
Abstract
This study aimed to determine the relationship between self-care agency and death anxiety among elderly individuals. The study sample consisted of 163 elderly individuals who applied to the internal medicine and chest diseases outpatient clinic of a university hospital. Death anxiety (DAS) and Self-care agency (SCAS) scales were used for data collection. The mean DAS score of the participants was found 6.76 ± 3.25 and low. The mean SCAS scores was 94.35 ± 16.37 and moderate. A positive very weak correlation was found between self-care agency and death anxiety (p = 0.044, r = 0.158). Elderly individuals without regular income had higher levels of death anxiety compared to those with regular income (p < 0.05). A significant difference was found in death anxiety levels with respect to the sex and marital status (p < 0.05). The low-level death anxiety on elderly individuals may have a positive effect on maintaining their self-care agency. Nurses should engage in training activities and interventions to increase the levels of self-care agency and determine the death anxiety among elderly individuals.
Introduction
With the prolonged life expectancy, the proportion of the elderly population in the total population has increased. Moreover, aging has become an important health issue, which has influenced social policies worldwide (Karahan & Hamarta, 2019). The World Health Organization’s successful approach to aging envisages a safe, healthy, and socially active life. To be able to discuss about an elderly population with a good quality of life, all aspects of old age need to be investigated and evaluated (Demir, 2020; World Health Organization, 2017).
An important problem of old age is the presences of chronic diseases, which are various pathophysiological conditions with no sudden onset; these diseases do not often result in full recovery, requiring long-term treatment and care (Gorman, 2014). Individuals with chronic disease have higher death anxiety levels than individuals without chronic disease (Karahan & Hamarta, 2019). Studies show that individuals feel closer to death owing to the physiological and psychological changes that occur with aging and in the last period of life, respectively, and as death anxiety levels increase, the chances of elderly individuals living a harmonious life decrease (Adelirad et al., 2021; Assari & Lankaran, 2016; Erdoğdu & Özkan, 2007; Öztürk et al., 2011; Suhail & Akram, 2002). Death anxiety in elderly individuals is closely associated with their health status. Factors affecting death anxiety include the presence of chronic diseases, sex, physical health, and religious and cultural beliefs (Tang et al., 2002)
Self-care agency is defined as ‘‘an individual’s ability and willingness to participate in self-care, which is known to affect self-care behaviors’’ (Orem 1991). Self-care agency is associated with self-care status among individuals with chronic diseases (Çiftçi et al., 2015). There is a negative correlation between self-care agency and depression (Işık et al., 2020), and the level of death anxiety increases with that of death-related depression (Kurt Magrebi & Akçay, 2020). Enabling self-care is considered a fundamental component in the management of chronic diseases (Le Roy et al., 2014). Helping individuals develop self-care skills is an important role played by nurses. Nurses should be aware of the self-care agency levels of patients and the factors affecting these levels to plan the most appropriate care program for patients and to support self-care agency among elderly individuals with chronic diseases.
This research was conducted with the aims of (a) determining death anxiety levels and factors affecting them, (b) determining self-care agency levels and factors affecting them, and (c) determining the relationship between self-care agency and death anxiety among elderly individuals with chronic diseases.
Materials and Methods
Type of Study
This study was designed as a descriptive and correlational study.
Study Site
The study was performed in the internal and chest diseases outpatient clinic of a university hospital in Turkey.
Study Population and Sample Size
The study population consisted of individuals aged ≥ 65 years with at least one chronic disease who presented to the internal and chest diseases outpatient clinic of a University Hospital for treatment. The study sample included 163 individuals who met the inclusion criteria and agreed to participate in the study.
The G-power 3.1.9.2 program was used to calculate the sample size (Faul et al., 2009). Sample-size calculation was based on Kurt Magrebi and Akçay (2020)’s study examining death anxiety and death-related depression levels among nursing home residents, which reported the correlation between death anxiety and age as r = 0.30. In the reference study, the effect size and power were not presented, and the sample size was not calculated (Kurt Magrebi & Akçay, 2020). Therefore, it was deemed appropriate to increase the sample size. The literature recommends increasing the sample size by at least 15% for possible losses (Yıldırım Kaptanoğlu, 2013) therefore, the sample size was increased by 40% in the present study. A total of 48 individuals were added to the calculated number, and the sample size was determined to be at least 163 individuals with a margin of error of 0.05% and 95% power.
Inclusion Criteria
Presenting to the relevant outpatient clinic, being ≥ 65 years of age as of the date of the research, having at least one chronic disease, and agreeing to participate in the research.
Exclusion Criteria
Patients with a diagnosed or reported psychological problem (depression and suicidal tendencies, among others) and those who lost a first-degree relative in the previous year were excluded from the study.
Data Collection Techniques and Tools
The data were collected using “Elderly Information Form (EIF),” “Death Anxiety Scale (DAS),” and “Self-Care Agency Scale (SCAS).”
Elderly Information Form
The form contains questions regarding the socio-demographic characteristics of elderly individuals.
Death Anxiety Scale
DAS was developed by Templer (1970) and adapted to Turkish by Şenol (1989), who included elderly patients in his study. Akça and Köse (2008) conducted a second validity and reliability study to further develop the scale by including different groups of individuals. The scale consists of 15 items, which are binary Likert-type questions (Correct/Incorrect). Correct answers are scored 1 point, whereas wrong answers receive 0 points. While scoring, items 1, 4 and 8-14 are scored as correct and the others as incorrect. Each score obtained is coded as 1, and if the total score 7 or more, it indicates the presence of death anxiety in the elderly individual. The score that can be obtained ranges between 0 and 15 (minimum = 0 points; maximum = 15 points). Higher score indicates higher levels of death anxiety whereas a lower score indicates low death anxiety. The Cronbach’s alpha coefficient of the scale was calculated as 0.79 (Akça & Köse, 2008). In the present study the Cronbach’s alpha coefficient was 0.74.
Self Care Agency Scale
SCAS was developed by Kearney and Fleischer (1979), and the study on the validity and reliability of the Turkish version of the scale was conducted by Nahcıvan (Nahcivan, 1994; Nahcıvan, 2004). SCAS is a self-report scale in which individuals evaluate their ability or power to perform self-care actions. The scale consists of 35 items scored using a 5-point Likert-type scale. Each statement is scored from 0 to 4: 4, “defines me a lot;” 3, “defines me somewhat;” 2, “I have no idea;” 1, “defines me little;” and 0, “does not define me at all.” A total of 8 items of the scale (items 3, 6, 9, 13, 19, 22, 26, and 31) are coded in reverse. The maximum score that can be obtained is 140. Cronbach’s alpha coefficient of the scale was calculated as 0.89. In the present study the Cronbach’s alpha coefficient was 0.87.
Data Collection
Data were collected between December 2021 and January 2022 through face-to-face interviews. Data collection lasted approximately 10–15 minutes for each individual. Owing to the coronavirus disease-19 pandemic, the interviews were carried out with precautionary measures in place, such as wearing masks and maintaining social distance.
Ethical Considerations
Ethics approval was obtained before initiating the research. (App. No: 2021/16-104, Date: 01.12.2021). Institutional permission has been obtained from the relevant hospital (Number: E-14567952-900-125620, Date: 07.12.2021). Oral and written informed consent was obtained from the participants. The research was carried out according to the principles of the Declaration of Helsinki.
Statistical Analysis
The data was analyzed using the Statistical Package for Social Science 22.0 program (Chicago, USA). Descriptive data were presented as percentage, mean, standard deviation, and minimum and maximum values. Kolmogorov–Smirnov and Shapiro–Wilk tests were used to assess whether the data conformed to a normal distribution. One-way analysis of variance, independent samples t test, Mann-Whitney U, Kruskall-Wallis test were used to analyze the data. The relationship between the scale scores was investigated using Pearson’s and Spearman correlation analysis. Values of p < 0.05 were accepted as statistically significant in all the analyses.
Results
The descriptive characteristics of the patients (N = 163).

HT: Hypertension DM: Diabetes mellitus CAD: Coronary artery disease COPD: Chronic obstructive pulmonary disease.
SCAS and DAS total scores according to the descriptive characteristics of the patients.
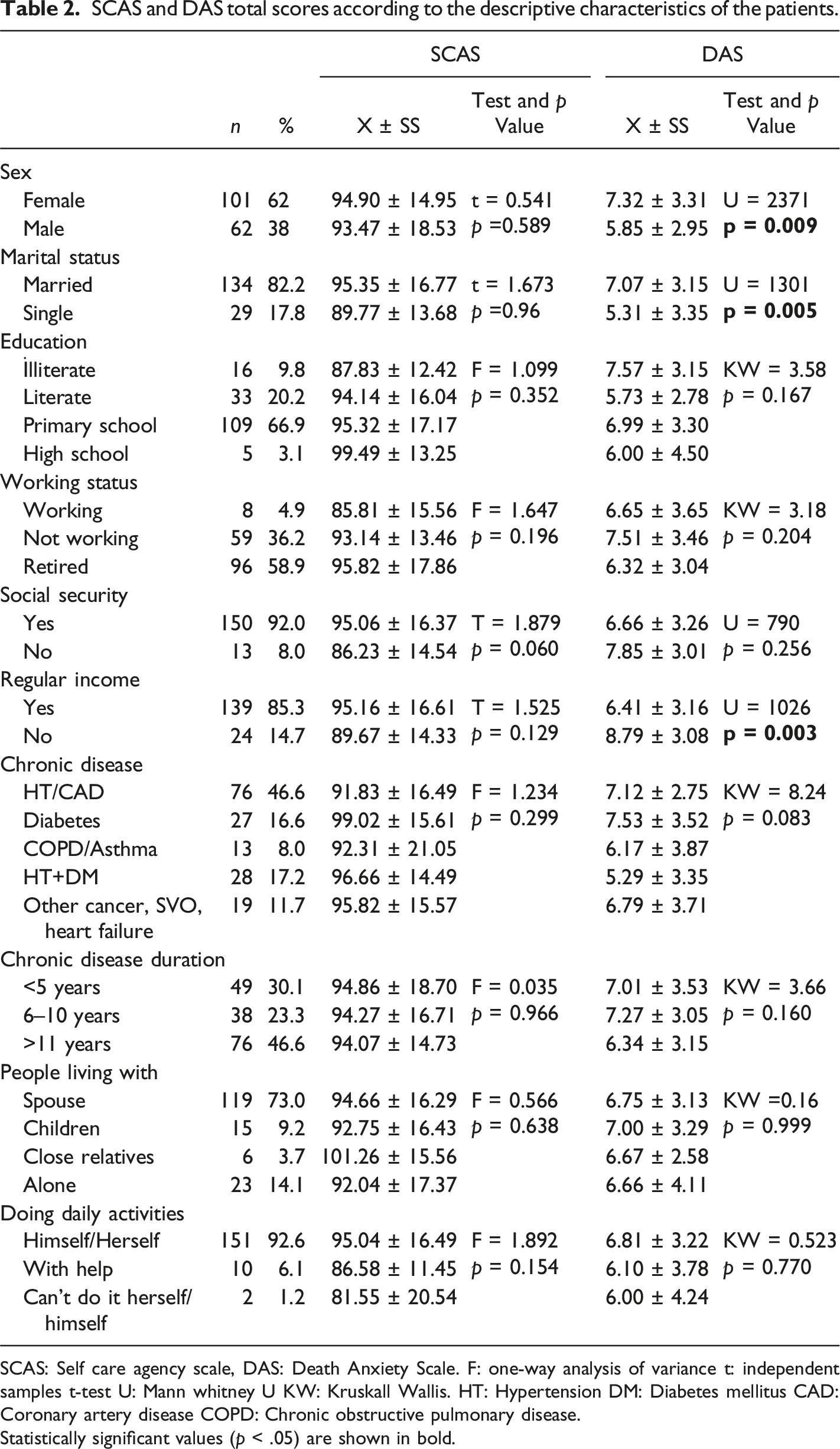
SCAS: Self care agency scale, DAS: Death Anxiety Scale. F: one-way analysis of variance t: independent samples t-test U: Mann whitney U KW: Kruskall Wallis. HT: Hypertension DM: Diabetes mellitus CAD: Coronary artery disease COPD: Chronic obstructive pulmonary disease.
Statistically significant values (p < .05) are shown in bold.
SCAS and DAS total scores of participants.
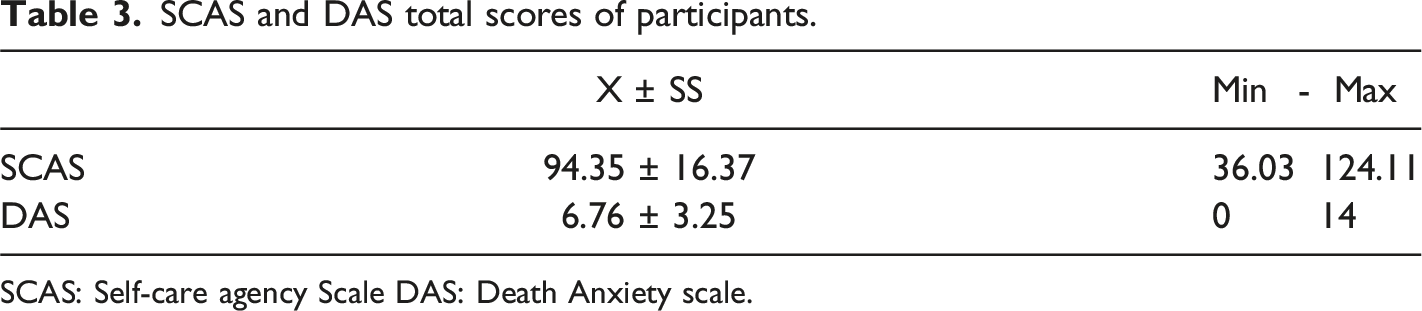
SCAS: Self-care agency Scale DAS: Death Anxiety scale.
Correlation between age, SCAS, DAS total scores.
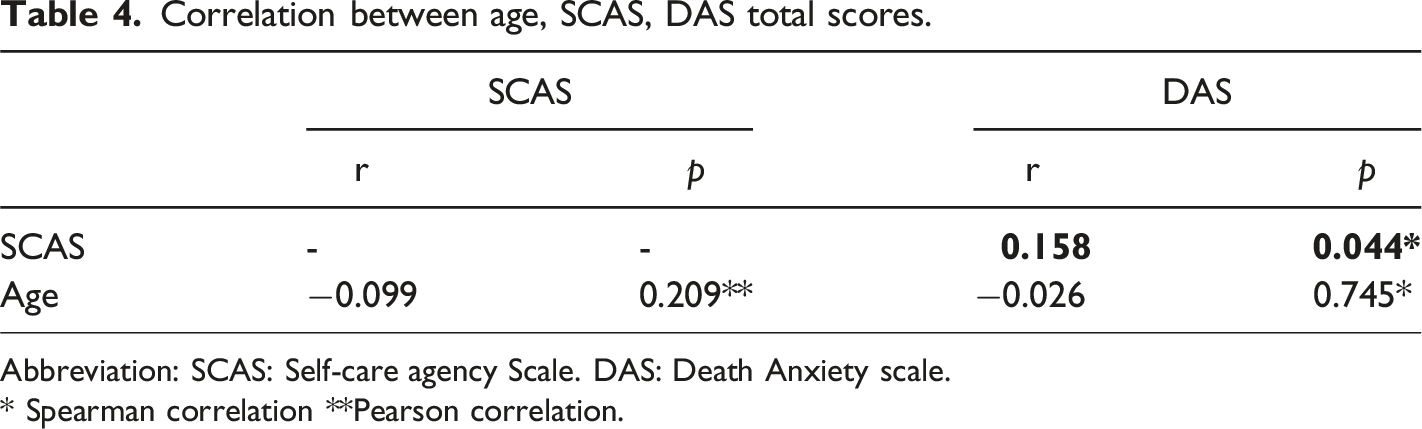
Abbreviation: SCAS: Self-care agency Scale. DAS: Death Anxiety scale.
* Spearman correlation **Pearson correlation.
Discussion
Death anxiety is a feeling experienced since birth. It lasts a lifetime, underlies all other fears, and its levels increase after one becomes aware that one will no longer exist, may lose oneself and the world, and may become nothing (Ayten, 2009). Although the concept of death is natural and acceptable, it is frightening and worrisome for many people (Wysokiński et al., 2019). Death anxiety levels increase with age (Sayın Kasar et al., 2016). In the present study, the mean DAS scores of the participants was 6.76 ± 3.25. The death anxiety level of individuals >65 years of age was reported as 7.73 ± 2.63 (Sayın Kasar et al., 2016). In another study, it was reported that the majority of elderly participants (48.9%) had moderate death anxiety levels (5.61 ± 3.07) (Köstek, 2015). There are also studies in the literature reporting that elderly individuals have low levels of death anxiety (Kutlu et al., 2021; Sinoff, 2017).
Death anxiety has been associated with many socio-demographic characteristics, such as sex, marital status, education, income level, and age. In the present study, a significant difference was found in DAS scores according to the sex, marital status and income level. Consistent with our findings, it is reported that women have higher death anxiety levels than men (Kutlu et al., 2021). However other studies in the literature also did not demonstrate any significant relationship between sex and death anxiety (Bayrak et al., 2019). Married individuals had higher death anxiety in the present study. Although it was reported that marital status was not a factor associated with death anxiety (Bayrak et al., 2019; Demir, 2020; Köstek, 2015), some studies reported that divorced elderly individuals had higher death anxiety levels (Pei et al., 2022; Tel et al., 2020).
In the present study, no significant relationship was found between educational status and death anxiety; other studies in the literature also supported our findings (Bayrak et al., 2019; Demir, 2020). In contrast, some studies reported that death anxiety decreases as the educational status of elderly individuals increases (Tel et al., 2020). Further, studies have reported that death anxiety is associated with educational status in men (Adelırad, 2021). Educational status is an important factor influencing the development of chronic diseases, drug use, proper nutrition, and healthy living habits.
In the present study, elderly individuals without regular income had significantly higher death anxiety levels compared to those with regular income (p < 0.05). Some studies reported that income level did not influence death anxiety levels (Bayrak et al., 2019; Demir, 2020). In contrast, other studies indicated that those with low and middle income levels experienced higher levels of death anxiety (Soleimani et al., 2020). The economic status of individuals is one of the important factors affecting living standards. In the present study, there is no significant difference between DAS scores and type of chronic disease. Individuals with heart disease have higher death anxiety compared to those without (Kaçan-Softa et al., 2011). The course of the disease, the lack of recovery despite treatment, the desperation that comes with the process, the experiences of severe pain, and personal thoughts about death can cause death anxiety in individuals with life-threatening diseases (Öztürk et al., 2011).
Self-care agency is an important parameter that brings meaning to life among older individuals. The SCAS score of the participants was 94.35 ± 16.37, and their self-care agency was at a moderate level. One study reported that self-care agency is high in individuals with cancer, a chronic disease (O’Regan et al., 2019). Moreover, it was reported that 84.3% of home-dwelling elderly individuals had a moderate and above self-care agency (Dale et al., 2012). The self-care agency score of elderly individuals was reported as 82.68 ± 16.39 (Karagözlü et al., 2012). In a study on elderly individuals in Japan, the self-care agency levels of physically active individuals were found to be significantly higher (Yoshimura et al., 2021). Having higher self-care agency levels improves the self-management capability of individuals in chronic diseases (Sousa et al., 2010). At the same time, high levels of self-care agency protect elderly individuals from depression (Tanimura et al., 2018). Education, physical exercise, and motivational practices that can increase the self-care agency levels of elderly individuals should be promoted by nurses.
In the present study, no significant relationship was identified between the descriptive characteristics of individuals and self-care agency. Studies report that women have higher self-care agency levels than man (Tanimura et al., 2018; Şahin Yıldız & Karaman Özlü 2021). In the present study, no significant relationship was found between educational status and self-care agency. However, there are studies in the literature reporting that patients' self-care behaviors are affected by their educational level (Şahin Yıldız & Karaman Özlü., 2021). Uğurlu et al. (2010) also found that self-care agency levels increased significantly as educational status increased. This may be attributable to the fact that individuals with higher educational status exhibit more self-care behaviors as they apply the information they obtain about their diseases more easily and have better social status and financial opportunities.
In the present study, no significant relationship was found between income status and self-care agency. In contrast, a previous study reported that individuals without income had the lowest level of self-care agency, whereas individuals whose income was higher than their expenses had the highest level of self-care agency (Uğurlu et al., 2010). Aging is a period of life that brings with it many physical, spiritual, and social problems, including a decrease in income level, independence, productivity, and social support (Kaçan-Softa et al., 2011). Decreased physical capacity with aging, changes in psychomotor structure and adaptation skills lead to limitations in independence and decreased functionality. Owing to increasing chronic and physical diseases, elderly individuals have difficulty performing daily life activities (Karakuş, 2012). A total of 46% of the individuals who participated in the present study had at least one chronic disease for >11 years. Studies report that 60%–70% of elderly individuals in Turkey have at least one chronic disease (Kutsal, 2006; Vatan & Gençöz, 2006). There is no significant relationship between the type and presence of chronic disease and self-care agency in the present study. However, it was reported that individuals with more than one chronic disease have lower levels of self-care agency (Gelik, 2019).
In the present study, there is no significant relationship between age and death anxiety and self-care agency. Some studies in the literature evaluating the relationship between age and death anxiety found no relationship (Demir, 2020; Köstek, 2015), whereas other studies identified a negative relationship between the two (Soleimani et al., 2020). Elderly individuals feel closer to death. Although some elderly individuals wait peacefully, accepting death, some want to live longer (Ertufan, 2008). Elderly individuals do not have the chance to postpone their death. The attitude of elderly individuals who do not have the ability to postpone death can manifest in the form of surrender or complete denial. In the literature examining the relationship between age and self-care agency reported a positive correlation (Gündoğan Gelik, 2019), negative correlation (Dale, 2012), or no significant correlation (Şahin Yıldız & Karaman Özlü, 2021).
The most important finding of the present study is the presence of a positive very weak correlation between death anxiety and self-care agency. Participants have low death anxiety. The low-level death anxiety on elderly individuals may have a positive effect on maintaining their self-care agency. Self-care agency is considered as one of the important factors affecting healthy and active aging (Demirtaş et al., 2017; Ferri et al., 2009). Individuals with better self-care agency have a better quality of life and perform better in terms of the management of chronic diseases (Altıparmak et al., 2011; Hançerlioğlu & Aykar 2018). There are no studies in the literature examining the relationship between death anxiety and self-care agency among elderly individuals with chronic diseases. Therefore, the results of the present study will guide further research on this subject.
Limitations of the Study
Data was collected from a single center; therefore, research results cannot be generalized to the entire population.
Conclusion and Recommendations
In the present study, the participants had moderate self-care agency levels. Their DAS total score was 6.76 ± 3.25 and low. A positive very weak correlation was found between death anxiety and self-care agency among participants. The low-level death anxiety on elderly individuals may have a positive effect on maintaining their self-care agency. Nurses play a role in assisting elderly individuals with chronic diseases by determining their self-care needs and helping them attain a level of function where they can independently perform self-care. In this context, our recommendations are: ➢ For healthy aging, elderly individuals should develop appropriate behaviors to deal with death anxiety, and necessary measures should be taken to improve their lives. ➢ Self-care agency is a skill gained gradually by an individual by regulating the internal and external conditions. It is influenced by the interests and limitations of the individual. Therefore, health professionals should focus on the abilities and skills of patients, encourage the patients, and provide training. ➢ Governments should develop projects in this regard as increasing the levels of self-care agency among elderly individuals with chronic diseases will reduce the cost of care. ➢ Although death is often an undesirable issue to talk about, death anxiety must be addressed when planning nursing care for elderly individuals with chronic diseases.
Footnotes
Acknowledgments
We would like to thank all the participants.
Author Contributions
Idea/Concept: SB, HT, HA, Design: SB, HTP, Data Collection/Processing: SB, HTP, HA, Analysis/Interpretation: SB, HTP, Literature Review: SB, HTP, HA, Drafting/Writing: SB, HTP, Critical Review: SB
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Committee Approval
Ethics committee approval was obtained before starting the study (App. No:2021/16-104, Date:01.12.2021). Institutional permissions were obtained from the relevant University (Number: E-14567952-900-125620, Date:07.12.2021). Participants' verbal and written consents were obtained. The research was carried out per the principles of the Declaration of Helsinki.
Informed Consent
Oral and written informed consent was obtained from the participants.