
Abstract
People with psychiatric disabilities experience significant impairment in fulfilling major life roles due to the severity of their mental illness. Recovery for people with serious mental illness (SMI) can be a long, arduous process impacted by various biological, functional, sociological, and psychological factors that can present as barriers and/or facilitators. The purposes of this study were to (a) investigate the International Classification of Functioning, Disability, and Health (ICF) framework’s ability to predict recovery in adults with SMI and (b) determine to what extent the ICF constructs in the empirical model explain the variance in recovery. Participants (N = 192) completed a sociodemographic questionnaire and various measures representing all predictor and outcome variables. Results from hierarchical regression analysis with six sets of predictors entered sequentially (1 = personal factors-demographics, 2 = body functions-mental, 3 = activity-capacity, 4 = environmental factors, 5 = personal factors-characteristics, and 6 = participation-performance) accounted for 75% (large effect) of the variance in recovery. Controlling for all factors, by order of salience, the factors found to significantly predict recovery were higher levels of significant other support, education, executive function impairment, and social self-efficacy; primary, non-bipolar SMI diagnosis; greater resilience; lower levels of explicit memory-health impairment, affective self-stigma, and cognitive self-stigma; being younger; fewer self-care limitations; less severe psychiatric symptoms; and being unemployed and unmarried. Findings support the validation of the ICF framework as a biopsychosocial recovery model and the use of this model in the development of effective recovery-oriented interventions for adults with SMI. Clinical and research implications are discussed.
Keywords
Mental health problems are quite common. Two of the top 10 health conditions adversely affecting Americans today are psychiatric: major depression (9.6%) and psychotic disorders (2.7%), ranked second and ninth, respectively (Blue Cross Blue Shield, 2019). Estimates indicate that nearly half the U.S. population will experience a mental illness during their lifetime (Kessler et al., 2007), whereas almost one in five adults live with a mental illness in any given year (Substance Abuse and Mental Health Services Administration [SAMHSA], 2019). Mental disorders range from mild to severe; serious mental illness (SMI) results in functional impairment, substantially limiting major life activities (National Institute of Mental Health [NIMH], 2019). This disability, or “role failure” (Haber & Smith, 1971), results from problems between a person (P) and their environment (E), or the P–E interaction (P × E; Wright, 1983). The U.S. Census Bureau assesses functional impairment (disability) in six broad areas: hearing, vision, cognitive, ambulatory, self-care, and independent living (Brault, 2009). Nearly one in 22 U.S. adults has an SMI (SAMHSA, 2019); however, there was a significant increase in depression from 2005 to 2015 (Weinberger et al., 2018). Compared with those with no distress, adults with severe psychological distress were 19.7 (17.8, 21.7), 13.0 (11.2, 14.9), and 11.5 (10.5, 12.6) times more likely to report impairment, or disability, in cognitive, self-care, and independent living, respectively (Lauer & Lauer, 2019).
Recovery, “positive adaptation to illness and disability, linked strongly to self-awareness and a sense of empowerment” (Hogan, 2003, p. 1469), requires developing “new meaning and purpose in one’s life as one grows beyond the catastrophic effects of mental illness” (Anthony, 1993, p. 15). In rehabilitation, adaptation to disability occurs when one develops a more well-rounded self-view, limits the effects to actual impairment (vs. spreading across one’s life) and focuses on personal assets (vs. comparing oneself to nondisabled peers; Wright, 1983). Thus, adaptation to disability, or recovery, “enables a person with [an SMI] to live a meaningful life in communities of his or her choice while striving to achieve full human potential” (Drapalski et al., 2012, p. 48).
The road to recovery can be a long and arduous process, impacted by various biological, functional, sociological, and psychological factors. Age, for example, had varying effects on recovery among people with SMI; current age was inversely related to recovery (Corrigan et al., 1999), and age at onset (i.e., before the age of 18 years) was found to moderate the relationship between symptom severity and recovery (Roe et al., 2011). Recovery is also influenced by psychiatric symptoms and cognition. Specifically, psychiatric symptom severity was inversely related to recovery, and cognitive impairment was positively related to recovery (Best et al., 2020). One’s capacity, or functional ability, to complete major life tasks (e.g., self-care, problem-solving, interpersonal, work-related, housekeeping) has been linked to sustained recovery (Bond, 1995).
People with SMI may need hospitalization or intensive outpatient treatment (Parabiaghi et al., 2006), rendering health insurance necessary to access these services (Pevalin & Goldberg, 2003). Yet, those who experience negative attitudes from society often avoid seeking treatment (Wahl, 2012) and stop taking their psychotropic medications (Sirey et al., 2001). Conversely, social support and marital status have been associated with recovery among people with SMI (Pevalin & Goldberg, 2003), with levels of perceived social support linked to magnitude of recovery (Roe et al., 2011). Anticipation of future discrimination leads to self-stigma (Quinn et al., 2015), which in turn negatively affects self-efficacy and recovery for people with SMI (Drapalski et al., 2013). Meanwhile, qualitative studies found self-efficacy (Mancini, 2007) and resilience (Edward et al., 2009) central to recovery for individuals with SMI. Moreover, self-efficacy was found to mediate the effect of social support on recovery (Thomas et al., 2016).
Active participation in major life roles has been associated with recovery among people with SMI. For students, educational participation was critical to their recovery (Cook & Solomon, 1993), whereas adults reported that engaging in meaningful work was essential to their recovery (Dunn et al., 2008). In turn, integrated employment helps people with SMI reconnect with valued roles, participate in the community, feel self-efficacious, and achieve recovery (Fieldhouse, 2012). Leisure activities can provide a sense of meaning, reduce boredom (Iwasaki et al., 2014), and guide recovery (Burns-Lynch et al., 2016). Finally, effective health self-management was also associated with better recovery (Mueser et al., 2006).
Various models have been used to measure disability and promote recovery. Stark contrasts were noted in some of the earliest models, such as the medical model, which focuses on the individual’s pathology and seeks to cure the person, compared with the social model, which focuses on the environment and seeks to eradicate oppression (Marks, 1997). Newer models sought to improve conceptual limitations; for example, the functional model, focused on “role failure,” seeks to improve the P × E (Smart, 2009), whereas the recovery model posits that “staying in control of [one’s] life” is more important than returning “to premorbid level of functioning” (Jacob, 2015, p. 117). Research on the recovery model is not only sparse but also irrelevant, focusing on treatment delivery (Noiseux et al., 2009; Synovec, 2015) or medical and functional outcomes (O’Brien et al., 2012). Due to inherent individual flaws, scholars have advocated for the integration of models in general (Engel, 1977), and in recovery specifically (Levine, 2012).
The International Classification of Functioning, Disability, and Health (ICF) is a comprehensive framework which combines concepts from several models and provides a paradigm shift in focus from illness to health (World Health Organization [WHO], 2001). The ICF consists of two main parts: (a) functioning and disability (result of the P × E) and (b) P × E contextual factors. Three subparts comprise the first major part: (a) body functions and structures are characterized by the anatomy and physiology (or psychology) of the human body, (b) activity refers to the ability (or capacity) to complete a task, and (c) participation refers to actual engagement (or performance) in life roles. In the second part, there are two subparts: (a) environmental factors are external features in society and (b) personal factors include demographics and characteristics. So far, the ICF has been used to predict psychiatric symptoms (Sanderson et al., 2008), capacity (Linden et al., 2018), and participation (Sánchez, Rosenthal, Chan, et al., 2016). Most recently, it was modified to predict post-concussion functional recovery (van Ierssel et al., 2020). Despite its versatility, the ICF has not yet been operationalized as a discrete recovery model. The purposes of this study were to examine the following: (a) the ICF’s ability to predict recovery in adults with SMI and (b) to what extent the ICF constructs, body functions, activity, environmental factors, personal factors, and participation, in the empirical model explain the variance in recovery (see Figure 1).
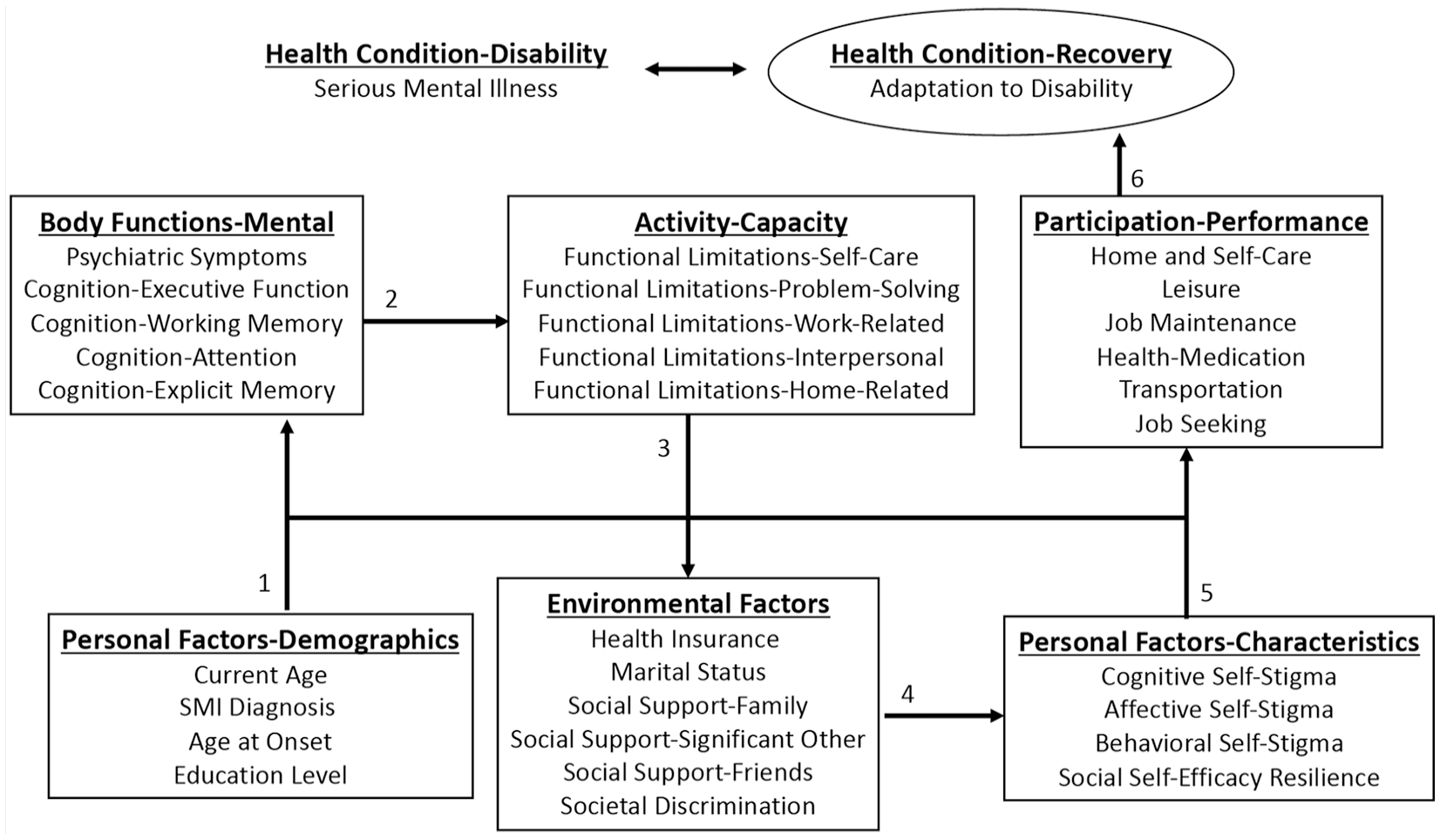
WHO’s (2001) ICF framework conceptualized as a Biopsychosocial Recovery Model for people with SMI in this study.
Method
Participants
Participants were psychosocial clubhouse members who met the following self-reported inclusion criteria: (a) ≥18 years old, (b) SMI diagnosis, and (c) ≥6th grade reading level. Most members (N = 195) expressed interest in the study and received a survey packet. Two of the 194 returned packets were missing >5% of survey items and excluded from this study. More than half the sample (51.6%) were prime working age (26–49 years), 33.9% were at least middle-age (50+ years), and 14.6% were young adults (18–25 years). SMI diagnoses were schizophrenia spectrum (26.0%), bipolar (35.4%), and major depressive (38.5%) disorders, with onset at ≤14 years (30.2%), 15 to 24 years (31.3%), 25 to 40 years (16.1%), and ≥41 years (15.1%). More than half of the participants were females (53.6%), and the majority identified as Caucasian (60.4%), followed by African American (19.3%), and Other (5.2%). Participants were fairly educated: 76.2% completed high school and nearly one-fourth (24.2%) earned a college degree. The majority of the sample was unmarried (78.6%) and unemployed (62.5%). Almost half of the participants (47.9%) received Medicare and/or Medicaid, 41.1% had none, and 10.9% had private or employer health insurance.
Measures
Various instruments and a sociodemographic questionnaire were used to measure the construct of recovery and all constructs in the ICF. See Table 1 for scale descriptive statistics.
Descriptive Statistics for Study Measures (N = 192).
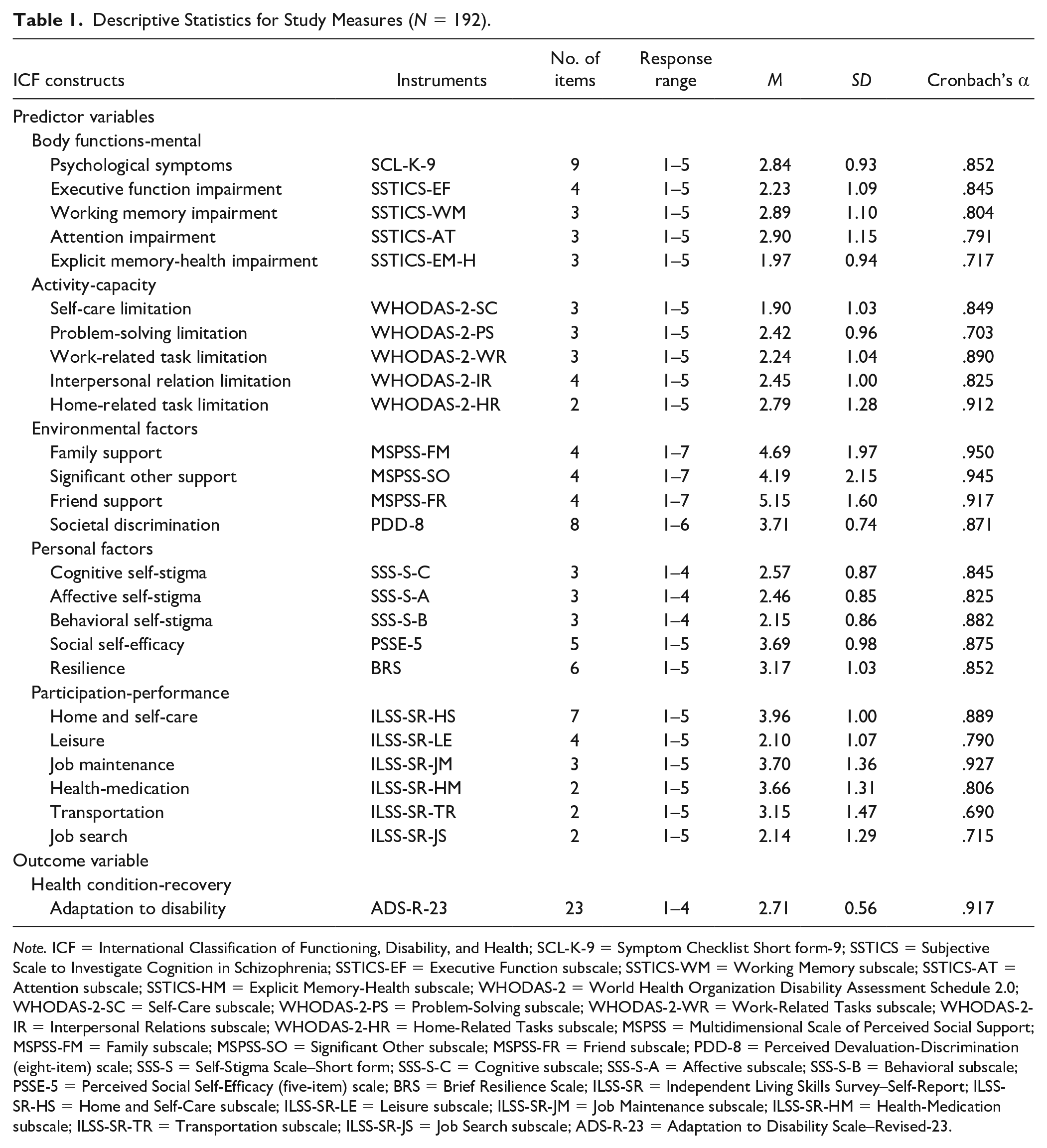
Note. ICF = International Classification of Functioning, Disability, and Health; SCL-K-9 = Symptom Checklist Short form-9; SSTICS = Subjective Scale to Investigate Cognition in Schizophrenia; SSTICS-EF = Executive Function subscale; SSTICS-WM = Working Memory subscale; SSTICS-AT = Attention subscale; SSTICS-HM = Explicit Memory-Health subscale; WHODAS-2 = World Health Organization Disability Assessment Schedule 2.0; WHODAS-2-SC = Self-Care subscale; WHODAS-2-PS = Problem-Solving subscale; WHODAS-2-WR = Work-Related Tasks subscale; WHODAS-2-IR = Interpersonal Relations subscale; WHODAS-2-HR = Home-Related Tasks subscale; MSPSS = Multidimensional Scale of Perceived Social Support; MSPSS-FM = Family subscale; MSPSS-SO = Significant Other subscale; MSPSS-FR = Friend subscale; PDD-8 = Perceived Devaluation-Discrimination (eight-item) scale; SSS-S = Self-Stigma Scale–Short form; SSS-S-C = Cognitive subscale; SSS-S-A = Affective subscale; SSS-S-B = Behavioral subscale; PSSE-5 = Perceived Social Self-Efficacy (five-item) scale; BRS = Brief Resilience Scale; ILSS-SR = Independent Living Skills Survey–Self-Report; ILSS-SR-HS = Home and Self-Care subscale; ILSS-SR-LE = Leisure subscale; ILSS-SR-JM = Job Maintenance subscale; ILSS-SR-HM = Health-Medication subscale; ILSS-SR-TR = Transportation subscale; ILSS-SR-JS = Job Search subscale; ADS-R-23 = Adaptation to Disability Scale–Revised-23.
Health condition-recovery
The 23-item Adaptation to Disability Scale–Revised (ADS-R-23; Sánchez, Umucu et al., 2016), which assesses the value change process a person experiences as a result of their SMI, was used to measure recovery. The ADS-R (Groomes & Linkowski, 2007)—revised from the Acceptance of Disability Scale (ADS; Linkowski, 1971)—was abbreviated (e.g., items specific to physical disability were removed) and modified (e.g., the term “disability” was changed to “mental health problems”) to create the ADS-R-23 and better reflect the recovery experience of people with SMI. Respondents rate their level of agreement (1 = strongly disagree to 4 = strongly agree) with each item (e.g., “Though I have mental health problems, my life is full”), and higher scores indicate better adaptation to psychiatric disability or SMI recovery. Internal consistency reliability was excellent for the ADS (.93; Linkowski, 1971), the ADS-R (.93; Groomes & Linkowski, 2007), and the ADS-R-23 (.92; Sánchez, Umucu et al., 2016).
Body functions-mental
Psychiatric symptoms
A nine-item short form of the Symptom Checklist-90–Revised (SCL-90-R; Derogatis, 1992), the SCL-K-9 (Klaghofer & Brähler, 2001), was used to assess psychiatric symptoms. Respondents rate their level of distress (1 = not at all to 5 = extremely) for each item (e.g., “Worrying too much about things”); higher scores reflect greater symptom severity. Internal consistency reliability was good (.87; Klaghofer & Brähler, 2001).
Cognitive impairments
Cognitive impairments were measured with the Subjective Sale to Investigate Cognition in Schizophrenia (SSTICS; Stip et al., 2003). The SSTICS assesses cognition in executive function, working memory, attention, explicit memory, language, and praxia. In total, 13 items were used to assess cognitive impairment in executive function (e.g., “Do you have difficulty planning out your activities as easily as you used to?”), working memory (e.g., “Do you have difficulty memorizing things, such as a grocery list or a list of names?”), attention (e.g., “Are you absent-minded or up in the clouds?”), and explicit memory-health (e.g., “Do you forget to take your medication?”). Respondents rate the frequency of their difficulty (1 = never to 5 = very often), with higher scores indicating greater cognitive impairment in the respective area. The SSTICS had adequate to marginal reliability for executive function (.67), working memory (.55), attention (.61), and explicit memory (.58; Stip et al., 2003).
Activity-capacity
Activity limitations
The World Health Organization Disability Assessment Schedule 2.0 (WHODAS-2; Üstün et al., 2010) was used to assess functional limitations. The WHODAS-2 covers six major life domains: cognition (e.g., problem-solving), mobility (e.g., standing), self-care (e.g., hygiene), getting along (e.g., interactions with others), life activities divided into two parts (i.e., household and work), and participation (e.g., community activities)—omitted for this study. Respondents rate their level of difficulty (1 = none to 5 = extreme or cannot do) for each item (e.g., “Maintaining a friendship?”); higher scores indicate greater functional limitations in that domain. The WHODAS-2 was reported to have excellent internal reliability for cognition (.94), self-care (.92), getting along (.94), and household (.92) and work (.94) activities (Üstün et al., 2010).
Environmental factors
Social support
The Multidimensional Scale of Perceived Social Support (MSPSS; Zimet et al., 1988) measures emotional support from family, friends, and significant other. Respondents rate their level of agreement (1 = very strongly disagree to 7 = very strongly agree) with each item (e.g., “There is a special person who is around when I am in need”), with higher scores reflecting higher levels of perceived social support. The MSPSS had good internal consistency reliability for family (.87), friends (.85), and significant other (.91) subscales (Zimet et al., 1988).
Societal discrimination
The Perceived Devaluation-Discrimination (eight-item) scale (PDD-8; Link et al., 2008)—abbreviated from the PDD (Link, 1987)—measures perceived societal discrimination toward people with SMI. As recommended by Sánchez (2014), terms were revised (e.g., “person with mental health problems” replaced “former mental patient”) to meet current standards. Respondents rate their level of agreement (1 = strongly agree to 6 = strongly disagree) for each item (e.g., “Most people think less of a person who has received mental health treatment”); higher scores reflect greater perceived societal discrimination. Internal consistency reliability was adequate for the PDD (.78; Link, 1987) and the PDD-8 (.74; Link et al., 2008).
Personal factors-characteristics
Self-stigma
The Self-Stigma Scale–Short Form (SSS-S; Mak & Cheung, 2010) assesses cognitive, affective, and behavioral self-stigma. Respondents rate their level of agreement (1 = strongly disagree to 4 = strongly agree) for each item (e.g., “My identity as a mental health consumer is a burden to me”), with higher scores reflecting greater self-stigma in the respective area. The SSS-S reported good internal consistency reliability estimates for the cognitive (.81), affective (.84), and behavioral (.80) self-stigma subscales (Mak & Cheung, 2010).
Social self-efficacy
The Perceived Social Self-Efficacy (five-item) scale (PSSE-5; Di Giunta et al., 2010)—created from the 25-item PSSE (H. M. Smith & Betz, 2000)—assesses self-beliefs in managing interpersonal relations. Respondents rate their level of perceived ability (1 = not well at all to 5 = very well) for each item (e.g., “actively participate in group activities?”); higher scores indicate greater perceived social self-efficacy. Internal consistency for the PSSE-5 was acceptable (.76; Di Giunta et al., 2010) yet lower than for the PSSE (.94; H. M. Smith & Betz, 2000).
Resilience
The Brief Resilience Scale (BRS; B. W. Smith et al., 2008) assesses a person’s ability to bounce back from stressful situations (i.e., resilience). Respondents rate their level of agreement (1 = strongly disagree to 5 = strongly agree) for each item (e.g., “I tend to bounce back quickly after hard times”), with higher scores indicating greater levels of resilience. Internal reliability for the BRS ranged from good (.80) to excellent (.91; B. W. Smith et al., 2008).
Participation-performance
Participation
Active participation in life roles were assessed with the Independent Living Skills Survey–Self-Report (ILSS-SR; Wallace et al., 2000). The ILSS-SR spans 10 major life areas; 20 items were used to measure participation in home and self-care, leisure, job maintenance, health-medication, transportation, and job seeking. Respondents rate their level of engagement (1 = never to 5 = always; informant version: ILSS-I) for each item (e.g., “Use public buses, trains, or subway?”); higher scores indicate greater participation. Reliability for ILSS-SR subscales ranged from poor (.44, transportation) to excellent (.90, job seeking; Wallace et al., 2000).
Procedure
Upon receiving Institutional Review Board (IRB) approval, study information was disseminated to four psychosocial rehabilitation clubhouses in Texas and Wisconsin. Interested participants were administered, by the author, paper survey packets with numbered envelopes; responses were kept confidential. Average completion time was approximately 45 min. For their time spent on the study, participants were provided a monetary gift card as compensation.
Data Analysis
Simple imputation using regression to compute estimations based on values of related items within the measure was applied to replace missing data (<5%). Imputation is preferred over case deletion because sample size is maintained and sample representativeness is unaffected (Fox-Wasylyshyn & El-Masri, 2005). Data were analyzed with IBM SPSS Statistics (Version 25). G*Power (Faul et al., 2009) was used to conduct an a priori power analysis for the total R2 value for a multiple regression analysis with 32 predictor variables, power = .80, alpha = .05, and yielded a minimum sample of 193 for a medium effect size (f2 = .15; Cohen, 1988). A post-hoc power analysis (for model, N = 192, α = .05, f2 = .15) reached 0.7995860 (Faul et al., 2009). In addition, four variables were dummy coded (1 = group membership or 0 = no membership; Pedhazur, 1997) because the data were categorical: SMI diagnosis (schizophrenia, bipolar, depression), health insurance (insured), marital status (married), and employment status (employed).
Hierarchical regression analysis (HRA) was conducted with recovery as the dependent variable and six sets of predictors entered in sequential steps: (a) personal factors-demographics, (b) body functions-mental, (c) activity-capacity, (d) environmental factors, (e) personal factors-characteristics, and (f) participation-performance. Order entry was determined causally, temporally, and logically (Cohen et al., 2003). For example, in adults with SMI, demographic factors (age at onset) antedate mental functions (psychiatric symptoms), which in turn affect functioning (interpersonal relations) and impact external experiences (societal discrimination), which influence personal characteristics (social self-efficacy), which then restricts participation (employment) and ultimately impedes recovery. HRA is particularly useful when more than one predictor variable is used to measure a construct (Hoyt et al., 2006), as the change in R2 (ΔR2) shows the combined contribution (of the variable set) in predicting (variance) the criterion, whereas sr2 shows the unique contribution (of each variable) of variance in (predicting) the criterion.
Results
Correlations were computed for all potential variables. For primary SMI diagnosis (i.e., depression, bipolar, and schizophrenia), only bipolar disorder was correlated with recovery (r = −.15) and thus selected for use in the HRA. Correlation matrices for all variables are presented in Table 2 (Pearson product-moment correlations) and Table 3 (Spearman rank-order correlations).
Pearson Product-Moment Correlations, Means, and Standard Deviations for Variables Used in Hierarchical Regression Analyses.
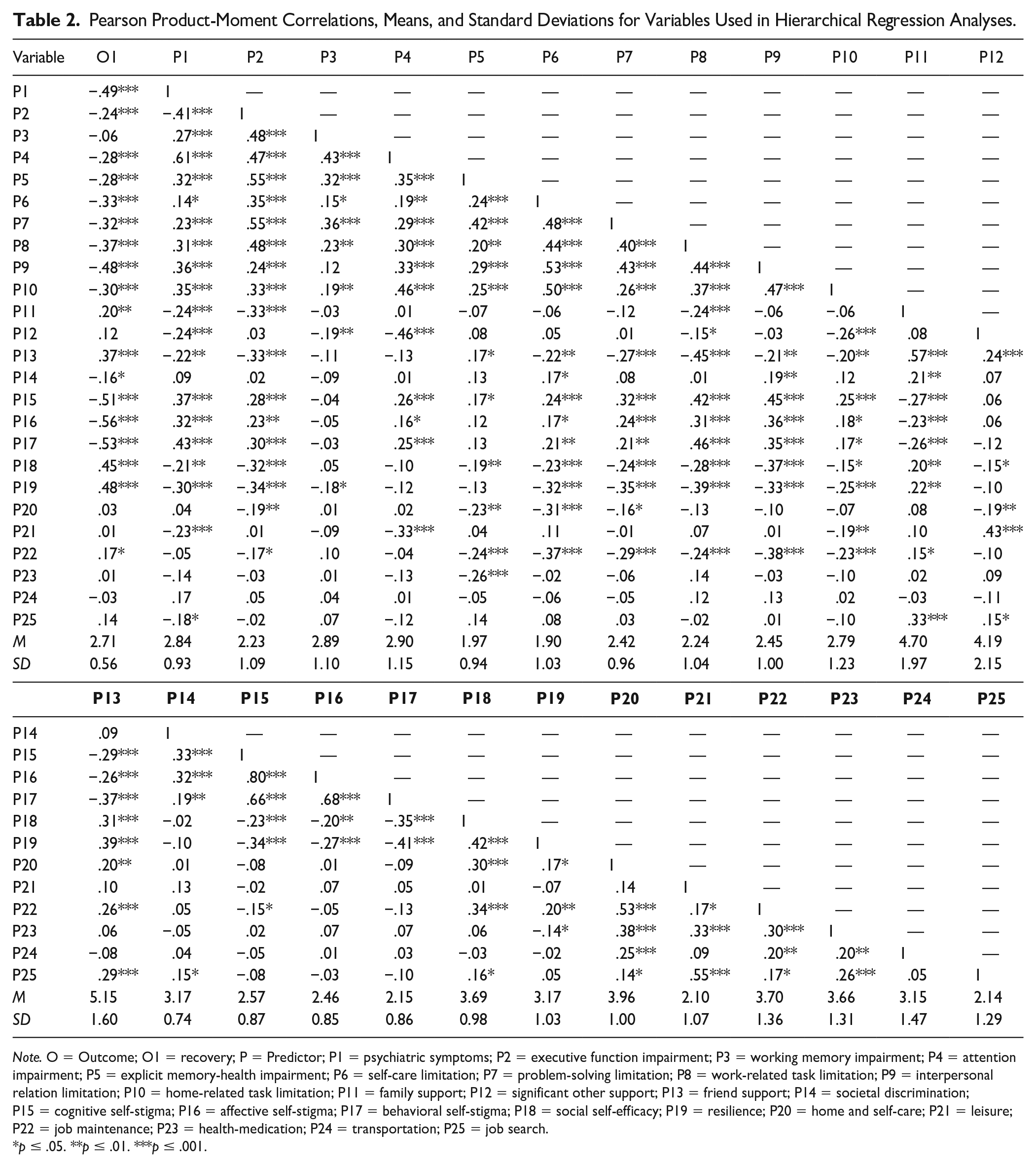
Note. O = Outcome; O1 = recovery; P = Predictor; P1 = psychiatric symptoms; P2 = executive function impairment; P3 = working memory impairment; P4 = attention impairment; P5 = explicit memory-health impairment; P6 = self-care limitation; P7 = problem-solving limitation; P8 = work-related task limitation; P9 = interpersonal relation limitation; P10 = home-related task limitation; P11 = family support; P12 = significant other support; P13 = friend support; P14 = societal discrimination; P15 = cognitive self-stigma; P16 = affective self-stigma; P17 = behavioral self-stigma; P18 = social self-efficacy; P19 = resilience; P20 = home and self-care; P21 = leisure; P22 = job maintenance; P23 = health-medication; P24 = transportation; P25 = job search.
p ≤ .05. **p ≤ .01. ***p ≤ .001.
Spearman’s Correlations for Categorical Variables Used in Hierarchical Regression Analyses.
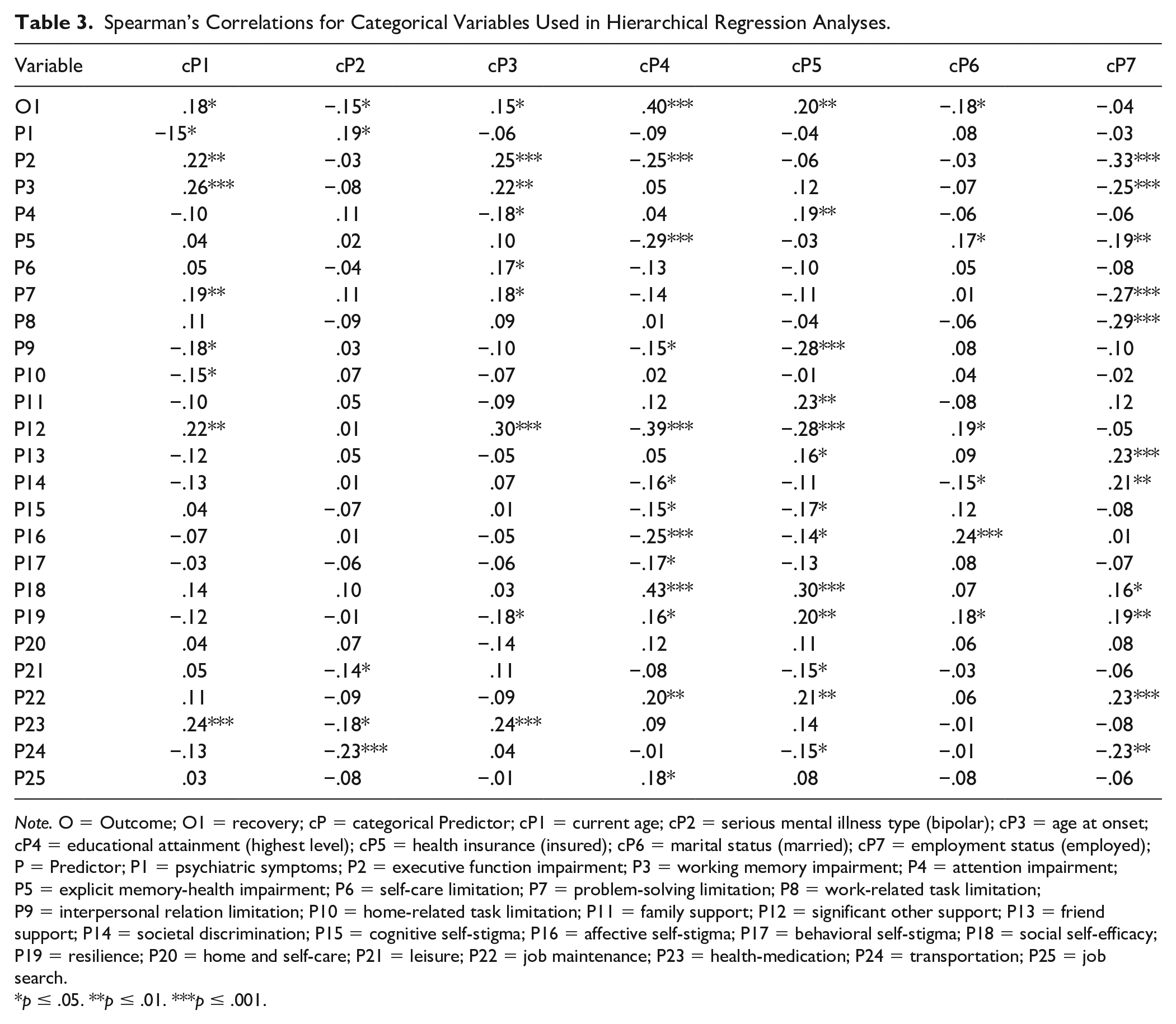
Note. O = Outcome; O1 = recovery; cP = categorical Predictor; cP1 = current age; cP2 = serious mental illness type (bipolar); cP3 = age at onset; cP4 = educational attainment (highest level); cP5 = health insurance (insured); cP6 = marital status (married); cP7 = employment status (employed); P = Predictor; P1 = psychiatric symptoms; P2 = executive function impairment; P3 = working memory impairment; P4 = attention impairment; P5 = explicit memory-health impairment; P6 = self-care limitation; P7 = problem-solving limitation; P8 = work-related task limitation; P9 = interpersonal relation limitation; P10 = home-related task limitation; P11 = family support; P12 = significant other support; P13 = friend support; P14 = societal discrimination; P15 = cognitive self-stigma; P16 = affective self-stigma; P17 = behavioral self-stigma; P18 = social self-efficacy; P19 = resilience; P20 = home and self-care; P21 = leisure; P22 = job maintenance; P23 = health-medication; P24 = transportation; P25 = job search.
p ≤ .05. **p ≤ .01. ***p ≤ .001.
HRA results, including ΔR2, unstandardized regression coefficients (B), standard errors (SE B), and standardized coefficients (β) for the predictor variables are presented in Table 4.
Hierarchical Multiple Regression Analysis for Prediction of Recovery (N = 192).

Note. SMI = serious mental illness.
p ≤ .05. **p ≤ .01. ***p ≤ .001.
Personal factors-demographics (current age, SMI diagnosis [bipolar], age at onset, and education level) were entered first. This set explained 25% of the variance in recovery, R2 = .251, F(4, 182) = 15.269, p < .001. Bipolar diagnosis was negatively associated with recovery, β = −.159, t(186) = −2.46, p = .015, whereas education level was positively associated with recovery, β = .439, t(186) = 6.587, p < .001.
In the second step, variables related to body functions-mental (psychiatric symptoms and cognitive impairments) were entered. This variable set explained 16% more variance beyond the variables from Step 1, R2 = .415, ΔR2 = .163, F(5, 177) = 9.872, p < .001. Psychiatric symptoms were negatively associated with recovery, β = −.384, t(186) = −4.92, p < .001.
Variables related to activity-capacity (functional limitations) were entered in Step 3. The activity set explained 13% more variance beyond the variables from previous steps, R2 = .541, ΔR2 = .127, F(5, 172) = 9.521, p < .001. Work-related, β = −.212, t(186) = −3.09, p = .002, and interpersonal, β = −.147, t(186) = −1.99, p = .048, limitations were inversely related to recovery.
In Step 4, environmental factors (health insurance [insured], marital status [married], social support, and societal discrimination) were entered. This variable set explained 7% more variance beyond the variables from prior steps, R2 = .611, ΔR2 = .069, F(6, 166) = 4.927, p < .001. Significant other support was positively associated with recovery, β = .287, t(186) = 3.72, p < .001.
Personal factors-characteristics (self-stigma, social self-efficacy, and resilience) were entered in Step 5. These variables explained 11% more variance beyond those from prior steps, R2 = .716, ΔR2 = .105, F(5, 161) = 11.869, p < .001. Affective self-stigma was negatively associated with recovery, β = −.232, t(186) = −2.89, p = .004, whereas social self-efficacy, β = .194, t(186) = 3.37, p = .001, and resilience, β = .192, t(186) = 3.33, p = .001, were positively associated with recovery.
In the final step, variables related to participation-performance (employment status [employed] and engagement in life roles) were entered. This variable set explained 3% more variance beyond the variables from all prior steps, R2 = .747, ΔR2 = .032, F(7, 154) = 2.759, p = .010. Employment status was negatively related to recovery, β = −.144, t(186) = −2.68, p = .008. The final regression model accounted for 75% (a large effect size; Cohen, 1988) of the variance in recovery. Controlling all factors, the significant predictors of recovery were current age, SMI diagnosis, education level, psychiatric symptoms, impairments in executive function and explicit memory-health, self-care limitation, marital status, significant other support, cognitive and affective self-stigma, social self-efficacy, resilience, and employment status.
Discussion
Recovery is a major goal in rehabilitation; however, exploring the role of biopsychosocial factors in facilitating recovery is not always considered. This is the first study to evaluate WHO’s ICF for recovery in adults with SMI. The regression equations derived from the data collected indicate that recovery can be predicted from the group of 32 independent variables examined for people with SMI. The model allows for prediction of 75% of the variance in recovery scores, with variables from all ICF constructs accounting for variance in recovery.
Clinical Implications
Findings from this study suggest several relevant implications for directing and informing clinical practices in rehabilitation counseling. By order of salience, the following were related to recovery: higher levels of significant other support, education, executive function impairment, and social self-efficacy; primary, non-bipolar SMI diagnosis; greater resilience; lower levels of explicit memory-health impairment, affective self-stigma, and cognitive self-stigma; being younger; fewer self-care limitations; less severe psychiatric symptoms; and being unemployed and unmarried.
Personal factors-demographics were associated with recovery. Contrary to prior findings, older age (Salzer et al., 2018) and bipolar disorder (Strauss et al., 2012) were associated with lower levels of recovery in this study. People are living longer and working well-past traditional retirement age. Consumers with bipolar disorders (Sánchez, 2018) and older adults (Cichy et al., 2017) have unique vocational needs; thus, rehabilitation counselors should consider impairment and age differences when designing employment service programs (O’Neill et al., 2017). In line with prior research (Kane et al., 2016), education level was directly related to recovery in this study. Students with SMI often struggle to meet academic requirements while coping with their mental illness (Shor, 2017). Supported education (SEd) was developed to assist people with SMI integrate into postsecondary institutions (Unger, 1989) and complete their education or vocation goals (Unger et al., 1991). While completion rates for students with SMI in SEd are higher than (Parten, 1993) or equal to (Unger et al., 2000) those of peers without mental illness, some exhibit low participation (Frankie et al., 1996). Motivational interviewing can help increase retention in SEd programs and completion of postsecondary educational or vocational programs (Manthey, 2011).
Body functions-mental was a significant predictor of recovery. In the present study as with previous research, psychiatric symptom severity (Chang et al., 2013) and explicit memory-health impairment (Wingo et al., 2009) were inversely associated with recovery. Contrary to prior study findings (Martínez-Arán et al., 2002), impairment in executive function was positively related to recovery in this study. This discrepancy may be related to the inverse relationship between mood symptoms and cognitive impairments (Harvey, 2011). Thus, treatment should aim to ameliorate symptoms and increase strategies to compensate for health-related memory impairment to better facilitate recovery. Psychotropic medications are established first-line treatment for controlling psychiatric symptoms (Stern et al., 2018); however, nonadherence to prescriptions is common among people with SMI and the leading cause of relapse in mental illness (Barkhof et al., 2012). Systematic and meta-analytic research evidence supports the use of psychoeducation (Zhao et al., 2015), motivational interviewing (Wong-Anuchit et al., 2018), and behavioral strategies (Kreyenbuhl et al., 2016) to improve medication adherence for people with SMI.
Activity-capacity was also a significant predictor of recovery. Recovery was inversely related to self-care limitations and corresponds with the literature (Bond, 1995; Harvey et al., 2007). Active engagement in self-care has been associated with greater medication adherence and mental health (Bible et al., 2017). Rehabilitation counselors should incorporate interventions to increase self-care function to promote recovery. An intervention that combined skills training and health management was found to improve social functioning and independent living skills among older adults with SMI (Bartels et al., 2004). Telerehabilitation technologies have been shown to improve self-care among persons with SMI (Forducey et al., 2012) and should be considered for clients who live in rural areas or for whom transportation proves a barrier.
Environmental factors were associated with recovery. Although perceived social support from a significant other predicted recovery and aligns with prior findings (Boucher et al., 2016; Johnson et al., 2003), married adults with SMI reported lower levels of recovery, which contrasts with previous research (e.g., Farina et al., 1963). One reason for this unexpected finding may be that perceived quality of support has more influence on recovery than marital status (Goering et al., 1992). Level of, and satisfaction with, partner support directly correlated with recovery in adults with SMI (Ezquiaga et al., 1998). Rehabilitation counselors working with consumers who are married and rate support from their spouse low should consider couple-based interventions to improve support quality. For example, partner-assisted interventions (e.g., partner serves as a coach) could be used to assist with making changes to improve mental health, disorder-specific interventions (e.g., depression) could be used to teach the couple adaptive interaction patterns to reduce psychiatric (e.g., depressive) symptoms, and couple therapy (e.g., cognitive-behavioral) could be used to improve partner interactions and reduce relationship distress (Whisman & Baucom, 2012).
Personal factors-characteristics were also associated with recovery. In line with prior findings, social self-efficacy (Mancini, 2007) and resilience (Edward et al., 2009) were positively correlated with recovery in this study. Meanwhile, cognitive and affective self-stigma were inversely associated with recovery. In a recent study, internalization of stigmatizing beliefs (cognitive self-stigma) resulted in decrement of self-esteem (affective self-stigma) and impeded recovery (Cunningham & Lucksted, 2017). Due to the interrelated relationships among self-efficacy, resilience, and self-stigma, interventions should seek to increase self-efficacy, promote adaptive coping, and replace negative thoughts. One option, Recovery Camp, a therapeutic recreation program designed to facilitate “a sense of purpose toward overcoming challenges brought about by living with a mental illness” (Moxham et al., 2015, p. 61), was found to improve social self-efficacy and resilience. Alternatively, Narrative Enhancement and Cognitive Therapy (NECT) combines (a) psychoeducation to debunk stigmatized myths regarding mental illness and recovery, (b) cognitive restructuring to challenge negative self-beliefs and teach adaptive skills, and (c) psychotherapy to enhance the construction of personally useful stories (narratives) of oneself, one’s mental illness, and oneself in relation to one’s mental illness (Yanos et al., 2011), and it was successful in increasing self-esteem and reducing self-stigma in adults with SMI (Hansson et al., 2017; Roe et al., 2014). NECT was also found to increase levels of hope agency (Roe et al., 2014), which helps foster resilience (Ong et al., 2006).
Participation-performance was a significant predictor of recovery. Contrary to research evidence, being employed (Bond et al., 2001; Saavedra et al., 2016) had an inverse association with recovery in the present study. This discrepancy makes sense, however, if participants felt demoralized (Link, 1987), were underemployed (Cook, 2006), experienced work-related stress (Honey, 2004), or perceived their work as insignificant (Dunn et al., 2008). People with SMI are less likely to be hired into executive positions based on employer “perceptions of potential poor work performance” (Glozier, 1998, p. 793) and more likely to be paid lower mean wages than those with no mental illness (Baldwin & Marcus, 2006). Conversely, employment of people with SMI is most associated with positive employer attitudes, which are related to company size, past positive contact with people with SMI, and higher education level of employer (Mangili et al., 2004). Rehabilitation counselors should be cognizant of societal stigma, understand its negative impact on employees with SMI, and attempt to reduce discrimination by employers and within organizations. In two studies, imagined contact was effective in improving attitudes in work situations: “expected work-related outcomes and support for the rights of people with disabilities, via enhancing the belief in performance level” (Carvalho-Freitas & Stathi, 2017, p. 256). Furthermore, rehabilitation counselors should work with consumers to carefully consider if, when, and how to disclose their SMI at work (MacDonald-Wilson, 2005) and identify types of employment that align with their values and would provide a sense of purpose (Mancini et al., 2005). Vocational services should build work self-efficacy, increase work motivation, teach work-related skills, assess person-job fit, create opportunities for advancement, be a source of social support, and provide access to consumer-oriented programs (Dunn et al., 2010). Finally, being that recovery is not predicted by employment, they “should be viewed as independent and different outcomes,” and thus, rehabilitation counselors should include both employment and recovery as treatment outcome measures for vocational services (Young et al., 2019, p. 502).
Research Implications
Findings from this study support the use of the ICF as a model to predict recovery for adults with SMI. Although most of the associations between predictors (e.g., psychiatric symptoms, education) and recovery were in the expected directions, some were surprising. First, impairment in executive function was positively related to recovery. Examining the effect of treatments such as cognitive remediation—found to reduce psychiatric symptoms and improve cognitive functioning in people with SMI (Deckersbach et al., 2010)—on recovery seems warranted and relevant due to potential contraindication. Second, being married was associated with lower levels of recovery. Future studies should explore the effects that marriage duration (Cheung, 2000) and marital quality (Cullen et al., 2017) have on recovery for people with SMI. Third, participants who were employed reported lower levels of recovery. It would be beneficial to examine how perception of employer stigma (Link, 1987), meaningfulness of work (Leufstadius et al., 2008), and type of employment (O’Neill et al., 2017) impact recovery. Finally, HRA only permitted testing direct relationships between predictor variables and the criterion. While path analysis would allow for testing of both direct and indirect relationships, there were too many variables of interest in proportion to participants (Pedhazur, 1975). Recruitment of large samples in future studies would allow for utilization of such analytic methods. Longitudinal research is also recommended to ascertain causal relationships between predictor variables and the criterion. Subsequent to assessing recovery, the ICF could be used to assess more specific rehabilitation-related outcomes for adults with SMI, such as vocational recovery (Glässel et al., 2011).
Other interesting developments included predictor variables that were insignificant when first entered into the model but then became significant when additional variables were entered. This is most likely due to suppressor effects, “a variable [i.e., suppressor] which increases the predictive validity of another variable (or set of variables) by its inclusion in a regression equation” (Conger, 1974, pp. 36–37). For example, classical suppression would explain why support from significant other, a variable that is uncorrelated with the criterion but significantly correlated with another predictor variable, increased the predictive power of the HRA model (Horst, 1941). In reciprocal suppression, two predictors that either (a) correlate negatively with the criterion but positively with one another (e.g., cognitive and affective self-stigma) or (b) correlate positively with the criterion but negatively with one another (e.g., age and resilience), will increase both of their beta weights (Watson et al., 2013). With cross-over suppression, if all three variables (i.e., both predictors and the criterion) positively correlate with one another, the weight for the stronger predictor will increase (e.g., social self-efficacy) and the sign of the weaker predictor will change (e.g., age; Watson et al., 2013). In the future, suppressor variables should be considered along with mediator and confounding variables (MacKinnon et al., 2000).
Limitations
The study findings should be considered within the following limitations. The ICF was not designed to be a discrete model but rather a framework. Despite some studies validating the ICF to conduct various types of evaluations (e.g., vocational rehabilitation; Saltychev et al., 2013) and to assess different outcomes (e.g., work participation; Martins, 2015), the ICF is still relatively new and there are more established models to measure psychosocial adaptation, or recovery. Survey administration occurred in-person at each agency during operating hours; thus, members not in regular attendance may have been excluded (Sánchez, Rosenthal, Tansey, et al., 2016). Finally, self-report data were used, which may adversely affect the reliability or validity of responses; however, self-report measures have proved useful for assessing psychiatric symptoms (Eisen et al., 2000) and functional outcomes (O’Malia et al., 2002) in people with SMI.
Conclusion
This was the first study to apply the ICF to better understand recovery in a sample of adults with SMI and provides empirical support for its use as an interactive framework for predicting recovery, which consists of multiple latent variables, including biopsychosocial factors. The final model accounted for 75% of the variance in recovery; social support, education, and social self-efficacy were the strongest predictors. Further research is needed to explain the complex interactive relationships of factors influencing recovery for adults with SMI.
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The work for this manuscript was funded, in part, by the Rehabilitation Research and Training Center on Evidence-Based Practice in Vocational Rehabilitation (RRTC-EBP VR) at the University of Wisconsin-Madison and the University of Wisconsin-Stout with funding provided by the U.S. Department of Health and Human Services, National Institute on Disability, Independent Living, and Rehabilitation Research (H133B100034; PI Fong Chan) and by the Psychosocial Rehabilitation and Health-and-Related Disparities Research Lab (PsyR HaRD) at The University of Iowa (COE4724; PI Jennifer Sánchez). The ideas, opinions, and conclusions expressed, however, are those of the author and do not represent recommendations, endorsements, or policies of the sponsors. The sponsors had no involvement in the study design, data collection, or write up.