
Abstract
Atypical gunshot wounds present a challenge for the forensic expert, and sometimes differentiating these from a blunt trauma can be difficult. A careful crime scene investigation can be helpful in finding additional evidence and clarifying the nature of the injuries. We describe a case of an unusual craniocerebral injury that was initially interpreted as a blow from a wooden object. The appearance of the wound lacked the classical characteristics of entrance and exit bullet wounds, but the investigation showed it was due to the ricocheting of a destabilized bullet. Potentially lethal, craniocerebral gunshot injuries are a common occurrence in developing countries even in non-conflict areas, with very bad outcomes even when treated aggressively in specialized neurosurgical facilities. The authors briefly discuss similar cases and opinions in the relevant literature, emphasizing the importance of a rational approach during the reconstruction of the crime scene.
Introduction
Gunshot wounds deserve special forensic evaluation due to the high mortality accompanying such events. Especially in developing countries, conflict areas or states with liberal policies regarding gun control, this type of wound has gained epidemic traits, and the prevalence of these occurrences is underreported. Some authors suggest classifying gunshot wounds or injuries (GIs) as a special form of blunt trauma. 1 The characteristic that separates GIs from other blunt traumatic events is the high velocity, and kinetic energy, that the missile, or the bullet, transmits to the tissues: hence use of the term “wound ballistics”. 2
Typical GIs leave little space to doubt the cause of the wound. However, the number of case reports of atypical wounds, with all the details related in this report (entrance or exit characteristics and trace wound patterns), show that these are a continuous challenge. 3 The recording and study of individual cases are continuously enriched with such atypical wound cases and patterns, and we previously reported a case of ours initially misinterpreted by the police as a GI. 4 Of course, several factors do play a role in the production of atypical GIs; the most important is the ricocheting of the projectile.1,2 Such a phenomenon is mentioned in notorious and unresolved cases of famous assassinations, including JFK. 5 Craniocerebral GIs account for a high portion of all lethal gunshots, with penetrating traumatic brain injury causing as many as 90% of all victims to die before arriving at hospital, and half of the remaining 10% will still die in the emergency departments. 6
Civilian casualties following gun assaults are a global issue of major concern, and easy access to weapons may be a facilitator. 7 Sources suggest a rise of gun violence in European countries, albeit Albania has no official prevalence data to offer. 8
We report the case of an unusual lethal wound in the occipital skull region of a victim, initially interpreted by the police as a blunt trauma due to a blow with a stick or other wooden object. Careful scrutiny of the scene raised several investigative doubts, and the event was thereafter registered as a gun crime.
Case report
A 37-year-old Albanian male was sent to a district hospital following craniocerebral trauma causing a deep wound in the occipital region of the skull, with profuse bleeding. His Glasgow coma scale upon arrival was 5 points (E = 2; V = 1; M = 2) and the surgeon on duty administered two packs of blood, as well as suturing the skull wound. Nevertheless, the patient did not survive and was declared dead approximately 60 min after admission, following brain trauma and haemorrhagic shock.
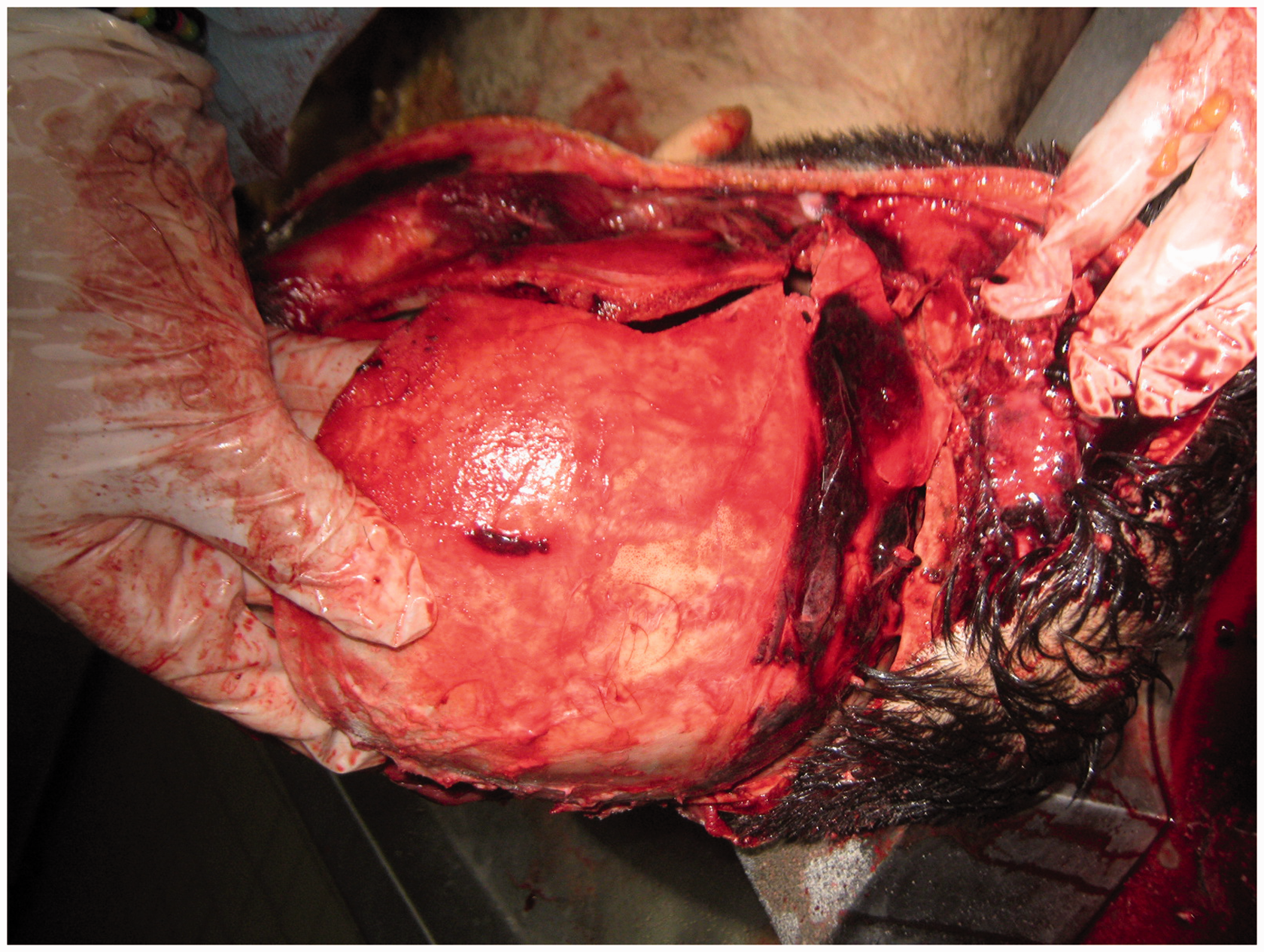
The skull wound (Figure 1) was an irregular laceration, with fractured bones palpable on examination (Figure 2).
Laceration and deep skull wound over the external occipital protuberance. Multiple, irregular and depressed fractures of skull bones, including occipital and temporal bones and reaching the posterior cranial fossa.
The traumatic event raised no doubts with regard to its criminal background, although the wound apparently was not compatible with a gunshot and was considered to be the result of an altercation. However, the crime scene examination showed several signs of bullets hitting the walls of the kitchen where the event took place (Figure 3).
Several bullet marks (A, B, C and D) on the walls and objects of the crime scene were seen. Further explanations for the investigator pointing with a pen on the wall (below point D) are given in Figure 4.
Thus, the bullet marks on the entrance door of the room (point A), then ricocheting over a wooden object (B), ceiling (C) and lateral wall (D), suggested that this was beyond all reasonable doubts due to gun fire; but most impressively, the criminal investigator was able to document the presence of torn human skin and hair on the lateral wall of the room (pointing pen; details in Figure 4).
Hair and skin torn out and impacted on the lateral wall of the crime scene, suggesting that the wound was caused from a gunshot, rather than from a blunt object hitting the head of the victim, as initially misinterpreted.
The suspicion that someone had fired a gun from outside the room, with the victim being shot at the entrance, was raised. Seemingly, the gunshot reached the back of the victim’s head, deeply lacerating the skin and other tissues, and fractured the skull bones (as documented in the Figures 1 and 2), causing the death of the victim. Torn portions of the skin and hairs followed the projectile trajectory and were embedded over the lateral wall of the room (Figure 4).
Law enforcement agents controlled the area the same evening the victim died in hospital, and indeed uncovered three bullet cases (positions 2, 3 and 4), but none of the bullets themselves. The assault gun, supposedly an Albanian-produced carbine SKS-45 (originally a Russian model), was never found; the number 1 in the reconstruction image pertains to the alleged position from where shooting took place (Figure 5). A, B, C and D in the same figure are the points of ricocheting of the lethal projectile, with the victim erect and facing the entrance door (number 5 of the reconstruction figure).
Crime scene reconstruction (see text for explanations).
Discussion
Atypical GIs are a challenge to forensic experts and medico-legal specialists dealing with such criminal events. The investigation of firearm injuries has been a recurrent theme in the specialized literature. 9 Exhaustive and detailed discussions are available as well, with Di Maio offering an overview of the technical aspects. 10
Craniocerebral GIs have a high potential to kill, even when treated aggressively in advanced neurosurgical facilities. The projectile will transmit the kinetic energy to the skull, fragmenting and fracturing bones, severing the brain parenchyma, and generating secondary missiles that will damage brain structures further. 11 Some authors suggest an interesting clinically oriented algorithm of treatment options, based mainly on the Glasgow coma scale score. 11
For a bullet to cause an atypical entrance wound, it must undergo destabilization prior to entering the body. In these circumstances, the bullet will encounter an important yaw process, which is otherwise negligible in typical entrance wounds caused by bullets travelling in a straight course. 12 In our case, we describe an atypical deadly skull wound, very probably due to the ricocheting of one of the bullets shot by the perpetrator. Presenting neither an entrance nor an exit point, the wound itself was initially interpreted erroneously as not being a gunshot wound. Large yawing angles or even tumbling in flight of the bullet will nevertheless produce wounds of strange appearance, clearly indicating a destabilized bullet. 13 A rational and recorded approach to crime scene investigation, as clearly advised, will reveal important detailed information helpful to the police and prosecution, dealing routinely with this type of criminal case. 14
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.