested, and focal subarachnoid hemorrhage was present over the surface of bilateral cerebral hemispheres. On further examination, there was a giant solitary cyst inside the third ventricle that measured 4.2 cm in diameter, containing thick greenish-brownish gelatinous and mucoid fluid suggestive of a colloid cyst present (Figure 3). The lateral ventricles were dilated due to the cyst. Both lungs were congested and edematous. All the other organ systems showed no abnormalities.
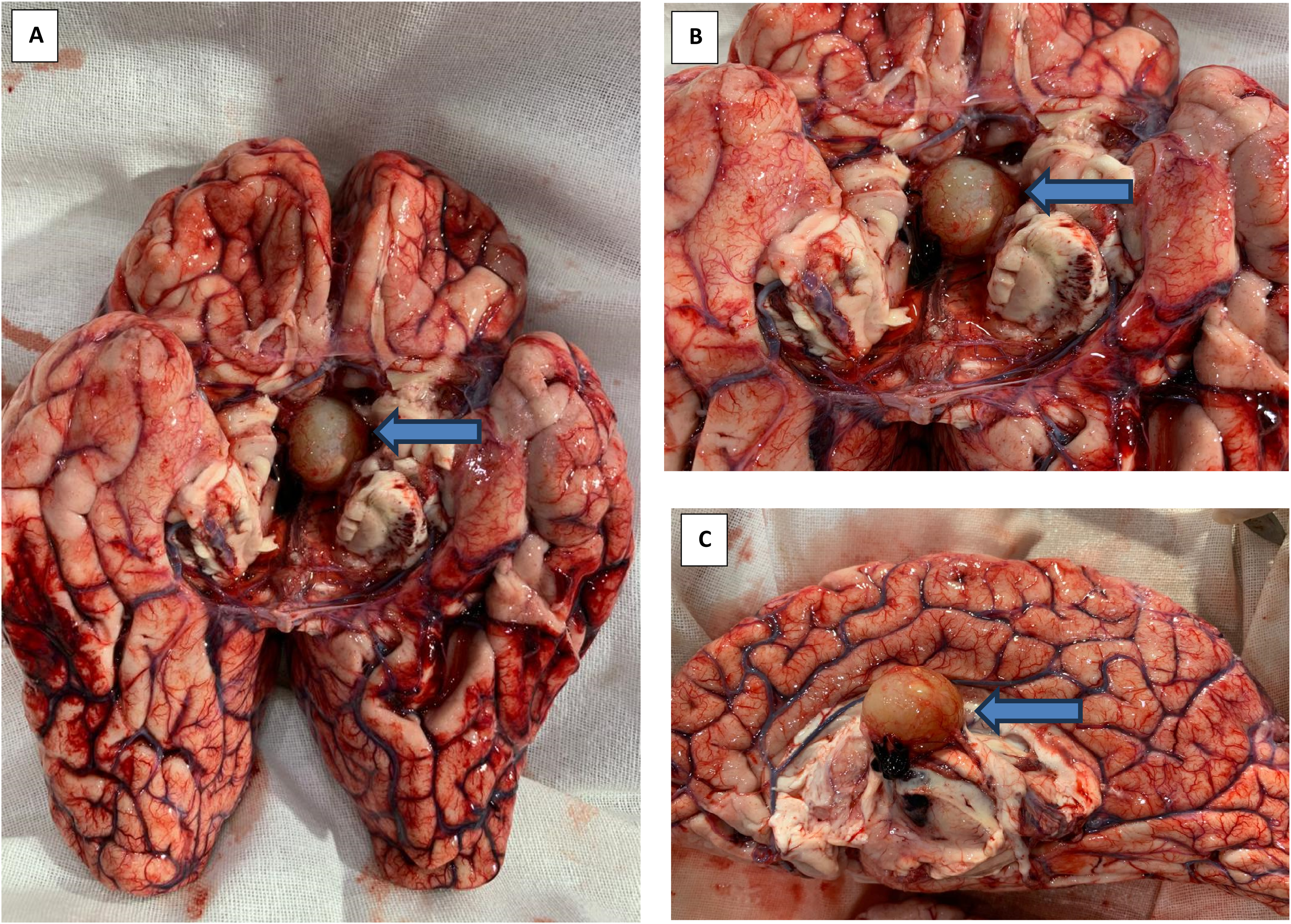
(A) 4.2 cm diameter colloid cyst (blue arrow) in the third ventricle. (B) The colloid cyst is brown in color, containing gelatinous and mucoid fluid. (C) Stalk of the colloid cyst (blue arrow) along with necrosis of the surrounding area of brain.
Case-4
A 36-year-old male was brought dead to the emergency room of the hospital at 5:30 pm. On post-mortem examination, the brain was edematous and congested, and on further sectioning, there was a solitary cyst inside the third ventricle that measured 3.0 cm in diameter and contained thick greenish-brownish gelatinous and mucoid fluid suggestive of a colloid cyst (Figure 4). Both lungs were congested and edematous. All the other organ systems showed no abnormalities.
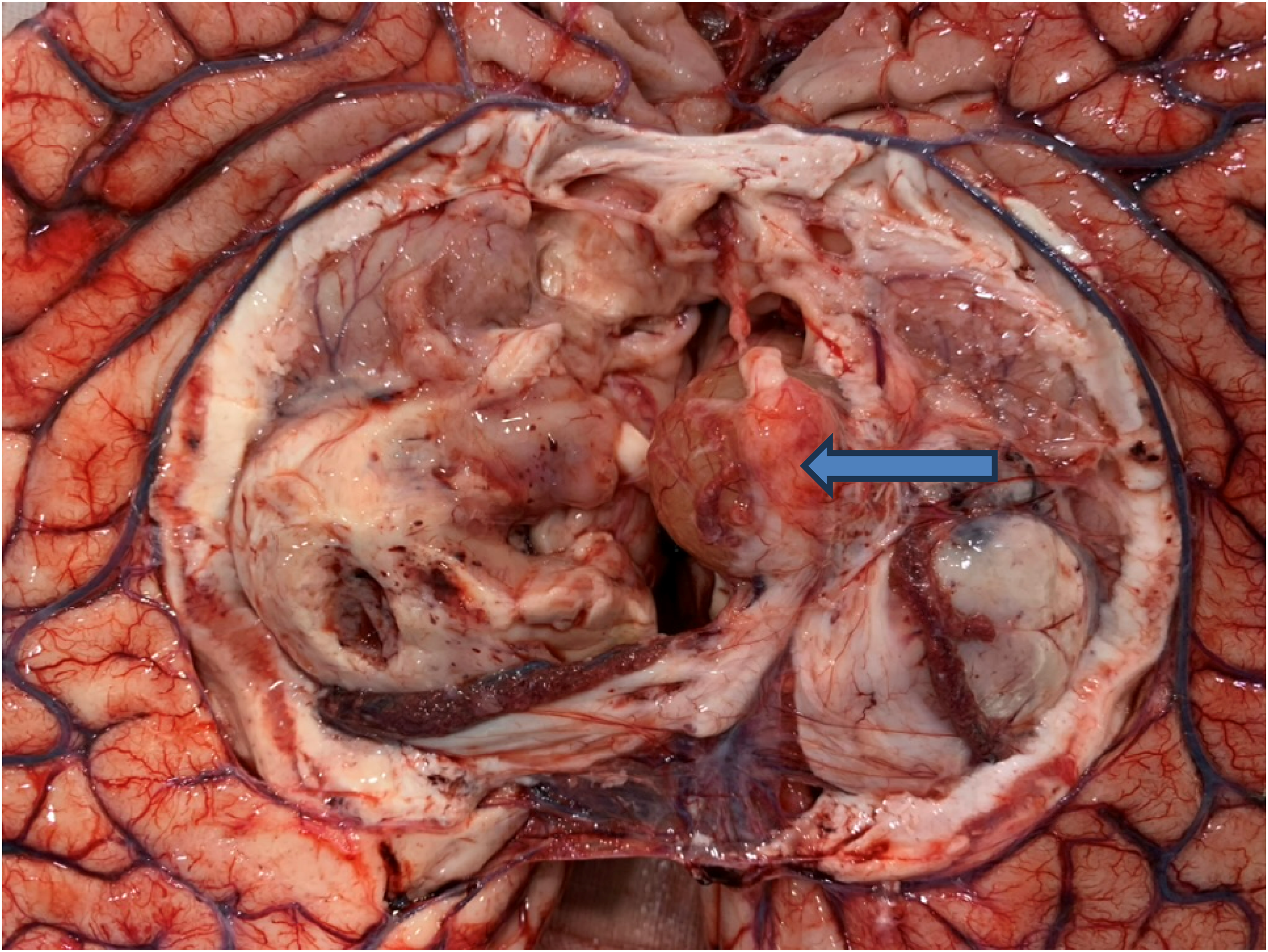
A 3.0 cm diameter, brown color colloid cyst (blue arrow) along with necrosis of surrounding brain matter.
Case-5
A 73-year-old male was brought dead to the emergency room of the hospital at 12:10 am. He had a history of some unknown illness for the past 1½ months. On post-mortem examination, the brain was soft, edematous, and congested, and on further sectioning, there were two solitary cysts inside the third ventricle that each measured 1.5 cm in diameter and contained thick greenish-brownish gelatinous and mucoid fluid suggestive of a colloid cyst (Figure 5). Both lungs were adhered to chest wall at places and congested. The rest of the organ systems showed no abnormalities.
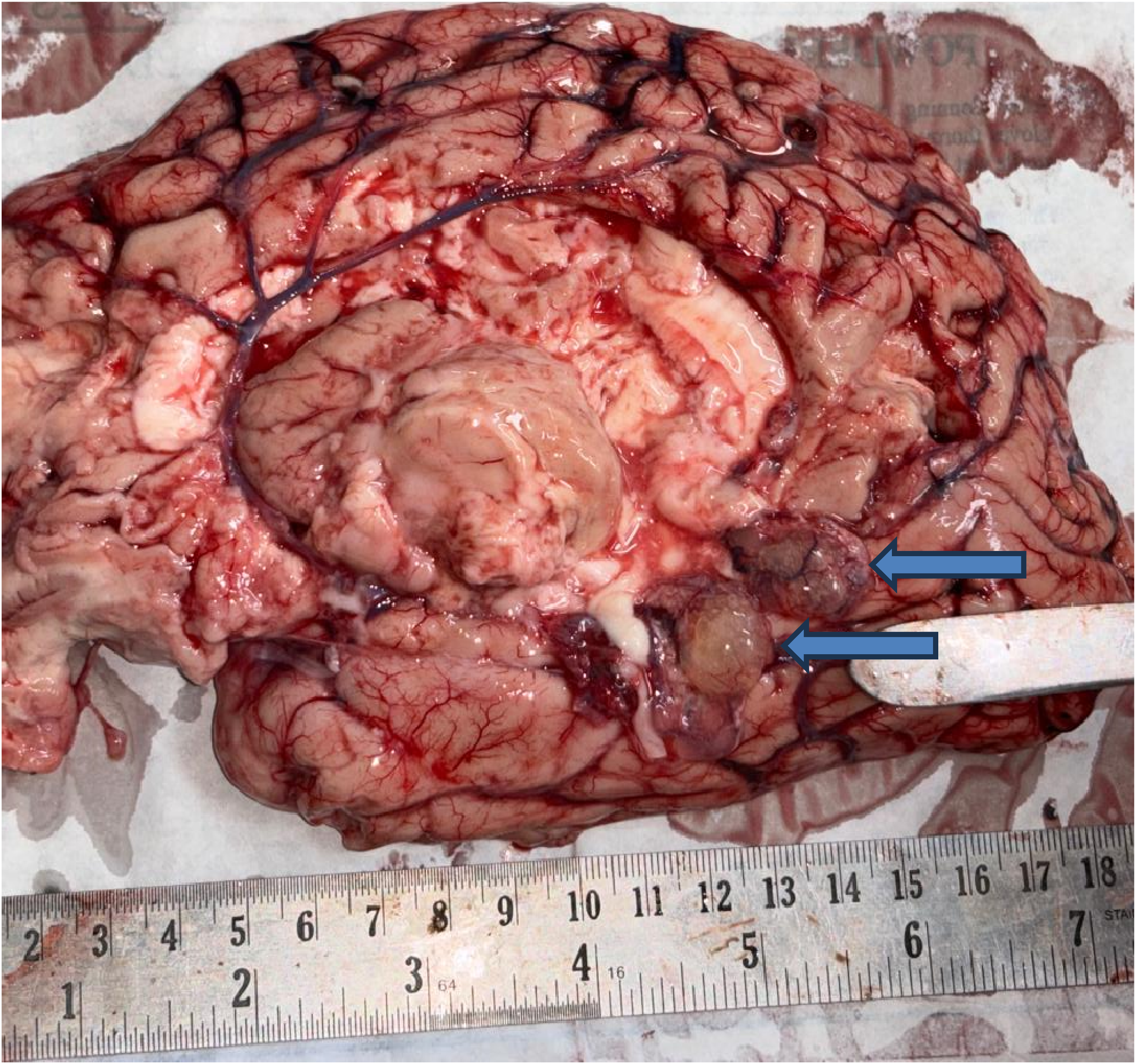
A 1.5 cm diameter, brown color colloid cyst (blue arrow) displaced from the third ventricle to lie over the cerebral cortex.
Discussion
Intracranial space-occupying lesions (ICSOLs) are described as a masses within the cranial cavity. They have a diverse etiology, and include benign or malignant neoplasms, inflammatory or parasitic lesion, hematoma, or arterio-venous malformation, 10 colloid cysts account for 1%–2% of ICSOLs. 11
Intracranial colloid cysts are congenital neuroepithelial cysts, which are benign supratentorial lesions. Some mention it as an endodermal congenital malformation. 12 These rare entity, contain mucoid and gelatinous material. They typically arise within the third ventricle of the brain and can pose a significant risk of sudden death if left undiagnosed or untreated. These cysts gradually enlarge and obstruct cerebrospinal fluid (CSF) flow, leading to obstructive hydrocephalus and, thus, increased intracranial pressure (ICP).
The most common clinical symptom is an episodic headache, which results from obstruction of CSF flow, however, non-specific signs and symptoms are predominant. Since most of them have headaches, it might be misinterpreted as either migraine headaches, Infarcts, transient ischemic attacks, or other brain tumor entities.13,14 As mentioned in case-1 and case-2, both of them had a prior history of headaches, and in case-3, an NCCT head was done, and a diagnosis of ?infarction of the brain was made, which ultimately turned out to be a colloid cyst on autopsy. Patients may also have vague neurological manifestations, as was seen in case 2.
Clinically, the signs and symptoms (mainly headache) can appear at any age, but the cysts do not usually become symptomatic until the third or fourth decade of life. Of the 5 cases encountered in this study, the age range is between 28 years and 73 years.
The diameter of colloid cysts varies from a few millimeters to several centimeters, with symptomatic cysts typically being 1–2 cm in diameter. 15 As per our cases, the cyst size was between 0.5 cm to 4.2 cm.
Human CSF production has a circadian variation, which has been demonstrated using magnetic resonance phase imaging. The average CSF production is at a minimum of around 18:00 h and has a night peak, about twice the daytime values, at around 02:00 h. 16 However, none of our cases showed any such association.
On autopsy, the macroscopic examination of cases of intracranial colloid cyst shows a circular solitary cyst inside the third ventricle of varying size containing thick brownish gelatinous fluid and mucoid fluid. The cyst not only obstructs the outflow of CSF, but as the size increases, it causes pressure necrosis of surrounding areas of the brain, like the hypothalamus, as seen in case 3 and case 4. Perimesencephalic nonaneurysmal subarachnoid hemorrhage is the benign form of subarachnoid hemorrhage, though its underlying cause remains unidentified and also debatable. 17 We found subarachnoid hemorrhage in case 3, whose source remained unclear, whether its occurred due to colloid cyst enlargement or due to the fall after developing neurological symptoms. An alternative mechanism or sudden death in addition to CSF outflow obstruction can be due to compression of hypothalamic structures, which have centers for cardiovascular regulation leading to reflex cardiac effects. Care must be taken while dissecting the brain as these cysts might either get displaced or might rupture as seen in case 5.
Conclusion
The observation made from the five cases confirms that even though the intracranial colloid cyst of the third ventricle is rare and a benign tumor, it can cause sudden death irrespective of its size. Amongst all the sudden death cases encountered at autopsy, the diagnosis of colloid cysts must be considered even if they are found incidentally. Neither the age of the deceased, gender, size of the cyst, degree of third/lateral ventricular dilatation, nor the duration of clinical symptoms appear to provide reliable indicators of the risk of sudden death. Since small cysts might be missed during dissection or might carry a risk of being ruptured while dissecting the brain, utmost care must be taken. The role of virtual autopsy, which includes postmortem computed tomography (PMCT) prior to traditional autopsy, enhances the chance of detecting colloid cysts. If a patient presents with intermittent headache, colloid cysts must be kept as one of the differential diagnoses, even if they are a rare entity. Early detection followed by a total excision carries an excellent prognosis. Prompt neurosurgical intervention can be lifesaving.
Footnotes
Authors contributions
Munesh Kumar- Conception, design and drafting of the article. Sunita Das- Conception and design of the article. Vijay Sharma- Critical revision and approval of the version to be published. Deep Roy- Critical revision and approval of the version to be published. S.K. Tandon- Critical revision and approval of the version to be published.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.