
Abstract
The article revisits and updates an earlier model (Livneh, 2001) that examined the building blocks that constitute the dynamics of psychosocial adaptation to chronic illness and disability (CID). In the revised tripartite model, the author reconstructs and refines the earlier model based on recent theoretical formulations, clinical reviews, and research findings. In the revised model, the author discusses three overarching components, namely, antecedents (causes of medical conditions, background variables), processes (the dynamically unfolding course of post-CID events), and outcomes (anticipated exit indicators that serve, as snapshot end products, to assess the individual’s experienced and reported quality of life following onset of CID). The article concludes with a brief review of the model’s practical and research implications.
The study of the building blocks, structural fabric, and dynamic processes inherent in psychosocial adaptation (PA) to chronic illness and disability (CID) has occupied rehabilitation, mental health, and medical professionals for more than half a century (Livneh & Antonak, 1997; Marini & Stebnicki, 2018). Theoretical, clinical, and empirical findings, however, have yielded only limited consensus among these professional groups. The bulk of the dissenting views has centered on the following domains: (a) the conceptual scaffoldings (e.g., medical events, social and environmental conditions, CID-generated reactions, coping strategies, and outcome indicators and measures of success) that underlie any comprehensive, integrative, and heuristic model seeking to depict current (and future) understanding of the structure and process of PA to CID; (b) the nature and structure of the psychological reactions (periodically referred to as phases or stages) that follow the aftermath of sudden CID onset (e.g., linear vs. nonlinear, phase-like vs. random); (c) the relative importance to be assigned to the antecedent events to the onset of CID and to the contextual influences encountered concurrently with the onset and with subsequent progression of the CID; (d) the background, or contextual, characteristics that interact with (moderate), link (mediate), or merely present themselves, noncausally, during the adaptation process; (e) the scope of contextual features (e.g., environmental resources) and personal attributes (e.g., personality characteristics, coping modes) that make up the bulk of the PA structure and process; and (f) the choice, individual or set, of psychosocial and medical/health outcome indicators to be employed as measures of successful PA to CID.
An additional unresolved issue centers on a contrast drawn between the nature of adaptation to acquired or adventitious CID and that driven by genetic or congenital in origin. In this study, the author focuses exclusively on CIDs triggered by the former group of onsets (CIDs whose origins are due to illnesses, injuries, life-threatening diagnoses, and related adversarial conditions, such as spinal cord injuries [SCI], cancer, multiple sclerosis [MS], heart conditions, traumatic brain injuries [TBI], and the like). As any effort to address the many novel and unique constructs (e.g., early life experiences of public- and self-stigmatization, development of self-concept, reduced learning and socialization opportunities, efforts directed at self-determination, experiencing no abrupt transition from pre- to post-CID status) generated by models of psychological adaptation to genetic and congenital CIDs would necessitate a complex and lengthy two-tier model, the author elected to focus, in this study, on the former group of medical conditions.
The presence of these inconsistent, often conflicting, perceptions of the nature, structure, and dynamics of PA to CID has done little to derail the interest of rehabilitation professionals from continuing to explore and understand these processes. Since the groundbreaking models of Lazarus and Folkman (1984) and Moos and Schaffer (1984), a cornucopia of PA to CID models have been proposed, targeting a wide range of medical conditions, including cancer (Mishel, 1988, 1990; Naus et al., 2009; Somerfield, 1997; Somerfield et al., 1999), TBI (Kendall & Terry, 1996), heart condition (Holahan et al., 1997), SCI (A. Craig et al., 2017; Middleton & Craig, 2008), MS (Pakenham, 2012), rheumatoid arthritis (Walker et al., 2004), diabetes (Deary et al., 1997), fibromyalgia (Muller et al., 2020), and generic chronic illness (H. M. Craig & Edwards, 1983; Deckert & de Groot, 2018; Maes et al., 1996; Moss-Morris, 2013; Samson et al., 2007; Stanton et al., 2001; Wright & Kirby, 1999). These models, along with a wide range of related theoretical conceptualizations, clinical reports, and empirical findings on coping strategies and resources, CID-triggered reactions, and rehabilitation outcomes, provided the structural fabric upon which the present integrated model is erected.
Twenty years ago, Livneh (2001) presented a conceptual model that sought to integrate existing knowledge about the various components, structures, and processes underlying PA to CID. In that discussion, the author argued that although a general consensus has not yet been reached on the final structure of such a model, a sound conceptual framework of adaptation to CID must include the following three essential domains. These include:
Antecedent or background features and events that provide the backdrop to CID onset and address at least the immediate past or, alternatively, the cause(s) of CID onset. Encompassed in this temporality domain (refer to the top panel of the model diagram) are both: (a) the medical and/or environmental causes that trigger CID onset or diagnosis and (b) the contextual/status variables (existing biological, psychological, sociocultural, and environmental conditions or events) within which these causally linked events are anchored.
The actual PA process that unfolds following CID onset or diagnosis. The most widely theorized and researched subdomains of this process typically include (refer to middle panel of the diagram): (a) the CID-specific medical/functional characteristics (i.e., severity, duration) and their associated psycho-medical aspects (e.g., uncertainty, uncontrollability); (b) the internally driven and phenomenologically experienced reactions (e.g., anxiety, depression) to the loss of bodily parts or functions (also regarded as filtering or mediating agents); and (c) more specific, that is, state-like, CID-triggered stress-reducing cognitive appraisal (e.g., threat, benefit finding), impact perception (e.g., illness intrusiveness), and coping launching (e.g., problem-focused) modalities.
The outcomes that follow successful (as well as unsuccessful) adaptation. That is, the “end result” reached at the presumed completion of the PA process (refer to bottom panel of the model). At the present, the overarching umbrella under which most of the suggested outcome indicators are placed is referred to as quality of life (QOL; Bishop, 2005; Bishop et al., 2009; Livneh, 2001). These indicators are further collapsed under three primary functional headings, namely, (a) intrapersonal (health/biomedical and psychological), (b) interpersonal (family/marital and peer/social), and (c) extrapersonal (external environment or community-based, such as work or academic performance).
The framework adopted by the original model, then, provided the scaffoldings for the present revised model. More specifically, over the past 20 years, the author has continued to incrementally incorporate and revise the original model by aggregating quantitative and qualitative data that were amassed from numerous sources (refereed professional journals, conference presentations, book chapters, and books). Newly introduced, or previously nonincluded, constructs (e.g., certain coping models and conceptualizations, CID impact-producing perceptions, CID-triggered psychological growth models) were carefully scrutinized and, when relevant, incorporated into the present model. Most pertinent modifications to the earlier model were realized in its central panel, namely, the process of adaptation. In contrast, very little new data and relevant suggestions were provided on any useful modifications to be made to the remaining two panels, those of antecedent and outcomes indicators.
Undergirding the proposed integrated model are several assumptions. These include (a) parsimony—despite the history-rich complexity of portraying the process of PA to CID, the proposed model seeks to adopt, within reasonable limits, a reductionist view of such a process; (b) phenomenology—the proposed model posits that the experience of CID can be best understood as an interactive relationship between the subjective (self-awareness of the individual with CID) and the objective (life space or the external environment), thus acknowledging the heterogeneity of the adaptation process; (c) dynamical perspective—PA is imbued in a gradually unfolding process that follows a quasilinear progression, initiated by the sudden onset or diagnosis of CID, and proceeds through efforts to personally manage such an experience, culminating in a defined outcome (degree or level of adaptation); (d) trans-situational generality—the model assumes that the structure and process of PA, despite its heterogeneity across different CIDs, still harbors a common structural and dynamic core; (e) multidomain span—the model maintains that PA to CID necessitates recognition that multiple functional (e.g., affective, behavioral) and life (e.g., domestic, occupational) domains are involved in the process; (f) time dependence—the model described is not meant to indicate a final conceptual framework of PA to CID but rather a “work in progress,” as new theoretical advances, clinical insights, and empirical findings will continue to shape its future structure; and (g) emergent process—the complexity of the construct termed “PA to CID” suggests that it is, with all likelihood, an emergent phenomenon and not reflective of first principles. Although encountered more frequently in the hard sciences literature, the intent underlying this terminology is to suggest that PA may emerge from more fundamental, and likely presently hidden, constructs and processes, many of which are linked to unexplored, or only partially explored, neurophysiological and related biomedical systems and activities. Viewed from a slightly different perspective, the model depicted here characterizes our current state of knowledge about PA to CID (epistemological view) rather than an empirically valid reflection of objective reality (ontological view).
An Integrated Model of PA to CID
In the following paragraphs, a brief overview of the three model components is provided (for an earlier version, refer to Livneh, 2001). In the present study, a special emphasis is placed upon recent developments that pertain to the middle panel of the model, that is, the mediating or moderating role assumed by the adaptation process. This in-depth exploration of the model’s middle panel structural ingredients is undertaken because of the recent interest in several of its subcomponents and related constructs. To provide the reader with a better cognitive map of the various conceptual units subsumed under the model, a combined alphabetic–numerical system is included (see Figure 1).
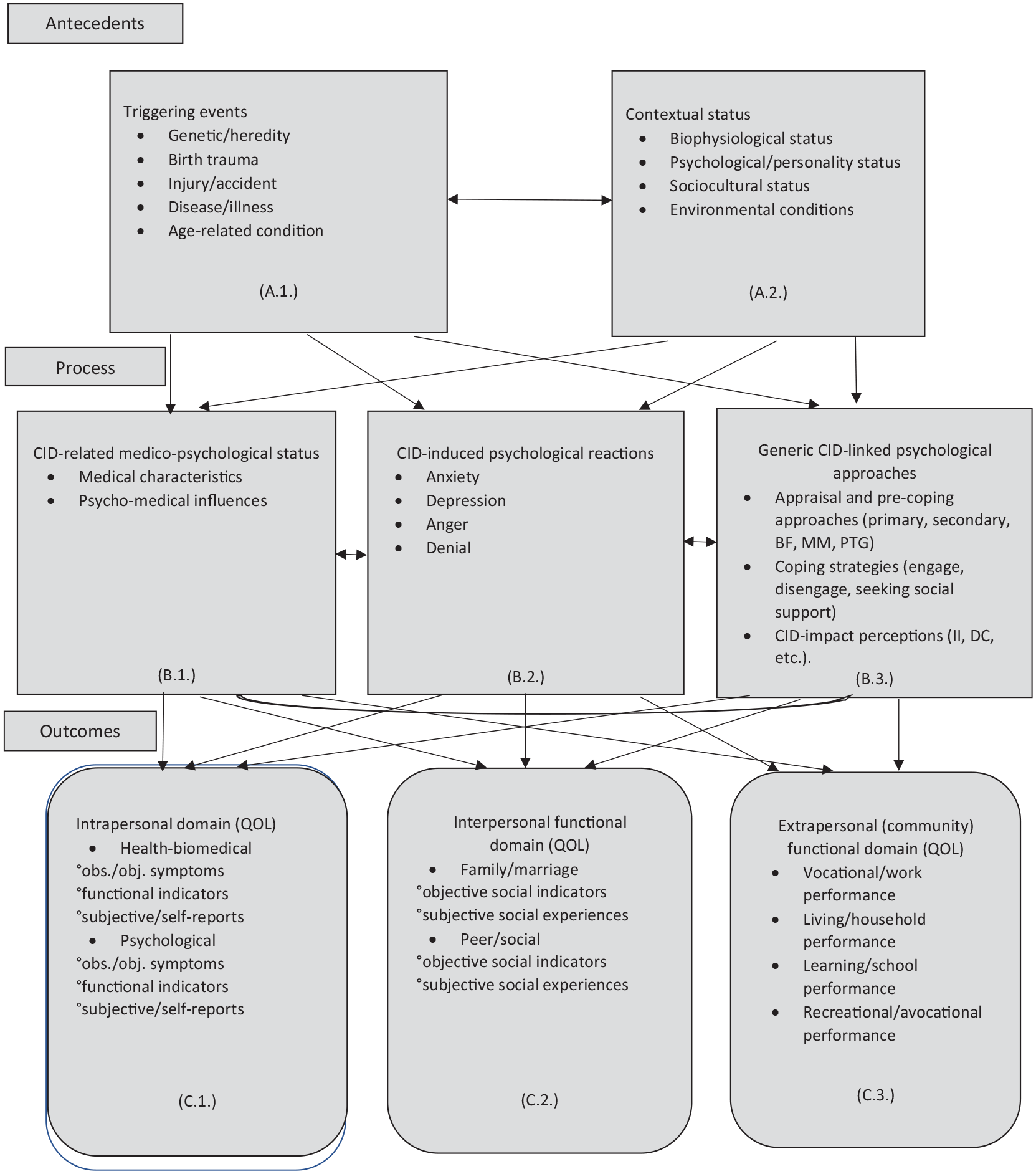
A model of the structure, content, and process of psychosocial adaption to CID.
A. Antecedents
Conditions and events that prevailed during the time of onset of CID are included in this category. They could be regarded as reflecting a pre-CID status. More specifically, antecedents include both causally linked triggering events (A.1.) and contextual variables (A.2.) that may be further subdivided into biophysiological (A.2.a.), psychological/personality (A.2.b.), sociocultural (A.2.c.), and environmental (A.2.d.) statuses.
A.1. Triggering events
These events address specific causes that underlie CID onset. They range from genetic/hereditary medical conditions, birth-related traumas, sudden-onset events (injuries and accidents), progressive diseases and illnesses, to age-related medical conditions and bodily deteriorations (Livneh, 2001; Middleton & Craig, 2008; Moss-Morris, 2013).
A.2. Contextual status
Included under this domain are four primary sets of status variables. They are as follows:
A.2.a. Biophysiological characteristics
These are composed of both diffuse (extended) and focal (situational) biographical status variables, such as age at onset of CID, chronological age, overall health status, gender, ethnicity, religious beliefs, socioeconomic status, educational level, occupational status, financial status, and cognitive capacity (i.e., intelligence).
A.2.b. Psychological or personality-related characteristics
These are composed of cognitive, affective, and behavioral variables, often termed internal psychological resources (see Note 1), and these include both trait-like personality attributes (e.g., optimism/pessimism, hope, neuroticism, self-concept/esteem, body image, personal identity, self-efficacy, resilience, virtue, locus of control, sense of coherence, agency/communion, hardiness, mastery, personal belief system, motivation, personal values, lifestyle) and state-like characteristics (e.g., cognitive, psychosexual and moral developmental stages, future goals and plans).
A.2.c. Sociocultural status
These include interpersonal and familial variables, such as available familial and social support systems, social integration, family developmental stage, performed familial and social role(s), and cultural meaning of health and illness.
A.2.d. Environmental and related community-linked features
Encompassed here are such resources (or their absence) of external (i.e., physical) conditions, economic conditions, stigmatizing/attitudinal barriers, physical/architectural barriers, prevailing community-triggered stressors (e.g., crime, poverty), medical- and health-related services/facilities, financial establishments, and religious/spiritual organizations (Middleton & Craig, 2008; Wright & Kirby, 1999).
An integrated approach to considering the abovementioned triggering and context status variables can also be taken through the prism of the diathesis-stress model. Briefly, this model advocates that many psychiatric disorders are precipitated by a complex interaction of a (genetic, biological, physical, and psychiatric) predisposition to vulnerability, that is, diathesis, and stressful life events encounters (environmental stressors) by the person during the life span. The antecedents presented earlier would, then, reflect such a view. However, although meritorious in its own right, this model is only marginally relevant to the domain of adaptation to acquired CID, as it (a) was developed in the context of explaining psychopathological disorders (e.g., schizophrenia, bipolar disorder); (b) does not directly address the impact of sudden, severe physical and neurological CIDs; and (c) places a disproportional degree of weight for the onset of future psychiatric conditions on genetic, physiological, prenatal, and early postnatal factors.
B. Process
The middle panel of the adaptation to the CID framework is composed of three overarching components. They are (a) CID-linked medical status characteristics and events (B.1.), indicating a “state-like” influence; (b) specific CID-triggered psychological reactions that serve as filtering (mediating or processing) mechanisms (B.2.); and (c) generic psychological strategies and processes that come into focus following the onset of trauma-induced life crises, including that of CID (B.3.). These three components, therefore, indicate a CID-saturated status (see Note 2).
B.1. CID-related medical status
Two subcategories are recognized in this domain. The first subcategory is composed of medically determinable characteristics (B.1.a.). Included among these CID-triggered characteristics and influences are the degree of life threat and probability of mortality, functional restrictions, mobility impairment, course and pace of CID, prognosis, duration of the condition, degree of severity, presence and degree of pain, presence of fatigue, visibility of symptoms (and their cosmetic impact), medical side effects, and treatment regimen and adherence to it. The second subcategory (B.1.b.) is composed of more diffuse psychomedical influences, such as perceived uncertainty and ambiguity (of future), unpredictability (of present and future), uncontrollability of life events, and perceived stigma. All these CID-generated effects continuously interact with both generic psychological mechanisms (B.3.) and specific psychological reactions (B.2.) that emanate from the onset or diagnosis of CID (H. M. Craig & Edwards, 1983; Moss-Morris, 2013)
B.2. Specific CID-generated psychological reactions
The onset or diagnosis of CID triggers a series of individually experienced psychodynamic reactions. They may be interpreted as “raw reactions” to the onset of traumatically induced events that alter one’s life and may result in a chronic medical condition, debilitating consequences, or death. These phenomenologically reported reactions have been documented in the CID literature and span a wide range of medical conditions (Koenig & George, 1998; Livneh & Antonak, 1997; Scott et al., 2013; See et al., 2003; Turner & McLean, 1989; Vandereycken, 2005). Traditionally, these reactions have been viewed in the context of phase- or stage-like models of adaptation (Livneh & Antonak, 1997; Marini, 2018; Smedema et al., 2009). The lack of consistently supportive empirical findings for a universal (trans-situational and across CIDs) progression of such “stages” resulted in a more modest approach that argues for individually determined, clinically observed, and phenomenologically experienced (idiosyncratic) temporal progression of psychodynamic reactions.
In contrast to psychiatrically observed clinically diagnosed symptoms, these reactions to CID are regarded as normal responses, despite occasional exacerbation into clinically reported levels, following a traumatic, often life-threatening personal injury (e.g., SCI, TBI, amputation), diagnosis (e.g., cancer, cardiovascular condition, amyotrophic lateral sclerosis), or life course-altering disease (e.g., MS, Parkinson’s disease, blindness). More specifically, these CID-triggered, internally driven reactions have been traditionally collapsed into phenomenologically observed clinical categories, namely, anxiety, depression, denial, anger, and acceptance. The first four reactions have been generally observed to subside, over time, while that of CID acceptance has been observed to increase (see Note 3). Indeed, empirical findings from several longitudinal studies have indicated that self-reported experiences measuring the presence of these reactions confirmed reduction in reaction magnitude and impact on one’s life over time. These findings have been reported for people who sustained cancer (Carver et al., 1993; Compas et al., 1999, for anxiety, denial, and depression), cardiovascular disease (Terry, 1992, for anxiety and distress), MS (Pakenham, 1999, for depression and distress), and SCI (Kennedy et al., 2012, for anxiety; Kortte et al., 2010, for depression). Findings indicating fluctuations in experienced reactions (depicting a curvilinear trend over time) have also been reported (e.g., Stanton & Snider, 1993, for depression and anger among cancer patients; Lowe et al., 2000, for anxiety and negative affectivity, among cardiovascular disease survivors; Kennedy et al., 2000, for anxiety and denial, among SCI survivors; and Couture et al., 2012, for depression, among people undergoing amputation). Of interest were findings suggesting that reactions exhibiting a u-curved distribution, followed patients awaiting surgical interventions (e.g., mastectomy), and discharge from the hospital to the community (e.g., following SCI inpatient rehabilitation). In both cases, heightened anxiety and psychological distress were reported in anticipation of these events, following an earlier downtrend of reactions after CID onset, and later a reemergence of decreased distress, as successful resolution was achieved.
Also of note are findings that these reactions interact with antecedent variables (triggering events [A.1.] and the more static contextual variables [A.2.]), and the process-based components that include: (a) medical status following CID onset (B.1.) and (b) the broader, generic CID-elicited psychological mechanisms (e.g., appraisal modes, coping strategies [B.3.]). These interactions may also be regarded as filtering mechanisms, serving to moderate and/or mediate how psychosocial outcomes unfold. Finally, although two of the reactions, namely, depression and anxiety, have been traditionally regarded as state-like, temporally bound responses to a traumatic and life-altering event, such as CID onset, it should be acknowledged that in certain circumstances they have been treated as outcome variables. In the context of the present model, and in lieu of these reactions’ fluctuating clinical properties, their appropriateness to serve as long-term, stable outcome variables is questioned and they have been “assigned” the status of process variables.
B.3. Generic CID-elicited psychological modalities
These broad modalities (mechanisms, strategies) represent a range of psychological (psychodynamic) perceptions, defensive mechanisms, management efforts, appraisal modes, and coping strategies that combine both trait-like and state-like processes. They serve to mitigate, mediate, and filter the psychological impact experienced following stressful life events, traumatic experiences, and, more specific to the present model, the sudden onset or diagnosis of CID. The many constructs hypothesized to occupy this role can be conveniently classified under the following broad categories: (a) appraisal and related pre-coping approaches (B.3.a.); (b) coping strategies (B.3.b.); and (c) perceptions of CID impact on, intrusion into, and interference with daily life (B.3.c.). The following discussion focuses on the, arguably, most widely encountered CID-triggered, stress-minimizing modes recognized in the literature.
B.3.a. Appraisal and pre-coping approaches
Although various classification systems of appraisal of stressful, traumatic, and CID-linked impact have been proposed, they could be parsimoniously collapsed into the following categories:
B.3.a.i. Primary appraisal, including the initial appraisal of the significance or magnitude of the traumatic experience, that is, harm and/or loss incurred by the traumatic event, typically referring to a recently experienced trauma (in the immediate past, such as CID onset); appraisal of threat, referring to an imminent trauma (in the near future, such as the anticipation of a life-threatening diagnosis or surgery); or appraisal of challenge, also a future-oriented approach where potential benefits to be gained from the traumatic experience are assessed (Lazarus & Folkman, 1984; Moos & Holahan, 2007; Samson et al., 2007; Stanton et al., 2001).
B.3.a. ii. Secondary appraisal, addressing the availability of personal resources, or more specifically, coping options that could be mobilized to manage the engendered stress and the likelihood that each option will achieve the goal of reducing trauma-generated stress. Furthermore, during secondary appraisal, the individual also assesses event characteristics, such as its controllability, changeability, uncertainty, and spread (Lazarus & Folkman, 1984; Moos & Holahan, 2007; Pakenham, 2012; Stanton et al., 2001).
B.3.a.iii. A third group of more recently proposed appraisal-like constructs (or pre-coping modes) in the aftermath of CID onset may also be considered. These appraisals stem from the adversities inherent in the onset and diagnosis of CID and focus on incurred loss, unfulfilled hopes, and shattered beliefs. If left unattended or when spiraling unchecked, they exert a deleterious influence on the person’s ingrained assumptions about the world, life, and self (Janoff-Bullman, 1992; Taylor, 1983; Tedeschi & Calhoun, 1995). The shattering of these cherished assumptions is often accompanied by feelings of meaninglessness, purposelessness, and truncated personal growth. A group of counterbalancing appraisal efforts and resources, at times anchored in unrealistic, overoptimistic, even illusory, perceptions (Taylor, 1983), that has been suggested to mitigate the influence of these events include: (a) benefit finding (BF; reducing stress by identifying positive outcomes resulting from a traumatic experience; Helgeson et al., 2006; Helgeson & Zajdel, 2017; Pakenham, 2005); (b) meaning-making (MM; composed typically of both presence of meaning and search for meaning), which includes having purpose in life (reinterpreting or reappraising a traumatic event; deRoon-Cassini et al., 2009; Park, 2010; Thompson et al., 2003); and (c) perceiving post-traumatic growth (PTG; at times referred to as stress-related growth, adversarial growth, flourishing, and thriving; Pakenham, 2012; Stanton et al., 2001; Tedeschi et al., 1998). These appraisal, or pre-coping, efforts reflect a quasi-independent facet of a complex and broad set of coping resources. All three constructs have been examined as both process variables (predictors or mediators) of adaptation and outcomes (Greenberg et al., 2020; Helgeson et al., 2006; Park, 2010; Park & Folkman, 1997). In the context of the present framework, due to the fluidity of their clinical unfolding, they are regarded as process variables rather than psychosocial outcomes. BF, MM, and PTG are thought to occur later than primary and secondary appraisals and typically operate when initial psychic equilibrium has been more fully achieved following the traumatic event. Moreover, it has also been suggested (Helgeson et al., 2006; Martz & Livneh, 2016) that BF and MM may be more proximal to the stress onset or occurrence of the traumatic event, while PTG is experienced at a more distal juncture. Meta-analytic studies, systematic reviews, and related informal reviews of research findings have supported the beneficial effects of these constructs in predicting successful PA to CID (Barskova & Oesterreich, 2009; Martz & Livneh, 2016; Park, 2010; Psarra & Kleftaras, 2013). A dissenting perspective on the veridicality of these constructs, and in particular PTG, has also been advanced. According to this view, the boundary between actual and perceived growth is blurry at best, if not unattainable. Furthermore, such assumed growth could reflect an illusory belief, not anchored in reality, thus merely indicating a wishful thinking cognitive function or the existence of a quasi-denial mechanism (Livneh et al., 2019; Zoellner & Maercker, 2006).
B.3.b. Coping strategies
Coping strategies refer to both trans-situational and transtemporal mechanisms (Carver et al., 1989; Tobin et al., 1989) as well as to situation-specific and time-specific efforts (Endler & Parker, 1994; Lazarus & Folkman, 1984; Moos & Holahan, 2007) to diminish and nullify stress engendered by a traumatic life event, including CID onset. They are typically classified according to their functionality (increasing probability of resuming pre-CID activities and maintaining positive psychological well-being), structure (engagement vs. disengagement coping, approach vs. avoidance), level of adaptation (a continuum representing adaptive to nonadaptive coping efforts), and temporality (preventive coping and reactive coping; Livneh, 2016; Martz & Livneh, 2007; Skinner et al., 2003). Empirical research findings have consistently demonstrated that engagement coping strategies, including problem-focused, active, planful, cognitive restructuring, and positive reappraisal, are linked to better PA. In addition, more recent expansions of these engagement-type, action-oriented coping have also included models of self-management (de Ridder et al., 2008) and self- and emotion regulation (Koechlin et al., 2018; Wiebe & Korbel, 2003) as means of combating the functional challenges of CID. The merits of engagement coping have been documented among people with a wide range of CIDs, including cancer, heart disease, SCI, amputations, TBI, diabetes, MS, and related neuromuscular diseases (Livneh & Martz, 2012; Maes et al., 1996; Martz & Livneh, 2007). In contrast, coping efforts termed disengagement coping, including wish fulfilling, escape avoidance, distancing, social withdrawal, rumination, blaming others, self-criticism, and substance use strategies, are associated with poorer PA among these groups. A third cluster of coping strategies, often regarded as a distinct modality, includes those strategies of perceived and received (seeking and finding) social support (Folkman & Moskowitz, 2004; Livneh & Martz, 2012; Skinner et al., 2003). This cluster has been found to be independent of the first two in a number of studies (Amirkhan, 1990; Carver et al., 1989; Dunkel-Schetter et al., 1992; McColl et al., 1995). The use of seeking social support strategies has also been found to be linked to better PA among people with CID (Chronister, 2009; Livneh & Martz, 2012; Manne, 2003). The clinical unfolding and adaptation relevance of these three broad coping modes have been observed to be both mutability and controllability dependent on the nature of CID (Livneh & Martz, 2012; Penley et al., 2002; Stanton et al., 2007). The use of denial (considered both a defense mechanism and a coping modality), for example, presents a rather complex picture, as findings on its (in)effectiveness to ward off CID-generated stress are often inconsistent and are time dependent on proximity to CID onset (Goldbeck, 1997; Livneh, 2009; Livneh & Martz, 2012).
B.3.c. Perceptions of CID influence
Perceptions, or beliefs, of the role CID plays in navigating and challenging one’s life, lifestyle, and QOL are also of importance as mediators and moderators of PA. Two leading models that have examined the nature of such perceptions dominate the literature. They are illness intrusiveness (II; Devins et al., 1983; Devins & Deckert, 2018) and disability centrality (DC; Bishop, 2005; Bishop et al., 2007). When comparing these two perceptions/belief-associated approaches with the previously reviewed process-related constructs of BF, MM and PTG, two primary differences become evident. First, the appraisal and coping constructs tend to focus mostly on the more adaptive (i.e., positive) nature of the PA process, presenting an optimal view of human adaptation under adverse conditions. The II (B.3.c.i.) and DC (B.3.c.ii.) models, in contrast, realistically acknowledge the potentially nonadaptive (i.e., negative) features of this process, with a discussion of such notions as CID intrusiveness into, and loss of control over, one’s life. Second, while the earlier constructs are more limited in their explanatory scope, II and DC suggest dynamic, even if constrained, “mini models” that encompass several subcomponents. They may, therefore, be regarded as stripped-down perspectives on PA to CID whose focus resides in a central construct (i.e., II, DC). The II model, for example, focuses on “illness induced disruptions to valued activities and interests” (Devins & Binik, 1996, p. 642). In a somewhat similar, but truncated, version of the leading models of PA to CID, it seeks to highlight the role of II in bridging between the burden imposed by CID and its functional limitations and psychosocial well-being. Empirical findings have supported the association between II and psychosocial outcomes (e.g., Devins, 2010; Devins & Deckert, 2018). The DC model, partially derived from the framework proposed by Devins and his colleagues, relies on two psychosocial mechanisms, namely, domain satisfaction or importance (maintenance of satisfaction in central life domains and reprioritization of these central domains to minimize perceived gaps between anticipated and wished for QOL) and domain control (perceived impact exerted by CID onset on one’s capacity to control newly encountered life conditions and pursed plans). As with Devins’ model, these two related domains of DC are viewed as moderators of CID impact on PA. Supportive evidence of the viability of the DC construct as a mediator of PA to CID was furnished by Bishop (2005; Bishop et al., 2008).
Other, more diffuse models of CID-influenced perceptions exist (B.3.c.iii.) and may be collapsed into a single broad category. They include illness centrality (extended to such concepts as illness identity and internalized perceived stigma; Charmaz, 1991; Charmaz & Rosenfeld, 2010; Helgeson & Zajdel, 2017; Park et al., 2011), disability identity (or disability self-concept; Bogart, 2014, 2015), injury centrality (Shiloh et al., 2018), and survivor centrality (Helgeson, 2011). These constructs were found to be related to psychosocial outcomes, such as QOL and well-being in the hypothesized direction, in people with various medical conditions (Bogart, 2015; Helgeson, 2011; Helgeson & Novak, 2007; Park et al., 2011; Shiloh et al., 2018).
Finally, the process [B] component may also be recognized for incorporating rehabilitation and related therapeutic interventions. Due to space limitations, these are not addressed in the present study. A large body of literature (e.g., Chan et al., 2015; Kennedy, 2007; Marini et al., 2012; Marshak & Seligman, 1993; Martz, 2018; Radnitz, 2000) exists on how these interventions serve to direct, improve, and expedite the process of PA to CID.
C. Outcomes
Prior to suggesting a system for classifying outcome domains following CID onset, a mention should be made of an unresolved disagreement among researchers and clinicians as to the nature of the proposed outcomes. Two schools of thought on outcome conceptualization exist, and they could be simply termed as dichotomous versus continuous. The dichotomous, or discontinuous, view posits that psychosocial outcome indicators should be classified into either positive or negative. More specifically, those advocating this approach contrast positive or adaptive outcomes (e.g., low distress, high life satisfaction) with negative or nonadaptive outcomes (e.g., high distress, poor adjustment; Middleton & Craig, 2008; Moss-Morris, 2013; Pakenham, 2012; Samson et al., 2007). In contrast, proponents of a continuous approach to outcome measurement view them as spanning a continuum of outcomes, ranging from poor (nonadaptive) at one pole to excellent (adaptive) at the opposite pole, with numerous states of adaptative levels along this spectrum (Kendall & Terry, 1996; Lazarus & Folkman, 1984; Naus et al., 2009; Stanton et al., 2001; Weinert et al., 2008). The latter approach is adopted for the purpose of the present model. The rationale for advocating this approach stems from its consistency with the view that most human psychological and physical attributes follow a continuous, rather than discrete or dualistic, distribution (e.g., intelligence levels, personality types, psychiatric manifestations, attitudes, height, weight).
Although numerous approaches have been suggested to classify outcome domains in the context of PA to CID (e.g., H. M. Craig & Edwards, 1983; Deckert & de Groot, 2018; Moss-Morris, 2013; Ogles et al., 1996; Pakenham, 2012; Stanton et al., 2001; Wright & Kirby, 1999), the most comprehensive, detail-oriented models have focused on the overarching construct of QOL and its various facets, including life satisfaction, subjective well-being, and functional level. More specifically, three primary functional domains or strata have been proposed: intrapersonal, interpersonal, and extrapersonal (community-based). The intrapersonal or individual-based domain (C.1.) can be further divided into health/biomedical (C.1.a.) and psychological/subjective well-being (C.1.b.). The interpersonal or other-based domain (C.2.) can also be subdivided into two subcategories, namely, family/married life (C.2.a.) and peer/social relationships (C.2.b.). Finally, the extrapersonal or community/environment-based domain (C.3.) can be regarded as encompassing several subdomains, four of which are directly embedded in the field of rehabilitation. These include work/employment setting activities (C.3.a.), living/household tasks (C.3.b.), learning/school activities (C.3.c.), and recreational/avocational pursuits (C.3.d.; see Note 4).
C.1. Intrapersonal domain
The intrapersonal outcomes domain is composed of physical health-related (biomedical) and psychological health-related (mental health) indicators. Both can be further classified under three microanalytic categories.
C.1.a. Biomedical domain
In this context, the three subdomains take the form of (a) observed symptoms (C.1.a.i.) that reflect clinical markers, such as symptom severity, duration and frequency of the condition, degree of life threat, pain behaviors, and resultant complications; (b) residual functional strengths and limitations (C.1.a.ii.) marked by behavioral and performance activities and restrictions (trans-situational ADL indicators) and illness management skills; and (c) subjectively reported experiences (C.1.a.iii.) reflecting affective and cognitive indicators of one’s general health and specific biophysiological systems status.
C.1.b. Psychological domain
In this context, the three subdomains include (a) observed symptoms (C.1.b.i.), validated by both clinical professional testing and neuropsychological studies, that reflect certain clinical manifestations indicating depression, anxiety, psychological distress, denial, psychotic ideation, and the like; and (b) functional strengths and limitations (C.1.b.ii.) that indicate psychiatric functioning and behavioral/performance manifestations and may include withdrawal from social activities (depression), avoidance of specific situations (anxiety), refusal to follow, or ignoring, medical advice (denial), substance abuse (maladaptive coping), and combative or uncooperative behavior (anger/hostility). These outcomes represent long-term, trans-situational, and more stable facets of the adaptation process, unlike their process-phase counterparts that are viewed as more short-term, emerging, and state-like reactions. The third subdomain, (c) subjective self-reports (C.1.b.iii.), includes personal accounts of affective experiences (e.g., anxiety, depression, anger, emotional distress, and feelings of well-being), cognitive experiences (e.g., perceptions of oneself, distorted reality perceptions, concentration difficulties, and incidents of confused thinking), and behavioral manifestations (e.g., withdrawal from social/public encounters, alcohol or drug abuse, and engagement in hostile or dangerous activities). A certain degree of pragmatic overlap inevitably exists among the intrapersonal domain indicators due to the intricateness and interdependence of several of these subdomains.
C.2. Interpersonal domain
The interpersonal domain components can also be subclassified into two broad categories, namely, family/marital (C.2.a.) and social/peer relationships (C.2.b.). Both subcategories, of which the former refers to generic domestic/familial life activities while the latter focuses on broader social involvement, discussed here as a single category, suggest the following outcome indicators: (a) objective social functional indicators (C.2.a.i., for familial and C.2.b.i., for peer relations), addressing domestic roles and tasks (i.e., performance of parental and spousal roles, responsibilities, and activities), and social roles and activities (i.e., performance of social roles and activities such as maintaining friendships, helping others in need, avoiding angry outbursts); and (b) subjective social experiential indicators (C.2.a.ii., for familial, and C.2.b.ii., for peer relations) that are reflected in both affective (appropriateness of emotional expression in daily social encounters) and cognitive-behavioral (realistic perceptions of social encounters and perusal of socially embedded intellectual pursuits) domains, such as experiencing social anxiety, harboring hostile feelings toward others, and crying inappropriately during family gatherings (affective) and engaging in planning family’s future goals, financial decision-making, group-based task-oriented problem resolution, and helping children with homework assignments (cognitive-behavioral). Again, a certain degree of indicator overlap is to be expected among these subdomain characteristics due to their interdependent nature.
C.3. Extrapersonal domain
The final proposed domain is the extrapersonal one. Outcome indicators of this environmental- or community-linked domain may be conveniently classified under four primary and partially overlapping functional subdomains (life spaces, environments), namely, vocational (C.3.a.), living (C.3.b.), learning (C.3.c.), and recreational (C.3.d.) settings.
C.3.a. Vocational settings performance
Outcome indicators reflecting occupational activities focus on a range of work-related activities. These include indicators of employment status (i.e., full- or part-time), duration of employment, job skills acquired, salary level, work productivity, job retention, number of days missed per time unit, and so on. These indicators are viewed as a proxy for PA.
C.3.b. Living settings performance
Indicators included in this subdomain address capacity to acquire and sustain personal independence (independent living skills) within the immediate life space. More specifically, these indicators focus on the level of productivity and successful functioning as suggested by the performance of household activities and daily chores, negotiating home and local community physical environment, using public transportation, shopping, and so on. Success in completing these activities is viewed as a marker for adaptive PA.
C.3.c. Learning settings performance
Indicators that suggest PA in the subdomain of learning and training (school) pursuits, that is, academic, prevocational, and skill-building activities, refer to the following: attainment of a high school (or GED) diploma, college degrees, professional certificates and licensures, maintaining minimum level GPA while in school, earning of continuing education credits needed to secure and maintain professional certificates, and so on. Attainment of these learning goals is also interpreted as a marker of positive PA.
C.3.d. Recreational settings performance
The fourth and final subdomain of extrapersonal functioning is reserved to success in pursuing leisure time activities and related avocational interests. These recreational pursuits are regarded within the context of engaging in personal and social activities (sports, chess, music, and reading) and are further measured by yardsticks such as frequency (i.e., number of interests or hobbies pursued per a unit of time) and duration (i.e., duration of activity per unit of time).
Implications for Rehabilitation Practitioners and Researchers
The updated model presented here offers rehabilitation professionals a number of practical benefits. First, the model provides rehabilitation practitioners with a sweeping overview of the most prominent theoretically derived and empirically explored ingredients of the adaptation process to CID. Furthermore, it also offers clinical insights into the temporal and structural organization of this process, the latter derived from numerous data sources and professional disciplines, spanning rehabilitation, counseling, psychology, medicine, psychiatry, nursing, occupational and physical therapies, and social work. Second, the proposed outcome categories offer rehabilitation clinicians a multidomain and multidisciplinary perspective on how the affective, cognitive, and behavioral functioning of people with CID could be evaluated. The proposed outcome classification further allows for anchoring these outcomes within: (a) a number of contextual domains, including the living, learning, working, and recreational environments and (b) functional domains that range from person-focused to social-focused to community-focused areas. These clinical benefits could also serve as a blueprint for practitioners who seek to ensure that their clients and service recipients are not confined to merely a restricted, unidimensional view of clinical outcomes (e.g., decreased depression, job placement) but can benefit from a broader view of QOL-driven outcomes that addresses a wider spectrum of human functioning, across several and equally important life domains.
Research implications, stemming from the proposed model, should also be considered. First, the building blocks of the model suggest a wholistic, trans-CID view rather than individually tailored sets of models uniquely addressing different medical conditions and their associated adaptational processes. However, unique CIDs, reflecting differing functional limitations (e.g., mobility, sensory, cognitive, neurological, life-threatening), necessitate refinement of the model to best capture each condition's unique features. For example, application of the model to life-threatening CIDs (e.g., cancer) must take into account the unique structure and unfolding processes inherent in these conditions, such as emphasizing coping strategies geared toward managing pain and side effects of biomedical treatment (e.g., chemotherapy), and reactions associated with fear of death. In contrast, in medical conditions associated with mobility impairments (e.g., SCI), one would expect to observe coping strategies that focus on negotiating architectural barriers and possibly visibility-induced stereotypical societal attitudes. In addition, the model could be further refined along lines comparing CIDs incurred adventitiously (e.g., amputation) versus congenitally (e.g., muscular dystrophy) or for those being mostly stable (e.g., SCI) versus fluctuating (e.g., MS) in their progress.
Second, research on PA to CID also requires the application of both qualitative and quantitative longitudinal research designs, employing a large number of participants, to examine the unfolding of each of the model’s components over time. Furthermore, these designs should be better suited to examining the nature and direction of interactions among pertinent components, their concomitant evolution over time (e.g., contextual influences and coping strategies, personality and environmental resources, and specific psychological reactions), and how these reported and observed changes in turn influence both domain-specific and global outcomes. Third, as the approach to measuring QOL assumes its prominent role as a global, unifying outcome, it stands to reason that future research should apply a fine-tuned exploration of its most essential ingredients. For example, the QOL panel is composed of various domains, one of which consists of a tripartite functional subdomain of intra-, inter-, and extrapersonal categories. Research could benefit from further examination of the concordance among these three outcome criteria subdomains. Questions to be addressed may include (a) to what extent the functional levels indicated by these subdomains intercorrelate and to what degree are they CID-specific? and (b) are the functional levels indicated by each subdomain manifest differential outcome patterns when predicted by selected antecedent (e.g., contextual) and process (e.g., coping) variables or by empirically informed interactions among them?
Finally, although the proposed model does not speak directly about the influence of biophysical, psychosocial, or cognitive interventions on QOL-associated outcomes, future research would benefit from aggregated empirical data that indicate how the application of therapeutic interventions during both the inpatient and the outpatient rehabilitation period (i.e., the process phase of the model) affects, modifies, and expedites psychosocial outcomes.
Conclusion
The onset of acquired CID sets into motion a series of physical, psychological, social, and environmental processes that influence the individual’s life and determine the trajectory of any encountered future experiences. In this study, the author expands and updates an earlier version of this model, first conceived 20 years ago. In the revised model, the author sought to integrate more recent clinical observations, theoretical perspectives, and empirical findings that undergirded the original model. Discussed were the model’s tripartite structure of antecedent, process, and outcome components. The antecedent factors provide the CID-triggering events as well as the personal and sociocultural backdrop to better understanding one’s pre-CID life space. The process-associated factors provide the dynamic fabric within which PA to CID unfolds, including its medical, perceptual, psychological, interpersonal, and environmental constituents. Finally, to thoroughly and accurately assess the degree of success of the evolving post-CID processes, it is necessary to establish a set of comprehensive criteria, and these were provided by the multicomponent nature of the personal, interpersonal, and ecological outcomes addressed by the model’s third component.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.