
Abstract
The purpose of the study was to examine whether disability acceptance, hope, and resilience mediate the relationship between functional disability and life satisfaction in people with a lived experience of an infectious viral disease (i.e., polio and postpolio syndrome [PPS]). Participants consisted of 157 individuals diagnosed with polio or PPS who were recruited from two community support organizations in Taiwan. Participants completed self-report questionnaires. Data were analyzed with a simultaneous regression analysis. The tri-mediation model indicated that disability acceptance, hope, and resilience were associated with life satisfaction, accounting for a large effect size of 46% of the variance in the life satisfaction scores. The direct effect of functional disability on life satisfaction became insignificant when the mediators were controlled for in the model. Hope, disability acceptance, and resilience were found to fully explain the association between functional disability and life satisfaction. This study demonstrated that positive psychosocial factors might help to buffer the indirect and direct negative effects of functional disability on life satisfaction. Implications of these findings for future research and clinical practice when supporting individuals with a lived experience of an infectious viral disease, including COVID-19, are discussed.
Keywords
According to the World Health Organization (2020), polio remains a significant health burden as there are 12 to 20 million polio survivors worldwide. In the United States alone, there are about one million people who have some type of polio-related impairment (National Institute of Neurological Disorders and Stroke [NINDS], 2020). In Taiwan, there were approximately 8,000 people diagnosed with polio between 1955 and 1985 (Centers for Disease Control and Prevention [CDC], 1982; Zhang, 2013). Polio, or poliomyelitis, is an acute viral infection that affects the motor neurons located in the spinal cord, brain stem, or neuromuscular system (Falvo, 1999; NINDS, 2020; Salcido, 2000). Approximately 25% to 40% of the individuals diagnosed with polio gradually develop new manifestations of poliomyelitis decades later in life (NINDS, 2020). The late onset of symptoms in polio survivors is known as postpolio syndrome (PPS). PPS has been described as the degeneration of oversized motor units that were produced after recovery from poliomyelitis. Common PPS symptoms include renewed muscle weakness, fatigue, sleep disturbance, pain, and cold intolerance (Farbu, 2010). These symptoms are severe enough to affect mobility, day-to-day functioning, and activities (Burger et al., 2010; Lund & Lexell, 2009; Perry & Clark, 1997), which consequently diminish life satisfaction (Atwal et al., 2013; Harrison & Stuifbergen, 2006; Jacob & Shapira, 2010; Kemp & Krause, 1999).
The polio epidemic that occurred during the 1940s to 1950s caused physical disability in millions of young children (Elrod et al., 2005). By the mid-1960s, polio vaccines were invented in industrialized countries and poliomyelitis became almost obsolete. Today, the contagious infection persists as a major public health risk in underdeveloped countries where the vaccine is not widespread, and often individuals may have polio without even realizing it (Pierini & Stuifbergen, 2010). Although the polio virus has disappeared in most countries, the persistent problems reported by individuals with a history of polio and the new problems reported by individuals with a confirmed or suspected diagnosis of another contagious disease (e.g., Ebola, COVID-19) remain a serious concern among disability and rehabilitation professionals. The field of rehabilitation counseling has long recognized the functional disability impact of contagious diseases, and these diseases were included under Section 504 of the Rehabilitation Act (Eisenberg, 1988). Investigation of factors influencing psychosocial adjustment of survivors of the polio epidemic, one of the most feared diseases in the early 1950s, can provide valuable information to help rehabilitation counselors work more effectively with individuals with chronic health conditions and disabilities during and after the coronavirus disease 2019 (COVID-19) pandemic to improve their physical health, mental health, and life satisfaction.
Rehabilitation counseling researchers have long recognized the need to consider positive human traits and supportive environments in the development of effective rehabilitation counseling practices (Chan et al., 2013; Wright, 1983). Positive human traits that have been frequently used to predict life satisfaction of people with chronic health conditions and disabilities include disability acceptance, hope, and resilience (Catalano et al., 2011; Chan et al., 2013; Ferrin et al., 2011; Moser et al., 2020). It is hypothesized that these factors may also have an influence on the life satisfaction of people with polio. The following sections will provide a review of the research literature related to disability acceptance, hope, and resilience.
Disability Acceptance
The concept of disability acceptance was advanced by Beatrice Wright (1983) based on her coping versus succumbing frameworks that involve accepting one’s disability as nondevaluating. Wright (1983) postulates that disability acceptance is a process of reevaluation of values and involves four value changes: (a) enlarging the scope of values is conceptualized as having an emotional realization that other values are possible and can be realized, even with the limitations of the disability; (b) containing the effects of the disability is defined as learning new skills and approaches to overcome limitations of the disability; (c) subordinating the physique is described as changing from overemphasizing physical appearance to positive personality traits; and (d) transforming comparative-status values to asset values is stated as moving away from external standards toward personal assets to meet situational demands. Disability acceptance (self-acceptance) occurs when an individual begins to modify core values, reinvest in life and career goals, and incorporate disability into their self-identity (Chan et al., 2013; Ferrin et al., 2011; Livneh & Antonak, 1994). Disability acceptance has been found to be related to self-esteem, psychological well-being, and life satisfaction (Ferrin et al., 2011; Smedema et al., 2013).
Li and Moore (1998) conducted a correlational study to examine the relationship between disability acceptance and self-esteem in a sample of people with disabilities receiving state vocational rehabilitation services and found a correlation of .53 (a large effect size). Ferrin et al. (2011) conducted a cross-sectional survey study with a sample of Canadian adults with spinal cord injuries and found a significant relationship between disability acceptance, self-esteem, and life satisfaction. Lin et al. (2013) conducted a confirmatory factor analysis study in a sample of Taiwanese adults with spinal cord injuries and reported a medium effect size for the relationship between disability acceptance, functional independence, and life satisfaction. Maynard and Roller (1991) indicated people with PPS achieve disability acceptance when they have a better understanding of their levels of functioning and recognize there is no need to conceal their polio-related disability. Westbrook and McIlwain (1996) investigated the emotional reactions to having PPS and found that accepting the diagnosis was associated with the use of positive, adaptive coping strategies.
Hope
Hope is an important construct in positive psychology. Snyder and colleagues conceptualized hope as a cognitive construct that reflects people’s motivation and capacity to strive toward personally relevant goals (Shiri et al., 2012; Snyder et al., 1991, 2000, 2006). Hope is defined as a positive motivational state that is based on the interaction between agency (goal-directed energy) and pathways (planning to meet goals). Agency thinking is the perceived capacity to use imagined routes to goals and is the motivational component of the model (Snyder et al., 2000). Pathways thinking is defined as people’s belief that they can create plausible mental routes to desired goals (Snyder et al., 2006). According to Snyder, hopeful people are those who are persistent and creative in pursuing their goals. Pleeging and colleagues (2019) extracted 34 research studies from the World Database of Happiness to examine the existing literature on the relations between hope and subjective well-being. Their literature review indicated that the association of subjective well-being with the agency component of cognitive hope is stronger than that with the pathways component. They also evaluated the magnitude of the zero-order correlation coefficients across the 34 studies. Their correlation analyses indicated that cognitive and emotional hope have a relatively strong positive relationship with subjective well-being. There is also strong evidence in the rehabilitation literature to support the positive relationship between hope and life satisfaction among people with chronic illnesses and disabilities (Blake et al., 2018; Chan et al., 2013; Kashdan et al., 2002; Smedema et al., 2013, 2014). A study investigated the effects of hope on individuals with PPS in comparison with healthy controls (Shiri et al., 2012). The results indicated that hope was correlated with mental and physical health–related quality of life for individuals with PPS and not for the control group. Longitudinal research has demonstrated hope as one of the important determinants for life satisfaction (Marques et al., 2011, 2013). A recent scoping review demonstrated that hope is positively related to life satisfaction and negatively associated with negative disability adjustment among people with PPS (Sulaiman et al., 2019).
Resilience
Positive coping or “bouncing back quickly” from significant adversity to move on with life aligns with resilience concepts (Dyer & McGuinness, 1996; Todd & Worell, 2000). Resilience continues to thrive as a psychosocial asset within the broader psychology and rehabilitation literature (Catalano et al., 2011; Chou et al., 2013; White et al., 2010). The construct of resilience has been explored among people with physical disabilities, and resilience has been found to be inversely associated with depression and positively correlated with life satisfaction in this group (Catalano et al., 2011; Quale & Schanke, 2010; White et al., 2010). A recent study investigated the relationship between resilience factors and depression in a large sample of older adults with PPS (Pierini & Stuifbergen, 2010). The results of a regression analysis indicated that four of seven resilience variables accounted for 30% of the variance in depressive symptoms.
Study Purpose
Because polio is often thought of as a disability of the past, rehabilitation counselors may lack the knowledge and training in biopsychosocial intervention strategies for the adults now exhibiting PPS symptoms in their late forties or beyond (Halstead, 2011). In addition, there is a paucity of research on positive psychological factors that mediate the relationship between functional disability and life satisfaction among people with PPS in Taiwan. Additional research on both functional disability and positive psychosocial factors such as disability acceptance, hope, and resilience is critical to inform rehabilitation professionals on how to best provide biopsychosocial interventions to persons with PPS and other infectious viral disease survivors to improve life satisfaction. The purpose of this study was to examine whether disability acceptance, hope, and resilience mediate the relationship between functional disability and life satisfaction in a sample of Taiwanese adults with a lived experience of an infectious viral disease. Specifically, we hypothesized that disability acceptance, hope, and resilience mediate the relationship between functional disability and life satisfaction among people with polio or PPS.
Method
Procedures
An a priori power analysis was conducted to determine the appropriate sample size for the present study using the G*Power software (Faul et al., 2009). With a power at .95, an alpha level of .05, and four predictors, 129 participants were found to be required for a medium effect size (f 2 = .15; Cohen, 1992), a sample size that was exceeded in the present study. We selected a medium effect size based on published positive psychology studies in rehabilitation counseling (Chan et al., 2013; Sung et al., 2013). Data for all predictor and criterion variables were screened for missing data, outliers (using Cook’s distances), and multicollinearity, and a simple imputation method using regression was utilized to replace any missing data.
Adults with a lived experience of polio were recruited from two community support organizations for people with poliomyelitis in Taiwan. Information about the study was distributed to members with help from staff of the two organizations. Participants signed a consent form before participating in the study. Staff provided paper-and-pencil self-administered surveys to participants, and assistance for completing the survey if needed. Participants received a gift card equivalent to US$4 upon completion of the survey.
Participants
One hundred and fifty-seven individuals with polio and/or PPS were recruited to participate in this study. Participants included 84 (53.5%) males and 73 (46.5%) females who ranged in age from 19 to 63 (M = 44.70, SD = 0.65) years. A majority of the participants were either married (45.9%) or single (45.2%), with 3.8% divorced, 1% widowed, and 2.5% co-habituating; three participants (1.5%) did not report their marital status. The educational attainment of participants included those who had not completed high school (22.3%), had obtained a high school diploma (36.9%), had obtained an associate degree/bachelor degree (36.3%), and had obtained graduate degrees (3.1%); two persons did not report their level of education. In addition to the PPS, participants reported secondary health conditions, including fatigue (64.3%), lordosis (63.1%), obesity (50.3%), muscle weakness (48.4%), pain (40.1%), muscle contracture (39.2%), carpel tunnel syndrome (36.3%), and temperature intolerance (36.3%).
Measures
All of the psychological measures in the present study had been translated into traditional Chinese using the back-translation method (Van de Vijver & Hambleton, 1996). Three experts reached consensus for the item translation and adjustment.
The World Health Organization Disability Assessment Schedule (WHODAS 2.0)
The Chinese version of the WHODAS 2.0 thirty-six-item scale was utilized in this study. A few items were slightly adjusted to fit the Taiwanese culture. Adjustment was based on the consensus of three experts. The WHODAS 2.0 is a 36-item measure that was developed by the World Health Organization (Üstün et al., 2010) to assess activity limitations and participation restrictions experienced by an individual irrespective of medical condition (e.g., “How much difficulty have you had in the past 30 days in standing for long periods such as 30 minutes?”). Each item is rated on a 5-point Likert-type scale, ranging from 1 (none) to 5 (extreme or cannot do). Functional disability scores are calculated by averaging ratings across the WHODAS items. The average score ranges from 1 to 5, with higher scores indicating a more severe level of disability. According to the WHODAS manual, the internal consistency reliability (Cronbach’s α) of the WHODAS 2.0 thirty-six-item version was computed to be .98 (Üstün et al., 2010). The Cronbach’s alpha for the present study was computed to be .95.
The Satisfaction With Life Scale (SWLS)
The SWLS was developed and validated by Diener et al. (1985) to measure life satisfaction in the general population. It consists of five items such as “In most ways my life is close to my ideal” and “I am satisfied with my life.” Each item is rated on a 7-point Likert-type scale from 1 (strongly disagree) to 7 (strongly agree), with total scores ranging from 5 to 35 and higher scores indicating more life satisfaction. Diener et al. (1985) reported acceptable levels of internal consistency reliability estimates ranging from .61 to .81. The SWLS received validity support based on its correlations with other measures of subjective well-being, such as the Self-Esteem Scale and the Affect Balance Scale (Diener et al., 1985). For this study, the Cronbach’s alpha was computed to be .90.
The Brief Disability Acceptance Scale (BDAS)
The BDAS was developed by Tansey and associates (2016) to assess acceptance of disability. It is an abbreviated version of the Multidimensional Acceptance of Loss Scale (Ferrin et al., 2011). It is composed of eight items (e.g., “I am a person of value even though I have a disability” and “Regardless of how others see me, I know that I have personal strengths”). Each item is rated on a 5-point Likert-type type rating scale ranging from 1 (strongly disagree) to 5 (strongly agree). To facilitate interpretation, an average score is computed for the BDAS with higher scores indicating a greater level of disability acceptance. The Cronbach’s alpha for the BDAS was reported to be .90 and was correlated with resilience (r = .41, p < .001) and life satisfaction (r = .38, p < .001). In the present study, the Cronbach’s alpha was computed to be .92.
The Adult Trait Hope Scale (ATHS)
The ATHS was developed by Snyder et al. (1991) to measure the construct of dispositional hope. It is composed of four agency items (e.g., “I energetically pursue my goals”), four pathways items (e.g., “There are lots of ways around any problem”), and four distractor items (e.g., “I feel tired most of the time”). Each item is rated on an 8-point Likert-type rating scale 1 (definitely false) to 8 (definitely true). The distractor items are not included in scoring. To facilitate interpretation, an average score is computed for agency and pathway scores, with higher scores indicating a greater level of hope. The ATHS has test–retest coefficients (more than 3–10 weeks) ranging from .70 to .80 (Snyder et al., 2006). The Cronbach’s alpha is reported to be .74 to .84 for overall hope for students and clinical populations (Synder et al., 1991). This clinical instrument demonstrates both internal and temporal reliability with two separate yet related agency and pathways factors and an overarching hope factor (Babyak et al., 1993), as well as extensive support for convergent and discriminant validity (Cheavens et al., 2000; Snyder et al., 1991). In the present study, the Cronbach’s alpha coefficient was computed to be .93 for the total scale.
The Brief Resilience Scale (BRS)
The BRS was developed by Smith et al. (2008) to assess resilience as the ability to bounce back from adverse events. It contains three positive valence items (Items 1, 3, and 5) and three negative valence items (Items 2, 4, and 6). Each item is rated on a 5-point Likert-type scale ranging from 1 (strongly disagree) to 5 (strongly agree). Negative valence items are reverse scored; the six items are averaged so that high total scores indicate higher levels of resilience. Cronbach’s alpha coefficients of the BRS were reported to range from .80 to .91. Test–retest reliability of the scale was reported to range from .61 to .69 (Smith et al., 2008). In the present study, the Cronbach’s alpha was computed to be .79.
Data Analysis
A simultaneous regression analysis was used to compute the direct and indirect effects of disability acceptance, hope, and resilience on the relationship between functional disability and life satisfaction. The Statistical Package for the Social Sciences (SPSS 26.0) was used for the preliminary analyses of descriptive statistics and correlation coefficients. The PROCESS v3.4 macro for SPSS, written by Andrew Hayes (2017), was used to estimate the total, direct, and indirect effects, and to implement the bootstrap testing approach recommended by Hayes (2017) to test our mediation hypothesis. The Baron and Kenny (1986) procedure was used to examine the potential mediators between functional disability and life satisfaction. In this procedure, the following three steps are completed:
Step 1: Estimate the relationship between the independent variable (X) on the dependent variable (Y).
Step 2: Estimate the relationship between X and the hypothesized mediator (M) to test the mediator variable as the dependent variable.
Step 3: Estimate the relationship between M on Y controlling for X.
If all three relationships are present, the data are consistent with the hypothesis that variable M completely or partially mediates the X–Y relationship. If the effect of X on Y is no longer significant, M fully mediates between X and Y (full mediation). If the effect of X on Y is still significant, but in a smaller magnitude, M partially mediates between X and Y (partial mediation; Baron & Kenny, 1986; Hoyt et al., 2008). In this study, it was hypothesized that the association between functional disability and life satisfaction is mediated by hope, disability acceptance, and resilience.
Results
Preliminary Analysis
Means, standard deviations, and the correlation matrix for variables in the hypothesized mediational model are shown in Table 1.
Correlations, Means, and Standard Deviations for the Independent Variable, Mediators, and Dependent Variable.
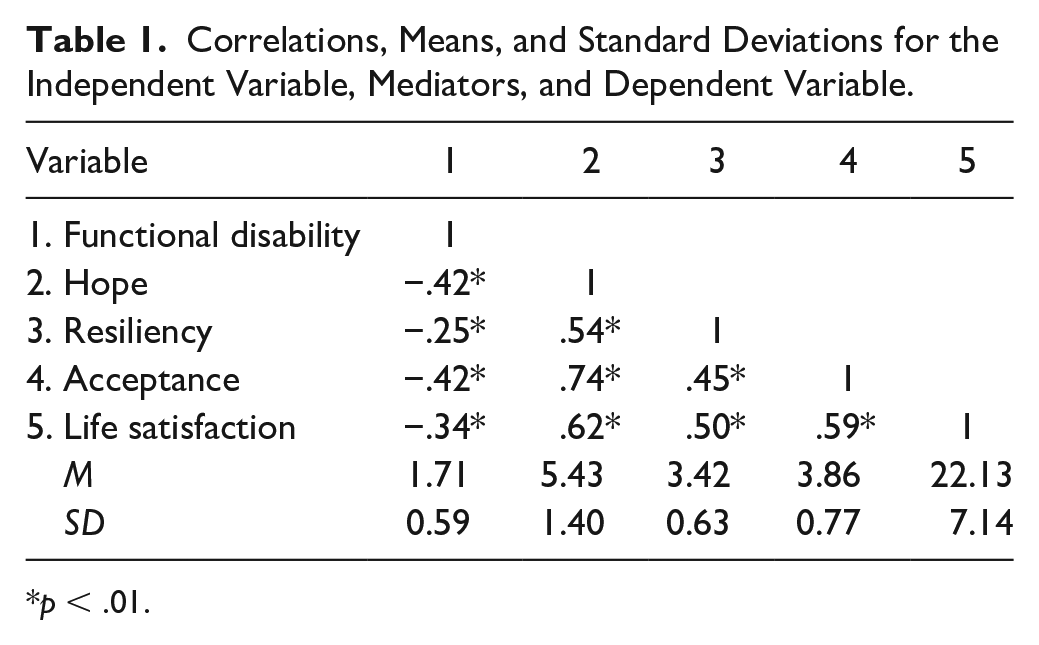
p < .01.
The average functional disability rating of 1.71 (SD = 0.59; range = 1–5) indicated relatively low functional disability scores for participants in this study. The mean scores for disability acceptance, hope, and resilience were 5.43 (SD = 1.40, range = 1–8), 3.86 (SD = 0.77; range = 1–5), and 3.42 (SD = 0.63; range = 1–5), respectively. Participants reported moderate levels of disability acceptance, hope, and resilience in this study. The mean life satisfaction score was 22.13 (SD = 7.14; range = 5–35), indicating a median level of life satisfaction. Results from the correlational analysis indicated robust relationships among functional disability, life satisfaction, and the mediators (i.e., disability acceptance, hope, and resilience), ranging from .25 to .74 with all correlations significant at p < .001 (see Table 1). Functional disability was negatively related to disability acceptance (r = −.42), hope (r = −.42), resilience (r = −.25), and life satisfaction (r = −.34). Hope was positively associated with disability acceptance (r = .74), resilience (r = .54), and life satisfaction (r = .62). Resilience was positively related to disability acceptance (r = .45) and life satisfaction (r = .50), and disability acceptance was positively associated with life satisfaction (r = .59).
Mediation Analysis
In this study, it was hypothesized that the association between functional disability and life satisfaction is mediated by disability acceptance, hope, and resilience. This tri-mediation model is graphically depicted in Figure 1.
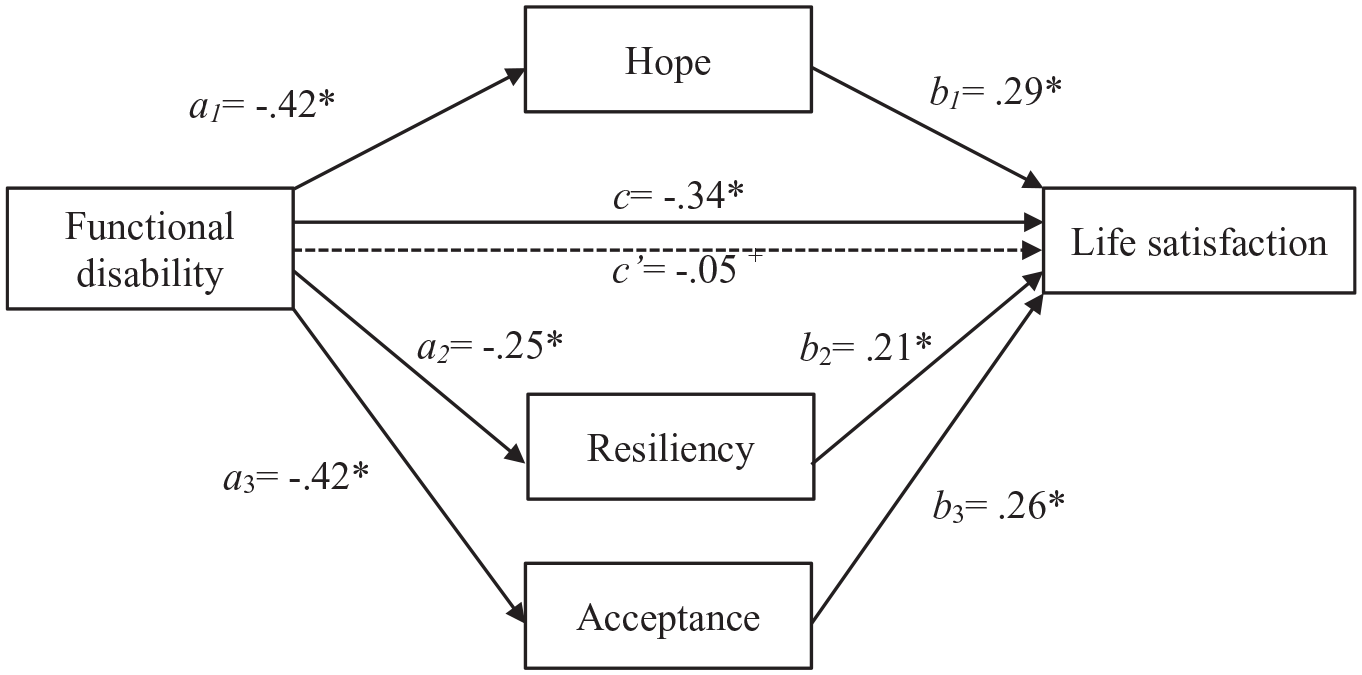
The tri-mediation model of the effect of functional disability on life satisfaction.
Direct effects
For Step 1, the relationship between functional disability (X) and life satisfaction (Y) was assessed. The total effect (c) between functional disability and life satisfaction was significant, β = −.34, p < .001, 95% confidence interval (CI) = [−.49, −.19]. Functional disability has a negative effect on life satisfaction. For Step 2, the relationship between functional disability (X) and each of the mediators (M) was assessed. Functional disability was directly, negatively related to disability acceptance: β = −.42, p < .001, 95% CI = [−.57, −.28]; hope: β = −.42, p < .001, 95% CI = [−.57, −.28]; and resilience: β = −.25, p < .01, 95% CI = [−.41, −.10].
For Step 3, the relationships between each of the mediators and life satisfaction (Y) were assessed while controlling for functional disability (X) and other mediators. A simultaneous regression of life satisfaction (Y) onto functional disability (X), disability acceptance, hope, and resilience was used. Step 2 implies that each mediator is uniquely related to life satisfaction (Y) while controlling for the other mediators and functional disability (X). The tri-mediation model accounted for 46% of the variance in life satisfaction, R = .68, R2 = .46, F(4, 152) = 32.21, p < .001, which is a large effect size (Cohen, 1988). All of the three mediators (disability acceptance, hope, and resilience) were significantly, independently associated with life satisfaction, βs = .29, .26, and .21 respectively. Importantly, the direct effect (c′) between functional disability and life satisfaction was no longer significant after controlling for the effect of the mediators, β = −.05, p = .45, indicating that these mediators completely mediated the direct effect of functional disability on life satisfaction.
Indirect effects
The mediation effects were estimates of the indirect effects of functional disability on life satisfaction through disability acceptance, hope, and resilience. As mentioned, the specific indirect effects are considered statistically significant if the bias-corrected bootstrap CIs for the products of these paths do not include zero (Hayes, 2013). Using the PROCESS procedure with 5,000 bootstrap samples, findings revealed c′ was not significant after controlling for the total indirect effects. Indirect effects of functional disability on life satisfaction through disability acceptance, point estimate = −.11, 95% CI = [−.20, −.03]; through hope, point estimate = −.12, 95% CI = [−.23, −.04]; and through resilience, point estimate = −.12, 95% CI = [−.11, −.01] are all significant. This finding indicates functional disability has a negative impact on disability acceptance, hope, and resilience. Strengthening these positive human traits can reduce the negative effect of functional disability on life satisfaction.
Discussion
The purpose of this study was to examine disability acceptance, hope, and resilience as hypothesized mediators for the relationship between functional disability and life satisfaction for individuals with a history of polio. The tri-mediation model indicated that disability acceptance, hope, and resilience were associated with life satisfaction, accounting for a large effect size of 46% of the variance in life satisfaction scores. Disability acceptance, hope, and resilience were found to be full mediators of the relationship between functional disability and life satisfaction, as the direct effect of functional disability on life satisfaction became insignificant (p > .05, ns) after controlling for the effects of the mediators. In the present study, participants were on the spectrum of high functioning, with the average of 1.71 for the functional disability rating (range = 1–5). Participants in this study reported moderate levels of disability acceptance, hope, resilience, and life satisfaction. Although there was not a direct effect of functional disability on life satisfaction when levels of disability acceptance, hope, and resilience were all controlled for in the mediation model, functional disability did have significant direct effect on each of the mediators that led to a negative indirect effect among each of the meditators on life satisfaction (−.11 to −12.).
The current study suggested disability acceptance, hope, and resilience were positively and significantly related to life satisfaction, supporting results from previous studies (Farbu & Gilhus, 2002; Jacob & Shapira, 2010; Kemp & Krause, 1999; Saeki & Hachisuka, 2006; Winberg et al., 2014). In accordance with previous findings, functional disability was found to be negatively and significantly related to disability acceptance, hope, and resilience and life satisfaction (Farbu & Gilhus, 2002; Harrison & Stuifbergen, 2006; Kemp & Krause, 1999; Stuifbergen et al., 2005). Findings in our study are also compatible with those of a scoping review study among polio survivors (Sulaiman et al., 2019). Researchers found positive, significant associations between life satisfaction and health status, disability attitude, and hope across 34 studies. Conversely, functional disability was negatively, significantly associated with health status, disability attitude, hope, and life satisfaction (Sulaiman et al., 2019).
Disability acceptance is fundamental to positive adjustment, in which disability is integrated into one’s way of life (Ferrin et al., 2011; Pierini & Stuifbergen, 2010; Wright, 1983). Disability acceptance has been suggested to be an integral source of successful coping with PPS (Pierini & Stuifbergen, 2010). In our study, disability acceptance is also a relatively large mediator, consistent with previous findings regarding people with disabilities (Smedema et al., 2013; Sung et al., 2013). A greater level of disability acceptance among individuals with polio and PPS suggests a high level of reconciling the existence of the disability; reaching a new and positive sense of self-concept; and seeking new values, meanings, and future goals. Empirical evidence supports the link of disability acceptance to other positive personality correlates and reduced functional disability, including work-related limitations (Donaldson-Feilder & Bond, 2004; Ferrin et al., 2011).
We also found a relatively large mediational effect of hope through functional disability and onto life satisfaction (Van Leeuwen et al., 2012). In the context of polio and PPS, perceived hope has a unique benefit in elevating both mental and physical health, which are salient predictors of life satisfaction (Magaletta & Oliver, 1999; Shiri et al., 2012). Individuals with higher hope tend to be satisfied with what they have accomplished in life (Kwok et al., 2015). Hope is strongly correlated with greater life satisfaction in a majority of cross-sectional studies (Bailey et al., 2007; Wong & Lim, 2009). Longitudinal research has identified hope as an important predictor of future life satisfaction after controlling for initial life satisfaction (Marques et al., 2011, 2013). This reveals the importance of hope to people with polio and PPS, as they are expected to experience longevity with advances in technology and medicine (Pierini & Stuifbergen, 2010).
Resilience was also been found to mediate functional disability on life satisfaction in our study. A recent meta-analysis research of 60 studies on personality and individual differences demonstrated the positive effect of resilience on psychological health in the general population (Hu et al., 2015). Findings concluded resilience has negative effects on poor psychological health and enhances positive psychological health. In addition, resilience was also found to be a mediator between ill-health and positive psychological health, which is in congruence with our results. Moreover, resilience has been identified as the most prominent source of positive adaptation and subjective well-being in two systematic reviews with a total of 66 empirical studies (Cosco et al., 2017; Gartland et al., 2019). A greater level of resilience among individual with PPS, then, indicates the propensity to return to a certain degree of normal functioning and psychological status (Nemati & Maralani, 2016).
Implications for Rehabilitation Counseling Practice
The fear and uncertainty surrounding the COVID-19 pandemic may feel new to many of us. However, it is peculiarly familiar to those who lived through the polio epidemic of the last century. Findings of the present study contribute important implications for rehabilitation counselors in providing positive psychosocial interventions among people with polio and other infectious diseases that may result in persistent physical or mental health limitations (e.g., COVID-19). This study provides empirical evidence that not all persons with polio and PPS experience severe disability, especially among those reporting high levels of disability acceptance, hope, and resilience. Although disability acceptance, hope, and resilience are related factors, they each represent unique, malleable assets that can be targeted through rehabilitation efforts to improve psychosocial adjustment outcomes—regardless of disability severity. However, functional disability should also be targeted using biological or medical interventions (e.g., medications, occupational therapy, physical therapy) in rehabilitation settings, given that functional disability had a direct and negative effect on positive psychosocial factors that may have contributed to moderate levels of life satisfaction (M = 22.13; SD = 7.14; range = 5–35) reported by participants in this study.
The specific psychosocial interventions for increasing disability acceptance, hope, and resilience include counseling, education, and training. Creating opportunities for people with PPS to experience success may lead to reconstructed cognitions. Modifying one’s environment is an applicable strategy to re-form the internal perception (Sung et al., 2013). Synder and Lopez (2002) conceptualized a theory on hope in conjunction with cognitive behavior therapy for goal attainment. One of the key features of cognitive behavior therapies is transforming problems into operationally defined goals (Beck, 1995). Research suggests the usefulness of breaking down a difficult goal into several simpler and more easily attainable subgoals (Snyder, 1994; Snyder et al., 2006). Hope is often described as consisting of three subscales: agency, goals, and pathways (Anestis et al., 2013). Therefore, increasing one’s self-efficacy and sense of agency in life while simultaneously creating clear goal plans is critical to fulfilling these subscales and promoting hope. Vague, long-term goals lacking a clear pathway or long lists of objectives can seem difficult or unrealistic to achieve, and with this, one may experience feelings of anxiety, helplessness, or perhaps hopelessness. Breaking down difficult goals into smaller, specific, subgoals promotes agency, creates a clear pathway, and illuminates the primary goal in ways that can reduce anxiety and reinstill hope. Typically, there are several different pathways of reaching any goal. In the example of people with polio and PPS, appearing for a vocational rehabilitation session may be an effective stepping-stone or subgoal that might help create a pathway to developing a resume (another subgoal), receiving other expert guidance (subgoal), and ultimately securing a job (primary goal).
In the initial interview, identifying a client’s disability acceptance is critical to understanding their overall self-concept and their readiness for change. This helps rehabilitation counselors formulate clinical decisions and determine applicable strategies and interventions. For example, people with PPS with higher levels of disability acceptance are likely in the process of exploring transferable skills to seek a variety of effective rehabilitation services (e.g., traditional treatment, self-management, telehealth, online programs). Therefore, it is ideal to provide psychoeducational opportunities soon after the onset of disability to increase the likelihood of success in managing symptoms, which in turn can enhance disability acceptance (Sung et al., 2013). On the contrary, for people with PPS with low disability acceptance, emotional supports and environmental accommodations may need to be prioritized. Rehabilitation counselors can assist clients in making these value changes by helping them identify, bolster, and apply positive human traits or strengths in working toward goals. In addition, offering peer-to-peer support groups may also promote disability acceptance. Other methods for encouraging value change include helping clients find meaning, purpose, and positive consequences following the onset of a disability (Dunn & Dougherty, 2005).
In addition to disability acceptance, resilience can also be addressed after first inquiring about a client’s previous experiences with challenging situations and how they navigate and/or overcome barriers. Resilience is the general pattern of how a person bounces back from unfavorable life events. This strategy helps to inform the collaborative goal-setting process. Some clients may only focus on one fixed, rigid pathway to their goal, which can lead to persistent goal blockage. An achievable, clearly defined goal considered through multiple angles, approaches, and pathways then can improve future planning and chances of eventual success. In addition to goal setting, resilience also informs an individual’s problem-solving patterns. Exploring different problem-solving strategies can also be addressed in rehabilitation counseling to support positive coping. Resilience can be further established by developing competence, trust in one’s instincts, and tolerance of negative affect, stress, and uncertainty (Frain et al., 2008). Specific intervention targets, then, might be to improve skills in relation to self-management and competence (Frain et al., 2008; Sung et al., 2013). Together, this study’s findings support the potential value of positive psychological factors applicable to people with PPS. Rehabilitation counseling can include strategies that target disability acceptance, hope, and resilience as means to mediate the impact of functional disability on life satisfaction for Taiwanese individuals who experience PPS.
Limitations and Future Research Directions
There are certain limitations to consider when interpreting and applying the results of this study. This study was conducted with a convenience sample of Taiwanese people with polio and/or PPS, and limitations related to the size and generalizability of the sample with a certain infectious viral disease experience are noted. There is a possible sampling bias in this study due to an overrepresentation of individuals who are on the spectrum of high functioning; however, this reflected a similar demographic representation from the National Institutes of Health publication that people with polio were overall found to have a relatively higher functionality (Pierini & Stuifbergen, 2010). Therefore, the use of a random sample design is suggested in the future to improve the generalizability of the findings to people with polio and other infectious viral diseases. It is also important to note the limitations related to the self-report measures used in this study, which are susceptible to social desirability (Livneh & Antonak, 1994). In addition, the present study used a cross-sectional design, and the mediational effect of hope, disability acceptance, and resilience on the relationship between functional disability and life satisfaction may be better assessed using a longitudinal design. Future research should also assess functional disability and life dissatisfaction in rehabilitation populations with a history of a novel infectious disease such as COVID-19.
Conclusion
This study demonstrated that positive psychosocial factors are negatively linked to functional disability but positively related to life satisfaction, which might help to buffer the indirect and direct negative effects of functional disability on life satisfaction. Our results then reveal valuable insights for the applications of rehabilitation approaches when working with people with a history of polio or other infectious diseases with similar physical health or mental health consequences such as COVID-19. These findings suggest integrating psychosocial strategies that target disability acceptance, hope, and resilience as well as medical interventions such as physical and occupational therapy as vocational rehabilitation services might reduce the impact of disability and promote life satisfaction for people with a lived experience of an infectious viral disease.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.