
Abstract
Recent decades have been characterized by an exponential increase in medico-legal litigation and an accentuated interest in healthcare responsibility. This study aims to examine cases of alleged medical negligence in Cardiology and Cardiac Surgery in one of the largest hospitals in north-west Italy, over a 11-year period (2013–2023). The primary objective of this study is to conduct a comparative analysis between compensation claims initially advanced by patients (or their legal representatives) in the pre-trial phase and the final outcomes of legal proceedings brought before the court. This article provides an important opportunity for a critical and in-depth analysis of litigation in the fields of cardiology and cardiac surgery, with the aim of improving the efficiency of case management.
In the period 2013–2023, San Martino Polyclinic Hospital received a total of 1704 compensation claims, of which 39 (2.29%) were related to alleged cardiological and cardiosurgical professional liabilities. About 64.10% of the compensation claims (25 out of 39) were deemed illegitimate due to the absence of professional responsibility, and were therefore rejected by the Claims Management Committee (CMC). In 38.5% of cases, legal action was pursued, and in four cases, the hospital was ordered to compensate the patient for medical negligence. Conversely, in three cases, the Judge's ruling was in favour of the Hospital. Currently, eight legal actions remain ongoing, and their outcomes are pending.
Overall, over the 11-year study period, litigation cases in the cardiology and cardiac surgery fields were relatively infrequent.
Introduction
The last decades have been characterized by an exponential increase in medical-legal litigation and interest in healthcare responsibility. 1 While the likelihood of facing a lawsuit varies depending on the medical specialty, approximately one in three physicians can anticipate being sued at least once during their professional lives. 2 Currently, medical liability has become a major pitfall in modern healthcare practice. 3 A claim for medical malpractice falls within the context of civil law, where a medical error constitutes a tort, meaning an action that grants the patient the right to obtain compensation from their healthcare providers for damages suffered. 4 Civil law establishes what constitutes legal harm and defines when an individual can be held liable for such harm, thus ensuring that victims have the opportunity to obtain redress. In these cases, patients must demonstrate in court several fundamental elements: the existence of a duty of care owed by the physician to the patient, the breach of that duty through conduct that deviates from accepted standards of medical care, the causal link between the breach of duty and the damages suffered by the patient, and the demonstration of such damages. The possibility of being sued for medical malpractice represents a significant concern for all physicians, but is particularly felt among specialists such as cardiologists and cardiac surgeons, whose areas of practice are considered high-risk from a legal liability standpoint. The frequency of serious adverse events and complex interventional procedures significantly increases the risk of medico-legal disputes. 4 Given the high prevalence of cardiovascular diseases, the costs and consequences of questions and lawsuits in this area, a complete and in-depth analysis approach is essential.5–7 Relevant bibliographic sources8,9 indicate that over 98% of physicians in these specialties will face claims for compensation for negligence by the age of 65. Cardiac care is notoriously high-risk: for example, an analysis of 114,233 patients undergoing coronary artery bypass grafting revealed a 13.64% incidence of at least one complication (reoperation, hemorrhagic or postoperative shock, adult respiratory distress syndrome, hemodialysis, stroke, infection or sepsis).8,9 According to some insurance data, lawsuits in cardiovascular surgery are second only to those in orthopedics, gynecology, emergency surgery and general surgery. Furthermore, when they occur, these lawsuits often lead to high compensation amounts and a significant economic impact on the health system.5,10 In Italy, Law No. 24 of 2017 shifted the responsibility and costs of legal defenses onto healthcare facilities, to protect individual doctors from an excessive number of lawsuits. 5 The Liguria Region, since 2012, has created a protocol with a self-insurance system for healthcare companies, and compensations are paid by a regional fund. The protocol also defines how to manage complaints with the aim of reducing compensation costs, encouraging agreements without going to court and speeding up dispute resolution. The initial phase of a complaint involves collecting the necessary documents and appointing a medical examiner to assess the case. The medical examiner expresses an opinion to establish whether the damage is compensable and what amount is appropriate. Subsequently, an insurance expert summarizes the documentation and presents it to the Claims Management Committee (CMC), composed of medical and legal experts. The CMC decides whether to accept or reject the compensation request. If the request is accepted, a sum is proposed and, after acceptance, an agreement is signed. If the request is rejected, the insurance expert explains the reasons for the rejection. An additional “Regional Claims Committee” can provide a second opinion for cases with compensations equal to or greater than €150,000. 1
This study aims to examine the lawsuits for alleged medical negligence in Cardiology and Cardiac Surgery related to the San Martino Polyclinic Hospital in Genoa over 11 years (2013–2023). The main objective of this study is to conduct a comparative analysis between the claims for compensation initially advanced by patients (or their lawyers) in the pre-trial phase and the final outcomes of the lawsuits brought forward in court. This study represents an important opportunity to critically and in-depth analyse the phenomenon of litigation in the cardiology and cardiac surgery fields, with the aim of improving the efficiency of managing these cases.
The aim of the study is the description of CMC data, its perspective and the litigation scenario, including court management.
Materials and methods
Data concerning compensation claims related to alleged cardiological and cardiosurgical professional responsibilities received by the Claims Management Committee (CMC) of San Martino Hospital in Genoa during the decade 2013–2023 were collected.
We proceeded to analyze the health documentation relating to the cases of litigation received by the Legal Office of the San Martino Polyclinic Hospital and the related administrative and judicial procedures, from the initiation to the possible resolution.
The following data were examined:
type of the compensation request; whether or not the CMC formulated a conciliation proposal; reason for the recourse to the judicial phase, distinguishing between rejection of the compensation request or rejection of the other party's conciliation proposal; outcome of the judicial phase.
All compensation claims (whether resulting in biological damage or death) related to nosocomial infections acquired during hospitalizations were excluded from the analysis, with the exception of specific cases of infections directly related to the cardiological or cardiac surgery condition (for example, sepsis). Therefore, only surgical site infections, pericarditis, myocarditis and endocarditis were included.
The evaluation of medical malpractice claim cases was performed in different phases: initially, the case was assessed by the expert in Forensic Medicine who visited the patient (if still alive) and drafted a preliminary report. Subsequently, the case was analyzed by the CMC in which the expert in hygiene and preventive medicine, in Forensic Medicine and the Lawyers also provided their opinion. Therefore, a final report was drafted and based on this the decision to reject the request or propose an out-of-court conciliation solution was made. For each case of alleged claim for compensation for medical negligence in cardiology or cardiac surgery, the following were collected: preliminary Medical-Legal opinion; CMC assessment, evolution of the medical malpractice claim after the CMC decision (withdrawal of the claimant, mediation or civil proceedings) and the conclusion of the medical malpractice claim (also in economic terms) (Figure 1).

Flowchart detailing the procedural workflow for litigation case handling.
Results
Up to and including 2023, the hospital had 1217 patient beds.
In the period 2013–2023, San Martino Hospital received a total of 1704 compensation claims, of which 39 (2.29%) were related to alleged cardiological and cardiosurgical professional liabilities.
From the study of the 39 medical records relating to the selected cases, a prevalence of male involvement emerged (24 cases) with a mean age of 61.25 years, while for females (15 cases) it approximated 65 years.
With regard to the procedural outcomes, 23 cases (59%) resulted in death, of which 13 followed complications of cardiological events and 10 followed complications of cardiac surgery. Analysing solely the compensation claims that were the subject of litigation, a substantial stability emerged in relation to the number of events per year, with an overall reduction in the post-pandemic years (five cases in 2013, seven cases in 2014, six cases in 2015, four cases in 2017, three cases in 2018, five cases in 2019, one case in 2020, four cases in 2021, zero case in 2022 and one case in 2023), considering that in Italy there is a 10-year deadline to present the claim.
The time range (2013–2023) indicates the period during which the claims were received by the Hospital's Legal Office; however, in any case, all of the healthcare events occurred within the same 2013–2023 timeframe (Tables 1 and 2).
Summary of cardiological and cardiac surgery cases.

Summary of healthcare litigation cases, detailing their evolution into either out-of-court settlements or judicial proceedings, including eventual compensation awards.
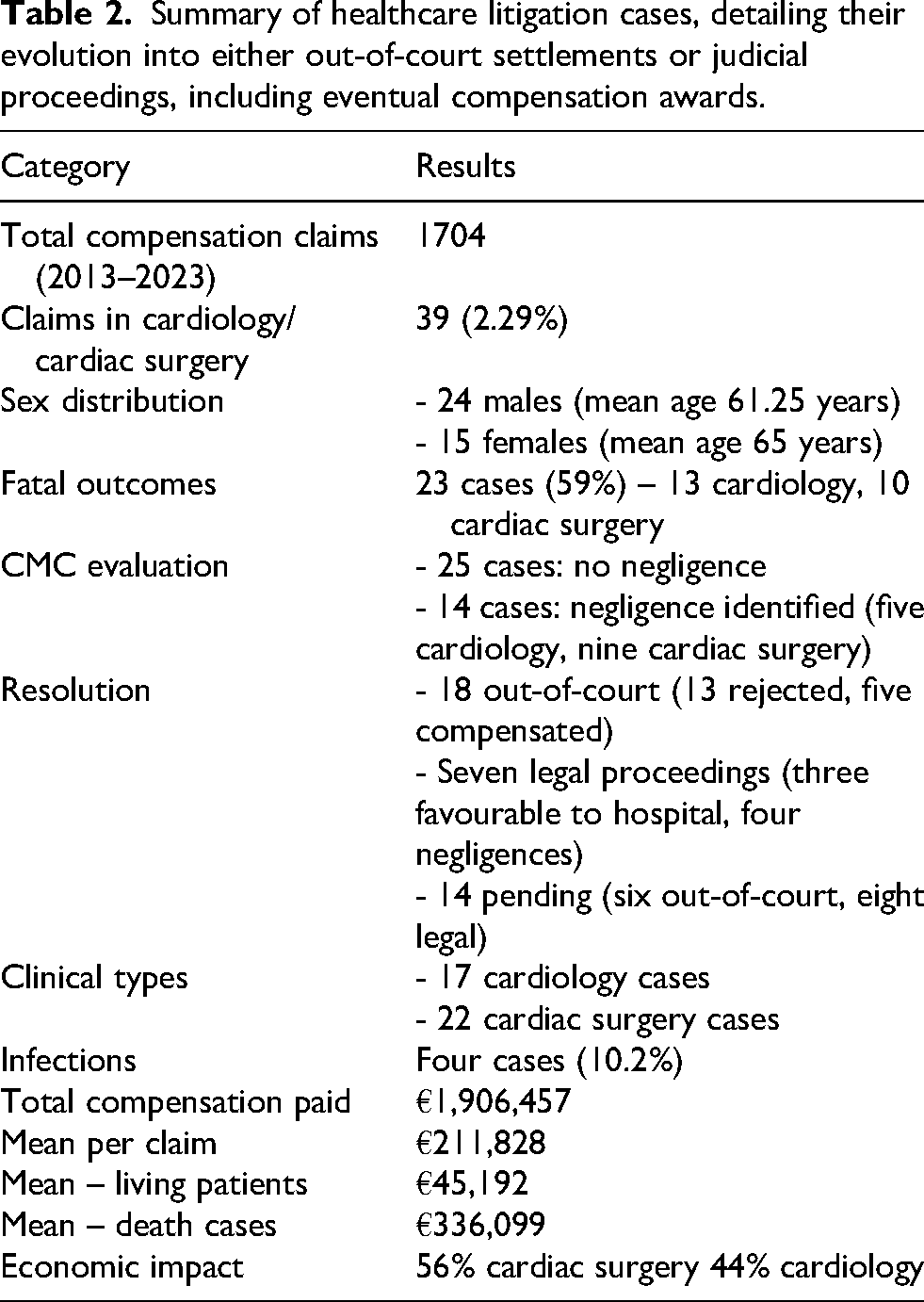
Overall, the Hospital's Claims Management Committee rejected the request (i.e., did not identify medical negligence) in 25 cases.
In 14 cases medical negligence was identified (of which five were in the cardiology field and nine were in the cardiac surgery field). However, a monetary agreement was reached with the patient in only five cases. In four cases, the patient did not accept the financial offer (legal proceedings were initiated) and in five cases, financial negotiations are still pending.
There were 18 cases resolved out of court: 13 cases were rejected by the Hospital's Claims Management Committee and did not proceed to judicial evaluation; in five cases, medical negligence was acknowledged and compensation was issued.
There were seven cases resolved through legal proceedings: in three cases, the judgment was in favour of the Hospital and medical negligence was not identified by the Judge; in four cases, medical negligence was identified.
There are six cases currently pending out of court: in five cases, negligence by the Hospital was acknowledged and negotiations on the compensation amount are underway; one case was recently rejected and judicial follow-up is awaited.
There are eight cases currently pending legal proceedings, and in all these cases, the Claims Management Committee had not identified medical negligence. Therefore, the patients sought judicial evaluation.
From a strictly clinical perspective, it was observed that of the 39 requests:
Seventeen cases were of a cardiological nature, specifically 10 concerned the diagnostic and therapeutic management of cardiac pathologies; five cases concerned interventional procedures; two cases concerned complications of coronary angiography.
Twenty two cases were of a cardiac surgery nature, and 15 concerned aortic and/or mitral valve replacement; five cases related to aortocoronary bypass; one case concerned valve replacement and aortocoronary bypass, and one case was related to ascending aorta replacement. Among these cases, an infection was present in four (10.2%) instances, following the provision of healthcare/medical treatment.
The study indicates that a total amount of €1,906,457 has been disbursed, to date, upon conclusion of nine disputes (five cases were resolved out-of-court, and four cases were resolved after legal action). The mean amount disbursed per claim is therefore €211,828; however, a distinction must be made between the mean amount disbursed for damages to a living patient, which is approximately €45,192. The mean amount disbursed for claims resulting in death, for which the mean outlay was approximately €336,099. The economic impact of cardiac surgical complications on the total was 56% while the remaining 44% was related to complications in clinical cardiology setting.
Discussion
The principal finding of this study is that a limited proportion of malpractice claims in cardiology and cardiac surgery resulted in confirmed medical negligence, reflecting the effectiveness of structured claims management and interdisciplinary evaluation.
According to the literature, adverse events in the medical field can occur either due to medical errors or in the absence of such incompetence or negligence. In the latter case, we refer to a “complication,” which is an event that, although foreseeable, cannot be avoided. 1
Regarding medical negligence litigation in Italy, the “Medmal Claims Italy Report” 11 analyses the period 2004–2020 in 67 healthcare facilities across 15 Italian regions. The report, based on approximately 30,930 claims, indicates that the most common errors are surgical errors (21.6%), followed by diagnostic errors (20.3%) and therapeutic errors (12.1%). Other causes include nosocomial infections (4.8%), invasive procedures (3.8%), accidental falls (13.6%), childbirth-related errors (2%) and anaesthesiologic issues (1.9%).
In our study, litigation was resolved out of court in about 46% of cases. In our assessment, the evaluation by the CMC facilitated a reduction in cases concluded through judicial proceedings, thereby decreasing litigation costs.
About 64.10% of the compensation claims (25 out of 39) were deemed illegitimate due to the absence of professional liability, and were therefore rejected by the CMC. Of these cases, 52% (13 cases) were closed without follow-up due to abandonment by the claimant and expiration of the statute of limitations, suggesting that numerous claims were initiated in an unsubstantiated manner.
Overall, in 15 cases (38.5%), legal action was pursued, and in four cases, the Hospital was ordered to compensate the patient for medical negligence. Conversely, in three cases, the Judge's ruling was in favour of the Hospital. Currently, eight legal actions remain ongoing, and their outcomes are pending.
Overall, based on the evaluations by the CMC and the Judge, medical error/negligence was ascertained in 14 cases (35.9%). However, these data are provisional, as an additional eight cases are under judicial review.
The Clinical Medical Committee (CMC) played a crucial role in managing litigation, demonstrating a significant impact in terms of both efficiency and cost containment. It is notable that approximately one-third of the total requests were rejected in the preliminary phase by the CMC, thus preventing the claim from progressing to more costly and prolonged legal stages. This finding not only attests to the effectiveness of the preliminary screening exercised by the CMC but also suggests that a relevant proportion of the compensation claims lacked objective foundation. The acceptance of the CMC's conclusions by the patients or their family members in these cases demonstrates the efficacy of the internal analysis in recognizing and communicating the appropriateness of the care provided, thereby ruling out the presence of professional liability or malpractice.
From a clinical perspective, the analysis revealed an asymmetrical distribution of accepted claims across disciplines: the CMC accepted nine cases of liability in the Cardiac Surgery field, a value almost double that found for Cardiology. This disparity suggests greater intrinsic complexity or a higher iatrogenic risk associated with major surgical procedures.
The specific etiological analysis within the CMC accepted cases shows a heterogeneous picture, without highlighting a specific predominant origin. However, certain clusters of events warrant attention: two of the cardiology claims specifically concerned complications arising during coronary angiography, while two accepted cardiac surgery events involved right atrial lacerations during valvular surgery.
Conversely, the cases rejected by the CMC consisted of 12 Cardiology cases and 13 Cardiac Surgery cases.
Comparing our data with those reported in the MedMal study, 11 we observe that the combined incidence of Cardiac Surgery and Cardiology in their sample (equal to 3.1% of total claims, with a slight prevalence in the Cardiology field compared to Cardiac Surgery, 1.6% vs. 1.5%) is higher than that found in our case series. This discrepancy could reflect a different screening methodology, or the effectiveness of the litigation management model adopted by our Hospital.
From an economic perspective, cardiac surgery cases exhibit a greater financial impact than cardiology cases, and in cases of mortality, the compensation amount was almost 10 times higher than the damages incurred by living individuals. To date, nine patients have been compensated, with an average of €211,828 per case. These figures are substantial and reflect the severity of cardiac pathologies and complications that result in significant morbidity.
Consequently, over the 11-year study period, litigation cases in the cardiology and cardiac surgery fields were relatively infrequent. In a substantial proportion of these cases, medical liability was not established. However, in cases where medical negligence was identified, the average compensation was considerably high. It must be considered that we evaluated a period of 11 years: the analyzed time window significantly influences the overall perspective.
In relation to previous research, the present results confirm certain trends already observed in national and international studies, although some discrepancies emerge that may reflect differences in case selection, healthcare systems, or medico-legal frameworks.
Analyzing the literature, a recent 9-year Chinese study examined 109 cases of medico-legal litigation related to coronary artery bypass grafting. According to the Authors, the median liability ratio was 30%. The primary postoperative complications in the disputed cases were: low cardiac output syndrome, postoperative hemorrhage, non-surgical site infections, surgical site infections, and arrhythmia. 12
Eltorai 8 analyzed 140 medico-legal litigation cases involving cardiac procedures. Cardiac surgeons were defendants in 47.8% of the cases, and cardiologists in 56.4%. Forty percent of the cases involved coronary artery bypass grafting, valvular surgery, or both; 50% of the cases resulted in a verdict favouring the defendant, 27.3% were decided in favour of the plaintiff, and 22.7% reached a settlement. According to the study, the most common cause of litigation was periprocedural error, most frequently attributable to inadequate adherence or fixation of the prosthetic valve (23.1%) or surgical site infection (15.4%). Catheterization constituted another prevalent cause of litigation (25%).
Wu et al., 13 in a 2017 article, analyzed malpractice litigation cases involving myocardial infarction in Taiwan from 2002 to 2013. They found that, out of a total of 36 cases, 28 resulted in the recognition of medical error, with an average payout of $100,639 ± 49,617. Cardiologists and emergency physicians were involved in 56.3% of the cases, with a favourable verdict in 92.6% of lawsuits. Other specialists, however, lost nearly 25% of the cases. The recognition of medical fault was mainly related to misdiagnosis of myocardial infarction in patients with typical chest pain and known coronary risk factors, failure to conduct a thorough medical assessment and appropriate investigations, and inadequate treatment.
Oetgen et al. 14 reported data on medical cardiovascular claims extracted from the registry of closed medical professional liability claims. Cardiologists were involved in 4248 claims out of a total of 230,624 (1.8%). In 18% of cases (770), liability was recognized, leading to compensation, with an average payout of $248,291. The most common error was misdiagnosis, particularly in relation to coronary atherosclerosis. Additionally, the authors highlighted that errors in the management of aneurysms and aortic dissections pose a high risk, as the percentage of paid claims is high, and the average compensation is particularly substantial.
Fernandez and Vidovich 15 analyzed claims related to cardiac tamponade from December 27, 2017 to November 19, 2018, using the LexisNexis Academic database. They identified 77 cases of medical negligence. Of these, 90% formally cited at least one physician, and 70% stated that the tamponade had an iatrogenic origin. Final rulings were in favour of at least one physician in 29% of cases, against at least one physician in 19%, while 17% of cases ended in a settlement.
Wang and Krishnan 16 analyzed cardiology claims from 2006 to 2015 in the United States, extrapolating data on a database of malpractice litigation liability insures, health systems and community hospitals. The authors showed an increase in claims from 2006 to 2015 of 91%; the main allegations were inappropriate medical treatment and diagnostic errors. However, 68% of compensation claims were dismissed, and 30% of the remainder were settled out of court.
To elevate the quality standards of healthcare, optimize risk management, and mitigate the frequency of complaints against cardiologists and cardiac surgeons, it is imperative to promote awareness and understanding of these issues. An approach that recognizes the analysis of medical errors as an opportunity for professional growth and continuous improvement is essential. 3
The sharing of medical error data facilitates the identification of critical areas and the development of targeted preventive strategies. This process mitigates the risk of future errors and enhances patient safety. Rather than solely imposing punitive measures for errors, such a system prioritizes the elucidation of root causes and the identification of effective solutions.
In cases where medical negligence in the cardiology field is suspected, it is imperative that the physician specializing in Legal Medicine seeks collaboration with specialists in cardiac pathology, cardiology, and/or cardiac surgery. Furthermore, adherence to specific guidelines for the analysis of cardiac-related deaths is necessary. This multidisciplinary and standardized approach is essential to ensure accurate medico-legal analysis and to prevent disputes, while contributing to the standardization of medical negligence assessments. 3
A comprehensive review of malpractice litigation in cardiology and cardiac surgery can elucidate common factors that predispose to adverse outcomes and facilitate improvements in clinical practice and preventive strategies. 8
Risk management, particularly in cardiology and cardiac surgery, necessitates a concerted commitment to risk mitigation and prevention. The integration of clinical practices, organizational frameworks, and regulatory compliance is paramount. 4
Finally, in terms of hospital resource management, the objective of extrajudicial litigation management is to expedite resolution and reduce compensation costs. However, should the medico-legal assessment, supported by experts in cardiology and cardiac surgery, identify compelling arguments in defense of the institution, progression to the judicial phase is advisable. Experience demonstrates that this course of action can yield substantial cost savings relative to compensation demands advanced by the opposing party.
In the context of cardiology and cardiac surgery, an effective risk management approach should focus not only on the identification of medical errors but also on their analysis as opportunities for professional growth and patient safety improvement. The findings of this study, showing a limited number of malpractice claims and a high proportion of out-of-court resolutions, highlight the effectiveness of a structured governance model based on interdisciplinary collaboration between medico-legal experts and clinicians. This model supports accurate evaluations, prevents unnecessary litigation, and contributes to the optimization of hospital resources. Such an approach is consistent with national and international trends emphasizing proactive risk management and system-based learning from adverse events. 17
The present findings have relevant implications for both clinicians and Forensic Medicine Specialists, as they highlight the importance of structured risk management systems and interdisciplinary collaboration in reducing litigation and improving patient safety.
The major limitations of the current study lie in its monocentric setting and the limited number of cases analysed. A further, significant constraint is the fact that 14 cases remain under evaluation due to protracted assessment periods and the inherent delays within the judicial system.
Broader multicenter investigations would help clarify the generalizability of these findings and support the development of national strategies to strengthen medico-legal governance and patient safety in cardiology and cardiac surgery.
Footnotes
Author contributions
Alessandra Zappi: conceptualization, investigation, writing – original draft, and methodology. Rosario Barranco: conceptualization, investigation, and methodology. Isabella Caristo: conceptualization, investigation, and writing – original draft. Francesco Ventura: conceptualization, investigation, and supervision.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Guarantor for the work
Francesco Ventura, Department of Legal Medicine, University of Genova, Via De’ Toni 12, 16132 Genova, Italy, tel + 39-010-3357838, fax +39-010-3537643, email: