
Abstract
The aim of this study was to determine nurses’ opinions on Do Not Resuscitate (DNR) orders. This is a descriptive study. A total of 1250 nurses participated in this study. The mean age of participants was 34.5 ± 7.7 years; 92.6% were women; 56.4% had bachelor’s degrees, and 28.8% were intensive care, oncology, or palliative care nurses. Most participants (94.3%) agreed that healthcare professionals involved in DNR decision-making processes should have ethical competence, while they were mostly undecided (43%) about the statement whether or not DNR should be legal. More than half the participants (60.2%) disagreed with the idea that DNR implementation causes an ethical dilemma. Participants’ opinions on DNR decisions significantly differed according to the number of years of employment and unit of duty. The results showed that most of the nurses had positive attitudes towards DNR orders despite it being illegal. Future studies are needed to better understand family members’ and decision makers’ perceptions of DNR orders for patients.
Whether or not to perform cardiopulmonary resuscitation (CPR) is a decision that makes the difference between saving and ending someone’s life. Do Not Resuscitate (DNR) orders not only make physicians and nurses question their moral values, but they also cause legal concerns. Moreover, in most countries DNR instructions are not clear, and therefore healthcare professionals face numerous ethical dilemmas (Akyıl, 2017; Kuvaki et al., 2014; Riva et al., 2019).
DNR orders are affected by numerous factors such as patient’s age, medical history, quality of life, and previous decisions, as well as physicians’ medical decisions, prolonged cardiac arrest, patients and their family members’ educational levels, healthcare professionals’ and patients’ religious beliefs, culture, and the law (Beaty, 2015; Chang et al., 2010; Emami-Razavi et al., 2014; Gouda et al., 2018; Hileli et al., 2014; Steinberg, 2011). Given fair use of resources, and the effective use of beds in ICUs are other factors affecting DNR orders (Baharoon et al., 2010; Büyükkoçak & Çakırca, 2007; Gönenç, 2015).
DNR is legal in the US, Australia, Canada, Taiwan, and in some European countries, and DNR decisions are discussed with patients and their family members, and patients can give legal written consent (Bossaert et al., 2015; Chang et al., 2010; Santonocito et al., 2013). But DNR is illegal in most Middle Eastern countries based on the Muslim belief that “only God knows when death will arrive and people cannot change this” (Baharoon et al., 2010).
A study conducted in Palestine reported that physicians and nurses had positive attitudes towards the legalization of DNR (Abdallah et al., 2016). Another study in Palestine pointed out that the religious beliefs of physicians and nurses greatly affected their opinions on DNR (Saifan et al., 2016). Another study in Iran indicated that nurses had negative attitudes towards DNR due to their Islamic beliefs (Mogadasian et al., 2014).
DNR order is not legal in Turkey, although the laws, regulations, and declarations do not have a definite provision concerning the practice. There are very few studies investigating healthcare providers’ opinions on DNR in Turkey. Kuvaki et al. (2014) reported that half of physicians thought that all DNR orders must be written and that nearly half the physicians did not know whether or not DNR was legal in Turkey. Çobanoğlu and Algıer (2004) conducted a study to determine the ethical problems that ICU physicians and nurses experienced and reported that nearly half the participants perceived DNR as an ethical problem.
Results of the studies that conducted on Muslim nurses’ opinions on DNR are limited (Mogadasian et al., 2014; Emami-rezavi et al., 2014; Saifan et al., 2016). Although there are limited studies that focused on the view of Muslim nurses about DNR, to the best of our knowledge there is no study focusing on comprehensive views of nurses on DNR orders in Turkey and other Muslim countries.
Methods
Study Aim
The aim of this study was to determine Turkish nurses’ opinions on DNR orders and investigate whether their opinions differed according their characteristics.
Design
This is a descriptive study.
Sample and Setting
The study sample consisted of nurses who were members of the Turkish Nurses Association and specialized nursing associations (oncology nursing, intensive care nursing, and surgical and operating room nurses). The inclusion criteria were being able to read and write in Turkish and being willing to participate in this study. Non-Muslim nurses were not included in this study. A total of 1250 nurses participated in this study.
Data Collection
Data were collected from July 2019 to September 2019 using an online survey. The online survey was emailed by association authorities to members. In addition, participants were asked to forward the survey to other nurses in their network.
This study was approved by Institutional Review Board at Koc University (IRB number 2019.035.IRB3.018).
Data Collection Forms
Data collected via online survey developed by the researchers based on a literature (Abdallah et al., 2016; Gouda et al., 2018; Saifan et al., 2016), and created using Google Forms. The survey consists of 12 questions on socio-demographic characteristics (age, gender, place of work, term of employment, etc.) and 28 statements about DNR orders such as “DNR orders are affected by religious beliefs,” “I think that DNR is appropriate for our culture,” “my cultural background affects my attitudes towards DNR,” “healthcare professionals involved in DNR decision-making processes should have ethical competence,” and “DNR should be a part of vocational training.” The survey was in Turkish and developed for this study. Participants were asked to fill out the survey by selecting “agree,” “neutral,” or “disagree” for the statement about DNR order.
Data Analysis
Data were transferred to Excel and analyzed using the Statistical Package for Social Sciences (SPSS, IBM v. 26.0) at a significance level of 0.05. Frequencies and percentages were used for categorical variables, while means and standard deviations were used for measured variables. The Pearson’s chi-square test was used to compare socio-demographic characteristics and participants’ opinions on DNR.
Results
Characteristics of the Sample
The total of 10,315 surveys were sent to members of nursing associations. Of the nurses 12.11% responded to the survey. The mean age of participants was 34.5 ± 7.7 years; 92.6% were women; 56.4% had bachelor’s degrees, and 28.8% were intensive care, oncology, or palliative care nurses. The mean duration of employment was 12.6 ± 8.6 years, and 38.3% had durations of employment of ≥16 years. The mean duration of employment was 12.6 ± 8.6 years. Of the participants, 79.9% had experience in caring for terminally ill patients (now or before), and 71.0% witnessed terminally ill person in their family; 76.8% had difficulty talking to patients; 63.8% had difficulty talking to family members about death; 71.0% had witnessed the terminal period of family members and relatives; 57.5% did not attend any conference, training, seminar, or course on approach to patients with terminal illnesses after graduation, and 95.0% were informed of patients’ rights (Table 1).
Participants’ Characteristics and Experiences With Terminally Ill Patients (N = 1250).

*Family health center, ministry of health, home health service, management, quality unit, infection control committee.
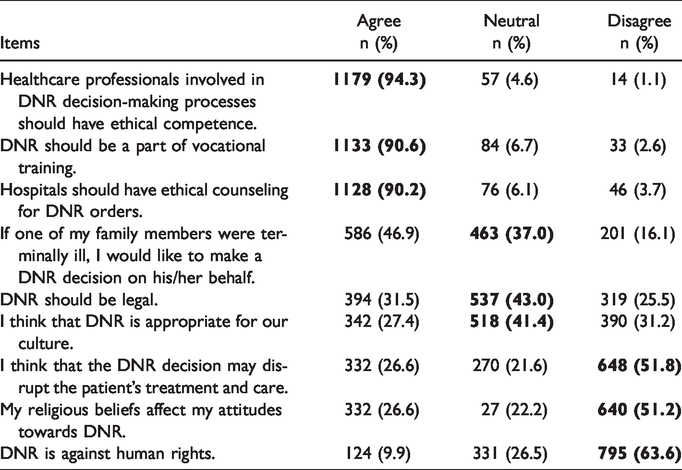
Table 2 shows the participants’ three frequently responses for each answer option (“agree,” “neutral,” and “disagree”) about DNR orders. Participants mostly agreed with the statements “Healthcare professionals involved in DNR decision-making processes should have ethical competence” (94.3%), “DNR should be a part of vocational training” (90.6%), and “Hospitals should have ethical counseling for DNR orders” (90.2%). They were mostly neutral about the items “DNR should be legal” (43.0%), “DNR is appropriate for our culture” (41.4%), and “If one of my family members were terminally ill, I would like to make a DNR decision on his/her behalf” (37.0%). They mostly disagreed with the items “DNR is against human rights” (63.6%), “I think that a DNR decision may disrupt the patient’s treatment and care” (51.8%), and “My religious beliefs affect my attitudes towards DNR” (51.2%) (Table 2). The top three frequently answered statements for each answer option (“agree,” “neutral,” and “disagree”) were shown in bold (Table 2) (see Supplemental File for all participant responses for all statements).
Participants’ Opinions on DNR (N = 1250).
Although not shown in table, participants’ responses to the DNR items were compared in terms of gender, year of employment, and unit of duty. The results showed that the intensive care/oncology/palliative care nurses agreed significantly more with the items “I think that CPR is futile (useless) in some cases and for some patients” (X2 = 48.024, p < 0.001), “If one of my family members were terminally ill, I would like to make a DNR decision on his/her behalf” (X2 = 21.920, p < 0.001), and “If I were a terminally ill patient, I would like my DNR order to be honored” (X2 = 33.572, p < 0.001) than did other participants. The nurses with 16 years of employment or more (X2 = 12.875, p = 0.045) and the intensive care/oncology/palliative care nurses (X2 = 43.823, p < 0.001) agreed significantly more with the item “DNR prevents unnecessary pain or suffering” than other participants. The nurses with 16 years of employment or more (X2 = 12.919, p = 0.044) and surgical clinic nurses (X2 = 39.190, p < 0.001) agreed about the item “Extending life is the goal of healthcare professionals regardless of the demands of the patient and his/her family members. CPR should, therefore, be performed in all circumstances”. The intensive care/oncology/palliative care nurses agreed significantly more with the item “I think that there should be legal regulations regarding DNR orders in Turkey” (X2 = 40.146, p < 0.001) than did other participants.
Discussion
To the best of our knowledge, this is the first study with a large sample to investigate Turkish nurses’ opinions on DNR. In this study participants had various opinions on the subject. Some were in favor of DNR, while others were neutral about some aspects of it. Participants’ opinions on DNR differed by year of employment and unit where they work. The American Heart Association Guidelines for CPR and Emergency Cardiovascular Care stipulate that “healthcare professionals should consider withholding or withdrawing CPR in children and adults when there is other strong evidence that further CPR would be against patient’s values and preferences or is considered futile” (Mancini et al., 2015). However, futility is not based on a precise and easily established criterion. Therefore, there is no consensus on what should be considered as “futile” treatment (Gönenç, 2015). In this study, the intensive care/oncology/palliative care nurses agreed with the idea that CPR is useless and that DNR prevents pain and suffering. In addition, the nurses with 16 years or more of employment agreed with the idea that DNR prevents pain and suffering. This result is not surprising if we consider that these nurses mostly providing care to terminally ill patients. More ever, it is known that nurses with years of professional work experience have better perceptions and acceptance of death (Cevik & Kav, 2013; Abu-Hasheesh et al., 2013; Yılmaz & Vermisli, 2015). This may be a reason of 16 years or more of employment agreed with the idea that DNR prevents pain and suffering. Oppositely of this result nurses with 16 years or more of employment and surgical nurses were in favor of the idea that CPR should always be performed. Surgical nurses mostly provide care to patients with more acute diseases and higher recovery rates than others. Therefore, it is thought that surgical nurses advocate CPR more than other nurses due to the nature of the patients they care for. However, most participants thought that CPR was ineffective for some patients under some circumstances and that not all patients with terminal illnesses should be kept alive until the end. Our findings are in line with the other studies’ results (Mostafa & El-Din, 2019; Oh et al., 2006). Given the nature of the issue, it is not surprising that participants’ opinions differ.
DNR order depends on values, norms, traditions, belief systems, and legal regulations. The decision to initiate or withhold resuscitation leads to ethical and legal debates in countries where DNR is not legal, including Turkey where DNR is discussed with reference to euthanasia, and therefore the crime of voluntary manslaughter defined in the Turkish Criminal Code becomes an important part of those discussions. This leads to ethical dilemmas and problems in terms of the quality and limits of the duties of physicians and nurses. Most of our participants agreed that DNR leads to ethical dilemmas, which has been reported by previous studies as well (Çobanoğlu & Algıer, 2004; Gönenç, 2015).
Although most of our participants knew that DNR is not legal in Turkey, they stated that there should be legal regulations concerning the practice. Nearly half the participants were neutral about the legality and execution of DNR, however, they agreed that health policies affect DNR orders, that there should be legal and written protocols on DNR, that the situation should be explained to patients with terminal illnesses and their family members, and that their DNR decisions should be made clear. The results of the studies conducted in Palestine where there is no legal regulations on DNR and has a primarily Muslim population similarly Turkey show that most of nurses who participated in studies agree that DNR should be regulated (Abdallah et al., 2016; Saifan et al., 2016), which is similar to our result.
Many studies show that religion and culture greatly affect physicians’ and nurses’ opinion on DNR (Abdallah et al., 2016; Emami-Razavi et al., 2014; Hileli et al., 2014; Saifan et al., 2016). Most Muslims believe that DNR is banned by Islam (Albar, 2007). According to Islam, death occurs by God’s permission, and the Quran stipulates that “If anyone slays a person, it would be as if he slew the whole people: and if any one saved a life, it would be as if he saved the life of the whole people” (Saifan et al., 2016). Mogadasian et al. (2014), found that Iranian nurses have completely negative opinions on DNR due to their religious beliefs. Our participants stated that their opinions on DNR were affected by their religious beliefs and that they were unsure DNR was appropriate for the Turkish culture.
DNR decisions are affected many factors, including who makes those decisions. A study reported that DNR decisions might be affected by physicians’ age, experience, education, religion, spouse and family pressure, and by the patient’s age and demands (Kuvaki et al., 2014). Another study examined nurses and physicians with more experience and training had more positive attitudes towards DNR decisions (Fallahi et al., 2016). In our study, ICU/oncology/palliative care nurses with more professional experience had more positive opinions on DNR. It was thought that this result is mostly since those nurses working in these departments have more experiences on providing care for terminal patients.
DNR is an order that requires clear communication between healthcare professionals and patients and/or their family members (Akyıl, 2017). It is defined by legal standards and regulations in countries such as the US, Canada, Germany, Switzerland, China, France, the United Kingdom, and Australia (Bossaert et al., 2015), where health institutions, physicians, families, and other interested parties can act more easily, clearly, and consciously about DNR, and both physicians and other parties (family, close friends, etc.) agree that patients should be involved in CPR decisions (Resuscitation Council (UK), 2014; Bossaert et al., 2015). One study reported that 30% of physicians agreed that patients should participate in DNR decisions even though DNR is illegal and there are no guidelines for DNR decisions in Turkey (Kuvaki et al., 2014). In this study, most of our participants stated that CPR and DNR decisions should be made by patients and their family members in this study. In this study, nearly half of the participants stated that they would like to be involved in DNR-related processes; however, most of them also stated that they had difficulty speaking to patients and their family members about death. Similar to our results other studies found that healthcare professionals have difficulty in discussing DNR decisions with patient/families (Akazi, 2014; Santonocito et al., 2013). This might be due to healthcare professionals’ fear, inexperience, lack of education, and communication problems about DNR decisions. Further studies should be done to explore the reason of this situation.
Another issue that causes a dilemma or is misunderstood is what kind of care should be provided to patients with a DNR order. Such patients do not receive CPR, ICU admission, intubation, or inotropic support, but they are provided with all treatment and care necessary for their comfort (Gouda et al., 2018). Some studies indicate that physicians are concerned that patients with a DNR order may be deliberately provided with low-quality care (Beach & Morrison, 2002; Gouda et al., 2018). Our participants think that DNR prevents pain, does not interfere with current treatment and care, and that patients both with and without DNR orders receive health care services of the same quality. Healthcare providers should be aware of that DNR, doesn’t mean, don’t treat. However, supportive care should be provided for all DNR patients (Mostafa & El-Din, 2019). Although there are finding in the literature such as DNR decision may negatively affect the patient’s care, thoughts of the nurses participating in this study is care of the patient should be continued even if there is a DNR decision that is considered as a positive result in terms of professional responsibility.
The greatest challenge of DNR orders for healthcare professionals is that they also participate in DNR decisions about their own family members. Turkish culture is collectivistic, mainly influenced by the Islamic religion, and family makes decision at the end of life for patients (Beaty, 2015). Most of our participants were hesitant about making DNR decisions for their family members. Similar to our results Gouda et al. (2018) found that healthcare professionals who had difficulty making DNR decisions for their family members stated that they would like DNR decisions to be made for themselves. Nurses want the patient’s family to participate in the DNR decision, but they are not willing to participate in this decision for their family. The reason for this situation can be explained by the feeling of fear, such as losing their relatives, separating from their relatives, and not being able to see their loved ones again. In addition, not having encountered this emotion nor even thinking about it before can influence the decision. However, it must be demanded by the patients who are cared for, for reasons such as asking their relatives to participate in the decision, respecting the autonomy of the patient, not causing harm and additional suffering, and potential benefits outweighing the potential burden (Aacharya & Maharjan, 2014; Fritz et al., 2017). Wherever in the world, it is difficult for people to make decisions about the end of life like DNR on behalf of their loved ones.
Limitation
People’s opinions on DNR are based on religious beliefs, cultural values, and laws. Therefore we cannot generalize the results.
Conclusion
The results show that most of nurses have positive attitudes towards DNR orders although it is not legal. DNR orders are affected by numerous legal, cultural, and personal factors and should be addressed by healthcare professionals and lawyers from different perspectives. Also, legal regulations and ethical principles should be established to avoid ethical dilemmas. Patients and their family members, physicians, nurses, managers, and policy makers should be provided with comprehensive training to systematize and manage DNR decision-making processes. We believe that our results will contribute to the preparation of procedures, for the implementation of DNR orders especially in the countries where DNR order is not common or legal. Future studies are needed to better understand family members’ and decision makers’ perceptions of DNR orders for patients.
Supplemental Material
sj-pdf-1-ome-10.1177_0030222820969317 - Supplemental material for Nurses’ Opinions on Do-Not-Resuscitate Orders
Supplemental material, sj-pdf-1-ome-10.1177_0030222820969317 for Nurses’ Opinions on Do-Not-Resuscitate Orders by Şenay Gül, Gülcan Bağcivan and Miray Aksu in OMEGA-Journal of Death and Dying
Footnotes
Acknowledgments
We would like to thank all the nurses who participated in the study.
Ethical Approval
This study was approved by the Ethics Board of Koc University (2019.035.IRB.3.018). A consent form was sent to participant with the survey and participant were asked to sign the consent prior to participation.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.