
Abstract
Post-mortem multi-slice computed tomography (MSCT) is a new approach in forensic pathology for gunshot injuries. This study determines the role of MSCT in the characterisation of single gunshot injuries. We report three cases. In the first case, an 80-year-old man was found dead in his bedroom with a gun. External examination showed devastating head injuries. In the second case, an 81-year-old man was found dead in his apartment, without a gun. External examination showed gunshot injuries. In the third case, a 56-year-old man was found dead on a road. MSCT and autopsy were performed in all these cases. MSCT not only allowed the determination of entrance and exit wounds but also showed some artefacts. In conclusion, radiology is fundamental for the reconstruction of gunshot injuries, and the manner of death can only be ascertained by autopsy.
Introduction
Recently, forensic pathology has benefited from new imaging technologies. In 1970, the College of American Pathologists noted the importance of radiological investigation in some cases of forensic interest by introducing ultrasound-guided anatomical sampling. 1 In 1984, Di Maio pointed to the necessity of using radiology in firearm-related deaths to find and identify bullets accurately. 2 Over time, there has been a shift from simple evaluation by conventional radiology techniques, ‘radiopsy’, to using heavy machinery, such as computed tomography (CT) and magnetic resonance imaging (MRI), that allows the analysis of the whole body, thereby determining a real virtual autopsy or ‘virtopsy’. Imaging techniques can provide data and may give more accurate answers in forensic investigation, and the need for radiological investigation is coupled with the fewer autopsies that are performed, essentially due to religious or socio-cultural reasons. 3 Virtopsy consists in the documentation and analysis of a body volume using multi-slice computer tomography (MSCT) and/or MRI, with three-dimensional (3D) reconstructions of surface, and processing of data by a Workstation. The choice of MSCT or MRI depends on the particular circumstances and whether they can provide answers to specific questions (for example, CTMS is extremely useful in identifying the presence of gas or metallic foreign bodies, while MRI is more appropriate for the study of soft tissues). Although virtopsy can be used for many purposes in the forensic field,4–26 one of its most important applications is the evaluation of gunshot injuries. Thali, father and promoter of the virtopsy project, and many other authors have suggested MSCT to study the lesions, to identify the bullet and to evaluate the bullet’s path.27–30 Bolliger et al., in 2008,10 compared traditional radiological MSCT with MRI and showed how MSCT can visualise the presence of bone lesions, foreign bodies and internal gases in the body. With regard to bone fractures, the authors pointed out the advantage of detecting regions that are not easily analysed with the autopsy. Analysing the disadvantages, MSCT presents a contrast resolution in soft tissues, lower than MRI; therefore, it is not the ideal choice for evaluating lesions of organs and soft tissues. In the case of gunshot injuries, MSCT has limitations: the difficulty in assessing the damage of vessel; the impossibility of a clear interpretation of images related to the multiple firearm injuries, especially in a case where the various trajectories tend to intersect; and the presence of artefacts data from the fragments of metallic residues of the shot. Some studies have considered the applicability of CTMS using experimental models such as blocks of soap31 or ballistic gelatine. 32 The contribution of CT in the evaluation of gunshot victims is crucial. However, it is important to recognise CT’s limitations along with its advantages.
Cases
To evaluate MSCT in the examination of gunshot victims, we present three cases of death from gunshot injuries. Cases 1 and 2 are suicides, and the third case was a homicide. In each case, crime scene investigations, ballistic examinations and external and internal examinations were performed. The tissue samples were stained with haematoxylin and eosin. Triangulations of the gunshot wounds and toxicological investigations were carried out. Before autopsy, each body underwent a total body MSCT with a 64-slice CTMS (Aquilion CX 64, Toshiba Medical System, Tokyo, Japan) supplemented with 3D reconstructions of the affected areas as well as the entire skeletal system.
Case 1
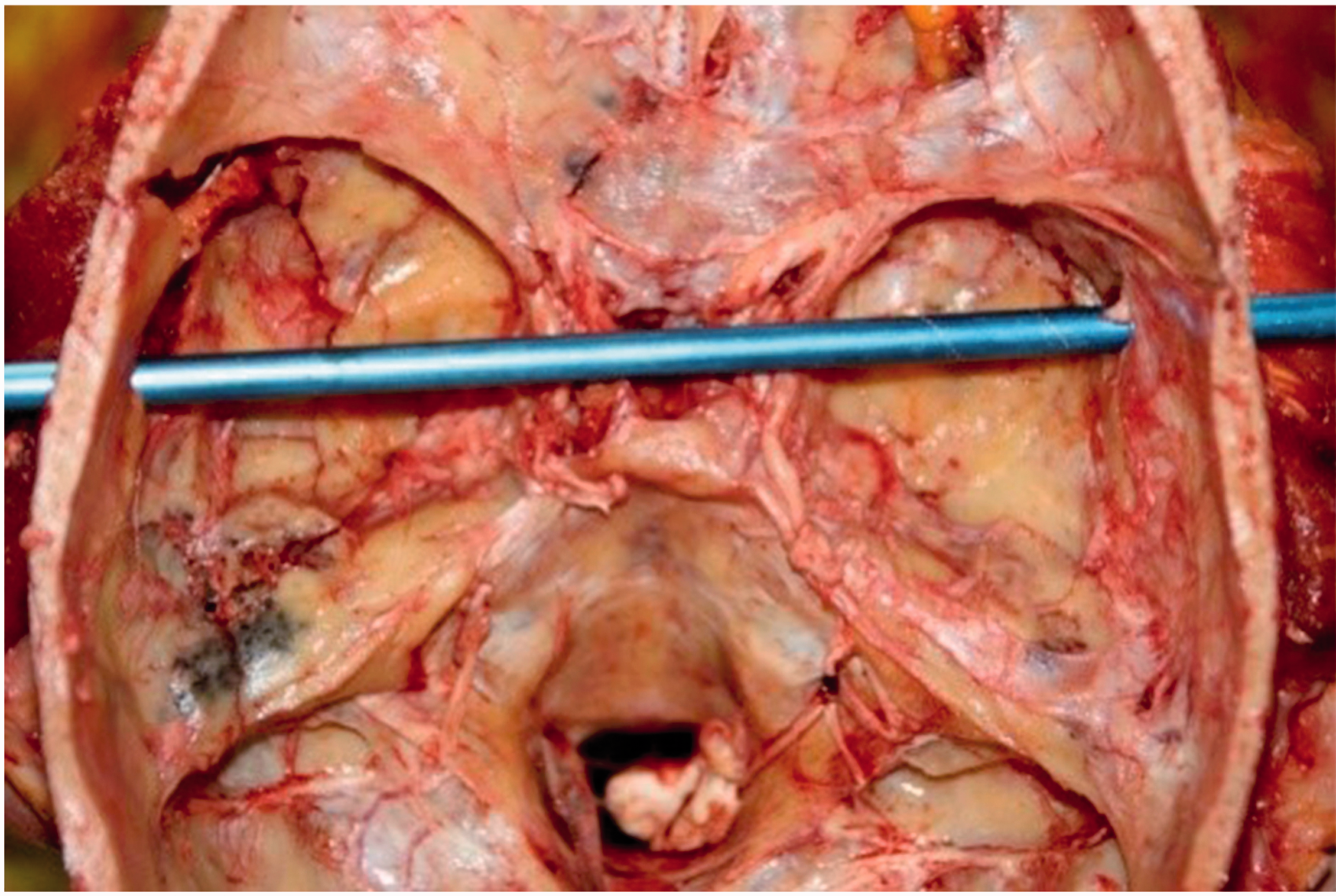
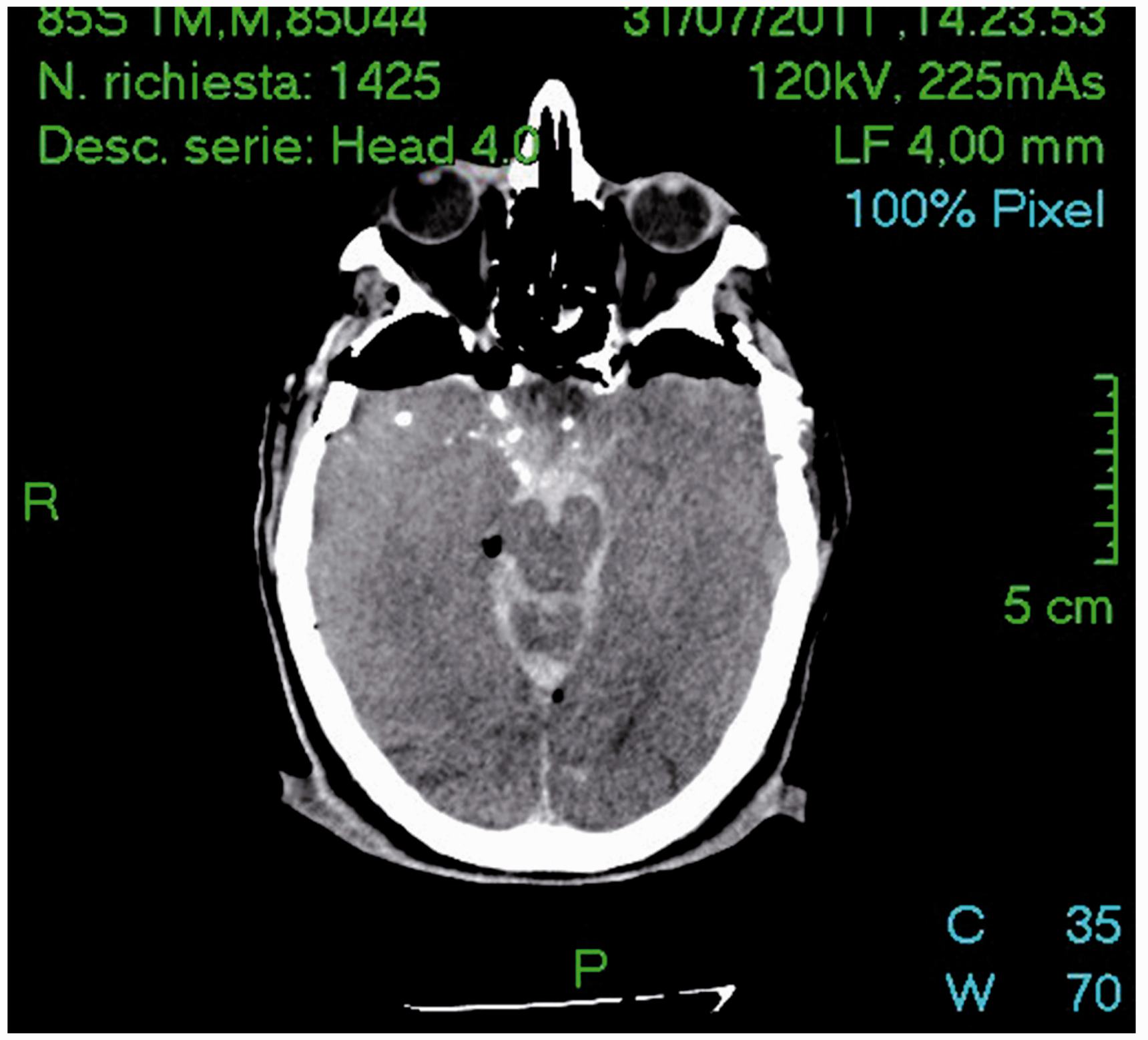
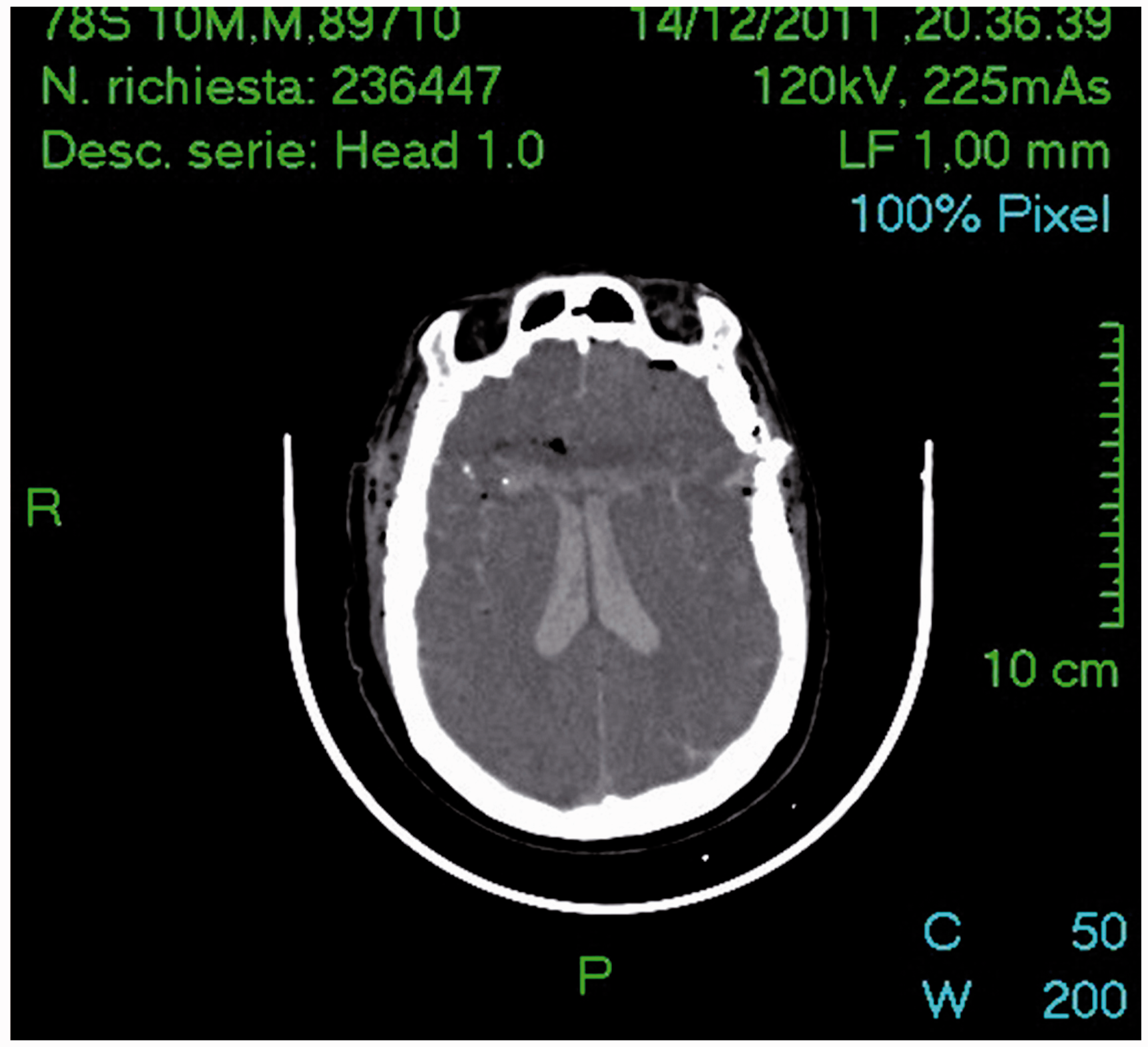
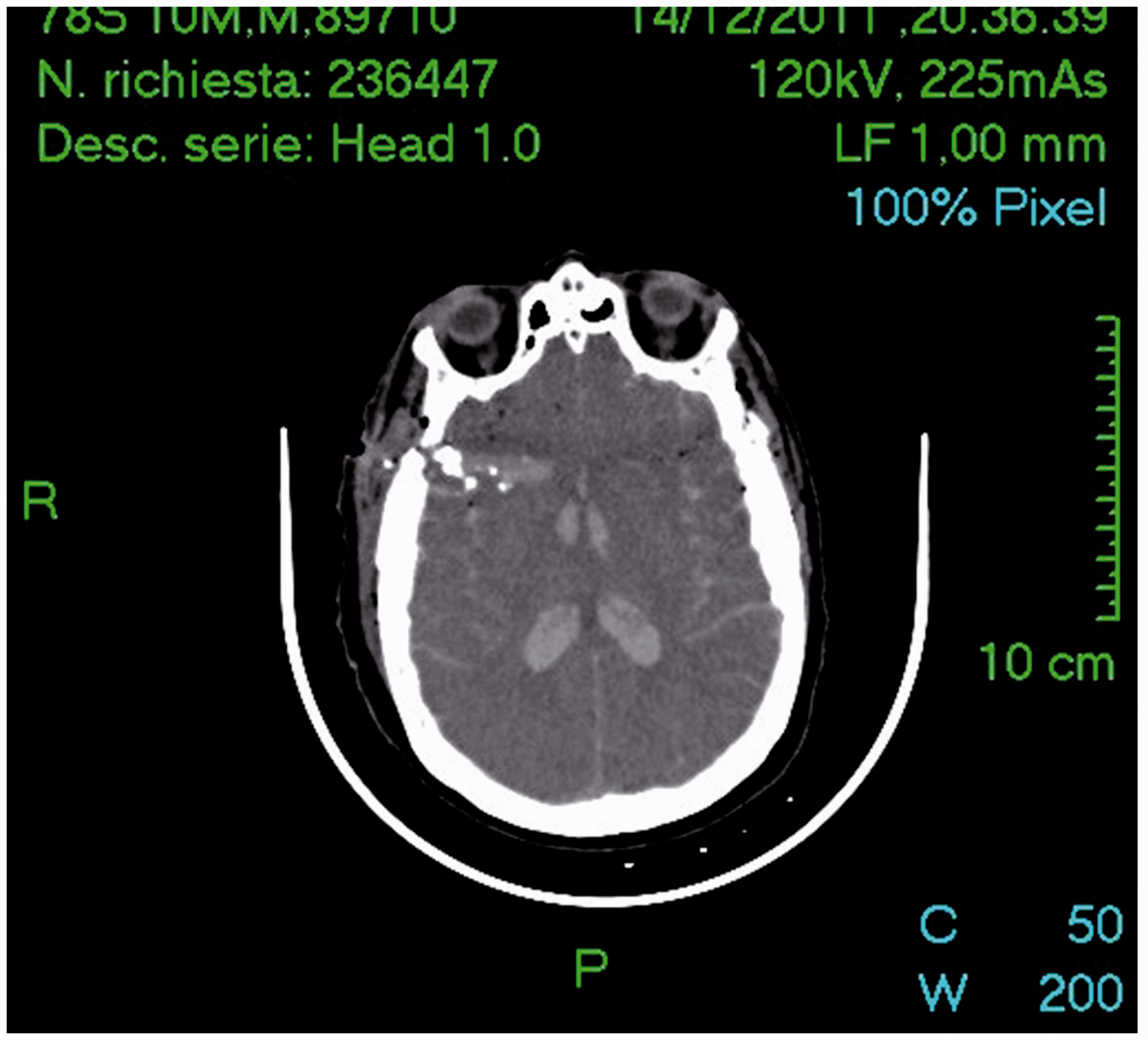
An 80-year-old man was found supine on his bed at home. The man had a gun in his right hand; a Lebel revolver of 8 mm calibre, FMJ ammunition. On external examination, a gunshot wound in the right temporal region with the characteristics of an inlet port (called FAF 1) was noted. Another gunshot wound was pointed at the left temporo-parietal region with the characteristics of an exit hole (called FAF 2). At autopsy, FAF 1 presented as a perforation of irregular shape with ecchymotic-excoriated contours. FAF 2 appeared as a star-shaped injury with jagged edges and no bruising. There was a fracture of the right orbit roof; bilateral fracture of the middle cranial fossa (Figures 1 and 2) was more evident to the left side; and presence of cerebral and cerebellar haemorrhage was also noted. There was a traumatic break up of left and right temporal and parietal hemispheres. Within the brain parenchyma, a pathway from bottom to top, from right to left, in an oblique direction with respect to the entrance hole was noted. CT, performed before the autopsy, showed the presence of a hole of cortical discontinuity at the right temporal and orbital area and discontinuity with jagged edges and bone fragments in the subcutaneous region of the left high temporal and orbital areas as, respectively, entry and exit hole of the gunshot wound (Figures 3 and 4). In addition, cerebral haemorrhage did not allow a good evaluation of the residual parenchyma, only examinable in the occipital and cerebellar lobes, and intra-parenchymal cerebral haemorrhage diffuse small gaseous areas.
Case 1. FAF 1, FAF 2 and the trajectory followed by bullet. Case 1. The trajectory at the opening of the skull. Case 1. MSCT imaging: entry and exit hole of the gunshot wound. Case 1. MSCT imaging: Bone fragments in the subcutaneous region of right temporal and orbital areas as exit hole.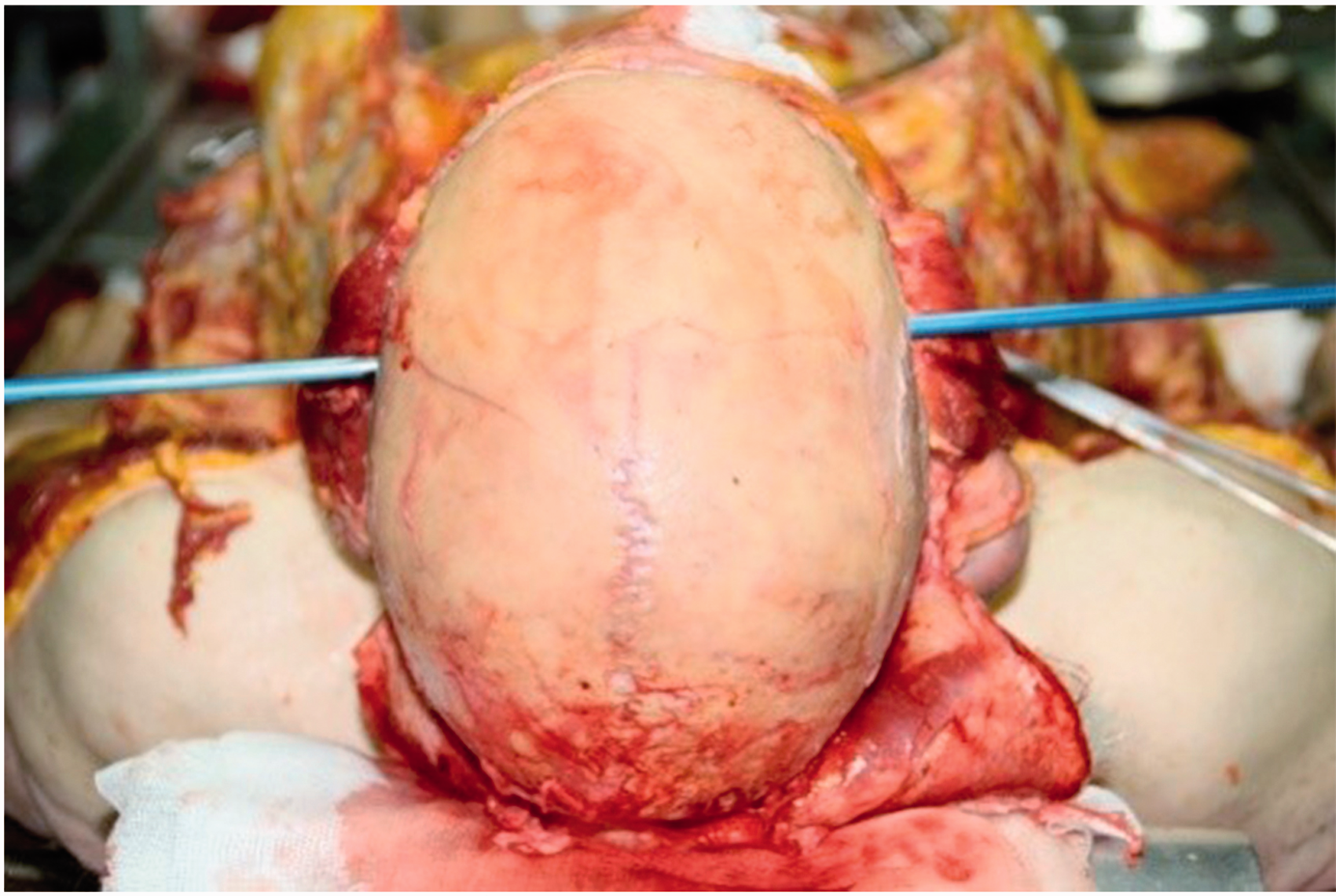

Case 2
An 81-year-old man was found lying on his back on his bed in his home. His weapon had been removed by the police who arrived before the coroner. The tested weapon was an Astra of 7.65 mm calibre. External examination recorded a gunshot wound in the right temporal region with the features of an entry hole (FAF 1) and another wound opposite on the left temporo-parietal region with the characteristics of an exit hole (FAF 2). At autopsy, FAF 1 presented with ecchymotic-excoriated contours and tattoo. FAF 2 was a hole with concentrically light red ecchymotic halo with jagged edges. When reconstructing the intra-corporeal path of the bullet, it was shown to have passed through the frontal and temporal region, reaching the left frontal, temporal and parietal regions (Figure 5). The direction of this pathway confirmed that it went from right to left and from bottom to top, in an oblique direction to the medial axis. Internal examination revealed intra-cerebral and cerebellar haemorrhage. Post-mortem CT was executed before the autopsy, which revealed a hole of cortical discontinuity and small bone fragments adjacent and within the brain, in correspondence with the temporal and orbital right areas, and another hole with the same characteristics but with jagged edges in the temporal and frontal area, with small bone fragments in the subcutaneous left region; these signs were due to the entry wound on the right and to the exit wound on the left. A hyper-dense streak is visualised in the brain associated with temporal and frontal air bubbles, as a representation of the path from left to right made by the bullet. In the left frontal region of the brain, adjacent to the exit hole, it was evaluated as a sagittal hyper-dense stripe, as for blood collection (Figures 6 and 7).
Case 2. Trajectory followed by bullet. Case 2. MSCT imaging: exit hole in left temporal region of the gunshot wound and path followed by bullet. Case 2. MSCT imaging: Bone fragments in the subcutaneous region of right temporal and orbital areas as entry hole.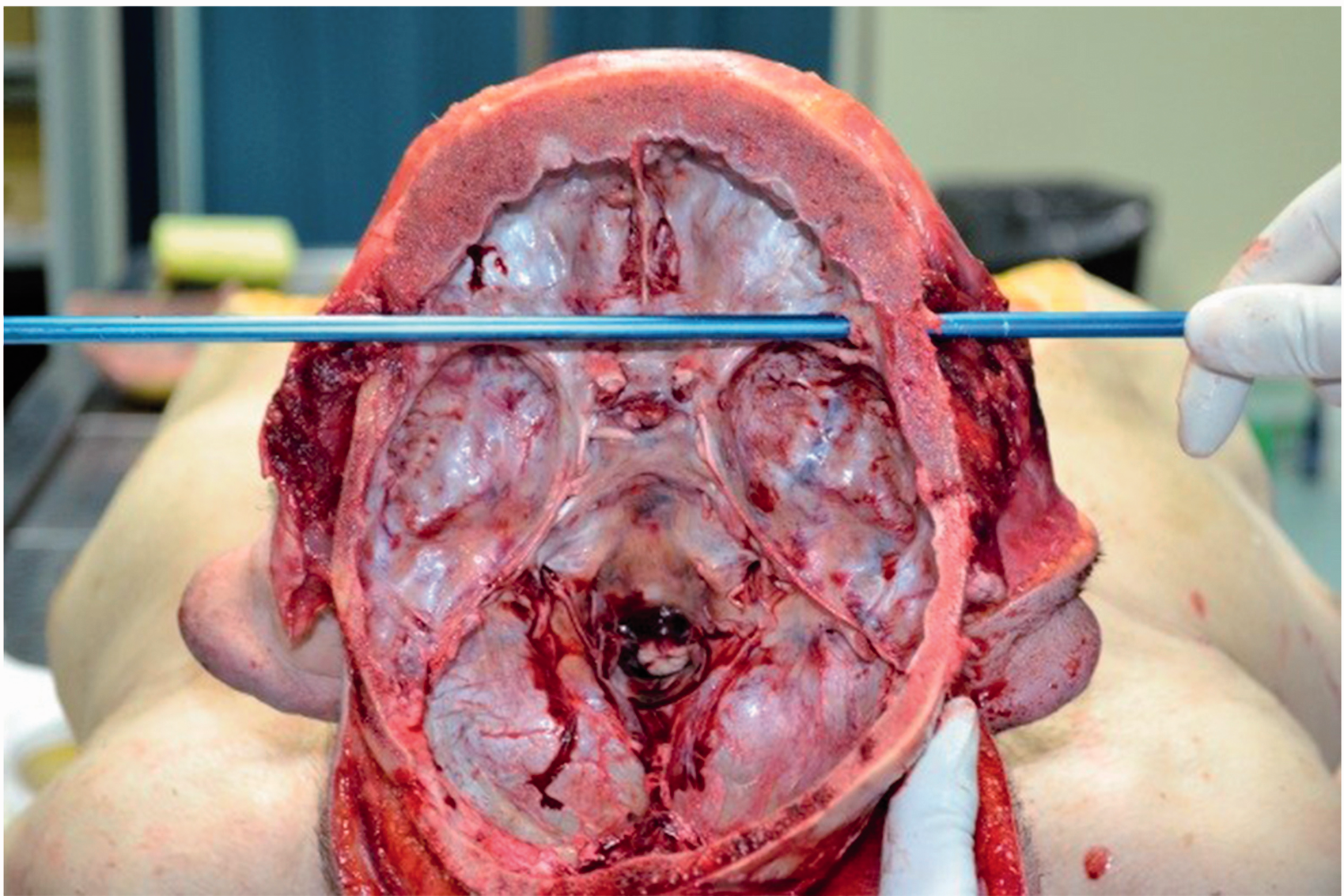
Case 3
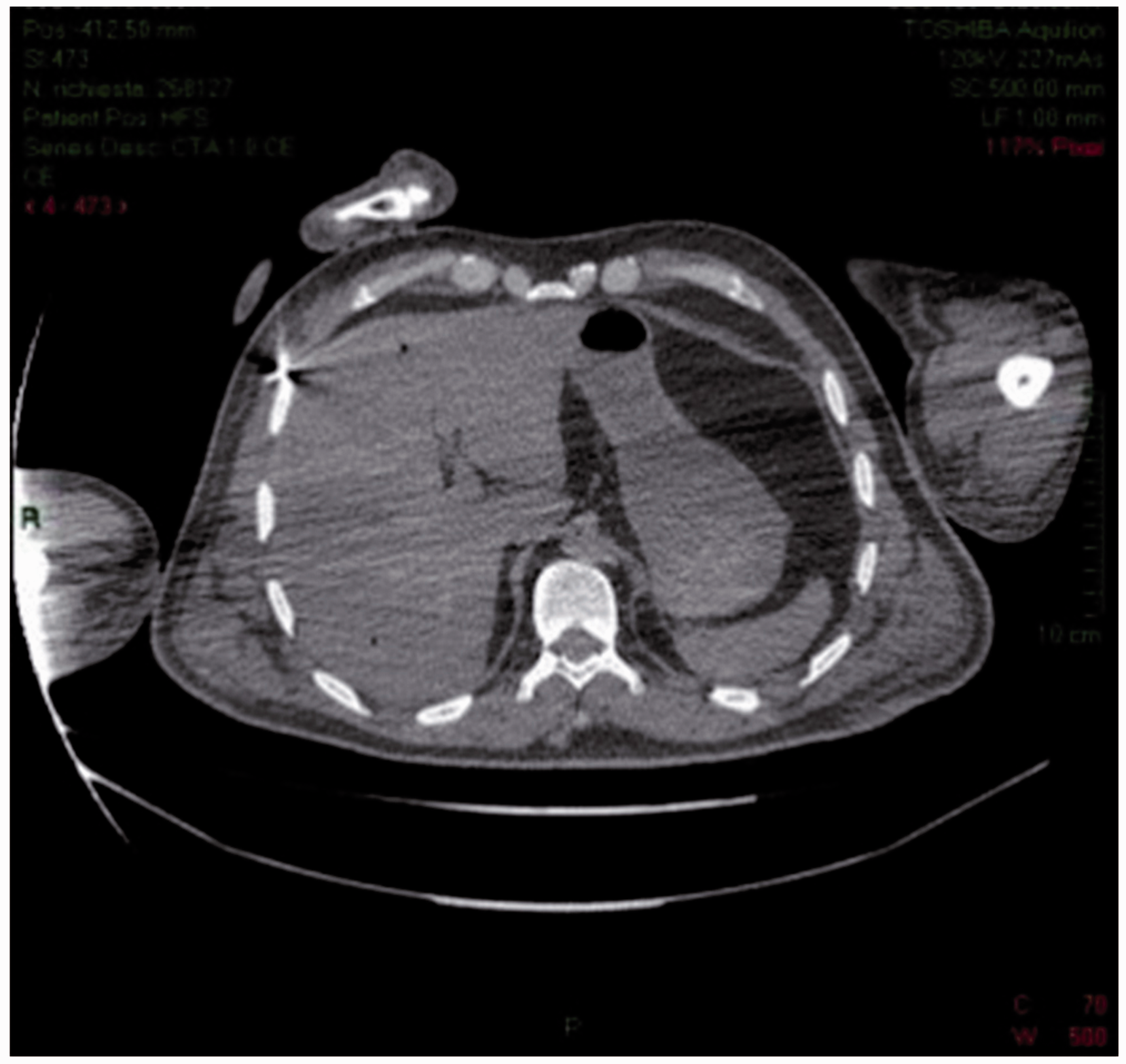
A 59-year-old man died in hospital after a craniotomy to remove a bullet in the brain. It was a homicide. The weapon was of 9 mm calibre. Autopsy revealed a wound in the right parietal region, which had been sutured due to the neurosurgical intervention (FAF 1). Two thoracic wounds penetrated from it up to subcutaneous and muscular areas, in the intercostal muscles, not piercing the right chest cavity (FAF 2 and FAF 3). FAF 2 showed entry wound characteristics with irregular ecchymotic excoriated contour; FAF 3 shows entry hole characteristics with bruised and irregularly oval ecchymotic contours. Such wounds accord with shooting by two individual gunshots, neither of which exited. It was important to find the two bullets. Opposite to the right supra-diaphragmatic muscle was an intramuscular ecchymotic area, on the level with the projectile’s impact; it was also shown in correspondence to the right haemithorax inner face, between the sixth and seventh rib and between the fourth and fifth rib, with a fracture of left lateral arch of the fourth rib. Internal examination revealed the presence of a bullet between eighth and ninth rib (Figure 8). Around the sixth rib, another bullet was detected, and there was a breakage of left orbit roof and a large intra-cerebral haemorrhage. On the basis of the CT report, we searched for the bullet in the brain but we did not find it; we later learned that the bullet had been removed by medical staff during craniotomy. MSCT, performed before the autopsy, showed the lack of bone in the left parietal region, with evidence of haematoma absorption in the same region. There were signs of a foreign body, such as a bullet, at the falx cerebri and a small hole in the contra-lateral parietal region with small bone fragments. Post-mortem imaging showed a foreign body, a bullet, at the right upper quadrant of the abdomen and another one between right hypochondrium and right hip (Figures 9 to 10).
Case 3. Bullet found in the torax. Case 3. MSCT imaging: presence of a foreign body, as bullet, at the right upper quadrant of the abdomen. Case 3: MSCT imaging: presence of another bullet between right hypochondrium and right hip.

Results and discussion
These aforementioned cases show the benefits and limitations of imaging techniques in forensic examinations. The benefits include the ability to preserve the morphological data forever thereby allowing the revisiting and reworking of the images and also the performance of measurements and evaluations not conducted in a first phase, with the opportunity of a 3D reconstruction of the body (by means of volume rendering tools). 33 Other important potentials are the elimination of biological risk for the personnel involved in medico-legal autopsy practices 34 ; the possibility of creating digital documentation in which the data can be transmitted at a distance, allowing for easy comparison between experts 35 ; the ability to run multiple virtual autopsies on the same subject without colliding with a previous dissection 1 ; less opposition to the investigation and autopsy by family members of some religions (Orthodox Judaism, Islam and others) 1 ; the acquisition of images with scan times rather short 27 ; and the chance to focus any traditional autopsy on the most significant findings, further reducing the time of investigation. 4 Disadvantages include the inability of the CTMS and MRI to detect any colour of post-mortem changes, which can be partially solved by techniques of volume rendering and surface 1 ; the alteration of post-mortem changes on the images produced by the various techniques (putrefactive gases, for example, can be confused with gas of intestinal origin or with the gases present in the context of a wound, creating artefacts that make virtual investigation strictly time-dependent) 1 ; and the difficulty in obtaining histological samples for anatomical-pathological analysis, even if this limitation is exceeded by using CT-guided biopsy techniques. 36 Moreover, we must also consider the higher costs of using these imaging techniques, 37 the fact that many centres do not have the equipment for a virtual autopsy and the logistical problems that some centres struggle with to use such imaging tools 38 (i.e. use of CTMS, MRI, etc. at night 39 ). We emphasise the importance of having qualified personnel (forensic radiologist) with the expertise and experience to carry out a medico-legal assessment of the images offered by virtual autopsy. 39 In gunshot cases, as demonstrated here, the forensic pathologist may have difficulty in reconstructing the dynamics of the shot, to determine the reconstruction of the entry and exit holes and to identify the intra-corporeal pathway.
In cases 1 and 2, there was a single gunshot injury with entry and exit holes and a complete intra-corporeal pathway due to suicide. The major advantage of CT was that the different morphology of the bone contours allowed for the reconstruction of entry and exit holes. This information was combined with the study of the characteristics of the holes at autopsy. CT made it possible to identify a hyper-dense streak, characterised by the passage of the projectile that caused the haemorrhagic infiltration constituting the intra-cerebral pathway. CT examination had its limits compared to autopsy in these cases, as it was impossible to show evidence of infiltration areas of entry hole as well as the typical distribution of blood stains on the skin of the hand that had gripped the weapon during firing. In addition, MSCT examination did not reveal fractures of the skull base and infiltration relative to subcutaneous haematoma, which were found at autopsy. In case 3, CT imaging analysis was more complicated, due to multiple gunshot injuries. The advantage of the CT was that the location of the two bullets in the abdomen is known, which proved useful at autopsy. However, the disadvantage of CT in this case was viewing an artefact, such as an extremely hyper-dense area, compatible with the image of a projectile. This figure was later discovered to be a false positive, presumably determined by the residue of the projectile itself.
From the analyses of these cases, we can infer that CT examination, in the case of death from a firearm, allows the detection of entry and exit holes, the reconstruction of the bullet path, although it does not enable one to determine the manner of death (suicide and murder?). This requires an external examination and a forensic autopsy. In addition, in these cases, MSCT overestimated the extent of intra-cranial bleeding and did not show linear skull fractures, such as those found in case 1 in middle cranial fossa, and the passage of air interferes with the vision of parenchyma or tissue analysed by post-mortem CT, constituting artefacts. The most significant artefact was the image of a bullet, which was not actually present, in case 3. Notwithstanding these limitations, we consider that in cases of death from gunshot wounds, a CTMS examination before autopsy is useful and can assist and direct the pathologist by reducing the time needed to carry out the examination and making it easier for the pathologist to find projectiles and to identify the site of entry and exit holes.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.