
Abstract
The current conceptual review sought to identify and describe how the end of life was conceptualized and operationalized in top-ranking, peer-reviewed social work journals considering the highly individualized and multidimensional experience of dying put forth by modern scholars and social work practitioners. An iterative content analysis of included articles (N = 103) revealed six themes within reported definitions and four themes within eligibility criteria. Definitions (n = 66) related to treatment responsiveness, the death process, dying, prognosis, admission to specific services, and old age. Eligibility criteria (n = 18) related to proxy assessment, diagnosis, prognosis, and functional ability assessments. Over one-third of included articles did not define what was meant by the end of life (36%; n = 37) and the majority did not include eligibility criteria (83%; n = 85). In conclusion, the complex lived experience of dying was not manifest within included articles raising important implications for research (e.g., measurement, meta-analysis) and social work practice (viz. service eligibility).
Death is an individualized, multidimensional experience as described by modern death and dying scholars and social work practitioners. Integral to both research and practice related to the end of life, social workers are obligated to engage in research-informed practice and practice-informed research. This predicates the use of a shared language (Hui et al., 2014) to assure parallel efforts in research and in caring for dying persons and their families and friends. This study sought to identify and describe how the end of life was conceptualized and operationalized within top-ranking, peer-reviewed social work journals considering the unique, systems-perspective of death.
Death: An Individualized, Multidimensional Experience
Death, though universal, is perceived uniquely and may be viewed from an ecological perspective (Bronfenbrenner, 1994). Modern theorists contend that dying occurs within a complex intersection of numerous systems—micro (individual), meso (agency or organizational), and macro (sociocultural). At the individual level, death is punctuated by both intrapersonal (viz. within oneself) and interpersonal (viz. between oneself and others) facets and reflects physical, psychological, and metaphysical components (e.g., existential, spiritual). Each of these components, in turn, has further systemic drivers (Copp, 1998; Fahm, 2014; Glaser & Strauss, 1965). Furthermore, death occurs in the space between an individual and the settings in which they are nested—roles at work, church, or in the community—and between the settings themselves. The highly individualized, ecological, and multidimensional nature of death is heralded as critical to understanding the end of life by modern death and dying scholars (Copp, 1998). The markedly complex experience of death is shaped by visible and invisible individual, social, and cultural components and must be reflected as such in research and in practice.
Early theoretical models of death and dying related primarily to psychological processes and the role of an attachment figure. Psychodynamic theories, for instance, posited that death instincts operated in conflict with life instincts. When an individual’s life instincts subsided, therefore, death instincts gained momentum. Later models hypothesized that dying persons would navigate a somewhat mechanistic protocol of five, inter-related psychological stages (e.g., denial, anger; Copp, 1998). Other stage-, phase-, and task-oriented models were later introduced (see Buckman, 1993). However, early frameworks failed to capture the lived experience of dying persons. More recent scholars have included reference to distinct intra- and interindividual processes and the influence of culture on death and dying. For example, Copp (1998) noted that one’s readiness to die (see Copp, 1996) is not simply physiological, but instead, reflects an awareness that one’s body is separate from one’s self.
Death has been acknowledged as both individualized and systems-oriented when defining effective social work in end-of-life care (National Association of Social Workers [NASW], 2004). Social workers are meaningful contributors to end-of-life care and essential to addressing the psychosocial concerns of people who are dying, as well as their families and friends (Brandsen, 2005; Gwyther et al., 2005). Social workers often support resolution of ethical dilemmas, knowledge dissemination of community resources, accounting for patients’ psychosocial histories, and the promotion of patient self-determination in interdisciplinary team meetings (Csikai, 2004).
Social workers are competent to attend to “biological, psychological, social, emotional, spiritual, practical, informational, and financial needs and challenges experienced by the client/patient, family, and caregiver” (Gwyther et al., 2005, p. 92). This systemic orientation recognizes that each person exists within a great nexus of systems (Siporin, 1980). In essence, death and dying theorists and social workers recognize that the end of life is much more than simply the cessation of bodily function.
Professional Obligations and Language
Social workers are obligated to engage in practice-informed research and research-informed practice. Code of Ethics documents for both the British Association of Social Workers (BASW; 2014), the National Association of Social Work (NASW; 2008), and competencies put forth by the Council on Social Work Education (CSWE; 2015) include reference to the professional obligation to support translational efforts across research and practice settings. Conceptualization (how something is defined) and operationalization (how something is measured) are key to this professional obligation. Researchers and practitioners must understand what is meant by the end of life and to whom the end of life refers (Hui et al., 2014) to facilitate such translation and to support dying persons and their families and friends. In research, conceptualization is essential to interpreting and replicating findings, instrument development and refinement, and to identifying best practices and programs through synthesis. In practice, definitions guide access and utilization of client services.
Defining the end of life and recognizing to whom it refers is key to social work research. Clarity is essential to communicating effectively, and thus to research (Carron & Brawley, 2000). Carron and Brawley (2000) note “a lack of conceptual clarity leads to inadequate or inappropriate measurement procedures that, in turn, lead to equivocal or uninterpretable results” (p. 98). Thus, identifying and describing key characteristics of the end of life in social work scholarship supports efforts to enhance definitional clarity and to develop and refine rigorous measures for the field.
Relatedly, identifying to whom the end of life refers supports research synthesis (viz. systematic reviews and meta-analyses). Put another way, researchers must know what is meant by the end of life and to whom the end of life applies (e.g., sample description) to compare studies quantitatively. Sample comparability assists researchers in identifying best practices in end-of-life care and supports generalizability of scholarly literature. Furthermore, research syntheses can enhance the likelihood of clients’ access to best practices by establishing evidence for what works and for whom—a critical component of the ethical codes for both the NASW and BASW.
Defining the end of life also relates to social work practice. A lack of consensus, for instance, influences who receives end-of-life care. Some organizations use biophysiological models to identify those at the end of life. The National Health Service (NHS) states end-of-life care is meant for people who are likely to die within 12 months (NHS, 2015) and the American Medical Association (AMA) relates the end of life to the last 6 months of life (AMA, 2016). Service eligibility, specifically, is dependent upon these conceptualizations of the end of life. In the United Kingdom, people generally must have a prognosis of 12 months to death to qualify for end-of-life care (NHS, 2015). In the United States, patients must have a prognosis of 6 months or less to be eligible for hospice, palliative care, and respite care services under Medicare (Medicare.gov, 2016). The real-life translation of these narrow end-of-life criteria is that end-of-life care is being denied to some individuals, yet extended to others with similar disease trajectories solely on the basis of prognostication. Furthermore, these definitions do not consider the individualized and multidimensional nature of the end of life as do contemporary theories of death and dying, thereby rejecting the theoretical revolution in death and dying scholarship. It is dying persons and their families and friends who bear the burden when the complex lived experience of death is ignored by such groups.
This study upholds the individualized, multidimensionality of death as acknowledged by modern death scholars and the role of social workers as pertaining to end-of-life scholarship and practice. This study highlights the obligation to undertake research-informed practice and practice-informed research and the related importance of conceptualization and operationalization in these efforts. Because of these themes, this study aimed to assess the definitional content of the end of life, including what the end of life means and to whom it refers in social work scholarship as related to the individualized, multidimensionality of death. Here, the key characteristics of end-of-life definitions and eligibility criteria published in top-ranking, peer-reviewed social work journals are identified and described as framed by the understanding of death as a unique and systems-oriented experience to support both practice-informed research and evidence-informed practice.
Methods
An iterative content analysis was used upon data extraction to identify primary themes in social work scholarship as related to both conceptual and operational definitions related to the end of life.
Content Analysis
In every content analysis, Krippendorff (1980) notes that six questions must be addressed: (a) Which data are analyzed? (b) How are they defined? (c) What is the population from which they are drawn? (d) What is the context relative to which the data are analyzed? (e) What are the boundaries of the analysis? and (f) What is the target of the inferences?
Key characteristics of conceptualizations and eligibility criteria of the end of life were analyzed within the peer-reviewed social work scholarship. To define the data, the authors used a purposive sampling frame that was limited to the top 10 social work journals as classified by Hodge and Lacasse (2011) and the Journal of Social Work in End-of-Life and Palliative Care. Purposive samples are common in content analyses and are used to provide new perspectives on a topic. This approach is generally well-received so long as no claims of generalizability are made to groups with different characteristics (Drisko & Maschi, 2016).
This approach to select the top 10 social work journals and the Journal of Social Work in End-of-Life and Palliative Care was chosen to provide theoretical richness and highlight the impact of conceptualizing and operationalizing end of life in high-visibility contexts. These journals are understood as containing the most rigorous research in the social work discipline as ranked by several bibliometric indexes including the Google Scholar h-index, the g-index, and when available, Thomson ISI impact factors. High-quality, peer-reviewed social work scholarship was examined in the following journals: British Journal of Social Work, Social Work, Child and Family Social Work, Social Service Review, Research on Social Work Practice, Health & Social Work, International Journal of Social Welfare, Social Work Research, Families in Society, and Journal of Social Work Education. These journals account for 13.5% of the 80 social work journals identified in the most recent ranking of journals in social work at the time of this study (Hodge & Lacasse, 2011). And as the preeminent peer-reviewed outlet for scholarship regarding end of life and end-of-life care in social work, the Journal of Social Work in End-of-Life and Palliative Care was also included in the sampling frame. Because this is a purposive sample, the sample size in relation to the population is sufficient.
Krippendorff (1980) notes that content analyses require clear context relative to which the data are analyzed. These journals are understood as highly ranked in the social work discipline as denoted by several bibliometric indexes as previously noted. Thus, articles contained within these journals are assumed to possess comprehensive, targeted, and appropriate methods. Themes drawn from these intellectual contributions ought to reflect the advanced expertise of included articles’ authors. Relatedly, Krippendorff notes that content analyses require a clear target of inference. The authors’ intended scope of inference is the most rigorous, peer-reviewed scholarship in social work.
The boundaries of the analysis were demarcated as follows: First, an electronic search of each of the 11 journals was performed whereby articles were included if (a) published in English, (b) between January 2004 and January 2016, and (c) contained any variant of “end of life” (e.g., end-of-life, EoL) in the article title or abstract. The search was limited to articles published after 2004 as this timeframe aligns with the release of the NASW Standards for Social Work Practice in Palliative and End of Life Care—understood as a disciplinary effort to standardize related social work practice in the United States. Second, social work experts in end-of-life care were asked to identify articles believed to serve as seminal texts in the field between January 2004 and January 2016 (e.g., NASW Palliative and End of Life Care Expert Steering Committee). Third, the reference lists of included articles were also searched for articles meeting the inclusion criteria (i.e., reference harvesting).
Three graduate research assistants undertook data extraction upon identifying articles for inclusion using the aforementioned criteria (N = 112). Once articles were identified, the following information was extracted and entered into an Excel spreadsheet: reference, study objective and design (e.g., experimental, quasi-experimental), sample demographics, the conceptual definition of the end of life, eligibility criteria, intervention used (if applicable), and outcomes. The first author assured quality extraction by crosschecking 50% of all articles entered (n = 56).
Next, book reviews and duplicate articles were identified and removed (n = 9). The authors then conducted an iterative content analysis to synthesize the key characteristics of definitions and eligibility criteria obtained from included articles. This process included a separate concurrent coding method for conceptual definitions and eligibility criteria. Specifically, the authors utilized an emergent coding approach to identifying the key characteristics definitions and eligibility criteria as a team. Emergent coding, as opposed to a priori coding, was chosen as consensus did not exist among professional practice and research organizations regarding the end of life. This strategy allowed the authors to identify and refine themes derived organically from published scholarship.
To begin, the authors reviewed the articles to identify novel, literal codes while sorting first conceptual definitions and then eligibility criteria. The authors then compared notes, reconciled differences, and created a consolidated checklist for application in a single, comprehensive session. Disagreements regarding classification were resolved during this concurrent process via peer debriefing and consensus building between the authors (Erlandson, Harris, Skipper, & Allen, 1993). Authors each created their own log used to compare notes and reconcile any differences (Garrison, Cleveland-Innes, Koole, & Kappelman, 2006). An agreed upon coding schema was created once differences between logs were fully reconciled. The authors then applied the schema to included articles.
Differences between the authors’ coding was often rooted in difficulty assigning definitions and eligibility criteria to a singular, primary theme. Instead, definitions (and eligibility criteria) often shared qualities of more than one theme. To remedy these concerns, the authors worked to classify definitions and eligibility criteria based on the components that appeared most commonly in included articles. For example, one such article included numerous references to the end of life: words and phrases referred to “the dying,” “those with life-threatening illnesses,” and “hospice patients” (Arnold, Artin, Griffith, Person, & Graham, 2007). It was thus reasonable to assume that the definition reflected numerous themes. As a result, the current authors used Adobe PDF and Word search functionality to ascertain the included article authors’ primary foci. For this example, the current authors affirmed the phrase “the dying” appeared twice as often as other literal codes. Thus, the end-of-life definition for this example was classified as related to “dying.”
Results
Descriptive Summary of Included Articles
An overview of the articles included in this study can be found in Table 1 (N = 103), and data are available from the first author upon request. Of the journals searched, no qualified articles were found within Child and Family Social Work, Social Service Review, International Journal of Social Welfare, or Social Work Research. Nearly 30% of the included articles were qualitative studies (n = 30), though literature reviews were also common (n = 27; 26%). Editorials, quantitative, and mixed methods studies were also included in the sample.
Characteristics of Included Articles (N = 103).
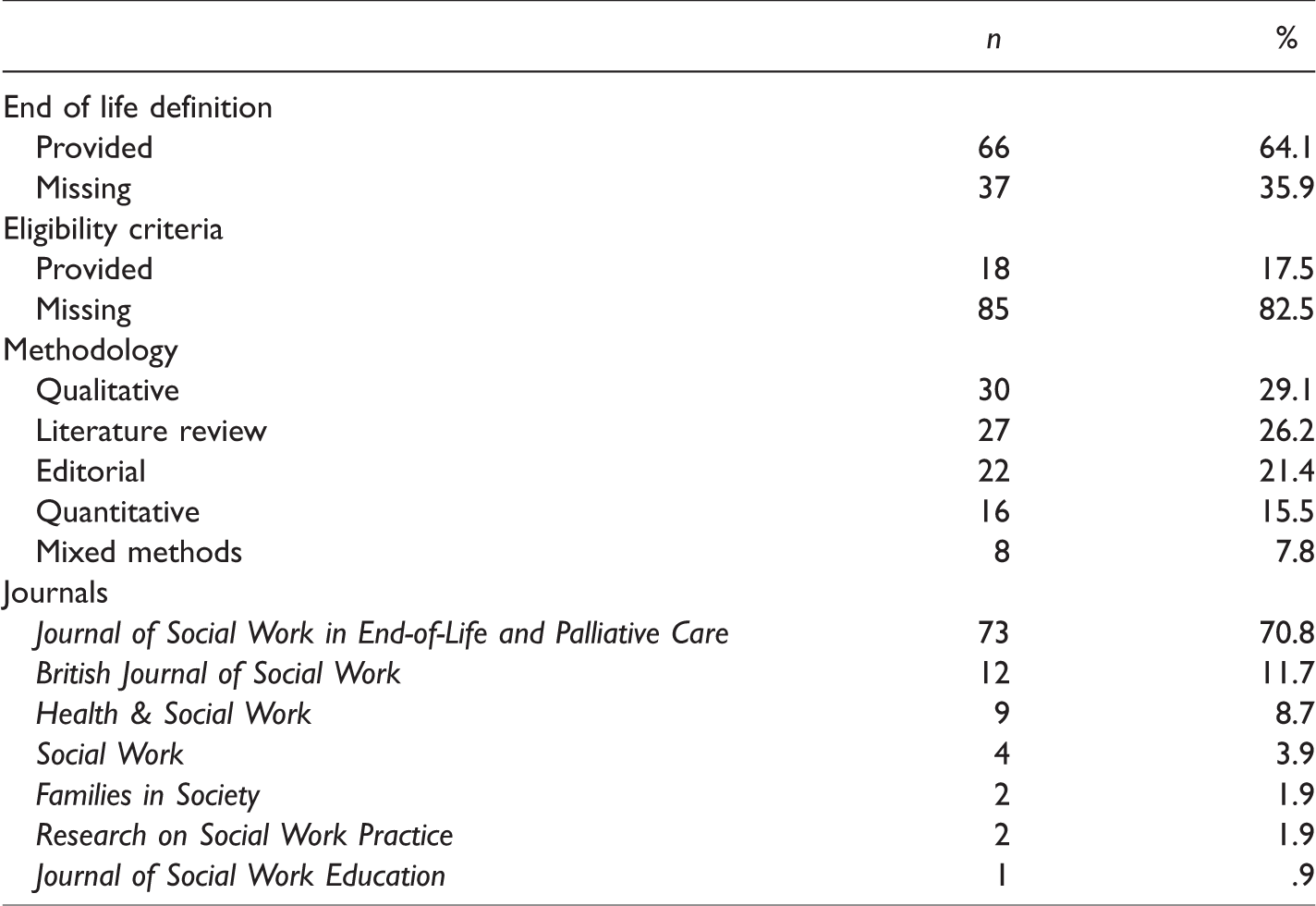
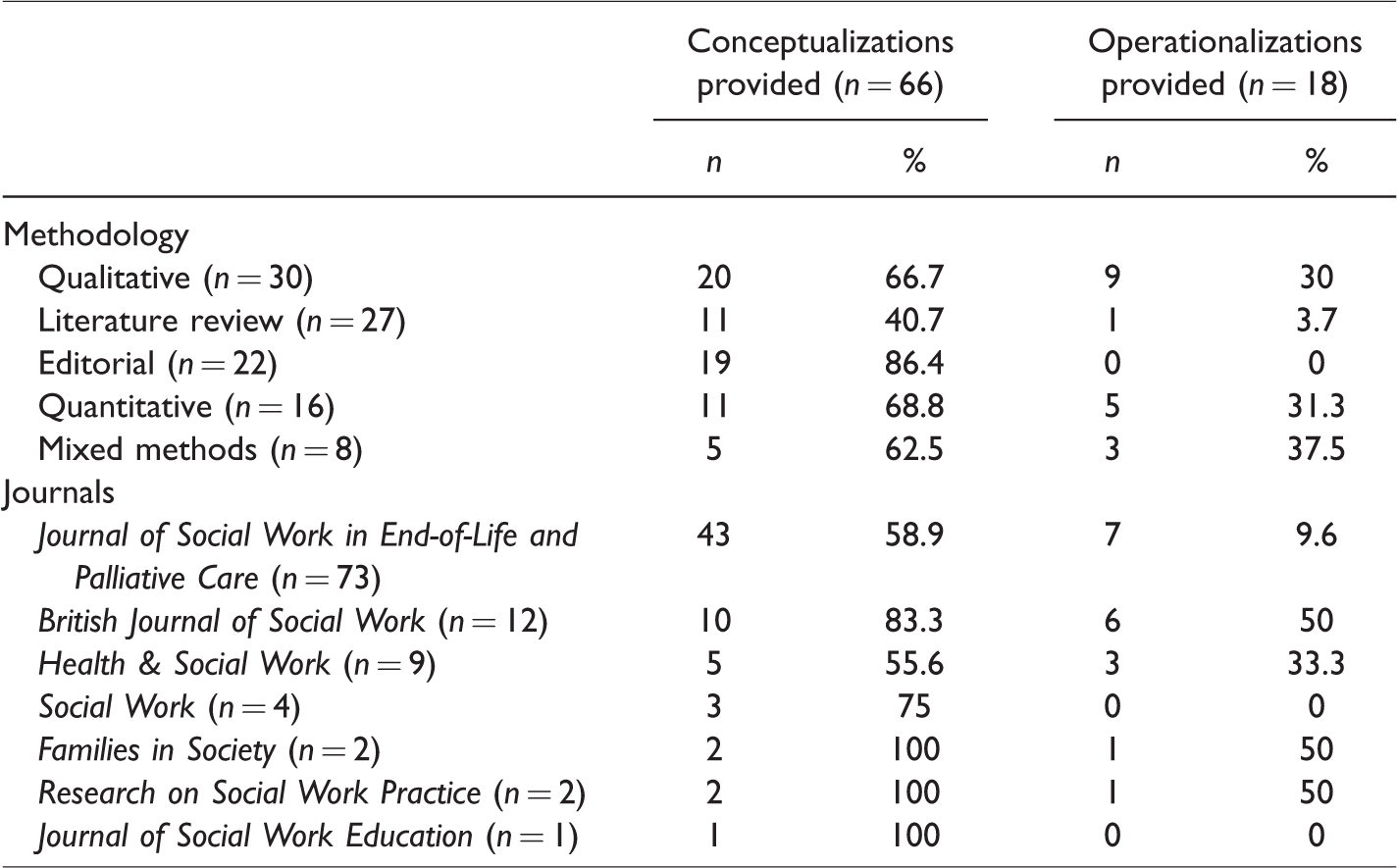
Table 2 provides more detail regarding the frequencies of conceptual and operational definitions within the different types of study methodologies and journals. Importantly, editorials reported conceptual definitions of the end of life most frequently and mixed methods study designs reported operational definitions most frequently. Also, while most (i.e., five of the seven) of the journals contained 75% or more articles with conceptualizations of the end of life, not one journal contained more than 50% of articles with operationalizations of the end of life.
Percentages of Methodologies and Journals That Contained Conceptualizations and Operationalizations of the End of Life (N = 103).
Defining the End of Life
Of the 103 articles, approximately 64% (n = 66) contained definitions of the end of life (see Figure 1). Six primary themes emerged upon completion of the content analysis. These themes were classified as unresponsive to treatment (n = 17), the death process (n = 15), dying (n = 12), prognosis (n = 11), admission to specific services (n = 6), and old age (n = 5).
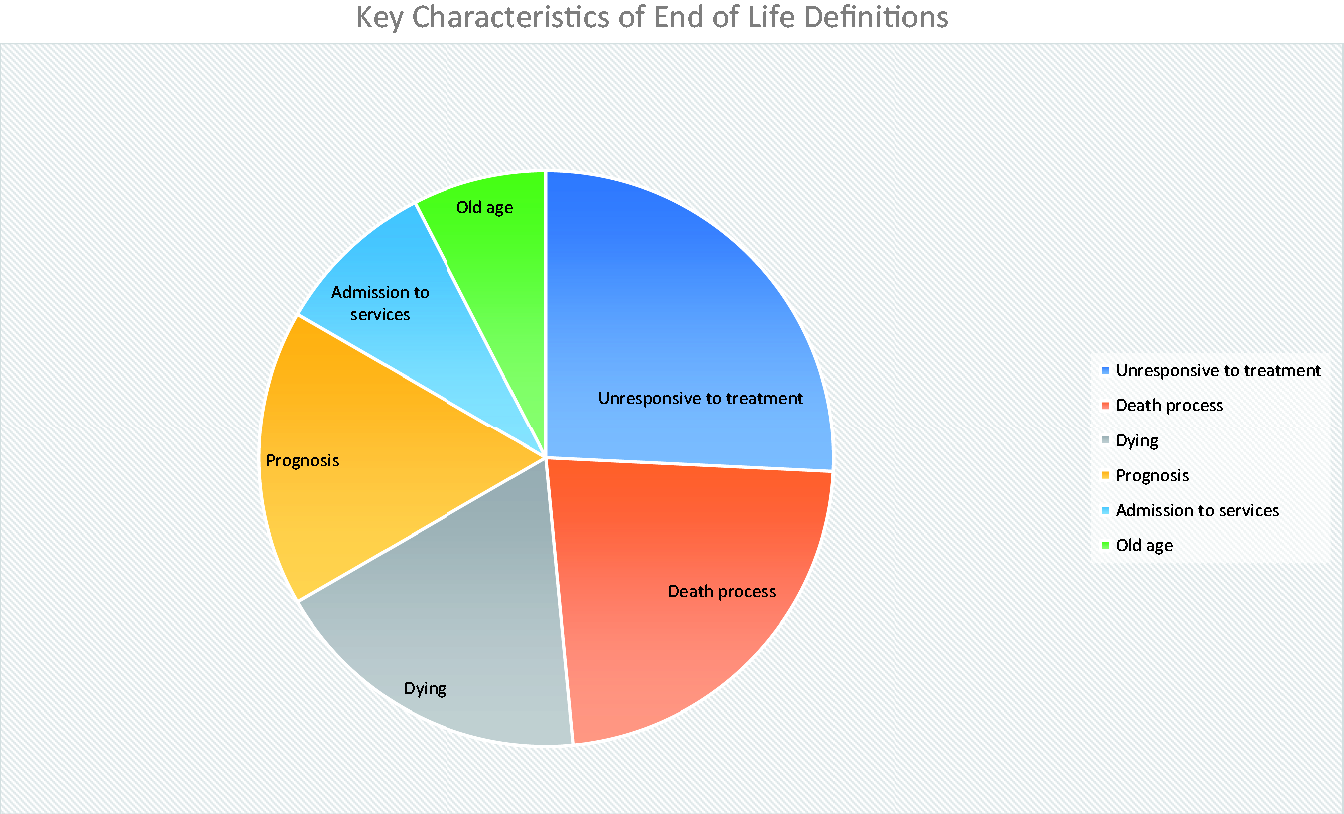
Distribution of key characteristics of end of life definitions provided in included articles published in top-ranking social work journals, 2004–2016.
Unresponsive to Treatment
Definitions related to unresponsive to treatment included having “serious or life-limiting illness” (Morrissey, 2011), clients “who are living with and dying from life limiting illness” (Gwyther et al., 2005), and those who are “severely compromised” (Bern-Klug, 2004) and “terminally ill” (Altillo, Gardia, & Otis-Green, 2007; Anastas, 2011; Brandsen, 2005; Chan et al., 2005; Gardner, 2008; Hebert, 2008; Higgins & Altillo, 2008; Johnson & Stadel, 2007; Mackelprang & Mackelprang, 2005; McCormick, 2011; Miller, 2007; Miller & Hedlund, 2005; Robertson, 2009; Russell, 2015). These definitions focused upon unlikely recovery and failed curative treatments.
Death Process
The second most common theme related to a death process, most often with a focus on a series of milestones. For instance, Simons and Park-Lee (2009) defined the end of life as “when death is anticipated.” Similarly, other definitions discussed advancement toward death: those who are “approaching death” (Murty, Gilmore, Richards, & Atilio, 2012) or “individuals in preparation for death” (Ai, Hopp, & Shearer, 2006). The end of life was also defined as when one has begun to prepare or journey toward death” (Kane, Hamlin, & Hawkins, 2005; Kehl, Kirchhoff, & Hovland-Scafe, 2010; Rose & Shelton, 2006; Sanders, Bullock, & Broussard, 2012; Taylor-Brown & Sormanti, 2004). Waldrop (2007) defines the end of life as a “downhill trajectory,” whereas Agllias (2011) speaks to “impending death” and Munn and Zimmerman (2006) refer to a “predictable death trajectory.” A distinction of this category from others is that the end of life was defined by a progression of events, as opposed to an objective qualities (Hughes, 2013; Nelson-Becker, 2013; Nelson-Becker et al., 2015; Werner, Carmel, & Ziedenberg, 2004).
Dying
A substantial portion of the end-of-life definitions centered simply upon “dying.” Literal codes included “dying” or “people who are dying” (Arnold et al., 2007; Berzoff et al., 2006; Chow, 2013; Christ & Blacker, 2005, 2006; Gustavson & Dal Santo, 2008; Kramer, Pacourek, & Hovland-Scafe, 2003; Jennings & Morrissey, 2011; Jones, 2005; Leichtentritt, 2011; Paul, 2013; Walsh, Corbett, & Whitaker, 2005).
Prognosis
Specific timelines (i.e., time until death) also emerged in literal codes. For example, “less than 6 months to live” was used to define the end of life in three articles (Baker, 2005; Enguidanos, Cherin, & Rumley, 2005; Miller, Hedlund, & Soule, 2006). The end of life was also defined as a period of 12 months prior to death (Brown & Walter, 2014), a “few weeks or months of rapid decline” (Black, 2007), the “last month of life” (Munn & Adorno, 2008; Munn & Zimmerman, 2006), the “last weeks or months of life” (Waldron, Kernohan, Hasson, Foster, & Cochrane, 2013), the last “days or months” (Bern-Klug, Kramer, & Linder, 2005), the “final years” (Flowers & Howe, 2015), and “near the time of death” (Drolen, 2012).
Admission to Services
The end of life was also defined based on services required or admission to specific settings. For instance, Manthorpe and Samsi (2012), Payne (2008), and Murty, Sanders, and Stensland (2015) framed the end of life as a time of “high support needs” and “high levels of disability.” Similarly, the end of life was described as related to persons receiving the “provision of palliative care until death occurs” (Csikai, 2004). In contrast, Rizzo and Rowe (2016) defined the end of life more broadly: any “vulnerable adult” on Medicare services, whereas Colon (2005) only included Medicare beneficiaries who received hospice services.
Old Age
Literal codes least common in this study linked the end of life with old age. “Declining elders” (Hiyoshi-Taniguchi, Becker, & Kinoshita, 2013), those in “very old age” (Ray et al., 2014), “older persons” (Waldrop, 2006), and “older adults . . . with chronic illness and multiple comorbidities” (Bullock, McGraw, Blank, & Bradley, 2005; Witten, 2014) were considered at the end of life.
Eligibility Criteria
Of the 103 articles, less than 18% (n = 18) reported how individuals were designated as being at the end of life via eligibility criteria. Four themes emerged from the content analysis and were classified as the following: proxy assessment (n = 9), diagnosis (n = 4), prognosis (n = 3), and functional ability assessments (n = 2).
Proxy Assessment
The most common criteria used to determine whether an individual was at the end of life required proxy- or caregiver assessment. In such cases, assessments were made by professional caregivers (e.g., physicians, nurses; n = 6) or informal caregivers (e.g., spouse, adult children; n = 3). For informal caregivers, three studies focused on participants whom had experienced the death of a family member, companion, or friend (Hughes, 2013; Luptak, 2006; Munn & Zimmerman, 2006). Another study queried caregivers of older adults at the end of life (Hiyoshi-Taniguchi et al., 2013). Pediatric oncology social workers were also asked to share their experiences with children receiving end-of-life care (Jones, 2005). “Social workers who care for people facing death and bereavement issues” (Chow, 2013), “health-care social workers” who were “professionally involved in the care of dying patients” (Leichtentritt, 2011), hospital social workers (Aldredge & Conlon, 2012), and social workers at long-term care facilities (Munn & Adorno, 2008) were all asked about their professional experiences related to the end of life.
Diagnoses
“Dementia” (Lacey, 2006), “HIV/AIDS” (Creal, 2013), “advanced cancer” (Gardner, 2008), and “heart failure” (Hopp, Thornton, & Martin, 2010) were all noted as requisite criteria for study inclusion within the included articles.
Prognosis
Prognostication emerged as a common theme when identifying whether an individual was at the end of life within included social work literature. Definitions included persons “with a life expectancy of less than 6 months” (Hebert, 2008), those “likely to die within 6 months” (Kramer, 2013), and individuals who “have … 12 months or less to live” (Enguidanos et al., 2005).
Functional Ability Assessments
The least common criterion used to identify to whom the end of life referred relied on use of previously validated measures. Examples included hospitalized participants must have had “a midrange [score of 40–50] Palliative Performance Score” (Waldrop, 2006) and community-dwelling adults receiving hospice services who “had a Palliative Performance Scale score of 40 to 50 or higher” (Waldrop, 2007).
Supplementary Findings
Several findings emerged unrelated to the study aims. First, 4 of 11 journals contained no articles related to the end of life (Child and Family Social Work, Social Service Review, International Journal of Social Welfare, and Social Work Research), and approximately 82% of the journals searched (n = 9) had fewer than 10 articles related to the end of life during the 12-year data collection period. Furthermore, the Journal of Social Work in End-of-Life and Palliative Care contained over 70% of all articles included in the current review (n = 73). This is a logical expectation that not only points clearly to the importance of the Journal of Social Work in End-of-Life and Palliative Care but also indicates a dearth of studies related to the end of life in other social work journals despite the universality of death.
Second, results revealed that over 80% of included articles did not include eligibility criteria and 36% of included articles did not contain a definition for the end of life.
Absent or limited conceptualizations and eligibility criteria are not unique to the study of the end of life nor to the discipline of social work. Vague conceptualization has been noted regarding family and school relationships (Moon & Rao, 2010), loneliness (Evans & Dingus, 1987), and therapies for individuals reentering society from incarceration (Kenemore, 2014). It is possible that definitions were not provided because readers were expected to understand what was meant by the end of life leading researchers to believe conceptualization was unnecessary. However, due to the variability noted across definitions put forth by the AMA, NHS, and Medicare, this is unlikely the case. It is also possible that detailed definitions and eligibility criteria were presented initially in longer forms of the included articles but may have been removed due to manuscript length constraints of journals. However, the absence of definitions and eligibility criteria does pose concern for this study aims—one cannot assess what is meant by the end of life or to whom it refers in social work scholarship if such information is not provided.
Discussion
This study sought to capture what is meant by the end of life and to whom it refers in social work scholarship by identifying and describing key characteristics of end-of-life definitions and eligibility criteria published in top-ranking, peer-reviewed social work journals. This study did this with the understanding that modern death and dying scholars and social work recognize death as an individualized, multidimensional experience and that the way the end of life is understood shapes both research and practice. The resultant themes, then, are understood as critical components of the end of life within the most rigorous social work literature.
The end of life within this context refers to persons who are of older age, unresponsive to life-saving treatments, and receiving supportive services during a time-limited, dying process. Eligibility criteria used to ascertain whether an individual is at the end of life, in turn, reflects specific diagnoses or prognoses, and proxy or functional ability assessments. No primary theme captured adequately the lived experience of dying persons as neither individuality nor multidimensionality emerged as central to definitions and eligibility criteria in social work scholarship.
The following sections address benefits and barriers with each of the emergent themes regarding the end of life in the social work literature. Broad considerations are discussed regarding the themes, the lived experience of dying persons, and conceptual opacity. Finally, three elements are presented that are believed to be critical to creating a framework for capturing the individuality and multidimensionality of the end of life in social work scholarship.
Broad, Flexible Definitions Offer a Wide Net
Three themes (i.e., dying, death process, and proxy assessments) left great space for interpretation. The broad, subjective nature of these definitions raises concern regarding practice and research. However, these themes also offer increased flexibility as to whom the end of life applied potentially reflecting the lived experience of dying persons more than more narrow themes.
Defining the end of life as “dying” provides social workers nearly unlimited opportunity regarding to what the end of life refers and to whom the end of life applies. However, casting this broad net may inadvertently lead to capturing individuals who do not see themselves as dying in research. In addition, such a broad definition of the end of life makes eligibility for services difficult to assess, as it is unclear who is and is not dying by this standard.
Several codes also related to understanding the end of life as contingent upon undergoing a death-related process raising concerns for translational efforts in practice and research. Reliance on definitions focused on process proves problematic, as well. For example, persons who complete a living will can be considered at the end of life as they are undergoing a death-related process (e.g., preparing for death). Skilled nursing facilities are another example. In the United States, these facilities frequently provide rehabilitative care for patients exiting hospitals. Recently, these agencies have been approved to provide end-of-life care by providing advance care planning services to Medicare-enrolled patients as a billable service (Centers for Medicare and Medicaid Services, 2016). However, the service may be provided to a patient who received a knee replacement and simply needs inpatient physical therapy. Researchers have noted similar concerns with process-based definitions and have called for further constraints to assure reliability and validity of associated measures (see Abdel Latif, 2012; Parry & Roth, 1997; Van Ness, 2005).
Regarding our efforts to examine the extent to which the lived experience is captured in social work scholarship related to the end of life, not one characteristic relied on self-identification or self-assessed measures. Proxies’ assessment was often used to identify dying persons. However, proxy assessments, even when completed with the utmost care by professionals, rarely reflect the patients’ perspective (Arons, Krabbe, Schölzel-Dorenbos, van der Wilt, & Olde Rikkert, 2013; Crocker, Smith, & Skevington, 2015; Sneeuw, Sprangers, & Aaronson, 2002; Zucchella, Bartolo, Bernini, Picascia, & Sinforiani, 2015). Some evidence indicates that proxies project their own experiences onto the other persons when providing assessments to researchers and to care teams (Arons et al., 2013). Oftentimes, proxies believe that the person whom they are assessing has a lower quality of life (QoL) that the person would report for themselves. Therefore, it is possible that proxies would designate patients to be at the end of life when the patient does not believe that to be the case. The NASW Standards for Social Work Practice in Palliative and End of Life Care (2004) denotes clearly that social workers in end-of-life care settings are to identify and define needs from the client’s perspective and a large body of research holds that proxy reports are to be treated with caution (Zucchella et al., 2015).
In addition to these concerns, taking into consideration the ethical codes and aims of social work, it is worrying that individual experiences were absent in the social work literature. Social workers are called to encourage self-identification and completion of self-assessed measures to promote empowerment and self-determination. Such perspectives ensure that autonomy remains intact for dying persons. Although bias and burden are inherent, self-assessment remains the gold standard in areas surrounding the end of life (see Sneeuw et al., 2002; Zucchella et al., 2015).
Narrow Definitions and Arbitrary Exclusion
Six themes (i.e., unresponsiveness to treatment, prognosis, diagnosis, admission to services, old age, and functional ability) were identified and are considered markedly narrow. These definitions are thus easier to understand compared to broader themes but may exclude persons who identify as at the end of life due to their rigidity.
Unresponsiveness to treatment was reflected via the presence of serious, life-limiting illness (viz. “terminally ill”) or a state of severe compromise. The conceptual focus on failed curative treatments may provide helpful guidance for social work practitioners’ identification of persons at the end of life as this demarcation is associated with the beginning of palliation and comfort care strategies (National Hospice and Palliative Care Organization [NHPCO], 2017; Snow, Warner, & Zilberfein, 2008). This may help to assure access and utilization of appropriate services.
Definitions and eligibility criteria often cited prognostication or diagnoses as key to describing those at the end of life. Although these simplistic approaches allow for clear “sorting,” so to speak, prognoses and diagnoses are problematic in determining when a person is at the end of life. For example, accurate prognostication is difficult to achieve and previous studies have revealed recurrent inaccuracies (Christakis & Lamont, 2000). In addition, contention exists regarding which diagnoses should be considered chronic and life-threatening (Bernell & Howard, 2016). The ultimate end of an individual’s life can only be known after it has occurred and the innumerable trajectories of dying translate to variable periods of time when a patient could be considered at the end of life. This uncertainty in the nature and timing of death are likely drivers of different intradiscipline definitions of the end of life (i.e., <6 months, <12 months). However, these criteria are inadequate for determining if a person is at the end of life, because these definitions may incorrectly include people who do not identify as being at the end of life or incorrectly exclude people who do identify as being at the end of life.
Admission to specific services and use of previously validated measures central to definitions and eligibility criteria may prove supportive in social work practice and research. However, longer life expectancies among people living with chronic conditions may also result in the artificial labeling of those with “high support needs” and “high levels of disability” as at the end of life when that same individual may not see themselves as dying. In the same way that prognostic and diagnostic criteria are inappropriate to use as sole indicators of people being at the end of life, admission to services and functional ability measures may inappropriately include or exclude people from being designated as at the end of life.
Upholding Lived Experiences or Conceptual Opacity?
The emergence of numerous themes in conceptual and operational definitions may reflect the disciplinary understanding of the mutual importance of numerous factors regarding the end of life as is noted in the NASW Standards for Social Work Practice in Palliative and End of Life Care (2004). However, it may also point to limited conceptual clarity surrounding the end of life in social work. The presence of no less than four emergent themes in conceptualizations and operationalizations may reflect that social workers recognize the many varied experiences of persons during this developmental stage. Lamont (2005) recognized that the end of life reflects a period when medical care is distinct from other periods during the life course. The author continues stating that “efforts must be made to improve the prospective identification of the end of life” and that such efforts must take place “at a population level to ensure wide applicability” (Lamont, 2005, p. 1). What might be interpreted as conceptual opacity may in fact be an effort to paint death with broad strokes in both social work scholarship.
However, it is also possible that the emergence of no fewer than four themes is evidence of limited conceptual clarity—a concern known to exist throughout social work literature. Constructs previously critiqued include vicarious traumatization (Baird & Kracen, 2006), burnout (Maslach, 1987), compassion fatigue (Adams, Boscarino, & Figley, 2006), recovery (Leamy, Bird, Le Boutillier, Williams, & Slade, 2011), group cohesion (Carron & Brawley, 2000), and interprofessional interventions (Reeves et al., 2011).
With this in mind, it is possible that when social work authors referenced the “end of life” in their work, it was believed that their readers understood what they mean due to the pervasive presence of the phrase in society. However, this study results indicate that authors are not, in fact, describing the same concept. Thus, readers cannot be expected to understand the authors’ exact focus. This opacity is not unlike findings presented by Smith and colleagues regarding QoL (Smith, Avis, & Assmann, 1999). The authors note that QoL is often used as a “generic label” and is interchanged with other physical and psychosocial variables (Smith et al., 1999). Therefore, it is possible that the end of life is similarly shrouded in genericism—written, read, and interpreted in a multitude of ways.
Conceptual Framework for Understanding the End of Life in Social Work
As previously noted, this study results point to the end of life in social work scholarship as a time when persons who are of older age are unresponsive to life-saving intervention. Those at the end of life include individuals receiving supportive services in the midst of a constrained, death-related process. Diagnoses, prognoses, and proxy and functional ability assessments are often used to identify dying persons. However, these characteristics neglect the interrelated systemic forces at work—the recursive influence from and toward familial, community, or societal/cultural systems. Thus, included social work scholarship did not encompass the multidimensionality identified as critical to the lived experience of dying persons. Missing, too, is recognition of individual perspective—perhaps most evident by the frequent reliance on proxy assessment in the identification of eligible persons (Copp, 1998). Based on this study findings, the following are recommended as key to creating a framework for describing the end of life in social work:
Embrace parallel language in end-of-life practice and research to enhance translational efforts. Increase use of self-identification and self-assessed measures in practice and research to encourage client empowerment, self-determination, and autonomy. Integrate a multidimensional, systems-oriented perspective into conceptual and operational definitions of the end of life in social work scholarship.
Limitations
The primary limitation of this study is the inability to generalize the studies in this small number of journals to a larger, professional stance on a definition of the end of life. Relatedly, the restricted sampling frame does not allow for inclusion of social work scholarship published in high-impact, multidisciplinary journals indexed in other databases (e.g., Scopus). However, the narrow sampling frame and strict search criteria of this study reflects an effort to understand the end of life as reflected in the most preeminent journals in social work and thus—a reflection of the most strongly vetted and scrutinized literature in the discipline. Similarly, because this study only focused on social work-specific journals, it is not possible to say if these findings are consistent across end-of-life scholarship in other disciplines (e.g., medicine, sociology).
Also, the qualitative approach used may be associated with limitations. Considered both rich and complex, qualitative approaches have been critiqued as subjective and therefore biased (Hesse-Biber, 2017). However, efforts to reduce risk of bias were made by establishing a detailed, a priori protocol for article identification and data extraction. This study also relied upon an emergent, concurrent content analysis of the extracted data to synthesize key characteristics of included definitions and eligibility criteria, and embedded software tools were used when disagreements regarding primary themes emerged (i.e., search functionality).
Conclusion
How the end of life is defined and to whom it applies links closely to social work’s professional call to embrace research-informed practice and practice-informed research and ability to support dying persons and their families and friends (BASW, 2014; NASW, 2008). Parallel conceptual and operational definitions are also linked to effective communication (Hui et al., 2014). The creation and adherence to a singular, unified construct may raise concerns regarding the likely failure to integrate other, relevant factors to an individual’s lived experience. Thus, to construct and promulgate one widely held definition for the end of life in social work is perhaps impractical or impossible though professional organizations such as NASW or BASW may be best situated to offer guidance in this realm. The Society for Social Work and Research may also be well-suited to lead such a discourse and to develop a framework regarding the end of life and other, similar disciplinary research and practice areas. However, future practitioners and researchers are encouraged to embrace parallel language in their end-of-life efforts, to encourage empowerment, self-determination, and autonomy by using self-identification and self-assessed measures in practice and research, and to integrate a systems-oriented framework when defining the end of life while recognizing the importance of dying persons’ individual perspective.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.