
Abstract
Many physicians, particularly neurosurgeons, face malpractice claims during their career. The aim of this paper is to identify which factors increase the risk of litigation and influence legal outcomes relating to cerebrospinal fluid shunt management. Westlaw, an online legal database, was used to identify all medico-legal cases pertaining to cerebrospinal fluid shunts. Information regarding plaintiff demographics, defendant specialties, reasons for litigation, and trial outcomes were analysed. Thirty-six cases met criteria for inclusion. Most cases returned a defence verdict (44.4%), with delayed treatment or failure to appropriately treat patients with shunts the most common reason for litigation (66.7%). The average plaintiff verdict payout was $4,888,136.75 and average settlement $1,362,307.69. Delay or failure to treat resulted in the largest average payouts for plaintiff verdicts and settlements ($5,329,299.14 and $1,531,500.00, respectively).
Introduction
Malpractice litigation is a growing concern among medical professionals. Many physicians can expect to face a lawsuit during their career, but neurosurgeons rank among those most frequently sued with the largest mean payouts for legal cases. 1 Litigation against neurosurgeons is strongly related to the type of case rather than the complexity of the surgical procedure being performed. 2 This has led to an increased interest in analysing malpractice claims related to specific surgical procedures and medical conditions.
Cerebrospinal fluid (CSF) shunts are a common procedure, most frequently used in treating hydrocephalus to reduce the abnormal accumulation of fluid within the ventricular system of the brain. In the United States, it has been estimated that around 30,000 shunt procedures occur annually, with reports that over 20% of patients experience complications within the first year.3,4 Despite the prevalence of CSF shunts, however, litigation analysis of this procedure has not been reported. Our aim is to identify demographic characteristics, reasons for malpractice proceedings, and trial outcomes for such cases to identify ways of mitigating litigation and increase physicians’ awareness of the factors that may contribute to unfavourable legal outcomes.
Methods
We used the online legal database Westlaw Edge (Thomas Reuters) to conduct a systematic review of cases focused on the management of CSF shunts. This publicly available database provides users with access to attorney-verified medico-legal claims made in the United States. Since Westlaw does not contain any protected patient information, institutional review board approval was not required.
Search criteria focused on cases related to malpractice and treatment of patients with CSF shunts. Specific search terms included “malpractice”, “ventriculoperitoneal shunt”, “ventriculopleural shunt”, “VP shunt”, “ventriculoatrial shunt”, “lumboperitoneal shunt”, “lumbar shunt”, “brain shunt”, “intraventricular shunt”, “ventricular shunt”, and “intracranial shunt”. Each case was analysed to ensure that inclusion criteria were met. Duplicate cases or those unrelated to CSF shunts were excluded from further analysis.
The main outcomes recorded included demographic information of the plaintiffs, geographic location of trials, type of court, cause for litigation, and specialties of defendants. Trial outcomes and payouts for verdicts and settlements were also documented.
For our statistical analysis, means and standard deviations were used to summarise continuous variables. Comparative analysis of cases in favour of defendants versus plaintiffs was done using a t-test (parametric) or Wilcoxon rank-sum test (non-parametric). Frequencies and proportions were used to summarise categorical variables and compared using chi-square or Fisher exact tests. Significance was defined as p-value <0.05. All analyses were performed using SPSS Statistics Version 29.0.0.0 (IBM Corp., Armonk, NY, USA).
Results
Demographic information of plaintiffs
Seventy-six cases between 1990–2022 linked to CSF shunts were identified from our initial search, 36 of which met inclusion criteria. The remaining 40 cases were excluded due to duplicate files, insufficient information, or claims unrelated to CSF shunt management. From those included cases, 18 (51.4%) were female, 17 (48.6%) were male, and 1 (2.8%) case did not list the sex of the plaintiff (Table 1). The average age of plaintiffs was 21.0 +/− 15.0 years (range: 1 to 62 years). Eleven patients were younger than 18 years of age. Plaintiff ages were not reported in 16 cases.
Summary of Key Characteristics.

One case had sex unlisted.
Three cases had both jury verdicts and settlements for different defendants.
Two settlement amounts were confidential.
Geographic distribution
Seventeen states were represented in this study. The largest number of cases occurred in California, Florida, New York and Texas (n = 4, 11.1%, respectively) (Table 1). The next most frequently represented states were Illinois and Ohio (n = 3, 8.3%).
Specialties of defendants
Out of the 36 cases included the most frequently listed defendant was a hospital, medical centre or healthcare system (n = 23, 63.9%) (Table 1). The next most cited medical specialty was neurosurgery (n = 13, 36.1%), followed by emergency medicine (n = 6, 16.7%). Four cases had unnamed defendant specialties.
Types of shunts
Ventricular shunts were the most frequent type specified in medical malpractice litigation (n = 35, 97.2%). One case involved management of a lumbar shunt (2.8%).
Reasons for malpractice litigation
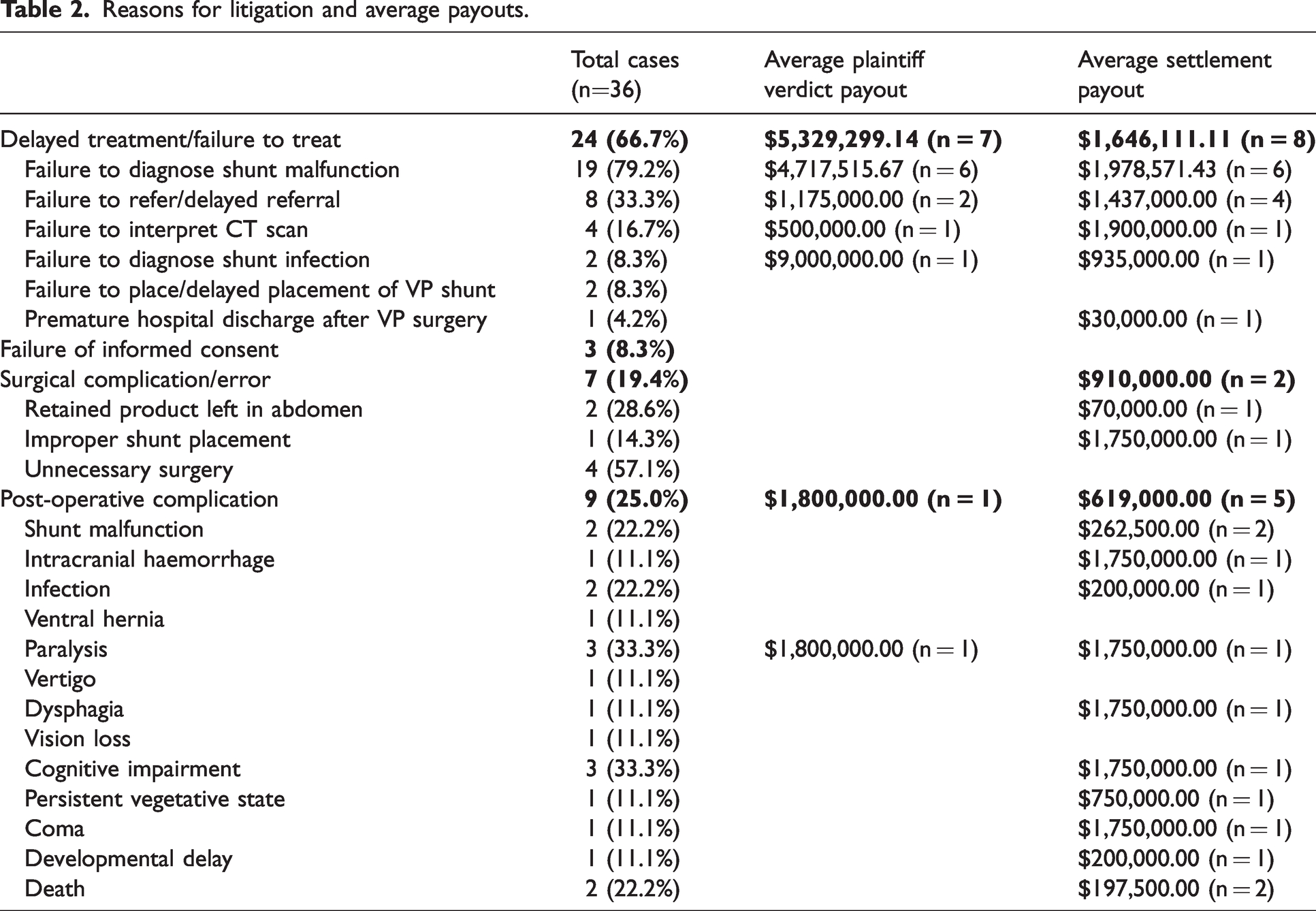
The most common reason for a lawsuit was delay in treatment or failure to treat (n = 24, 66.7%) (Table 2). Due to multiple factors that resulted in a failure to treat plaintiffs, the following subgroups were created: failure to diagnose shunt malfunction, failure to refer or delayed referral, failure to interpret CT scan, failure to diagnose shunt infection, failure to place or delayed placement of VP shunt, and premature hospital discharge after VP shunt surgery. Failure to diagnose shunt malfunction (n = 19, 79.2%) was the most common reason for litigation. The second most cited reason was post-operative complications after VP shunt surgery (n = 9, 25.0%), with paralysis and cognitive impairment being the most frequent complaints. Surgical complications or errors (n = 7, 19.4%) were the third most common reason for litigation with unnecessary shunt surgery (n = 4, 57.1%) the most frequent error, followed by surgical material left in the abdominal cavity (n = 2, 28.6%) and improper shunt placement (n = 1, 14.3%). Failure of informed consent prior to shunt surgery or revision was the least common reason for litigation (n = 3, 8.3%).
Reasons for litigation and average payouts.
Legal outcomes and payouts
Out of those cases that returned a jury verdict, the defence succeeded in 16 cases (44.4%) and the plaintiffs in 8 cases (22.2%) (Table 1). Fifteen cases (41.7%) resulted in a settlement. The average payout for cases resulting in a jury verdict in favour of the plaintiff was $4,888,136.75 and for settlements was $1,362,307.69. Payouts for successful plaintiffs ranged from $500,000 to $15,624,061, whereas settlements ranged from $30,000 to $4,100,000.
After analysing average payouts for plaintiff verdicts and settlements pertaining to each reason for litigation, the highest average payout was for delayed treatment or failure to treat that went to trial (Table 2). The average payout for plaintiff verdicts in these cases was $5,329,299.14 and for settlements $1,531,500.00. Among the subgroups involving delayed treatment/failure to treat category with at least two jury verdicts or settlement payouts, the highest average payouts were for failures to diagnose shunt malfunction with an average plaintiff verdict payout of $4,717,515.67 and an average settlement of $1,978,571.43. Failure to refer or delayed referral to a specialist resulted in a higher settlement than jury verdict payout ($1,487,000.00 vs $1,175,000.00, respectively). Failure to interpret a CT scan resulted in a lower jury verdict ($500,000.00) than settlement payout ($1,433,333.33), whereas failure to diagnose shunt infection resulted in a higher jury verdict ($9,000,000.00) than settlement cost ($935,000.00). However, there was only a single case listed for each of these outcomes.
Comparative analysis of plaintiff and defendant verdicts
There were no significant differences between cases that were ruled in favour of a plaintiff versus defendant. However, successful plaintiffs at trial were generally younger than those where the defence were successful (mean age 13.8 versus 27 years) (Table 3).
Comparative analysis of plaintiff vs defendant verdicts.
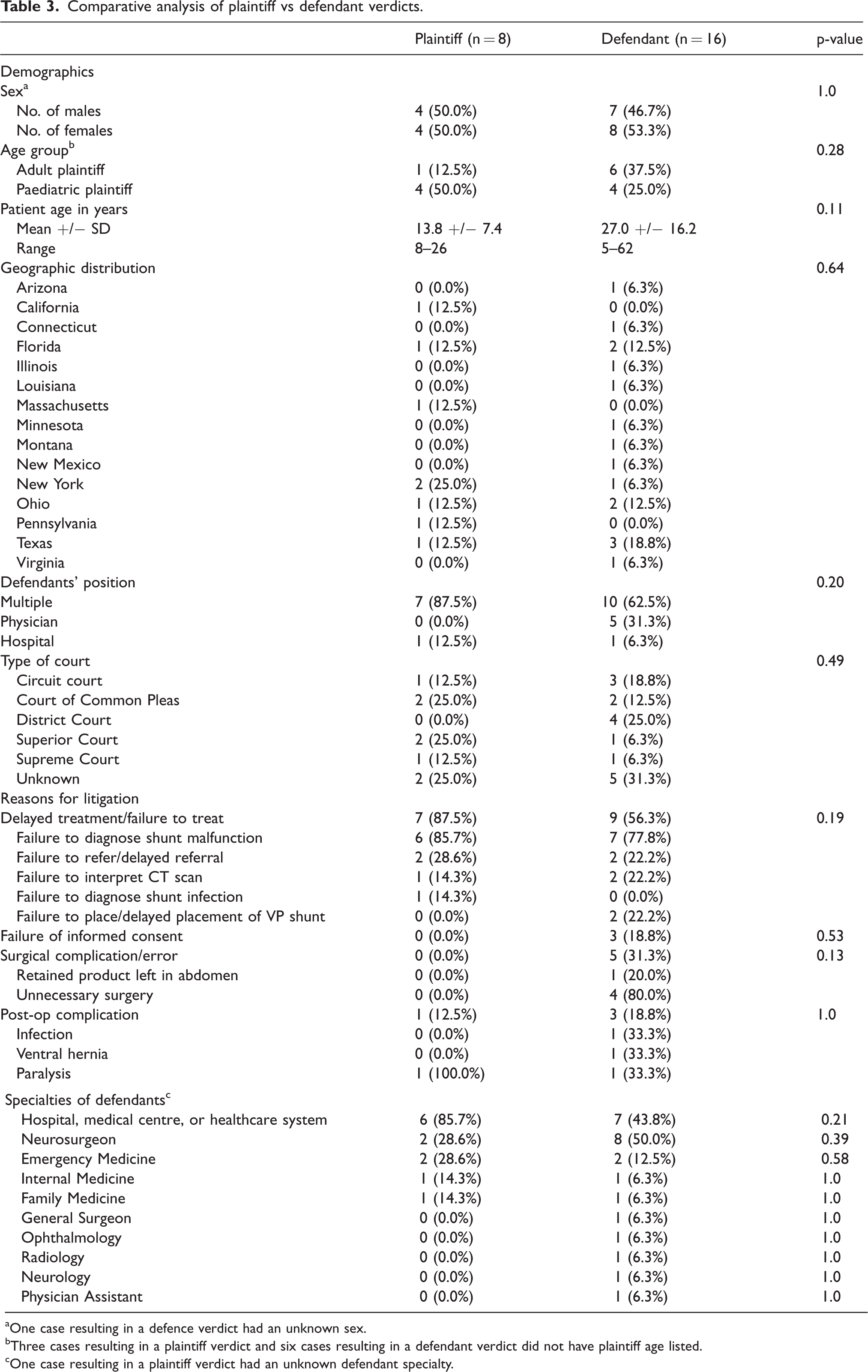
One case resulting in a defence verdict had an unknown sex.
Three cases resulting in a plaintiff verdict and six cases resulting in a defendant verdict did not have plaintiff age listed.
One case resulting in a plaintiff verdict had an unknown defendant specialty.
Out of 8 cases that resulted in a plaintiff verdict, 7 (87.5%) claimed for delayed treatment or failure to treat, with 6 (85.7%) of those cases citing a failure to diagnose shunt malfunction. Only 1 case (12.5%) resulting in a plaintiff verdict listed a post-operative complication. A majority of plaintiff verdicts listed a hospital, medical centre or healthcare system as a defendant (n = 6, 85.7%), with neurosurgeons and emergency medicine physicians listed as the next most cited specialties (n = 2, 28.6, respectively).
In the 16 cases returning a defence verdict, 9 (56.3%) listed the reason for litigation as delayed treatment or failure to treat. Seven (77.8%) were due to a failure to diagnose a shunt malfunction. The remaining successfully defended cases were for claims of a surgical complication or error (n = 5, 31.3%), post-operative complication (n = 3, 18.8%), and failure of informed consent (n = 3, 18.8%). Neurosurgeons were the most frequently listed defendant in successfully defended cases (n = 8, 50%), followed by hospitals (n = 7, 43.8%) and emergency medicine (n = 2, 12.5%).
Discussion
This study presents a 32-year review of litigation cases in the United States related to the management of shunts. The results suggest that several factors may contribute to malpractice proceedings against physicians with the most common factor a physician’s inability to appropriately treat patients with CSF shunts (n = 24, 66.7%), the most common reason failure to diagnose a shunt malfunction (n = 19, 79.2%). Shunt complications after insertion are common with most issues occurring in the first year after surgery.4,5 The revision rate among adults has been reported to be around 20–30%, but paediatric rates are reported as over 50%.6,7 Aside from the high rates of primary revision required, many patients with shunts require more than one revision during their lifetime. 8 Given the high rates of shunt malfunctions, it is not surprising that failure to diagnose a defective shunt is a primary reason for medical malpractice suits. Since the most common reason for shunt complications are malfunction, followed by infection, this further supports the finding that a failure to diagnose shunt malfunction was cited as a more frequent reason for litigation in this study than failure to diagnose a shunt infection (n = 2, 8.3%).8,9 High rates of medical malpractice associated with shunt complications, along with a lack of substantial improvements in shunt revision rates, highlight the need for continued research and improvements in this area.10,11
Post-operative complications were the second most frequently reported reason for court proceedings due to CSF shunt management (n = 9, 25%). Complications from a treatment or surgery are a common plaintiff complaint, as reported in a 2017 survey delineating the most common reasons for medical malpractice trials. 12 As most patients hope to recover after surgery without any major complications, the development of new symptoms and medical issues may lead them to believe this was due to malpractice. Given that a minority of cases arising from post-operative complications resulted in a favourable jury verdict for plaintiffs (n = 1, 11.1%), this indicates a potential disconnect between a physician's explanation of potential post-surgical outcomes and a patient's understanding of the risks.
Surgical complications, including unnecessary surgeries (n = 4, 57.1%), failure to remove surgical instruments from body cavities (n = 2, 28.6%), and improper shunt placement (n = 1, 14.3%), were another source of litigation in CSF management. Given the high rates of shunt placement and surgical revision, it is surprising that more cases related to surgical errors were not observed. Surgical complications, such as hardware misplacement, damage to nearby intracranial or abdominal structures, and poor surgical technique resulting in improper placement of shunt materials, are among some of the potential issues that may arise intraoperatively. Lower rates of litigation for intraoperative complications compared to post-operative complications may be due to more effective informed consent discussions between physicians and patients regarding operative risks rather than those that may occur after surgery.
An analysis of the cost of litigation for cases ending in plaintiff verdicts, compared with settlements, shows that the average cost of a settlement was significantly more cost-effective for physicians compared to cases that went to trial ($1,362,307.69 vs. $4,888,136.75). Although prior legal studies found jury verdicts resulted in smaller payouts for defendants compared with settlements, medical malpractice litigation has been shown to favour settlements as a less expensive option.13–15 This may be due to the fact that settlements often shorten the length of legal cases, resulting in lower attorney fees. Additionally, plaintiffs may be incentivised to accept a settlement offer due to a guarantee on a specified payment amount, rather than risk losing their case at trial.
Comparative analysis revealed that the majority of cases related to CSF management ended in a verdict in favour of the defence (n = 16, 44.4% vs n = 8, 22.2%). Prior studies have demonstrated that the court system tends to favour physician defendants, with a defence verdict reached in about 50% of cases with strong evidence of medical negligence and 80–90% of cases with weak supporting evidence. 16 Reports have also found that physicians who provide higher quality of care to patients tend to fare better in jury trials than those who were rated as providing inadequate service by hospital reviewers.17,18 Although plaintiffs continue to win cases that expert medical reviewers believe lack evidence of malpractice, this evidence suggests that jurors tend to favour physician defendants who they judged had provided credible proof of proper care.
This study is subject to several limitations that should be addressed. One such is the relatively small sample size. The use of specific search terms to query the Westlaw database could have resulted in cases using descriptive terminology of shunt procedures to be missed. Another limitation is that Westlaw only records cases that reached a jury verdict or settlement after the judicial process began, resulting in cases that were dismissed or settled prior to trial being excluded from the analyses. Furthermore, this study was limited to a single legal database. Although Westlaw aims to provide comprehensive information regarding medico-legal cases in the United States, there remains a possibility that not all cases pertaining to CSF shunt management have been included in the database.
Conclusion
This study provides a medico-legal analysis of 36 cases linked to the management of CSF shunts with failure to diagnose a shunt malfunction the most frequently cited cause. The most common legal outcome was a jury verdict in favour of the defendant; trials ending with plaintiff verdicts had a higher average mean payout compared with cases that were settled. The greatest mean payout costs for plaintiff verdicts and settlements were for claims citing a delay in treatment or a failure to appropriately treat patients with shunts.