
Abstract
Offender readiness is important to the success of substance abuse and therapeutic programs. Prisons provide a variety of programs, including reentry, vocational, and creative programs that have been shown to improve reentry success. And yet, the concept of program readiness has not been examined in these contexts. We explore the development of a broader measure of program readiness. Toward this goal, we developed a preliminary generalized program readiness measure for correctional programming more broadly. Results supported a two-factor measure, desire for help and recognition of program needs. These findings support continued research and development of a generalized program readiness measure.
Introduction
The United States has the largest inmate population in the world with over 1.9 million people in state and federal facilities (Sawyer & Wagner, 2024). Of those released, it is estimated that roughly one-third will be re-incarcerated within a year (Durose et al., 2014). Correctional programming has been shown to improve the successful reentry of incarcerated individuals. Multiple studies have shown that those who participate in correctional programs are less likely to engage in misconduct while incarcerated and are less likely to return after release (e.g., French & Gendreau, 2006; Langan & Pelissier, 2001; Taylor et al., 2019). Correctional facilities across the country offer a wide range of programs that enable offenders to improve their education, develop new skills, maintain an active and healthy lifestyle, and solve problems related to criminogenic behaviors related to addiction and mental health. Research has found that a wide range of prison-based programs have been associated with positive outcomes for inmates, including those centered on exercise and physical health (Loeb et al., 2013), religion (Dye et al., 2014; Hallett & McCoy, 2015), music (Bensimon et al., 2015; Tuastad & O’Grady, 2013), arts and crafts (Gussak, 2006), and anger management (Bus et al., 2009; Law, 1997). Prison programming is also important to facility organization and efficiency. Specifically, programming can have a significant impact on prison staff through reductions in inmate aggression and violence (Blevins et al., 2006; Lambert et al., 2010). Moreover, Howells and Day (2007) suggest that low engagement and non-completion of programs can lead to reduced institutional support and lower staff morale. Prison programs also require resources and staff, which increase facility costs. Correctional facilities operate under constant financial strain and have limited capacity for correctional programs. Given these institutional constraints, it can be useful for correctional staff to be able to identify which incarcerated individuals are ready, motivated, and interested in participating in available programs.
Despite the positive effects of correctional programming, it’s still largely unclear why offenders decide to initially engage in programs. Community-based studies have identified several factors that may influence program participation, such as gender, prior substance use (Butler et al., 2022; Sloas et al., 2017), race (Anderson et al., 2022), and the number of days incarcerated (Butler et al., 2022). Importantly, there is a growing body of evidence to suggest that an individual's level of readiness may be an important component in their decision to engage or participate in programs (McMurran et al., 2008; Simpson & Joe, 1993). This research has shown that treatment motivation and program readiness are significantly associated with program engagement at intake as well as during program participation (Garner et al., 2007; Joe et al., 2010). Most of the studies, however, have been limited to the examination of program readiness for therapeutic or substance abuse programs.
With this in mind, we argue that correctional facilities would benefit from a universal measure of program readiness that helps to inform all types of program participation. An accurate measure of program readiness may be utilized by correctional staff to improve the referral process, match inmates with the appropriate programs, satisfy program accreditation requirements, and maximize the use of limited resources (Mossière & Serin, 2014). Given the promising body of literature on the use of a treatment readiness measure in substance abuse and therapeutic programs, we explore the theoretical and practical applications of extending this concept beyond the treatment context. Toward this goal, the current study provides a preliminary conceptualization and development of a generalized program readiness measure in the context of broad inmate programming.
Treatment Readiness and Program Outcomes
Treatment readiness and similar concepts such as treatment motivation, readiness to change, readiness to engage, and offender motivation to change (Mossière & Serin, 2014) have been associated with successful program outcomes. Originally applied to addiction treatment, motivation has been regarded as a necessary component for clients to enter, continue, and complete treatment (Miller, 1985). It is broadly defined to include whether an individual is motivated to participate in treatment and has the desire to change their behavior (Ward et al., 2004). Simpson and Joe (1993)posit that motivation is comprised of three components—internal motivation, desire for help, and treatment readiness (see also Simpson et al., 1997). Desire for help is an internal factor consisting of interests and goals (McMurran & Ward, 2004), or the intrinsic need for change and a stake in support (Simpson & Joe, 1993). Treatment readiness can be defined as “the presence of characteristics (states or dispositions) within either the client or the therapeutic situation, which are likely to promote engagement in therapy and which, thereby, are likely to enhance therapeutic change” (Ward et al., 2004, p. 650). Treatment readiness was introduced in the offender context by Serin and Kennedy (1997) as part of a treatment responsivity evaluation in correctional programming (Serin, 1998). The model developed on this framework views treatment readiness as a multidimensional concept that extends beyond motivation and is a function of both internal and external factors (McMurran & Ward, 2010; Serin, 1998; Ward et al., 2004).
Prior research examining these concepts has found them to be important predictors of program engagement and retention. Studies evaluating treatment readiness and motivation among those in programs for drug addiction have uncovered significant associations with treatment engagement at intake and during-treatment (Garner et al., 2007; Joe et al., 2010; Pankow et al., 2012; Simpson et al., 2012). Moreover, a desire for help has been found to decrease program withdrawal in community drug treatment (Simpson et al., 1995), and improved psychosocial functioning and decreased criminal thinking for inmates in therapeutic communities (Joe et al., 2010).
Models Treatment Readiness and Motivation
There are three common theoretical frameworks used to model readiness and motivation constructs: the Transtheoretical Model (TTM), the Multifactor Offender Readiness Model (MORM), and the Readiness for Change Framework (RCF; Mossière & Serin, 2014). The TTM posits that individuals experience behavioral change as they progress through five stages which include pre-contemplation, contemplation, determination, action, and maintenance (Prochaska & DiClemente, 1982). While not originally designed to measure offender readiness, the five stages of change can provide an indicator of readiness that may help practitioners modify treatment (Serin & Kennedy, 1997). This model primarily targets the internal characteristics of the individual.
The MORM hypothesizes that changes in behavior are more likely to occur when the offender is ready to participate in treatment (Bosma et al., 2016; Ward et al., 2004). This can be defined as the existence of characteristics within the offender that promote engagement in the therapeutic process that then lead to behavioral change. When offenders are (a) motivated, (b) capable of responding to treatment, (c) believe the treatment is meaningful, and (d) are physically able to participate, then readiness for treatment is present (Bosma et al., 2016; Howells & Day, 2007). The MORM proposes that these characteristics are a product of internal factors—cognitive, affective, volitional, behavioral, and identity—and external factors, including circumstances, location, opportunities, resources, interpersonal supports, and program characteristics (Ward et al., 2004).
The RCF is a broader conceptualization that includes aspects of both the MORM and TTM, modeling readiness to change as a dynamic process that can be influenced by internal and external factors (Burrowes & Needs, 2009). The two elements of the RCF include the Context of Change Model (CCM) and the Barriers to Change Model (BCM). The CCM is composed of three interrelated concepts: (1) the individual's internal concept, (2) the catalyst for change, and (3) the environment of change. The BCM consists of 10 obstacles that represent barriers between the individual and behavioral change. Burrowes and Needs (2009) suggest that readiness for change can be assessed by identifying barriers (BCM) and the contextual factors (CCM) that may predict them.
Measures of Treatment Readiness
Several constructs have been created to measure program readiness. In a systematic review, Mossière and Serin (2014) identified 11 different constructs utilized to assess program readiness. While these measures serve the same overall purpose, they vary in their conceptual frameworks, population, and predictive validity. One of the scales that has been frequently implemented in practice and critically tested is the Texas Christian University CJ Client Evaluation of Self and Treatment (TCU CJ CEST) Intake (Mossière & Serin, 2014; Weinrath et al., 2019).
Studies evaluating the CJ CEST have found that treatment needs and motivation scales are significantly associated with treatment engagement at intake and during treatment participation among those in programs for drug addiction (Garner et al., 2007; Joe et al., 2010; Pankow et al., 2012; Simpson et al., 2012). Similar findings were also reported in a sample of inmates participating in a cognitive skills program, using the Corrections Victoria Treatment Readiness Questionnaire (Casey et al., 2007). However, results are mixed among studies using other measures of program readiness. For example, Sloas et al. (2017) examined treatment motivation and substance abuse program engagement in samples from correctional and community-based settings. Treatment readiness was measured using the Treatment Motivation Index, and findings showed no relationship to program engagement after the first 30 days.
The TCU CEST is an assessment that was originally designed to evaluate the drug-treatment process (Simpson et al., 1995, 2012). A conceptual model in and of itself, the CEST framework incorporates stages of change found in the TTM along with external factors considered in the MORM. This assessment emphasizes the importance of evaluating needs, functioning, and during-treatment change to gauge treatment progress toward the targeted intervention (Garner et al., 2007). The success of the CEST in community-based settings prompted its adaptation for use in criminal justice settings in what is referred to as the CJ CEST. The CJ CEST contains 21 scales that measure four domains that include treatment motivation, psychological functioning, treatment engagement, and criminal thinking (Garner et al., 2007). To provide greater flexibility in its administration, the CJ CEST has also been reformatted into single-page assessments termed the TCU Short Forms (Simpson et al., 2012). For the purpose of the current study, the following section will discuss the CJ CEST Intake Short Forms used to measure treatment motivation.
CJ CEST Intake Short Forms
The four CJ CEST constructs used to measure the treatment needs and motivation domains are comprised of two scales—desire for help and treatment readiness—and two index measures—treatment needs and pressures for treatment. Desire for help is regarded as an important aspect in achieving behavioral change, and represents the intrinsic requisite for change and interest in obtaining help (Joe et al., 2002; Prochaska & DiClemente, 1982). While one may possess the desire for change, individuals may also have commitment issues or a reluctance toward a level of commitment required. Thus, program readiness measures the choice for action through a commitment for participation in treatment (Joe et al., 2002). The treatment needs index contains a list of items that the individual may indicate as areas of additional help, and the pressures for treatment index highlights various areas where the participant may perceive external pressures (Garner et al., 2007).
Each scale includes 5–8 items measured on a 5-point Likert scale that ranges from 1 (strongly disagree) to 5 (strongly agree). Scores are calculated by summing the responses to items, dividing the sum by the number of items, and then multiplying by 10. Final scores range from 10 to 50 (see Garner et al., 2007). The CJ CEST Intake Forms, containing the treatment needs and motivation scales, have good test–retest reliability (Garner et al., 2007; Simpson et al., 2012), discriminate validity (Saum et al., 2007), and predictive and concurrent validity (Pankow et al., 2012). Additionally, it has now been applied in a number of settings. While originally designed as an assessment for planning and implementing addiction treatment, the CJ CEST has also been introduced in correctional settings for substance abuse and therapeutic communities (Garner et al., 2007; Prendergast et al., 2002; Saum et al., 2007; Simpson et al., 2012).
Current Focus
To date, program readiness constructs have primarily been used in substance abuse treatment programs and therapeutic communities. The correctional programs available to incarcerated persons are diverse and offer a variety of benefits, such as targeting criminogenic needs, improving physical or mental health, or, simply reducing opportunities to engage in otherwise negative behaviors. Investigations of program readiness and motivation scales have shown them to be useful in improving program effectiveness by effecting more efficient placements and developing methods to increase engagement and successful program completion. Therefore, the current study seeks to expand these findings of program readiness by developing a generalized measure for broad correctional programming. Specifically, the study employs exploratory and confirmatory factor analysis (CFA) techniques to develop a preliminary measure of program readiness that can be applied to all types of correctional programs.
Method and Data
Data were collected in February and March 2019 in a private U.S. southern prison housing minimum, medium, and maximum-security offenders. The target sample of incarcerees included those that were eligible and able to participate in programs, excluding those in restrictive housing or in administrative segregation. At the time of data collection, there were approximately 800 adult males who were eligible to participate in facility programs (Kaiser et al., 2021). Prior to administering the survey in each unit, researchers read a script that outlined the survey's purpose and distributed consent forms to those interested. Participants were informed that responses to the survey would be available only to researchers; the completed surveys would remain confidential and not be disclosed to prison staff.
The paper–pencil survey was administered in two stages. During the first stage, yielding 164 surveys, volunteers were brought to the visitation area where they were read questions aloud to increase accessibility and clarification. To ensure confidentiality, prison staff remained at the room's perimeter so that they were unable to view responses (Kaiser et al., 2021). In the second phase, additional blank copies of the survey and envelopes were left within each unit (Kaiser et al., 2021) to accommodate those who were unable to attend the in-person session, completing the survey on their own time. The researchers returned 1 week later to collect the responses which had been placed in a sealed envelope in a lock box inaccessible to staff. An additional 48 surveys were collected during this stage, bringing the total sample to 212, with a response rate of roughly 26% (Kaiser et al., 2021).
The average age of respondents was about 45 (SD = 11.90), and the average sentence length was 46.41 years. More than half of the participants reported a race/ethnicity of Black (60.1%). The remaining self-reported: White (27.9%), Other (22.0%), and Hispanic (4.88%). In comparing the two phases of collection, there were no significant differences in demographic characteristics or key variables such as program participation, program interest, and barriers to participation. Additionally, sample demographics not only closely resembled the facility population but also that of the local region (Kaiser et al., 2021). One participant's survey was excluded since the items under examination were not complete, bringing the final sample size to N = 211.
Variables
Program motivation/readiness was assessed using a revised version of the TCU CJ CEST instrument (Simpson & Joe, 1993). The CJ CEST was selected given its extensive testing and revisions as well as its ease of use and cost-efficiency. The TCU assessments have been examined since the early 1990s. In 2005, the CJ CEST had been utilized in 26 corrections-based programs and over 3,266 clients, with increased usage since then (Pankow et al., 2012; TCU Institute of Behavioral Research, 2005). The CJ CEST includes two scales and two indices that tap into treatment needs and motivation, including desire for help, treatment readiness, treatment needs, and pressures for treatment. All items are measured on a 5-point Likert scale (1 = strongly disagree to 5 = strongly agree). Additionally, items were re-worded for the correctional setting and to reflect all programs (e.g., the phrase “drug treatment” was changed to “programs”). A full list of the items included is in Table 1. Additionally, a comparison of the original CJ CEST and the revised version can be found in the Appendix (Table A1).
Description of Scale Items (N = 211).

Reverse coded so higher scores indicate lower negative traits.
Desire for Help. The desire for help scale consists of five items adapted for broad program assessment. For example, “I need help with my drug use” was reworded to “I need help with my problems,” and “I am tired of the problems caused by drugs” was reworded to “I am tired of the problems caused by my decisions.” The original scale included in the TCU CJ CEST contains six items measuring desire for help. However, given that the current implementation is in a correctional setting, “You will give up your friends and hangouts to solve your drug problems” was excluded.
Program Readiness. Program readiness contains four items adapted from the original eight in the CJ CEST scale. Four items specifically ask about drug treatment (“I need to stay in treatment”; “This treatment program gives me hope for recovery”; “I want to be in drug treatment”; “I am ready to leave this treatment program”), were excluded from the questionnaire. To adapt items for all programs, items such as, “I am not ready for this kind of treatment program” and “this kind of treatment program is not helping me,” were reworded to “I am not ready to participate in programs” and “the kinds of program offered are not helpful to me,” respectively.
Program Needs. Program needs was measured using four items that measure general program needs and recognition of problems. One item (“I need more group counseling sessions”) was excluded from the scale due to the broader nature of programs that include a number of settings.
Social Pressure. Social pressure was measured using four items from the original seven included in the CJ CEST. Since the current sample consists of adults currently incarcerated, four items (“I could be sent to jail or prison if I am not in treatment”; “several people close to me have serious drug problems”; “I have legal problems that require me to be in treatment”) were excluded. To adapt items to broad program assessment, “You have serious drug-related health problems” was reworded to, “I have serious health problems related to my past choices.”
Analytic Strategy
The purpose of the current study is to examine program readiness through an instrument for assessing program participation in correctional settings. A core method to accomplish this includes positing several possible models and comparing them to one another. The broad goal of this analysis is to identify a model with good absolute fit, good fit relative to other models, and one as parsimonious as can be allowed given fit indices. The analysis will be conducted in two steps.
First, exploratory factor analysis with varimax rotation will be conducted to investigate the underlying factor structure to the questionnaire items. Alphas and correlations will be examined as initial indicators of convergent and discriminant validity. Then, eigenvalues will be reviewed to identify the appropriate factor solution (Kim & Mueller, 1978). Second, hypothesized models will be evaluated based on fit indices, between-factor correlations, and modification indices using CFA. 1 In psychometric evaluations, CFA allows for estimation of scale reliability and the support of construct and discriminant validity (Hoyle, 2012). CFA also requires theoretical and empirical support in the specification of a factor model. Scale items were adapted from reliable scales with strong empirical support; therefore, CFA is a suitable analytic tool. Model fit will be examined holistically using five fit indices suggested by Credé and Harms (2015). First, the chi-square statistic will be included to reflect the model's ability to replicate the observed variance–covariance matrix from manifest variables and assess any misspecification of the model. The root-mean-square error of approximation (RMSEA), standardized root-mean-square residual (SRMR), comparative fit index (CFI), and Tucker–Lewis index (TLI) will also be presented to reflect the fit of the model. Finally, the CFA will be compared with several alternative models that are theoretically plausible. Good fit is not commensurate with best fit. Thus, if alternative models are not explored, the fit of the CFA cannot be supported as the ideal model.
Results
To examine initial tests of convergent and discriminant validity, Cronbach's alpha, correlations, and exploratory factor analysis (principal factor analysis with varimax rotation), were analyzed. Several items were significantly correlated among the items hypothesized to represent the same construct. However, several items that represent different constructs were also correlated. Results for the principal factor are presented in Table 2. Principal factor analyses were conducted for all 17 items. The Bartlett's test of sphericity was statistically significant (χ2 = 672.009, p < .000), indicating that the items were uncorrelated. Additionally, the Kaiser–Meyer–Olkin measure of sampling adequacy was .70, indicating that the data were suitable for factor analysis (Yong & Pearce, 2013).
Principal Factor Analysis Loadings (N = 178).

Note. Coefficients >.40 are shown in bold.
Reverse coded so higher scores indicate lower negative traits.
While the original CJ CEST included three scales representing distinct constructs, when using the Kaiser criterion (eigenvalues >1) and after examination of the scree plot (Figure 1) and parallel analysis, a two-factor solution emerged (2.70, 1.96). 2 Contrary to expectations, several items loaded on separate factors. Factor one was defined by five items, including Items 1 (I need help with my problems), 3 (my life is out of control), 10 (I need help with my emotional troubles), 11 (I need counseling sessions), and 17 (I have serious health problems related to my past choices). All five items center on recognizing that programs can help with areas of concern. Therefore, this factor was deemed recognition of program needs. Factor two was also defined by five items, including Items 2 (I desire to better myself), 4 (I am tired of the problems caused by my decisions), 5 (I want to get my life straightened out), 6 (Programs and classes give me a chance to solve my problems), and 14 (I have family members who want me to be in treatment). Since all five items centered on expressing a desire for addressing problem areas of one's life, this factor was deemed desire for help.
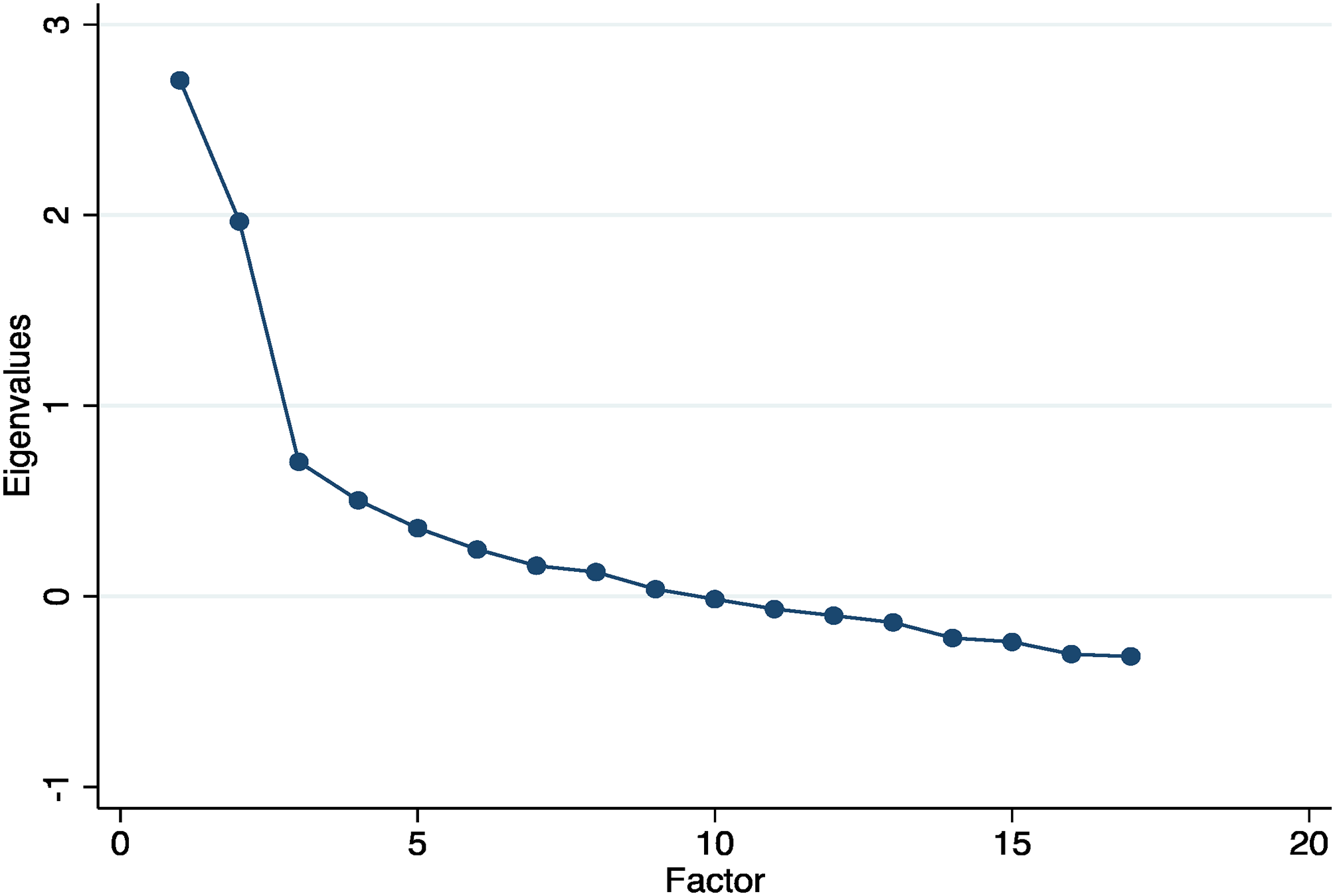
Scree plot of eigenvalues.
Before further examination of the emerging factor structure, CFAs were also conducted on the original three adapted scales (Table 3). Results indicated that this model had poor fit. The chi-square was statistically significant, and the RMSEA (.111), SRMR (.122), CFI (.687), and TLI (.607) did not meet minimum standards. This further confirmed the factor structure results that deviated from the original scale items.
Confirmatory Factor Analysis Results of Two- and Three-Factor Models (N = 187)

***p < .001.
Model fit of the resulting two-factor solution was examined using CFAs. Inspection of the CFA solution was conducted to find an appropriate measurement model and improve model fit. 3 First, Item 1 (I need help with my problems) cross-loaded on factors one (.46) and two (.30). To assess whether this item was exerting an adverse impact on the model, it was dropped, and fit was reassessed. 4 Then, the examination of modification indices of the unique-error terms warranted the inclusion of two correlations between error terms in the model (Hoyle, 2012; Kline, 2023). Correlation between error terms of Items 2 and 5, and Items 6 and 14 were freely estimated because they displayed the greatest modification indices values. Strong theoretical support justified the inclusion of these correlations. Items 2 and 5 both focus on the desire for improving life circumstances, while Items 6 and 14 centered on addressing problems through programming. Additionally, after further model comparison, including Item 13 (I need medical care and services) in Factor 1 improved overall model fit.
Table 3 presents the results of the CFA on the final two-factor model. Fit significantly improved with the inclusion of the two correlated error terms and the inclusion of Item 13. The chi-square was not significant, the RMSEA dropped to .045, the SRMR dropped to .056, and the CFI and TLI rose to .969 and .957, respectively. Additionally, the two factors were correlated (.224), indicating that variance in desire for help was related to recognition of program needs, and vice versa. Additional modification of the model was neither theoretically justified nor beneficial to model fit; thus this represented to best overall fit.
After the final model of best fit was determined, a preliminary test of predictive validity for the new program readiness measure was examined using bivariate correlations. Regarding program readiness, program participation (r = .009, p < .05) was not statistically significant, however, program interest (r = .30, p < .001) was positive and statistically significant. Directions for future research and limitations are discussed in the following section.
Discussion
Program readiness, treatment motivation, and similar concepts have been recognized as important factors for entering, continuing, and completing treatment (Miller, 1985). In general, these concepts can be defined as a desire to participate in treatment and exhibiting a desire to change behavior. Several measures have been developed and refined to gauge program readiness, monitor during-treatment progress, and improve the services provided to participants (Mossière & Serin, 2014). Specifically, the TCU CEST is an assessment designed to evaluate needs, functioning, and during-treatment progress toward a specific intervention (Garner et al., 2007). While originally designed for use within community-based settings, the successful outcomes verified from this assessment have led to its application in criminal justice settings in what is called the CJ CEST (Garner et al., 2007). Notably, the CJ CEST has been utilized in correctional substance abuse programs and therapeutic communities and has been found to be a reliable measure of treatment needs and motivation (Garner et al., 2007; Pankow et al., 2012; Prendergast et al., 2002; Saum et al., 2007; Simpson et al., 2012).
To expand the research literature, the purpose of the current study was to develop a measure of program readiness for all prison programming, utilizing a revised version of the CJ CEST short forms. The factors proposed in this study indexed two program readiness-related constructs that tap into the level of desire for help and ability to recognize needs for programs among adults in custody. The revised constructs/instrument did not completely conform to prior research examining the CJ CEST scales in that the constructs were intended to measure the motivation for program participation beyond just treatment for alcohol and substance addiction. Results from this study not only support the need for future research into a revised program readiness measure for broad programming and one that may also be useful for practitioners in correctional program placements. Additionally, the revised measure could represent a cost- and time-efficient method for offender program placement, and one that may improve dropout/failure rates.
Psychometric properties of 17 items composing three subscales and one index of the program readiness/motivation domain were analyzed. A two-factor model represented by desire for help (five items) and recognition of program needs (five items) resulted in the best-fitting model. This model was appropriately identified, where CFA models comprised of two or more factors must have two or more indicators each (Kline, 2023), and the model revealed good fit and parsimony. Additionally, results provided empirical support for these factors as distinct, but related factors of program readiness.
Recognition of Needs
This construct tapped into program-related areas where incarcerated persons need additional help. While not being specific to any one program or service, there are nonetheless problem areas that inmates recognize as being present and subject to improvement by program participation. This subscale most resembles a problem recognition construct utilized in original CEST scales (see Simpson & Joe, 1993). This scale represents the transition from “pre-contemplation” to “contemplation” in Prochaska and DiClemente’s (1982) model of change, where denial of having problems is the first barrier to behavioral change. The current scale thus appears to tap into the acknowledgment of a personal need for programs. Areas of concern or problems are diverse and unique to the various environments and circumstances that incarcerated individuals face. Additionally, there are countless unique programs offered across correctional facilities that can serve as outlets or help in dealing with problems. Future research into broad program readiness should consider additional items identified in empirical research as problem areas for justice-involved people, such as anger management, literacy, conflict resolution, communication with staff, gang involvement, and idle time, to name a few.
Desire for Help
The scale taps into the intrinsic interest of getting help. Once a need to deal with problems is acknowledged, an individual can transition to a stage of having a desire for assistance. This most closely resembles further movement toward the “action” stage for change model (Prochaska & DiClemente, 1982). The current study scale is also supported by early psychometric evaluations of the CJ CEST. Using a sample (N = 311) of participants admitted to methadone maintenance treatment at three locations, Simpson and Joe (1993) examined the psychometric properties of the CEST motivation scales. 5 The scales evaluated included problem recognition, desire for help, and treatment readiness, composed of 24 items. Similar to the current findings, factor analysis of all items composing the three scales revealed that several items loaded on different factors. Specifically, three treatment readiness items loaded with desire for help items. In the current study, the same revised item (“programs and classes give me a chance to solve my problems”) replicated this finding. Additional psychometric evaluations of the CEST motivation scales primarily examine them independently; thus further studies have not replicated this finding.
Limitations and Future Research
While the current study expands the correctional program readiness literature, there are also limitations to note. First, it is important to acknowledge differences in the current study sample that may contribute to findings. This study utilized minimum-, medium-, and maximum-security inmates from a private U.S. prison. The length of time spent at the current facility ranged from less than 1 month (5.3%) to 5 years or more (45.7%), and the average sentence length was 46.41 years (SD = 30.64). While specific time in the facility and sentence length are unclear in prior studies, the research assessing CJ CEST scales with correctional populations has primarily examined inmate participants in drug treatment programs and therapeutic communities ranging in time from 6 to 18 months (Garner et al., 2007; Saum et al., 2007; Simpson et al., 2012), or included those that had less than a year to 18 months remaining on their current sentence (Prendergast et al., 2002). As the characteristics of participants in this investigation had long-term sentences and differed significantly from the prior study samples, it may be the case that our study sample conceptualized problems differently and had different perceptions of what correctional programs could do for them. Future research should include more diverse samples of correctional program participants to further assess the impact of sample profiles in applying measures of program readiness.
Second, the sample size limits the interpretation of results. Structural equation modeling such as CFA requires large samples; however, there is no one-size-fits-all standard (Kline, 2023). Suggested sample sizes range from roughly 130 to >1,000, with some research even suggesting that samples of 100 can be used (Kline, 2023). Regarding the final model of best fit, the small sample size may be biasing the high loadings and correlations among only a few questionnaire items. Additionally, while our findings suggested that the final model had good fit, the sample size limits the ability to further examine predictive validity.
Third, the current study utilized data from a cross-sectional sample, which limits the ability to draw causal inference into the predictive validity of the new program readiness measure. Bivariate correlations were examined as preliminary tests of the relationship between program readiness and program participation as well as program interest; however, information was not available regarding when inmates participated in each program. Future research would benefit from large, longitudinal samples that would allow for pre- and post-program data and greater confidence in model estimates.
Conclusion
We hope that this exploratory study promotes further research into the development of a broad program readiness measure. Continued inquiry is needed into the conceptualization of motivation and program readiness within correctional program settings. While this is the first study to apply these concepts to fit a measure of broad correctional program readiness, the basic constructs for developing such measures still lack consensus on definition and measurement (Mossière & Serin, 2014). Moreover, further investigations would benefit from the use of samples that have not yet entered treatment and have not been mandated to participate. Mossière and Serin (2014) suggest that readiness is not an ideal measure for examining program outcomes, such as withdrawal and post-program misconduct. Arguably, treatment readiness should not be used to assess during-treatment progress, withdrawal, or outcomes such as recidivism and post-program misconduct. Rather, the ideal question is “why do offenders not participate in programs.” This may be attributed to “readiness” and “motivation” being used interchangeably, when they are conceptually different.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Notes
Author Biographies
Appendix
Comparison of Original and Revised Readiness/Motivation Scales
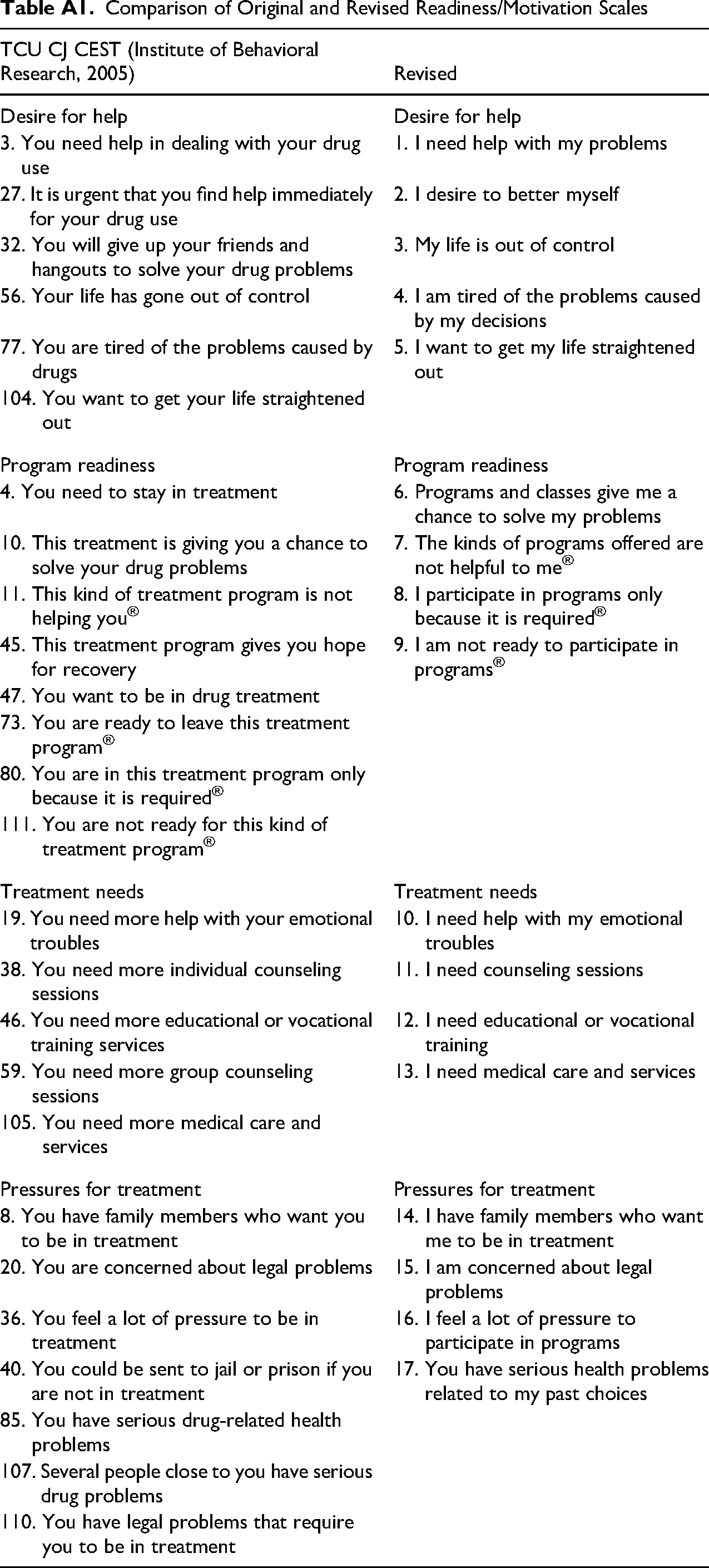
| TCU CJ CEST (Institute of Behavioral Research, 2005) | Revised |
|---|---|
| Desire for help | Desire for help |
| 3. You need help in dealing with your drug use | 1. I need help with my problems |
| 27. It is urgent that you find help immediately for your drug use | 2. I desire to better myself |
| 32. You will give up your friends and hangouts to solve your drug problems | 3. My life is out of control |
| 56. Your life has gone out of control | 4. I am tired of the problems caused by my decisions |
| 77. You are tired of the problems caused by drugs | 5. I want to get my life straightened out |
| 104. You want to get your life straightened out | |
| Program readiness | Program readiness |
| 4. You need to stay in treatment | 6. Programs and classes give me a chance to solve my problems |
| 10. This treatment is giving you a chance to solve your drug problems | 7. The kinds of programs offered are not helpful to me® |
| 11. This kind of treatment program is not helping you® | 8. I participate in programs only because it is required® |
| 45. This treatment program gives you hope for recovery | 9. I am not ready to participate in programs® |
| 47. You want to be in drug treatment | |
| 73. You are ready to leave this treatment program® | |
| 80. You are in this treatment program only because it is required® | |
| 111. You are not ready for this kind of treatment program® | |
| Treatment needs | Treatment needs |
| 19. You need more help with your emotional troubles | 10. I need help with my emotional troubles |
| 38. You need more individual counseling sessions | 11. I need counseling sessions |
| 46. You need more educational or vocational training services | 12. I need educational or vocational training |
| 59. You need more group counseling sessions | 13. I need medical care and services |
| 105. You need more medical care and services | |
| Pressures for treatment | Pressures for treatment |
| 8. You have family members who want you to be in treatment | 14. I have family members who want me to be in treatment |
| 20. You are concerned about legal problems | 15. I am concerned about legal problems |
| 36. You feel a lot of pressure to be in treatment | 16. I feel a lot of pressure to participate in programs |
| 40. You could be sent to jail or prison if you are not in treatment | 17. You have serious health problems related to my past choices |
| 85. You have serious drug-related health problems | |
| 107. Several people close to you have serious drug problems | |
| 110. You have legal problems that require you to be in treatment |