
Abstract
Increasing community participation can reduce the risk for functional disabilities; participation is influenced by person and environment contextual factors. Development and validation of a brief community participation assessment can advance and support evidence-based assessment in clinical rehabilitation counseling practice. It will be an invaluable rehabilitation and public health surveillance tool that can be used to gauge the health conditions and participation of people with disabilities. The current study evaluated and validated the Wisconsin Community Participation Scale (WCPS) in 982 individuals with chronic health conditions and disabilities. Participants indicated five most meaningful life roles: (a) being able to get around with or without help, (b) live independently with or without help, (c) live a healthy lifestyle, (d) work, and (e) engage in leisure and recreation activities. The WCPS scores were positively associated with physical health, mental health, and life satisfaction and negatively related to functional disability in the theoretically expected directions. The WCPS can help rehabilitation counselors assess their clients’ current level of participation in meaningful life roles that are important to them. Rehabilitation counselors can use the WCPS assessment data to guide treatment planning and empower clients to build confidence and self-efficacy to participate in personally meaningful activities in the community.
Keywords
A primary goal of rehabilitation counseling is to promote the inclusion of people with chronic health conditions and disabilities in all aspects of society (Chan et al., 2009). Rehabilitation counseling researchers have been conducting theory-driven research to inform the development and validation of effective rehabilitation counseling interventions to improve psychosocial, independent living, community participation, and employment outcomes of people with disabilities (Chan et al., 2009, 2019). The World Health Organization’s (WHO) International Classification of Functioning, Disability, and Health (ICF) model has gained widespread acceptance among the U.S. and international rehabilitation health researchers and professionals as a theoretical framework for applied research, case conceptualization, assessment, rehabilitation planning, and selection of effective rehabilitation and health services (Chan et al., 2019; WHO, 2001). The ICF is a biopsychosocial model of disability composed of four major constructs: (a) body functions and structure (impairment), (b) activity (limitation), (c) participation (restriction), and (d) person–environment (P-E) contextual factors. Within the ICF framework, community participation is considered an important rehabilitation and health service outcome and a pretest and posttest outcome variable in intervention research (Chan et al., 2019).
Participation is a subjective concept that is difficult to define and capture; evidence-based research and practice can be advanced through the development and validation of psychometrically sound clinical assessment instruments of community participation (Heinemann et al., 2010; Wu et al., 2019). There are several ICF-based participation measures such as the Impact on Participation and Autonomy Questionnaire (IPAQ) developed by Cardol et al. (2002). It is composed of 39 questions in five domains: a) Autonomy indoors, b) Autonomy outdoors, c) Family roles, d) Social relations, and e) Paid work and education.
Other measures place a strong emphasis on tracking daily tasks and the time and frequency spent on these tasks (Heinemann et al., 2010; Üstün et al., 2010). However, these participation measures have been described as too time-consuming and unwieldy for rehabilitation psychology and rehabilitation counseling practice in clinical settings, follow-up assessment after discharge from hospitals, or as a public health and rehabilitation surveillance tool (Wu et al., 2019).
Scherer and Glueckauf (2005) provided an alternative way to conceptualize community participation within an individual’s life context. Participation was described as an individual’s engagement in meaningful life roles such as employment, parenting, education, recreation, interpersonal relation, religion, and healthy living. Life roles are actions and behaviors within an individuals’ life context distinguished from basic functionality (Scherer & Glueckauf, 2005). Better physical health, mental health, and quality of life contribute to maintaining meaningful life roles and activities in society (Teunissen et al., 2019; Theis & Furner, 2011; Wu et al., 2019).
Researchers at the University of Wisconsin’s Rehabilitation Research and Training Center for Evidence-Based Practice in Vocational Rehabilitation (RRTC-EBP VR) developed the preliminary draft of a brief community participation measure (the Wisconsin Community Participation Scale [WCPS]) based on the meaningful life roles concept (Chan & Pfaller, 2016). Wu and colleagues (2019) validated the WCPS in a sample of people with multiple sclerosis and found that the most important and meaningful life roles were living independently, getting around, participating in recreational and social activities, and engaging in health-promoting behaviors, followed by participating in the personal life roles of children, spouses, parents, and full-time workers, whereas being a student, church member, and part-time workers were the least important. In the Wu et al. (2019) study, community participation was found to be correlated significantly with the 39-item IPAQ (r = .75, p < .001, large effect size), life satisfaction (r = .47, p < .001, medium effect size), and functional disability (r = −.68, p < .001, large effect size) in the theoretically expected directions. The strong association between WCPS and IPAQ supports the use of the shorter WCPS for rehabilitation counseling research and in clinical rehabilitation counseling practice (Wu et al., 2019).
Purpose of Study
As community participation is an important health and rehabilitation outcome indicator, a brief and psychometrically sound measure is needed in clinical rehabilitation counseling research and practice to measure the level of community participation in individuals with disabilities. A brief, validated measure will be an invaluable rehabilitation and public health surveillance tool that can be used to gauge the health conditions and participation of people with chronic health conditions and disabilities living in the community. The WCPS can be extended and refined to assess levels of participation more accurately and reliably in people with disabilities living in the community. The aim of the present study was to extend and refine the WCPS and validate this brief measure in people with chronic health conditions and disabilities living in the community. The following research questions were investigated:
Research Questions
Method
Participants
Nine hundred eighty-two community-dwelling individuals with disabilities were recruited for the present study. Participants ranged in age from 18 to 82 years (M = 40.65, SD = 12.88). Seventy-one (7.2%) of the participants were young adults between the ages of 18 and 24; 746 were prime working-age adults between the ages of 25 and 54 (76%); 123 were older working-age adults between the ages of 55 and 66 (12.5%); and 42 were retirement-age adults 67 years or older (4.3%). There were 686 (69.9%) women and 295 (30.0%) men. There were 798 European Americans (81.3%), 98 African Americans (10.0%), 40 Hispanic Americans (4.1%), 28 Asian Americans (2.9%), and 6 American Indians or Alaska Natives (0.6%). In terms of educational attainment, none reported having no formal schooling; one reported an elementary education (0.1%); 24 had a secondary education, no high school diploma (2.4%); 8 had a special education certificate of completion (0.8%); 149 had a high school diploma or General Educational Development credential (15.2%); 201 had a postsecondary education, no degree (20.5%); 198 had an associate degree or vocational/technical certificate (20.2%); 291 had bachelor’s degree; and 109 had master’s degree or higher (11.1%). We collected data for the 38 causes of disability described in the Rehabilitation Services Administration’s Case Service Report (RSA-911) manual. The most common types of disabilities include depression (15.1%), physical disorders (12.8%), anxiety (12.7%), arthritis (7.6%), diabetes (5.8%), and multiple sclerosis (2.6%).
Measures
Community participation
Community participation was evaluated using the Wisconsin Community Participation Scale (WCPS). It is composed of 12 meaningful life roles: employment, volunteer work, spouse, parent, children, student, recreation activities, getting around, live independently, social life, church member, and health-promoting activities. As a refinement to the original WCPS, we have added a 5-point importance rating scale for each life role and refined the anchor definitions of the 5-point participation rating scale to improve the precision of the participation ratings. The WCPS assesses the importance and the degree of participation in each life role from the perspective of people with disabilities living in the community. Respondents are asked to rate the level of importance for these 12 meaningful life roles on a 5-point Likert-type type scale (1 = not at all important, 2 = not very important, 3 = neutral, 4 = important, 5 = very important). They are also asked to rate how well they participate in those life roles on a 5-point Likert-type participation scale (1 = no participation and not considered, 2 = no participation, but considered, 3 = limited participation, 4 = good participation, 5 = excellent participation). The WCPS yields mean importance scores, relative importance scores, mean participation scores, and weighted participation scores. To account for life roles that are not important to the participants, we used the scoring method proposed by Baker et al., 1998, to weigh the participation scores with the relative importance scores using the following steps:
Add together each item of the mean importance scores to yield a total importance score (scores will range from 12 to 60);
Divide each mean importance score by the total importance score to yield a relative importance score for each item, the sum of which will add up to exactly one;
Multiply the relative importance score by the mean participation score to yield a weighted participation score for each item;
Sum each of the weighted participation scores to yield a total weighted participation score. Total weighted participation scores range from 1 (no participation and not considered) to 5 (excellent participation), with higher scores indicating higher levels of participation in life roles deemed important to the individual.
Functional disability
Functional disability was assessed by the WHO Disability Assessment Schedule (WHODAS 2.0; Üstün et al., 2010). It is composed of 12 functional limitations items (e.g., “How much difficulty have you had in the past 30 days in standing for long periods such as 30 minutes?”). Each item is rated on a 5-point Likert-type scale ranging from 1 (no difficulty) to 5 (extreme difficulty/cannot do). Functional disability scores are calculated by averaging ratings across the WHODAS items, with higher scores indicating higher levels of functional disability. Luciano et al. (2010) reported that patients on sick leave had higher functional limitations than those who were working. The internal consistency reliability coefficient (coefficient α; Cronbach, 1951) of the 12-item version of the WHODAS 2.0 was reported to be .98 (Üstün et al., 2010). In the present study, the coefficient α was computed to be .87.
Health-related quality of life
Health-related quality of life was assessed using the Short Form 12 (SF-12) health survey (Ware et al., 1996). It is composed of 12 items, within eight major domains: (a) Physical Functioning, with 2 items (e.g., “moderate activities, such as moving a table, pushing a vacuum cleaner, bowling, or playing golf”); (b) Role Limitations due to physical problems, with 2 items (e.g., “accomplished less than you would like”); (c) Bodily Pain, with 1 item (i.e., “during the past 4 weeks, how much did pain interfere with your normal work [including both work outside the home and housework]?”); (d) General Health, with 1 item (i.e., “in general, would you say your health is excellent/very good/good/fair/poor?”); (e) Vitality, with 1 item (i.e., “did you have a lot of energy?”), (f) Social Functioning, with 1 item (i.e., “during the past 4 weeks, how much of the time has your physical health or emotional problems interfered with your social activities [like visiting with friends, relatives, etc.]?”), (g) Role Limitations due to Emotional Problems, with 2 items (e.g., “during the past 4 weeks, how much of the time have you had any of the following problems with your work or other regular daily activities as a result of any emotional problems [such as feeling depressed or anxious]?”), and (h) Mental Health, with 2 items (e.g., “have you felt calm and peaceful?”). Each item is rated on either a 5-point Likert-type scale ranging from 1 (excellent) to 5 (poor) for 10 items (i.e., items 1, 4, 5, 6, 7, 8, 9, 10, 11, and 12), or a 3-point Likert-type scale ranging from 1 (yes, limited a lot) to 3 (no, not limited at all) for 2 items (i.e., items 2 and 3). Two summary scores—physical component summary (PCS) score and mental component summary (MCS) score—were computed using the weighted means of the eight domains and standardized to T-score, which was the average value in the 1998 U.S. population. High scores indicate higher levels of physical health and mental health. The average T-score for PCS was 36.54 (SD = 4.96) and 23.83 (SD = 6.77) in this study.
Life Satisfaction
The Satisfaction with Life Scale (SWLS) was developed by Diener et al. (1985) to measure life satisfaction. It is a five-item unidimensional scale, and each item is rated on a 7-point Likert-type rating scale ranging from 1 (strongly disagree) to 7 (strongly agree). Life satisfaction scores are calculated by summing ratings across items with higher scores representing higher levels of life satisfaction. The SWLS has been shown to have good convergent validity with other subjective well-being scales and discriminate validity from emotional well-being measures (Pavot & Diener, 1993). The coefficient α for the SWLS in the present study was computed to be .92.
Procedure
Data were extracted from the World Health Organization International Classification of Functioning, Disability, and Health (ICF) Public Health Surveillance project sponsored by the Department of Rehabilitation Psychology and Special Education at the University of Wisconsin-Madison (UW-Madison). Upon approval from the UW-Madison Institutional Review Board (IRB), adults with chronic health conditions and disabilities living in the community were recruited for the ICF study. The inclusion criteria included (a) the person must be at least 18 years old and (b) the person must have a self-identified disability. We used the Amazon Mechanical Turk (TurkPrime) service to collect data for the present study. To ensure the quality of the data, we relied on panels provided by TurkPrime. These panels use a screening method in which participants are receiving the same compensation for stating whether they are part of the targeted population or not, thus reducing the likelihood of participants faking a demographic or sample status (Litman et al., 2017). In the present study, we asked for 1,020 participants and received 1,019 surveys. Data screening reduced the usable surveys to 982 persons with disabilities. The ICF survey took approximately 30 to 40 min to complete, and participants who completed the survey received a US$10 gift card upon completion.
Data Analysis
Descriptive statistics, reliability analyses, and correlational analyses were computed using the IBM SPSS Statistics (version 26). Missing values were estimated using the simple imputation method provided by SPSS. A multiple regression analysis was used to examine demographic covariates as predictors of community participation.
Results
Rank Order for Importance and Participation in Meaningful Life Roles
Table 1 presents descriptive statistics for the mean importance scores, the rank order of the importance score, the relative importance scores, the mean participation scores, the weighted participation scores, and the rank order of the weighted participation scores for each meaningful life role.
Relative Importance and Degree of Participation in Meaningful Life Roles.
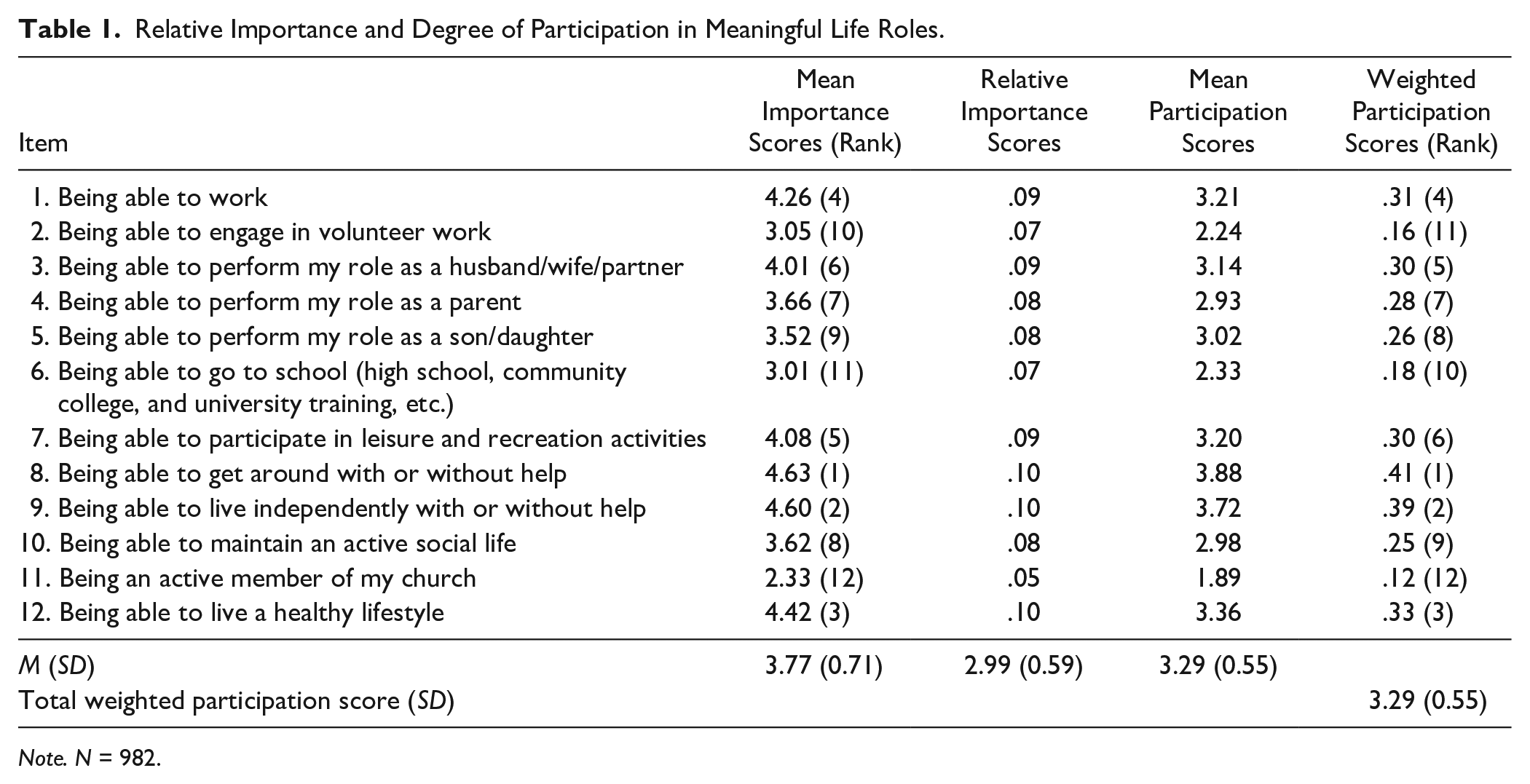
Note. N = 982.
Participants rated “Being able to get around with or without help,” “Being able to live independently with or without help,” “Being able to live a healthy lifestyle,” “Being able to work,” and “Being able to participate in leisure and recreation activities” as more important than other meaningful life roles. They also rated their levels of participation in these roles. “Being able to get around with or without help” (M = 3.88) and “being able to live independently with or without help” (M = 3.72) were close to four (good participation). “Being able to live a healthy lifestyle” (M = 3.36), “being able to work” (M = 3.21), and “being able to participate in leisure and recreation activities” (M = 3.20) were between the ratings of 3 (limited participation) and 4 (good participation). On the other hand, “being able to go to school” (M = 3.01) and “being able to engage in volunteer work” (M = 3.05) were rated as neutral; and “being an active member of my church” (M = 2.33) was rated as not very important. These three life roles had the lowest weighted participation scores. The total weighted participation score (participation weighted by importance) was computed to be 3.29 (SD = 0.55), indicating participants in this study were able to marginally participate in meaningful life roles relevant to their individual situations. Internal consistency reliability estimates (coefficient α) was .62 for the importance scale and .71 for the participation scale.
Demographic Covariates as Predictors of Community Participation
A multiple regression analysis was conducted with the demographic variables (age, gender [male was the focal group], race/ethnicity [White was the focal group], marital status [married was the focal group], educational attainment, income level [low income was the focal group]), body mass index (BMI), physical health component summary score and mental health component summary score as the predictor variables and community participation as the dependent variable. The regression results are presented in Table 2.
Demographic and Psychological Variable Predictors of Community Participation.
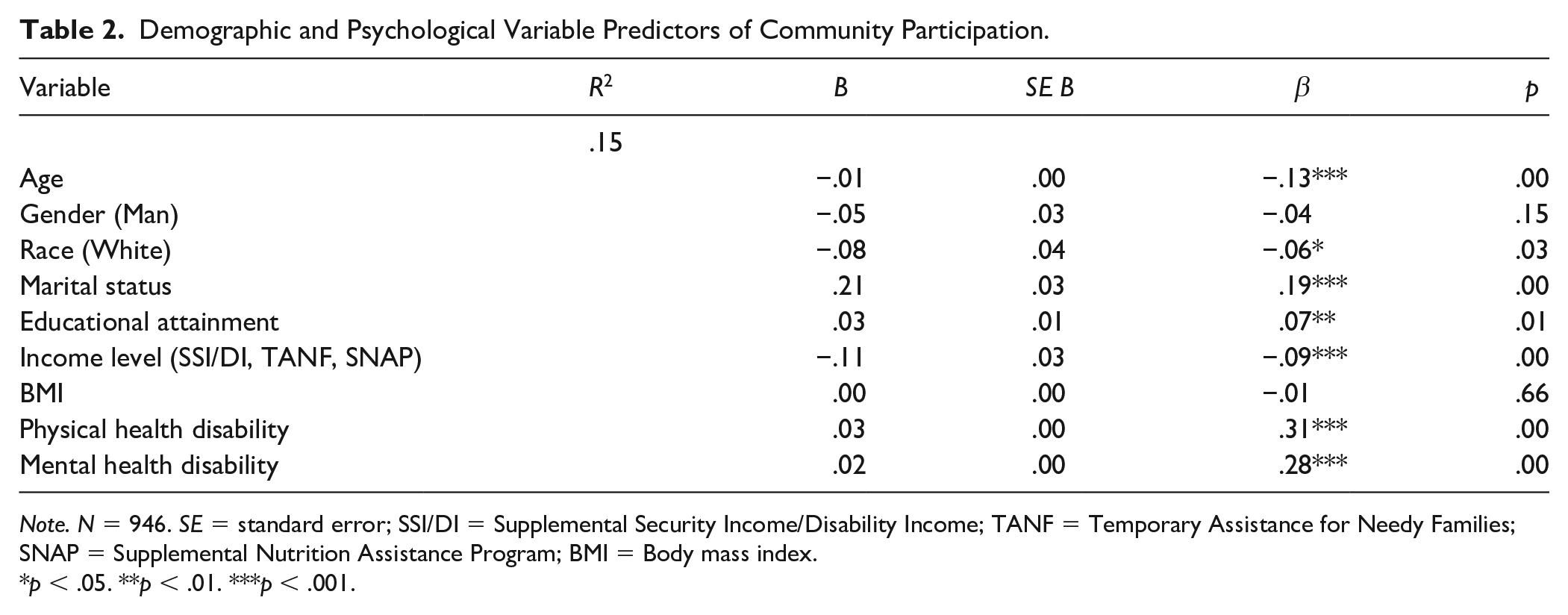
Note. N = 946. SE = standard error; SSI/DI = Supplemental Security Income/Disability Income; TANF = Temporary Assistance for Needy Families; SNAP = Supplemental Nutrition Assistance Program; BMI = Body mass index.
p < .05. **p < .01. ***p < .001.
Demographic variables accounted for 15% of the variation in community participation scores, R = .58, R2 = .34, f 2 = .52 (large effect size), F(9, 936) = 53.97, p < .001. Age, race/ethnicity, marital status, educational attainment, income level, physical health status, and mental health status were found to significantly contribute to explaining the variance in community participation scores, after controlling for the effect of other predictor variables in the model, with age, β = −.13, t(944) = −4.27, p < .001; race/ethnicity, β = −.06, t(944) = −2.15, p < .05; marital status, β = .19, t(944) = 7.19, p < .001; education attainment, β = .07, t(944) = 2.68, p < .01; income level, β = −.09, t(944) = −3.39, p < .001; physical health status, β = .31, t(944) = 9.92, p < .001; and mental health status, β = .28, t(944) = 9.21, p < .001.
Relationships Among Participation, Functional Disabilities, and Life Satisfaction
Within the ICF framework, functional disability is related to community participation, and community participation is in turn associated with life satisfaction. To evaluate the construct validity of the WCPS, we correlated the WCPS participation scores with functional disability and life satisfaction. WCPS scores were negatively related to functional disability (r = −.57, p < .01; large effect size) and positively associated with life satisfaction (r = .52, p < .01; large effect size) in theoretically expected directions (see Table 3).
Correlations Between the Wisconsin Community Participation Scale and Related Constructs.
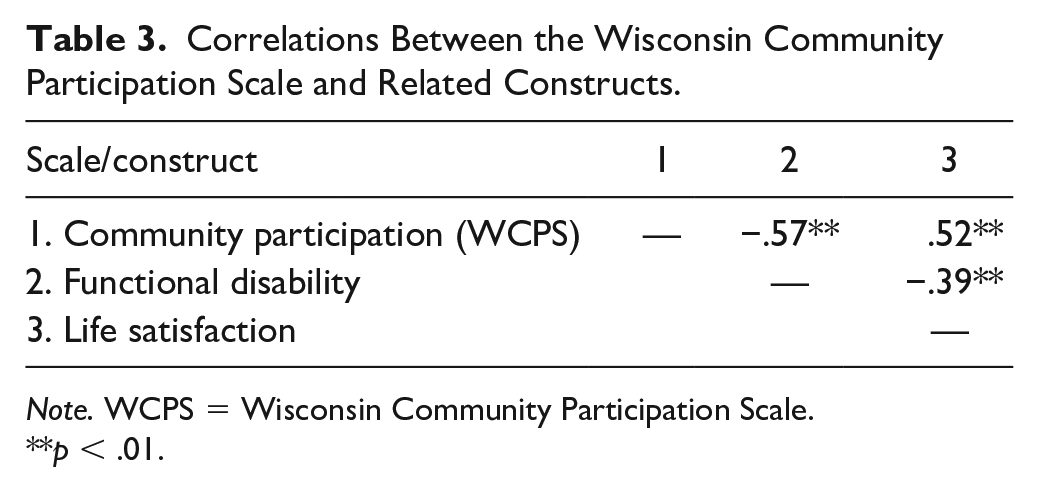
Note. WCPS = Wisconsin Community Participation Scale.
p < .01.
Discussion
The ICF model has been applied in rehabilitation counseling as a mechanism for case conceptualization, assessment, plan development, and the provision of effective vocational rehabilitation services (Chan et al., 2019). Community participation is a key construct in the ICF model of disability and is an important health and rehabilitation outcome measure. Active participation in the community is associated with better physical health, mental health, and life satisfaction (Chan et al., 2019). However, most existing measures of community participation are lengthy and difficult to use in clinical practice settings. Measures that ask clients to recount time and frequency they spend on specific tasks in the community are time-consuming and may be vulnerable to memory recollection problems.
In the present study, we validated the WCPS as a brief measure of community participation in a sample of adults with chronic health conditions and disabilities. We found that getting around, living independently, engaging in a healthy lifestyle, being employed, and participating in recreational activities are rated by people with disabilities living in the community as the most important areas of participation. The reliability of the WCPS is acceptable for a short test. Likewise, the construct validity of the WCPS, based on Cronbach and Meehl’s (1955) nomological network view, was demonstrated for the community participation construct of the WCPS and relationship with functional disability and life satisfaction measures in the expected theoretical directions. The degree of community participation varies based on age, race/ethnicity, marital status, educational attainment, low income, physical health status, and mental health status. Participants who were younger, White, married, educated, and with higher levels of physical and mental health were found to have higher levels of community participation level, whereas low-income individuals have lower community participation levels. It should be noted that of the demographic variables that predicted community participation, physical health status, and mental health status were the strongest predictors of community participation. This suggests people with higher levels of physical health or mental health are more likely to have higher levels of community participation.
Implications
Community participation is among the pinnacle of rehabilitation goals. However, community participation is a dynamic, context-dependent process, and each individual has different subjective needs and values for participation activities. Therefore, just rating participation level may not appreciate how each participation level influences quality of life, which makes it difficult to operationalize and generalize (Yaghmaian et al., 2020). For example, the COVID-19 pandemic presented a significant challenge for individuals with disabilities. It impacts health and life and causes social and economic disruptions (Goggin & Ellis, 2020; Lund et al., 2020). Stay-at-home orders, social distancing, hand hygiene, and mask-wearing resulted in social isolation and job loss. It significantly limited the opportunity for people with disabilities to participate in meaningful life roles, affecting their physical health, mental health, and quality of life. In extreme situations such as natural disasters, including pandemics, or in more generic situations, the WCPS provides a brief assessment that counselors can use to gauge their clients’ community participation and as a public health surveillance tool.
Rehabilitation counselors can use the WCPS to identify life roles that are important and meaningful to their clients. WCPS scores can provide rehabilitation counselors and other disability service providers with an understanding of the values and needs of their clients. It provides a mechanism for counselors to develop person-centered community participation interventions based on their clients’ life stages and subjective perceptions of life roles that are important as well as the barriers and facilitators that affect their participation. The WCPS can be an invaluable rehabilitation public health surveillance tool to gauge community participation levels of people with disabilities living in the community with taking into consideration their value of each community participation goal. The WCPS can also be used as an assessment tool for discharge planning for people with chronic health conditions to determine community participation goals and as a follow-up assessment after being discharged from the hospital. In addition, the WCPS provides a method to evaluate the effectiveness of health, social, and rehabilitation services in helping people with chronic health conditions as they seek to improve their levels of participation and integration in the community.
Beyond the benefits of the WCPS on rehabilitation planning, this study identified demographic variables that are facilitators (e.g., educational attainment, physical health, and mental health) and barriers (e.g., low income) related to community participation of people with disabilities. As physical health and mental health were found to be the strongest predictors of community participation, rehabilitation counselors should consider interventions that help their clients improve their physical health (e.g., physical activity and exercise, occupational therapy, physical therapy, assistive technology, and Tai-Chi), and mental health (e.g., physical activity and exercise, psychological counseling, mindfulness, and meditation).
As the data were collected prior to the COVID-19 pandemic, future studies could gather data during and after the health crisis to (a) better understand the impact of the pandemic on community participation of people with disabilities, (b) compare and contrast the community participation levels of people with disabilities before and after the pandemic, and (c) assess impacts across different demographic group. Such analysis could help rehabilitation professionals to gather insights regarding the impact of the COVID-19 pandemic on community participation and to develop interventions to increase community participation during the post-pandemic period.
Limitations
Several limitations of this study should be considered. The study used a convenience sample of adults with chronic health conditions and disabilities who are predominantly White. The overrepresentation of White individuals affects the generalizability of the findings of this study. Next, data for this study were collected through an online survey platform. This approach may have left out individuals lacking internet access or the ability to complete an online survey. The use of self-report measures could introduce social desirability biases. Although there are research studies supporting the use of TurkPrime to collect data for health and rehabilitation research (e.g., Ipsen et al., 2020; Mortensen & Hughes, 2018), recent articles have raised concerns about the quality of data collected via MTurk and TurkPrime (Chmielewski & Kucker, 2020), future research must build stronger screening procedures (e.g., adding an attention check question and checking for duplicate internet protocol [IP] addresses) to assure the quality of the data.
Conclusion
The present study validated the WCPS as a brief measure of community participation for people with chronic health conditions and disabilities. It is a psychometrically sound measure that can be used by rehabilitation counselors to assess clients’ perception of the importance of and their levels of participation in meaningful life roles. The WCPS can be used as a public health surveillance measure to measure levels of community participation of people with chronic health conditions and disabilities. Findings also provide support for integrating this clinical assessment instrument in the rehabilitation counselors’ toolkit to assist clients in achieving their community participation goals.
Footnotes
Author Note
Xiangli Chen is now affiliated with the Kessler Foundation, East Hanover, USA, and Beatrice Lee is now affiliated with Michigan State University, East Lansing, USA.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The contents of this article were developed with support from the Rehabilitation Research and Training Center on Evidence-Based Practice in Vocational Rehabilitation (RRTC-EBP VR) at the University of Wisconsin–Madison and the University of Wisconsin–Stout and with funding provided by the U.S. Department of Health and Human Services, National Institute on Disability, Independent Living and Rehabilitation Research (Grant H133B100034). The ideas, opinions, and conclusions expressed, however, are those of the authors and do not represent recommendations, endorsements, or policies of the U.S. Department of Health and Human Services.