
Abstract
This multiple case study analysis describes the immediate effects on speech fluency of transcutaneous electrical nerve stimulation (TENS) applied to participants with persistent stuttering and concomitant orofacial disorders. Study participants were 14 adolescents and adults who stuttered and had jaw clenching bruxism or mouth breathing. Participants experienced low-frequency TENS applied at mild motor level for 20 minutes with electrodes placed at the lower third of the face (Area A), submandibular region (Area B), posterior neck (Area C), or shoulder girdle (Area D), with speech fluency assessed immediately before and after each stimulation.For participants with stuttering and bruxism, AB stimulation reduced the median frequency of syllables stuttered by 27% and reduced the median duration of the three highest stuttering moments by 29%. In addition, for participants with stuttering and mouth breathing, CD stimulation reduced the median duration of the three highest stuttering moments by 28% and increased their median speech rate by 113%. As a single session of TENS may help participants with stuttering and concomitant orofacial disorders better use fluency shaping techniques, the therapeutic potential of TENS for treating stuttering should be further investigated.
Stuttering is a speech fluency disorder that usually begins in childhood (Smith & Weber, 2017). Individuals who stutter repeatedly experience involuntary speech disruptions during which they may produce part-word or one-syllable repetitions, sound prolongations or blocks, usually occurring at the first syllable of words (Blomgren, 2013; Smith & Weber, 2017). Persistent stuttering affects approximately 1% of the adult population with a sex ratio of four males for each female (Blomgren, 2013; Smith & Weber, 2017). Persistent stuttering can be managed with behavioral speech therapy (Blomgren, 2013) and pharmacological treatment (Stager et al., 2005).
An established behavioral approach for treating persistent stuttering is fluency shaping. The most common first technique of fluency shaping is to reduce speech rate by instructing patients to increase speech–sound duration (Blomgren, 2013). The second technique is to foster smooth speech by having patients produce gentle movements while speaking (Blomgren, 2013). However, a concern addressed in the present study is that fluency shaping techniques may be more difficult for people who both stutter and present a concomitant orofacial disorder such as bruxism or mouth breathing. Concomitant orofacial disorders change the isometric tension of face and neck muscles (see, e.g., Gelhaye et al., 2006 and Grünheid et al., 2009), creating difficulties for voluntary control of these muscles during speech.
Bruxism is an oral motor disorder characterized by repetitive jaw muscle activity mainly involving clenching or grinding the teeth (Lobbezoo et al., 2013). In jaw clenching bruxism, subjects have an extended tooth contact (Lobbezoo et al., 2013), which increases the isometric tension of jaw muscles (Grünheid et al., 2009). Dental wear, fatigue or pain in jaw muscles, and headache are common consequences of bruxism (Guaita & Högl, 2016). Although we found no research reporting the concomitant occurrence of stuttering and bruxism, this association may not be marginal. As both stuttering and bruxism may be considered movement disorders, basal ganglia dysfunction has been identified in both conditions (e.g., Alm, 2004 for stuttering, and Lobbezoo & Naeije, 2001 for bruxism). Second, jaw clenching bruxism frequently occurs in individuals with anxiety disorders (Guaita & Högl, 2016), and previous research has also suggested that individuals with persistent stuttering are more prone to social anxiety disorder (Iverach & Rapee, 2014). In fact, up to one-third of adults who stutter show symptoms compatible with social anxiety disorder (Iverach et al., 2018). Third, jaw clenching bruxism may also be a secondary side effect of psychiatric medication, such as selective serotonin reuptake inhibitors and neuroleptics (Guaita & Högl, 2016) sometimes used in pharmacological treatment for stuttering (Stager et al., 2005). Considering these factors, the incidence of jaw clenching bruxism may be significant among individuals with persistent stuttering. This association may be relevant to treatment, because increased jaw muscle tension caused by jaw clenching bruxism may, in turn, create difficulties in using fluency shaping techniques as a stuttering intervention. Jaw clenching bruxism may restrict the mouth opening during speech, presenting an obstacle to the production of wider movements needed to reduce speech rate. The increased jaw muscle tension may also be a barrier to voluntarily producing gentle movements in order to smooth speech.
Mouth breathing occurs when some condition significantly impairs nasal breathing, such as allergic rhinitis (Paul-Brown, 2004). If nasal obstruction is constant, breathing at rest may always be performed through the mouth (i.e., persistent oral breathing). On the other hand, if nasal obstruction is not constant, breathing at rest may be performed sometimes through the nose and sometimes through the mouth (i.e., intermittent mouth breathing). The lowered position of the jaw during mouth breathing changes the tongue position so as to move the tongue more posteriorly in the mouth cavity, decreasing the nasopharyngeal diameter. To increase the nasopharyngeal diameter for easier breathing, individuals with mouth breathing move the head forward (Cuccia et al., 2008). Indeed, previous research has shown that adults with mouth breathing since childhood have a forward leaning head posture compared with control adults without mouth breathing histories (Milanesi et al., 2011). Keeping the head in a forward position elicits a stronger contraction of the muscles in the lateral and the posterior neck, increasing the isometric tension of these muscles (Milanesi et al., 2011; Singla & Veqar, 2017). Thus, unlike individuals with jaw clenching bruxism, persons with chronic mouth breathing do not have increased jaw muscle tension, but, rather, decreased jaw muscle tension (Gelhaye et al., 2006). It is possible that the decreased jaw muscle tension (due to open mouth posture) and the greater stretching of these muscles (due to forward head posture) also creates difficulties for these patients’ voluntary muscle control during speech fluency shaping techniques for stuttering. While, in our practice, it has been common for people who stutter to also have intermittent or persistent mouth breathing due to allergic rhinitis, we found no prior research reporting the concomitant occurrence of stuttering and mouth breathing. Allergic rhinitis is characterized by inflammation of the nasal mucous membrane caused by an immune system response (Wise et al., 2018). Our patients live in an urban area with high levels of air pollution (Abe & Miraglia, 2016), perhaps increasing their likelihood of developing allergic and respiratory disorders (Patella et al., 2018) and mouth breathing.
In this study, we applied transcutaneous electrical nerve stimulation (TENS) to stimulate tense muscles in participants with persistent stuttering who also present jaw clenching bruxism or mouth breathing. TENS is a type of surface electrical stimulation (SES) that can be applied to treat neurological and motor conditions (Robinson & Snyder-Mackler, 2010). If TENS is adjusted to stimulate only afferent nerve fibers (i.e., sensory level), it may be applied for improving touch and pressure sensibility or treating acute pain (Robinson & Snyder-Mackler, 2010; Schuhfried et al., 2012). On the other hand, if TENS is adjusted to stimulate afferent and efferent nerve fibers (i.e., motor level), it may be applied for improving touch and pressure sensibility, reducing isometric muscle tension, or treating chronic pain (Robinson & Snyder-Mackler, 2010).
SES has gained popularity for treating speech–language pathology in the last few years. There are studies on voice disorders and dysphagia (e.g., see reviews by Gilman & Gilman, 2008; Miller et al., 2013). Relevant references for treating speech fluency include Remak (1858) and Tomazzetti (2004). Robert Remak (1858), a neurologist, applied SES to treat several conditions, such as muscle atrophy, tremor, writer’s cramp, and stuttering. He declared that it was possible to achieve significant improvements from stuttering with SES, applying direct current for some minutes at the neuromuscular junction in selected muscles; however, details of his technique are unknown. Tomazzetti (2004) used high-frequency (100 Hz) and high-intensity (the highest subjects could tolerate) TENS in combination with behavioral speech therapy to treat three adults with persistent stuttering. Sessions were 45 minutes long: 15 minutes for TENS followed by 30 minutes for behavioral speech therapy. During TENS, two muscle pairs were stimulated at the same time: first the orbicularis oris and the masseter, then, the buccinator and the mentalis, and finally, the sternocleidomastoid and upper trapezius. During speech therapy, several behavioral techniques were applied, such as identification of stuttering moments, eye-contact maintenance, and smooth speech. After 20 sessions, speech fluency improved in two participants and worsened in one. Although these two studies applied SES for treating stuttering and had some success, the broad utility of SES for stuttering treatment remains to be established.
The present study strove to evaluate the immediate effects of TENS on speech fluency for participants with both persistent stuttering and concomitant orofacial disorders. We hypothesized that low-frequency, mild motor level TENS would reduce isometric tension of jaw muscles (for participants with jaw clenching bruxism) and posterior neck muscles (for participants with mouth breathing), helping both participant groups utilize speech fluency shaping techniques to improve stuttering.
Method
Participants
Research participants for this study were 14 people with persistent stuttering (see Table 1). Eleven were male and three were female. Participants were adolescents and adults aged 13–38 years. All were native speakers of Brazilian Portuguese, spontaneously sought speech therapy due to stuttering, and all have been treated by the author using a comprehensive behavioral speech therapy approach over a period of several months (cf. Blomgren, 2013).
Participants’ Gender, Age, Speech Fluency, and Orofacial Disorders.

General inclusion criteria for this study included being an adolescent or adult (i.e., ages from 13 to 64 years), being in behavioral speech therapy for persistent stuttering for at least 6 months (a time period considered necessary to learn speech fluency techniques), and presenting concomitant jaw clenching bruxism or mouth breathing. Exclusion criteria included presentations of (a) very mild stuttering (in those cases, the frequency of stuttered syllables may fall within normal values), both jaw clenching bruxism and mouth breathing (this would place the participant in both groups, causing a bias in the statistical analysis); (b) only jaw grinding bruxism (with no jaw clenching bruxism); and/or (c) increased muscle tension in the neck and shoulder girdle for reasons other than mouth breathing (such as orthopedic issues).
Table 1 shows the participants’ frequency of stuttered syllables and speech rate in spontaneous speech immediately before the first TENS session. All participants presented a frequency of stuttered syllables that was superior to the general reference value for their respective age and gender among Brazilian Portuguese speakers without speech fluency disorders (cf. Andrade, 2006). Some participants presented speech rates below the reference values (Participants 1, 2, 6, 13, and 14), some were within the reference values (Participants 3, 4, 5, 7, 10, 11, and 12), and still others were above the reference values (Participants 8 and 9). Although the participants may have presented concomitant facial behaviors during stuttering moments (such as eye closure or facial tension), those behaviors were not analyzed in this study.
Table 1 also shows the participants’ concomitant orofacial disorders, with seven presenting jaw clenching bruxism and seven presenting mouth breathing (intermittent or persistent). During speech therapy, participants were screened for orofacial disorders. In the case of jaw clenching bruxism, participants were asked if they held their teeth together when awake or sleeping, or if they felt tension and fatigue in their jaw muscles. Those who answered positively were referred to their personal dentist, and the first seven participants in Table 1 were diagnosed with probable jaw clenching bruxism (cf. Lobbezoo et al., 2013), meaning that positive bruxism symptoms were found during clinical examination, including a rigid masseter muscle at palpation, pain in jaw muscles at palpation, or dental wear. Participants with no dental wear were usually instructed by their dentists to voluntarily keep teeth apart, avoid caffeine, and manage stress. For those presenting dental wear, dentists provided an acrylic or soft splint. In the case of mouth breathing, participants were observed for signals of impaired nasal breathing, such as decreased nasal resonance when speaking, incompetent lip seal, and forward head posture. They were also asked if they usually breathed through the nose or through the mouth, and if they had an upper airway disorder. Those with impaired nasal breathing were referred to their personal ear, nose, and throat physician when they were not already receiving medical care for this condition. The second seven participants in Table 1 were diagnosed with allergic rhinitis, meaning that they presented with the three cardinal symptoms of this disorder—nasal obstruction, mucous discharge, and sneezing (cf. Wise et al., 2018). All seven were administered flexible nasendoscopy in order to assess the upper airway, and their allergic rhinitis was treated with saline solution and medication.
Participants declared not to present any restraint for TENS (such as skin lesions, epilepsy, or heart disorder; Johnson et al., 2015). All participants or parents of participants (in the case of minors below the age of 18 years) signed an informed consent form authorizing the use of their data.
TENS
A transcutaneous neurostimulator (Ibramed Neurodyn II, Sao Paulo, Brazil) was used to provide electric current stimulation, configured as described here. TENS was the selected operating mode. The neurostimulator produces a rectangular-shaped alternating current, with balanced phases. At the mild motor level, TENS can be applied for improving touch or pressure sensibility and reducing isometric muscle tension (Robinson & Snyder-Mackler, 2010). Alternating current was chosen, because there was no need for polarity effects and because it minimizes the chances of chemical burns on the skin (Robinson & Snyder-Mackler, 2010). Discharge frequency was set at 10 Hz, because this frequency activates type I muscle fibers (Pette & Staron, 2000), which produce smaller isometric tension (Guyton & Hall, 1996; Pette & Staron, 2000). Wave duration was set to 300 µs. This value fitted both the small size of the electrodes used in this study and the desired intensity range (Robinson & Snyder-Mackler, 2010). The intensity of the current had to be enough for producing mild and comfortable muscle contractions. Each participant was free to choose their comfortable intensity. The intensity of the electric current was measured in milliamperes (mA). Time of stimulation was set at 20 minutes, consistent with Schuhfried et al. (2012) who suggested a stimulation time from 10-30 minutes. An intermediate value was chosen because 10 minutes could be insufficient to produce immediate effects, and 30 minutes could lead to muscle fatigue.
As depicted in Figures 1 and 2, four muscle regions were selected for stimulation (cf. Staubesand, 1988): (a) Area A was the region associated with the lower third of the face (Figure 1), with electrodes over the masseter muscle. The stimulation of the masseter muscle on the right and left sides also stimulated other muscles in the lower third of the face, such as the buccinator and orbicularis oris; (b) Area B was the submandibular region (Figure 1), with electrodes over the suprahyoid muscles; (c) Area C was the posterior region of the neck (Figure 2), with electrodes over the upper trapezius; and (d) Area D was the shoulder girdle (Figure 2), with electrodes over the trapezius.

Electrode Placement in the Lower Third of the Face and Submandibular Region.
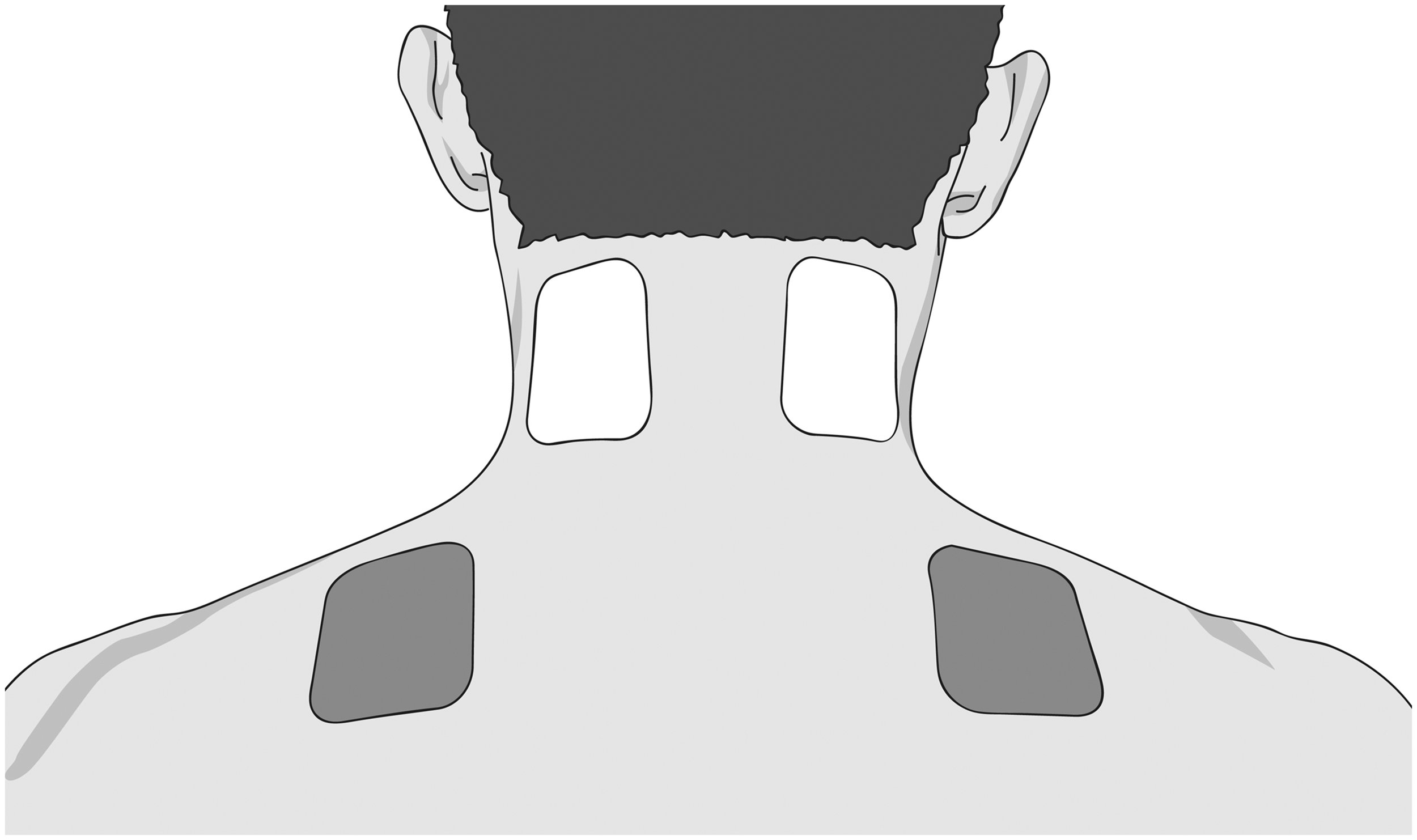
Electrode Placement in the Posterior Neck and Shoulder Girdle.
After the skin was cleaned with soap and water, adhesive electrodes (Spes Medica, Genova, Italy) were applied to the desired muscles. For the lower third of the face and the submandibular region, 3.5 × 3.5 cm electrodes were used. For the posterior neck and shoulder girdle, 4.5 × 5.0 cm electrodes were used.
Speech Data
A cardioid dynamic microphone (Shure SM48) was connected to a digital audio interface (M-Audio Mobile Pre USB) that was plugged into a computer. Praat software (Paul Boersma & David Weenink, praat.org) was used for signal acquisition. Sampling rate was set at 32 kHz and bit rate at 64 bits. Professional audio monitors (Edifier 2.0 R1000TC) were used for speech reproduction. The author recorded each participants’ speech data immediately before and after the TENS session. For speech stimuli in the form of the participants’ narrations, the author presented comic strips from Aragones (2002) with a sequence of six drawings containing no written text. Participants were instructed to describe the sequence of events presented by the comic strips, keeping in mind that a hypothetical person unable to see the comic strips should be able to understand the narratives. There were four different comic strips, randomized across AB and CD stimulations. The author then transcribed speech samples and identified stuttered disfluencies according to standards for the Brazilian Portuguese language (Andrade, 2006). The percentage frequency of stuttered syllables was calculated by dividing the number of stuttered syllables by the total number of syllables in the sample and then multiplying by 100 (e.g., 14.3%). Speech rate per minute was calculated by dividing the total number of fluent syllables spoken in the sample by the duration of the whole spoken sample in seconds and multiplying by 60 (e.g., 119 fluent syllables per minute). In addition, the duration of each of the three highest stuttering moments was collected, as these moments most accurately indicate stuttering severity (Maguire, Riley, Franklin & Gottschalk, 2000).Stuttering moments were identified in a transcription layer at Praat software, and speech waveform and sound spectrogram were analyzed to identify the onsets of vowels and consonants in order to determine the time duration of stuttering moments. The duration of the three highest stuttering moments, frequency of stuttered syllables, and speech rate were all utilized in data analyses.
Procedures
Because no participant had previously undergone TENS, all participants had a first session to become familiar with the procedure. Participants were connected to the neurostimulator and received stimulation for 20 minutes. Participants were allowed to try different intensities of muscle contraction, from very mild to intense to ensure that they would be able to choose a mild and comfortable intensity for intervention. Next, participants underwent two TENS trial sessions usually 2 weeks apart (the only exceptions were Participants 2, 8, and 9, who underwent the trial sessions one week apart). Spacing sessions ensured that fluency effects were due to TENS from a single session, rather than from the cumulative effects of shortly spaced sessions and because behavioral speech therapy was interrupted while participants underwent TENS testing. Spacing sessions ensured that fluency changes in the period were due to TENS and not to mixed effects of TENS and behavioral treatment. Participants were randomly assigned for the first stimulation to receive stimulation at either AB or CD regions. In the end, 13 subjects underwent to AB stimulation, and 13 subjects underwent CD stimulation (Participant 7 was not able to do CD stimulation, while Participant 14 was not able to do AB stimulation). On average, one hour was necessary for the whole procedure (i.e., recording speech sample before TENS, preparing the skin and attaching the electrodes, TENS session for 20 minutes, removing the electrodes, recording speech sample after TENS, and subjective report of positive and negative effects).
TENS is considered a safe technique with only minor side effects being reported, such as mild skin burning and itch under the electrodes (Johnson et al., 2015). Participants were examined for skin burning and were asked about any for itching under the electrodes, worsening in fluency, or any other complaints.
Statistical Analysis
The following data were analyzed using descriptive and inferential statistics: frequency of stuttered syllables, duration of the three highest stuttering moments, speech rate, and current intensity. An analysis of the histograms from all variables showed that some of them did not represent normally distributed data. Due to nonnormality, data are presented in terms of the median value for central tendency description and at the 25th and 75th percentiles for dispersion description.
Nonparametric tests were used for inferential statistics. Frequency of stuttered syllables, duration of the three highest moments of stuttering, and speech rate before and after TENS were treated as dependent variables and were compared using Wilcoxon matched pairs test due to equal numbers of data values in comparison groups. Current intensities in the four muscle regions (A, B, C, and D) were treated as independent variables and were compared using Kruskal–Wallis test, and the Mann–Whitney test was applied as post hoc test. For statistical significance, alpha was set at .05.
Results
Speech Fluency
As shown in Table 2, participant data were arranged in two subgroups regarding orofacial disorders (jaw clenching bruxism and mouth breathing) for analysis of AB and CD neurostimulations.
Participants’ Percentages of Stuttered Syllables Before and After TENS Sessions.

Note. Data are median percentages of stuttered syllables relative to uttered syllables during spontaneous speech at three percentile points. Electrode placements: A = lower third of the face, B = submandibular region, C = posterior region of the neck, D = shoulder girdle; TENS = transcutaneous electrical nerve stimulation.
aStatistically significant.
Participants’ Stuttering Length Before and After TENS Sessions.
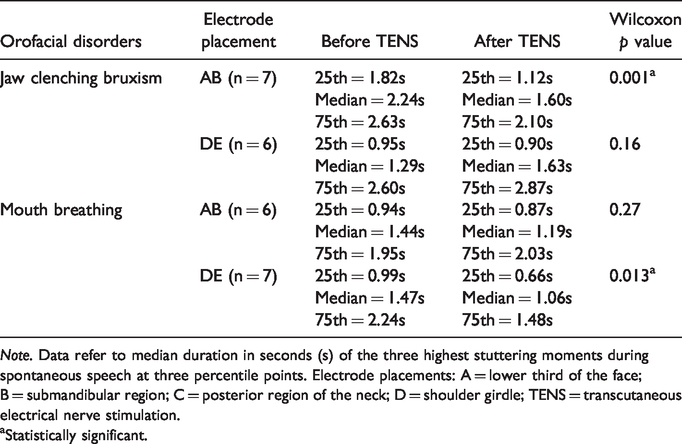
Note. Data refer to median duration in seconds (s) of the three highest stuttering moments during spontaneous speech at three percentile points. Electrode placements: A = lower third of the face; B = submandibular region; C = posterior region of the neck; D = shoulder girdle; TENS = transcutaneous electrical nerve stimulation.
aStatistically significant.
Seven participants had jaw clenching bruxism. Among participants in this group, frequency of stuttered syllables significantly decreased before and after AB stimulation (Z = 2.37, p = .018) such that the median decreased from 8.4% before TENS to 6.1% after TENS. Duration of the three highest stuttering moments also significantly decreased before and after AB stimulation (Z = 3.28, p = .001) such that the median duration decreased from 2.24 seconds before TENS to 1.60 seconds after TENS. Speech rate was not statistically different in pre- and post-TENS for AB stimulation. This group did not show statistically significant pre- and post-TENS differences for CD stimulation on frequency of stuttered syllables, duration of the three highest stuttering moments or speech rate. See Tables 2 to 4 for complete results on jaw clenching bruxism.
Participants’ Speech Rates Before and After TENS Sessions.

Note. Data are numbers of fluent syllables uttered per minute during spontaneous speech at three percentile points. Electrode placements: A = lower third of the face; B = submandibular region; C = posterior region of the neck; D = shoulder girdle; TENS = transcutaneous electrical nerve stimulation.
aStatistically significant.
There were seven participants with mouth breathing. For these participants, there were no differences in pre- and post-TENS frequency of stuttered syllables for CD stimulation. There was a significant pre- and post-TENS decrease in the duration of the three highest stuttering moments for CD stimulation (Z = 2.49, p = .013), with the median value having decreased from 1.47 seconds before TENS to 1.06 seconds after TENS. Speech rate significantly increased after CD stimulation (Z = 2.20, p = .028), with the median value having increased from 207 to 234 syllables per minute. Among this group of mouth breathing participants, there were no significant pre- and post-TENS differences for AB stimulation on frequency of stuttered syllables, duration of the three highest stuttering moments, and speech rate. See Tables 2 to 4 for complete results on mouth breathing. In addition, see Supplementary Table 1 for separate results of each participant in both AB and CD stimulations.
When participants were asked about the condition of their muscles, prior to TENS, several participants reported that it was hard to say if their face, neck, or shoulder girdle were tense or not. However, their awareness of muscle tension changed such that they reported a clear reduction in muscle stiffness and greater joint mobility for opening their mouths or rotating their heads after TENS. When asked immediately after TENS sessions how they evaluated their speech fluency, participants reported fluency improvement. Asked to explain why this happened, some participants reported that they just felt their speech was easier after TENS, though they were doing nothing different. Other participants reported that they were able to reduce speech rate after TENS, because it was easier to engage in a hyperarticulated speech style. Other participants reported that they were able to smooth their speech after TENS. Finally, some participants reported a decrease in covering strategies, such as word substitution and rephrasing. The positive effect of improvement in fluency lasted from 2 to 5 days, according to the participants’ subjective reports.
TENS Intensity
The participant-selected current intensity for TENS at mild motor level varied considerably (from 6 to 35 mA) and was related to which muscles were targeted for neurostimulation. Median intensity for the lower third of the face and the submandibular region was 10 and 13 mA, respectively. Median intensity for the posterior neck and the shoulder girdle was 19 and 20 mA, respectively. Statistical differences among the four regions (n = 52, H = 15.5, p = .0015) and post hoc tests (alpha at .008) revealed that intensity was different regarding the anterior and posterior body regions (i.e., A = B < C = D): for A and B regions, Z = −1.36, p = .17; for A and C regions, Z = −3.23, p = .001; for A and D regions, Z = −2.97, p = .003; for B and C regions, Z = −2.21, p = .03; for B and D regions, Z = −1.92, p = .05; for C and D regions, Z = −0.13, p = .90.
TENS Negative Effects and Side Effects
Among 26 TENS trial sessions, the most common side effect was sleepiness and associated reflexes (eye blinking and yawning), each occurring in 10 sessions (38%). This sleepiness side effect was up to 20 minutes after the TENS session, according to the participants’ report. The second most common side effect was a worsening in speech fluency, individually determined by analyzing the frequency of stuttered syllables and the three highest stuttering moments before and after each TENS session. If stuttered syllables or the three highest stuttering moments increased at least 120%, the procedure was considered harmful. Using those guidelines, four participants showed worsening in fluency in four sessions (15%). Stuttered syllables increased 159% for Participant 4 and 6 after CD stimulation. The three highest stuttering moments increased 168% for Participant 2 after CD stimulation and 191% for Participant 8 after AB stimulation. According to the participants’ subjective reports, this side effect lasted from 2 to 5 days. It may be noteworthy to mention the participants’ reactions following the worsening of fluency. Participants 6 and 8 did not regret the experience, because they declared they wanted to test if TENS could be useful for them. Participant 4 did not actually realize that he had a worsening of fluency after TENS, only realizing it when confronted with data analysis. His reduced stuttering awareness became an issue during speech therapy, since he then became aware that his reports of “good and bad days” were likely inaccurate. Finally, Participant 2 was astonished at her worsening of fluency after TENS. She reported that it had been previously unthinkable. In her mind, just wanting TENS to be effective should have been enough to make it effective. She had not actually realized that motor issues could be involved in stuttering. The experience of worsened fluency after TENS was a turning point in her speech therapy, as she then had a broader understanding of stuttering that was not restricted to psychological factors. Apart from these negative effects on key stuttering variables, other occasional side effects were reported in only one session (4%) and included muscle stiffness and headache. Itching and skin burning under electrodes were not observed in any session.
Discussion
Speech Fluency Improvement
One of the most critical peripheral SES effects at the motor level relates to which muscle fibers are stimulated. Mammalian muscle fibers can be classified into two types (Guyton & Hall, 1996; Pette & Staron, 2000; Robinson & Snyder-Mackler, 2010): Type I (“slow”) muscle fibers are composed of Iβ isoform in the myosin heavy chain, and show slower contraction, smaller isometric tension, and higher fatigue resistance; Type II (“fast”) muscle fibers are composed by other isoforms in the myosin heavy chain (IIa, IId, or IIb), and show faster contraction, higher isometric tension, and lesser fatigue resistance. When applying SES, previous research has shown that the frequency of 10 Hz stimulates the slow nerve and muscle fibers (Pette & Staron, 2000).
Speech fluency improvements found in this study among participants with both stuttering and concomitant orofacial disorders should be explained in terms of the effects of SES on these different muscle fiber types. For participants with both stuttering and jaw clenching bruxism, TENS targeting the lower third of the face and submandibular region (AB stimulation) significantly reduced by 27% the median frequency of stuttered syllables and significantly reduced by 29% the median duration of the three highest stuttering moments. Clenching dental arches many hours per day is a sustained contraction that increases isometric jaw muscle tension, increasing the number of both slow and fast fibers in these muscles (Grünheid et al., 2009). Three explanatory hypotheses emerge: (a) low-frequency TENS for persons with jaw clenching bruxism may have stimulated slow fibers in the jaw muscles; (b) following TENS, these participants would have been more prone to activate slow fibers to perform oral motor control; and (c) this newly favored activation of slow versus fast fibers temporarily decreased the isometric jaw muscle tension. Thus, for speech motor control, these participants would have benefited from the favored activation of slow fibers to engage in smooth speech or in a more hyperarticulated speech style, paving the way for easier use of fluency shaping strategies in speech production and immediately reducing stuttering frequency and duration. Future studies combining TENS with surface electromyography would be useful to clarify if the improvement of stuttering after TENS in persons who also have jaw clenching bruxism may be attributed to decreased tone in jaw muscles.
In addition to bruxism, several other factors may also increase the number or strength of fast fibers in jaw muscles. For example, participants with short faces have a higher number of fast fibers in jaw-closing muscles when compared with participants with average or long faces (Grünheid et al., 2009). The hardness of food chewed also affects muscle fibers types. In rats, long-term intake of a soft diet increases the number of faster fibers in masseter muscle compared with long-term intake of a hard diet (Grünheid et al., 2009). Also, participants with persistent pain in jaw muscles (due to temporomandibular disorder, e.g.) may have an increased number of fast jaw clenching fibers than participants with no persistent pain (Grünheid et al., 2009). Thus, an individual may face difficulties using fluency shaping strategies for reasons other than jaw clenching bruxism. For these people who stutter, low-frequency TENS applied to jaw muscles may be useful. In the stuttering literature, the fiber types of speech muscles and factors that affect those fiber types have been largely ignored, even though behavioral speech therapy heavily relies on voluntary motor control for improving fluency.
For participants with both stuttering and mouth breathing, TENS at the posterior neck and shoulder girdle (CD stimulation) significantly reduced by 28% the median duration of the three highest stuttering moments and increased by 113% the median speech rate. Due to a forward leaning head posture, the muscles of the posterior neck have higher isometric tension in mouth-breathing individuals (Milanesi et al., 2011; Singla & Veqar, 2017). This characteristic presumably increases the number of fast fibers in these muscles. Here too, several hypotheses for explaining the current findings emerge: (a) low-frequency TENS may have stimulated slow fibers in the posterior neck and shoulder girdle, (b) following TENS participants may have been more prone to activate slow versus fast fibers to perform posture motor control, and (c) as slow fibers produce less isometric tension than fast fibers, the muscle tension needed to keep the head in the forward position may have been temporarily reduced such that the head may have moved more backward, decreasing stretched jaw muscles and facilitating the voluntary control of these muscles for fluency shaping strategies and, ultimately, the immediate reduction of stuttering duration and increased fluent speech rate. Again, future studies combining TENS with surface electromyography would be useful to clarify if the improvement of stuttering after TENS in mouth-breathing subjects may be ascribed to the decreased muscle tone in the muscles of the posterior neck.
In addition to mouth breathing, other conditions may cause forward leaning head posture. One of them, now very common, is the daily use of smartphones. Previous research with young adults has shown that head flexion is significantly greater for text messaging compared with web browsing and video watching (Lee et al., 2015). Heavy smartphone users are prone to forward head posture (the so-called text neck), usually accompanied by pain (Lee et al., 2015). Another situation that may cause forward head posture is a heavy backpack carriage. For example, a study with adolescents showed that backpacks with weights above 10% of body weight are associated with forward head posture (Cheung et al., 2009). Thus, an individual may have forward head posture that is not due to mouth breathing. As forward head posture increases muscle tension in the lateral and posterior neck, it may make the use of fluency shaping strategies more difficult. Hence, low-frequency TENS applied to the posterior neck and shoulder girdle may also be useful for people who stutter who present a forward head posture for reasons other than mouth breathing.
Tomazzetti (2004) reported the effects of a combined intervention using TENS and behavioral speech therapy for three adults with persistent stuttering. High-frequency (100 Hz) and high-intensity (the most vigorous motor contractions that the participant could bear) TENS was applied to stimulate muscles in the inferior third of the face and in the lateral and posterior neck. According to the author, the participants did not have any concomitant orofacial disorder. After 20 sessions, fluency improved for two participants and worsened for one. As can be seen, Tomazzetti applied a different protocol compared with the present study. Presumably, the protocol applied by Tomazzetti activated type I and type IIA nerve and muscle fibers, possibly for two reasons. First, it has been already shown that the frequency of 100 Hz activates both slow and fast fibers (e.g., Huang et al., 2016). Mammals have three types of fast fibers, classifiable by their isometric tension and fatigue resistance: (a) type IIA produces less tension and are more fatigue resistant, (b) type IID has an intermediate pattern, and (c) type IIB produces higher tension and is the least fatigue resistant (Pette & Staron, 2000). Humans do not have type IIB that is typical of small animals like rodents (Sciote et al., 2003). Second, TENS produces continuous muscle contractions, as opposed to functional electrical stimulation that produces interrupted muscle contractions with a clear on–off pattern (Robinson & Snyder-Mackler, 2010). TENS induced continuous muscle contractions that may have prevented the activation of faster muscle fibers (i.e., type IID) that are less fatigue resistant and, thus, not suitable for prolonged activation. Therefore, the use of TENS and the 100 Hz frequency in Tomazzetti’s protocol presumably activated type I and type IIA nerve and muscle fibers. This seems a reasonable protocol given that the participants did not have concomitant orofacial disorders associated with an increased number of fast fibers in the muscles of the face and neck. Therefore, the specific stimulation adjusted for TENS may depend on the presumed muscle fiber types shown by the individual. Tomazzetti also reported that one of the participants showed worsening of fluency after the combined treatment and asserted that this participant did not see himself as prone to stutter and so did not fully engage in treatment. Although Tomazzetti ascribed the participant’s worsened fluency to his non-acceptance of stuttering, it may also be that high-frequency and high-intensity TENS was not appropriate for him due to some other condition that may have increased the number of fast fibers in his jaw muscles, such as short face morphology (Grünheid et al., 2009) or higher levels of testosterone or thyroid hormones (Pette & Staron, 2000). Finally, both of Tomazzetti’s participants with fluency improvement reported that TENS enhanced their muscle proprioception and that this helped them apply fluency shaping techniques (such as smooth speech) or stuttering modification techniques (such as cancellation) when speaking. Participants in the present study also made very similar reports. Therefore, both my results and those of Tomazzetti indicate that TENS warrants further investigation as a potentially useful means of enhancing the behavioral treatment of stuttering.
Of importance, TENS does not just act upon peripheral tissues. Rather, the nuclei of sensory and motor nerves in the central nervous system are also activated with this procedure (Schuhfried et al., 2012). Moreover, there is activation of upper brain regions, such as the somatosensory and motor cortices (Schuhfried et al., 2012). The activation of upper brain regions may be of interest to stuttering, because neuroimaging studies have shown altered brain motor activation patterns during speech production. Some speech production areas of the left cortex (such as the orofacial region of the primary motor cortex, the premotor cortex, and the supplementary motor area) may be underactive in adults who stutter, with compensatory activation of the homologous areas in the right hemisphere (Craig-McQuaide et al., 2014; Smith & Weber, 2017). When applying TENS, frequencies less than 50 Hz are used to increase sensorimotor excitability, while frequencies greater than 50 Hz are used to decrease sensorimotor excitability (Erro et al., 2017). Therefore, future studies might select participants with persistent stuttering without concomitant orofacial disorders in order to assess the variable effects on speech fluency of low-frequency (such as 10 Hz) and high-frequency (such as 100 Hz) TENS. Low-frequency TENS would presumably improve speech fluency (due to increased sensorimotor excitability) while high-frequency TENS would presumably worsen it.
At this point, it is worth mentioning the results from Tinazzi et al. (2006), who also found improvement in motor control after a single session of TENS. The authors applied TENS to 10 participants with writer’s cramp, a condition that shares motor tension characteristics with stuttering (Alm, 2004). The author set sensory level TENS at 150 Hz for 30 minutes, placing electrodes at flexor muscles in the right forearm. Participants were then asked to write a standard paragraph as quickly as possible before and after the TENS session. The authors then applied a TENS frequency greater than 50 Hz to decrease sensorimotor excitability (Erro et al., 2017) that may be a characteristic of forearm flexor muscles in participants with writer’s cramp. Also, sensory level TENS was designed to not activate muscles; a 150 Hz frequency might have otherwise stimulated contraction of the flexor muscles in the participants’ right forearm due to fast fibers activation. Study results showed that participants needed less time for writing following the TENS session. Interestingly, motor-evoked potentials showed that the right flexor muscles were more inhibited, while the right extensor muscles were more excited after the session. Tinazzi et al. speculated that the sensory inputs for forearm flexor muscles transiently decreased the excitability of the primary motor cortex, inhibiting flexor muscles, and assisting handwriting improvements that helped free writer’s block.
A final observation refers to the use of transcranial direct current stimulation to improve the fluency of adults with persistent stuttering. Transcranial direct current stimulation is another type of SES in which electrodes are placed on the scalp and the electrical current crosses the head. Chesters et al. (2018) applied a 1 mA anodal stimulation for 20 minutes to 15 male adults who stuttered. The anode electrode was positioned on the scalp at the region corresponding to the left inferior frontal cortex, and the cathode electrode was positioned at the right supraorbital ridge. During electrical stimulation, the participants engaged in speech fluency-inducing tasks (i.e., choral and metronome-timed speech). These combined procedures of electrical stimulation and fluency induction were repeated for five consecutive days. Results were a treatment-based significant reduction of stuttering severity in 1 week (both for free speech and oral reading) and in 6 weeks (for oral reading only). These authors speculated that transcranial direct current stimulation increased excitability in the left motor cortex that in combination with the behavioral speech tasks enhanced motor learning and led to stuttering improvement. The main difference in stimulated pathways between TENS and transcranial direct current stimulation is that TENS stimulates the whole neurological pathway from the peripheral nerves to the cortical somatosensory and motor areas (Schuhfried et al., 2012), while transcranial direct current stimulates only cortical areas (cf. Chesters et al., 2018). Future studies may compare the effectiveness of both SES techniques for treating persistent stuttering, while also attending to the participants’ personal profiles.
TENS Intensity
The use in this study of smaller current intensity for the muscles of the lower third of the face in comparison with the muscles of the posterior neck and shoulder girdle is compatible with the greater somatosensory representation of the face versus the posterior neck and back. Skeletal muscles have muscle spindles while their tendons have Golgi tendon organs as somatosensory receptors (Purves et al., 2004). The number of receptors is not the same across body muscles in that there is an inverse relationship between muscle size and the number of receptors (Purves et al., 2004). Muscle size is inversely correlated with movement precision. As muscles of the lower third of the face and the anterior neck are small and must produce very fine movements, receptors are dense within them (Purves et al., 2004). The higher the density of receptors in a muscle, the higher the somatic sensitivity of that muscle (Purves et al., 2004). The higher density of receptors is also associated with a higher number of afferent nerve fibers and a larger somatosensory representation in the nervous system. Thus, the smaller current intensity for muscles in the lower third of the face is compatible with these smaller muscles, the higher number of somatosensory receptors, and the larger somatosensory representation in the nervous system of that region when compared with the posterior neck and shoulder girdle (Purves et al., 2004).
TENS Negative Effects and Side Effects
TENS is considered a safe technique. When it is applied to treat acute pain, minor side effects such as skin redness and itching under the electrodes have been reported (Johnson et al., 2015). In this study, two side effects were more common—sleepiness and a worsening of speech fluency. The occurrence of sleepiness and related blinking and yawning reflexes suggests that the reticular formation was activated. The reticular formation is a group of small neuron clusters located throughout the anterior region of the brainstem (Purves et al., 2004). Sleepiness suggests activation of the superior portion of the reticular formation, supporting sleep and wakefulness, while blinking and yawning reflexes suggest activation of the inferior portion, supporting orofacial motor reflexes (Purves et al., 2004). Sleepiness and related reflexes were common side effects in this study due to the electrode placement. The muscles of the inferior third of the face and anterior neck are innervated by cranial nerves, whose nuclei are in the brainstem (Purves et al., 2004). The muscles in the posterior neck and shoulder girdle are innervated by cervical and thoracic nerves, whose nuclei are in the upper cord but convey inputs to the brainstem (Purves et al., 2004). Thus, activation of brainstem motor nuclei by TENS possibly activated the reticular formation, leading to sleepiness and related reflexes.
Worsening in fluency supposedly occurred when muscle fatigue occurred. Muscle fatigue takes place when there is insufficient energy to sustain muscle contractions (Guyton & Hall, 1996). In this situation, motor control was temporarily impaired. For some subjects, a stimulation of 20 minutes may have caused muscle fatigue. Although slow muscle fibers are more fatigue resistant than fast fibers, this does not mean that they do not fatigue at all. A muscle fatigue explanation for worsened fluency is also supported by subsequent applications of TENS with the same participants who showed worsened fluency. Subjective assessments of subsequent applications of TENS during speech therapy suggested that these subsequent TENS applications did not produce the same negative results regarding speech fluency, indicating that muscles became more fatigue resistant after a 20-minute stimulation. On the other hand, the possibility of worsened fluency, even if short-lived, implies a need for caution when applying TENS for the first time with participants who stutter, as one cannot yet predict who will experience this negative effect. To prevent worsening, the first stimulation may be done with intensity at the motor threshold (i.e., as soon as the motor contractions begin) and should not take place within a few days prior to important speech situations (such as public speaking).
Demand Characteristics and Placebo Effect
The immediate fluency improvements of most participants in this study could possibly be ascribed to demand characteristics. In other words, participants may have tried harder to use fluency shaping techniques immediately after receiving TENS to confirm the experimental hypothesis (Nichols & Maner, 2008). Second, the improvements in fluency might be credited to a placebo effect in that the participants’ belief that TENS could be effective was responsible for the immediate positive effects discovered. However, the specificity of treatment effects and their theoretical relationship to study hypotheses strengthen the validity of these case study findings. If demand characteristics or placebo were responsible for these changes, all participants would have been expected to improve. However, participants with jaw clenching bruxism did not improve with CD stimulation and those with mouth breathing did not improve with AB stimulation. In contrast, those with bruxism did improve with AB stimulation and those with mouth breathing improved with CD stimulation.
The effectiveness of TENS has been previously tested against placebo effects. A systematic review by Johnson et al. (2015) showed that TENS alone better reduced acute pain from physical trauma or medical procedures in adults than did placebo. TENS has also been effective for focal hand dystonia. Tinazzi et al. (2005) evaluated TENS versus placebo (a sham ultrasound treatment in which the ultrasound therapy device was turned off) in 10 participants with writer’s cramp. Participants treated with TENS showed a reduction of 25% in the time needed for writing and also reported a reduction in the subjective effort for writing. These improvements occurred immediately after the treatment and persisted for at least 3 weeks.
Limitations
Despite the aforementioned arguments, this multiple case study is limited by the absence of a control group. In addition, there were a small number of participants. Although speech fluency was assessed with speaking tasks in this study, future studies might also include reading aloud tasks in order to provide a more extensive fluency assessment. Future studies might improve on the diagnosis of jaw clenching bruxism by including electromyographic recording during wakefulness or sleeping (cf. Lobbezoo et al., 2013). Similarly, future studies might include an oral myofunctional assessment for participants with mouth breathing. Only the immediate effects of TENS in speech fluency were analyzed in this study, and future work should investigate long-term benefits. Despite these limitations, the present study presents a strong theory-based argument for potential benefits of TENS interventions to assist behavioral speech therapy for individuals with stuttering and concomitant-specific muscle tension impediments.
Supplemental Material
PMS915027 Suplementary Table - Supplemental material for Surface Electrical Stimulation for Persistent Stuttering and Concomitant Orofacial Disorders: A Multiple Case Study
Supplemental material, PMS915027 Suplementary Table for Surface Electrical Stimulation for Persistent Stuttering and Concomitant Orofacial Disorders: A Multiple Case Study by Sandra Merlo in Perceptual and Motor Skills
Footnotes
Acknowledgments
Bruno Guimaraes, a speech-language pathologist with vast experience with TENS for voice disorders, has provided technical assistance at the beginning of this work. Subjects have kindly authorized the use of their data. Dr. Irene Marchesan, a speech–language pathologist, has generously authorized the submission of the research project to the Ethics Committee of “CEFAC—Saude e Educacao”. JM has sat for photographic pictures, and Listo Studio has produced instructive drawings. Adail Sobral has provided English language editing. Two anonymous reviewers and the Editor, J. D. Ball, have provided valuable comments.
Article Notes
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.