
Abstract
The most common cause of sudden death during sexual intercourse in adults is heart disease, and it is usually the male, whereas the death of the woman is unusual. Generally, in these cases, death occurs as a result of cardiovascular disease. The authors report an unusual case of the sudden death of a young woman during sexual intercourse. The post-mortem investigations (autopsy, cardiac nuclear magnetic resonance and cardiac histology) demonstrated a previously undiagnosed arrhythmogenic right ventricular cardiomyopathy. The terminal cause of death was a malignant arrhythmia from arrhythmogenic right ventricular cardiomyopathy. This is the first report of a case in which sexual activity can be regarded as the triggering factor combined with cardiac disease to the woman’s death.
Keywords
Introduction
Sudden cardiac death is frequently observed in forensic practice, and it is often related to coronary atherosclerotic disease, followed by cardiomyopathies, myocarditis, valvular disease, vasculitis and channelopathies.1–3
Death during sexual activity is uncommon and can occur due to natural or traumatic causes.
If death results from traumatic causes, it is linked to extreme sexual practices used to increase the pleasure of the sexual experience. Sexual asphyxia is one of the most frequent causes of death reported in the literature with asphyxia the result of choking or strangulation.4–6
Few cases of sudden death during sexual intercourse are reported in the literature. The most common cause of sudden natural death in adults is heart disease, followed by malignancies and cerebrovascular events. 7 Sudden death following sexual activity due to exacerbation of previous cardiovascular disease has been studied by several authors. Most researchers demonstrated that in a person with coronary artery disease, the physical effort during sexual intercourse, other added factors, such as psychological stress (i.e. extramarital intercourse) and extraordinary climatic conditions may predispose, or lead to, sudden death.8,9 Moreover, all studies show that the fatal events mainly involve the man.10–13 Sudden death during sexual activity is very rare in women and can occur as a result of hypertensive chronic cardiovascular disease, aortic coarctation, atrioventricular node tumour, fibromuscular dysplasia of the atrioventricular node artery, air embolism or subarachnoid haemorrhage.14–17
In this study, the authors report (1) a case of a young and apparently healthy woman who suddenly died during intercourse and (2) an analysis of the cause of death.
Case report
The body of a 25-year-old married woman was found on her bed in her home. Her husband, a drug addict, reported that the death occurred during sexual intercourse. He had removed the body from the original place of death and had dressed the woman. The Judiciary ordered an autopsy on suspicion of murder.
Autopsy findings
The external examination revealed a marked conjunctival haemorrhage and dark-liquid stains, probably of gastroenteric origin. There was no sign of traumatic injury, particularly to the mouth and neck. The weight of the heart was 370 g with a transverse diameter of 13 cm and a longitudinal diameter of 11 cm; the heart was taken for further study after formalin fixation.
We also collected samples of tissues and fluids and the heart for further instrumental, histological and toxicological examinations.
Cardiac nuclear magnetic resonance study findings
Nuclear magnetic resonance (NMR) was performed using a 1.5-T scanner (GE Excite HDxt, Milwaukee, WI) with an eight-element (four anterior and posterior) phased-array receiver surface coil. The images were obtained by acquiring long- and short-axis black-blood spin echo Transmission system 1 (T1)-weighted sequences with and without fat saturation. The following parameters were used: thickness 3 mm, no gap, matrix 512 × 512 and field of view 28 cm. Post-mortem NMR images (Figure 1) of the heart showed marked thickening of the right ventricular myocardial free wall (hyper intense), with drop of the signal intensity in fat saturation T1w images, due to fibro-fatty replacement.
Long- (a, c) and short-axis (b, d) black-blood spin echo T1-weighted images. Images show marked thickening of the right ventricular myocardial free wall (hyperintense), with drop of the signal intensity in fat saturation T1w images (c, d), due to fibro-fatty replacement.
Toxicological findings
Toxicological tests were performed on the samples of cardiac blood and urine. Drug screening analysis was performed using gas chromatography/mass spectrometry. All specimens tested negative for alcohol and drugs (illegal and psychotropic).
Heart and histological findings
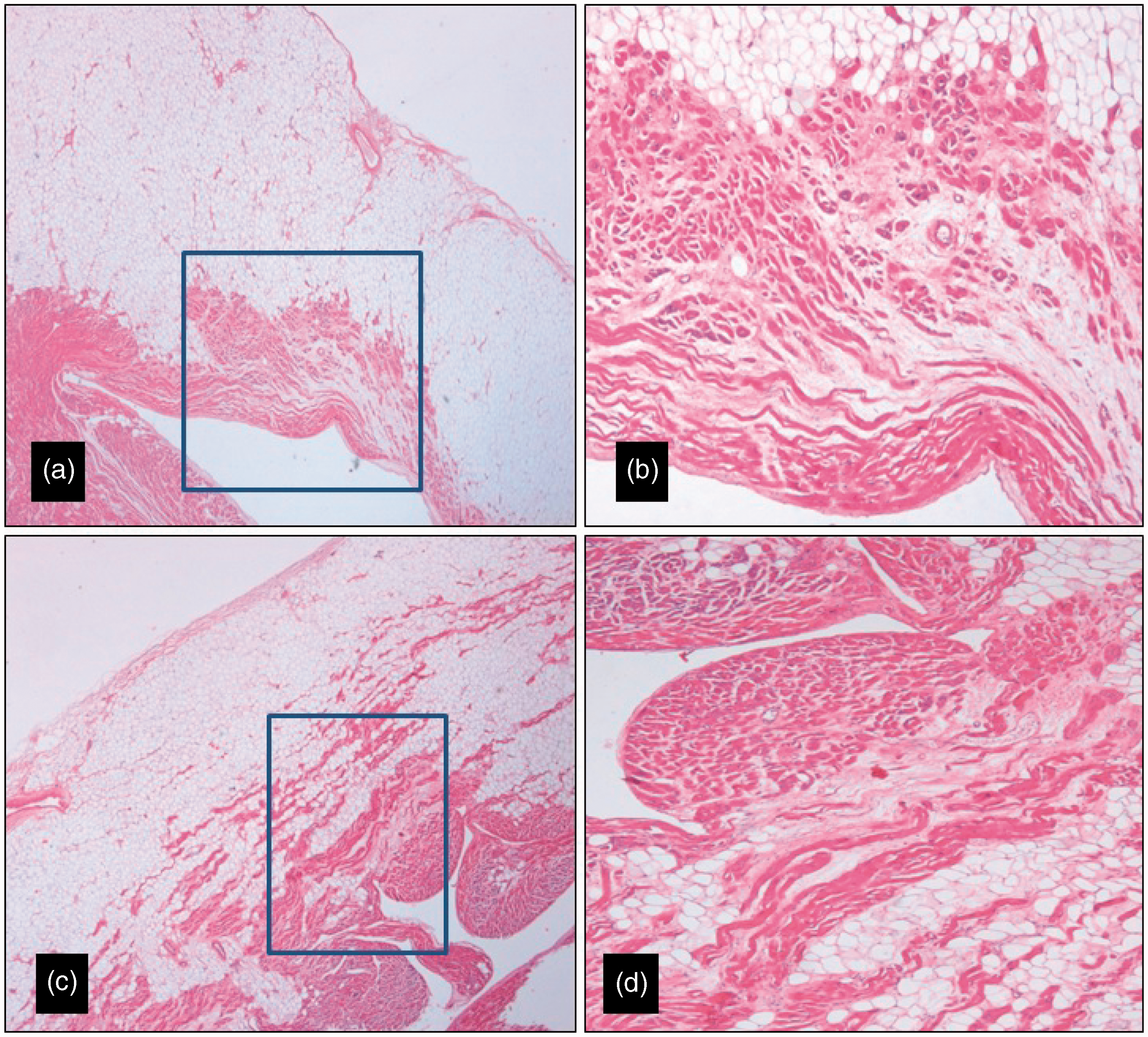
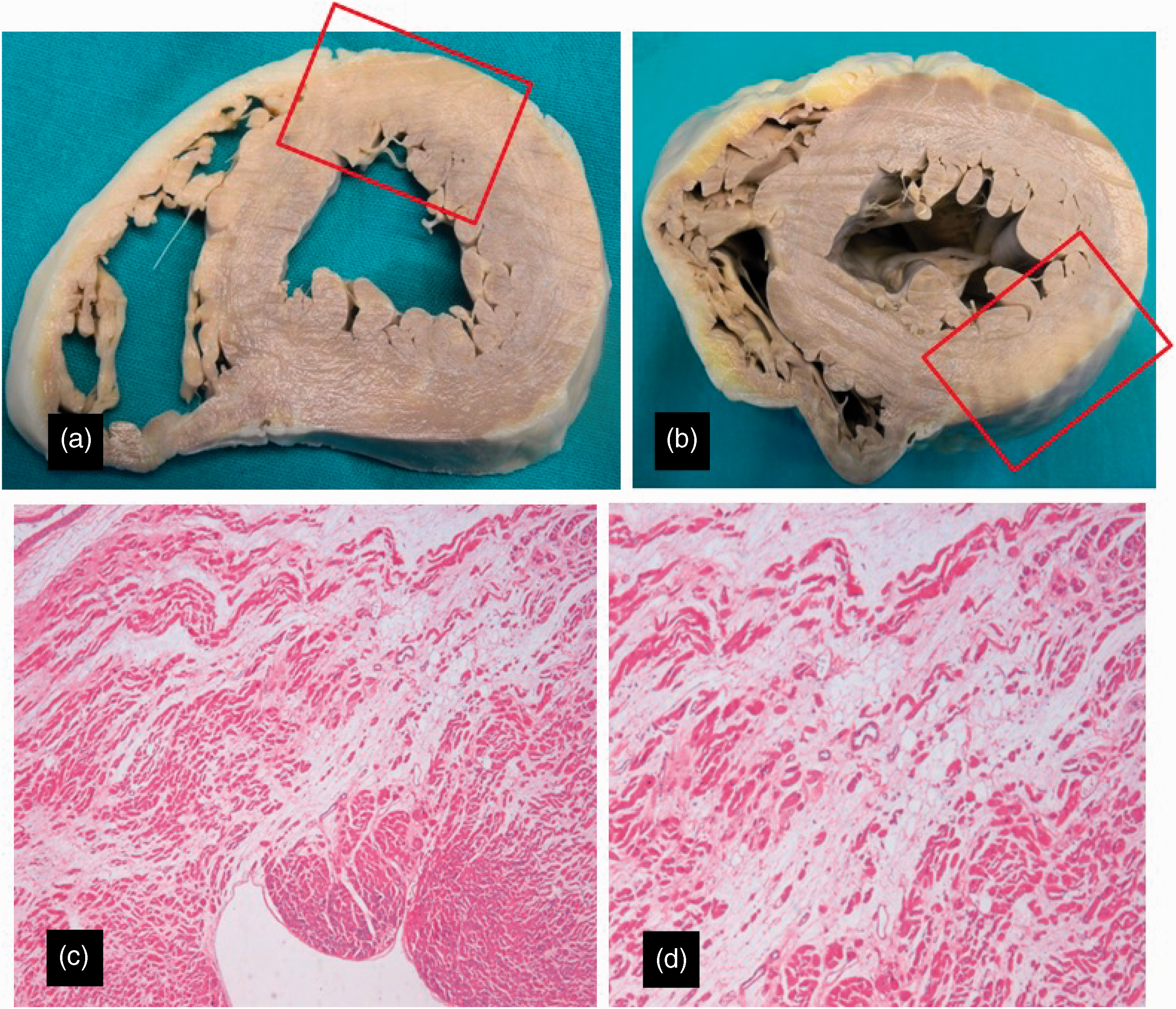
The heart examination showed ventricular walls thickness of 5 mm to the right and 12 mm to the left. The macroscopic and histological study of the right ventricular wall showed fibro-adipose infiltration of the myocardial “compacta” (Figure 2) with clear microscopic signs of transmural fibro-fatty progression (Figure 3). The macroscopic and histological study of the left ventricular wall showed areas of fibro-adipose infiltration in the anterior and posterior wall, without myocardial active healing (Figure 4). Therefore, there were sub-endocardial contracture bands in both ventricles and the small intramural coronary vessels exhibited fibromuscular dysplasia. The lungs showed acute pulmonary oedema, part of a haemorrhagic nature.
Macroscopic findings of the right ventricle. (a) Thick fatty infiltration involves the transmural compacta of the anterior right ventricular wall. (b) Widespread fatty infiltration of the free right ventricular wall that appears transparent to transillumination. Histological findings of the right ventricle. (a) and (b) Transmural fibro-fatty infiltration involves the anterior right ventricular wall. Haematoxylin and eosin stain. 2×. Macroscopic and histological findings of the left ventricle. Fibro-adipose infiltration is evident in the anterior (a) and (c) and posterior (b) and (d) left ventricular wall. Haematoxylin and eosin stain. 2×.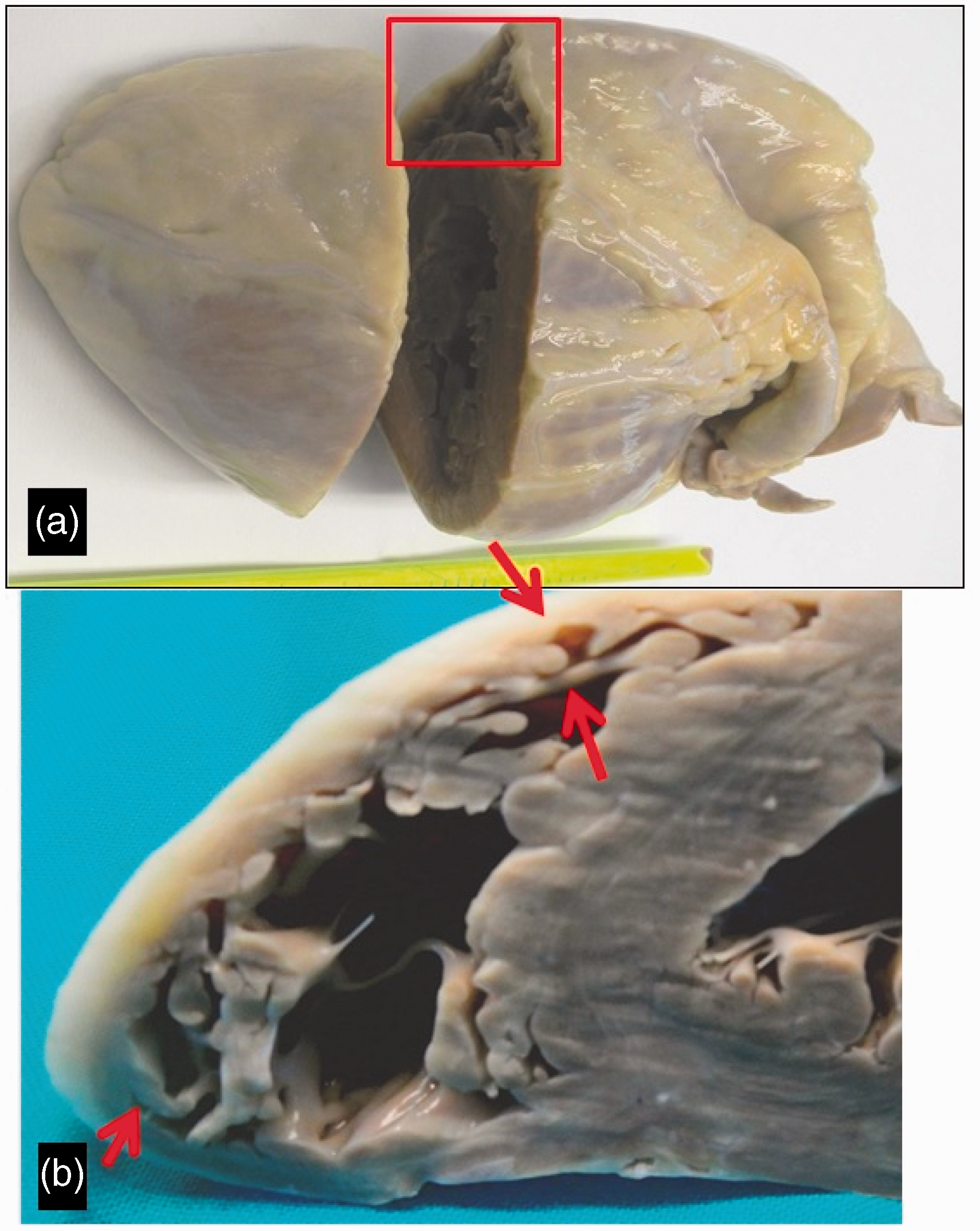
Discussion
In this reported case, the macroscopic and histological cardiac findings demonstrated a previously undiagnosed arrhythmogenic right ventricular cardiomyopathy (ARVC). ARVC is a particular kind of cardiomyopathy which is responsible for sudden death in young individuals and adults, with an annual incidence of sudden death estimated to be ≈2% that occurs, presumably, on the basis of a ventricular arrhythmia. 18 The most typical microscopic findings of ARVC are represented by two patterns, fatty and fibro-fatty myocardial infiltration. In the fibro-fatty variety, myocardial atrophy appears to be the consequence of myocyte death and repair by fibro-fatty replacement, mediated by patchy myocarditis. The left ventricle and ventricular septum can be involved in 50% to 67% of cases, often later in the disease, confirming poor prognosis. 19
In ARVC, the principal triggering factor for sudden death is exercise that can precipitate ventricular tachycardia. Many studies show the correlation between ARVC, exercise and sudden death. Indeed, athletes with ARVC were six times more likely to die on exertion compared to those with other cardiac pathologies. 20
Despite various studies about this correlation, literature has no reported cases of sudden cardiac death following ARVC during sexual intercourse. The case we present is the only one in which the cause of death was determined as acute heart failure due to malignant arrhythmias occurring during sexual intercourse in a young woman suffering from unknown arrhythmogenic right ventricular cardiomyopathy.
The physical activity of sexual intercourse was studied and many authors demonstrated that it is associated with increased myocardial oxygen demand and increased sympathetic nervous system activation.21,22 A study conducted to directly measure sympathetic neural drive during sexual activity shows that sexual activity in healthy adult male and female rabbits is associated with profound transient increase in sympathetic drive to the kidneys and particularly rapid dynamic changes in heart rate and arterial pressure. 23
Paton et al. 24 proposed that during sexual activity, there is a coactivation of cardiac sympathetic and parasympathetic systems that has the potential to be pro-arrhythmic, particularly where myocardial function is impaired. 25
Even if these studies were aimed to highlight the impact of sexual activity on the heart with coronary disease, the demonstration of sympathetic system activation and its potential pro-arrhythmic role could explain why in the presented case the ARVC took the form of sudden death during intercourse.
In conclusion, this is the first reported case of a woman suffering sudden cardiac death during sexual intercourse due to ARVC. The terminal cause of death was a malignant arrhythmia from ARVC in which the sexual activity can be considered the triggering factor contributing with cardiac disease to the woman’s death.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.