
Abstract
Coronavirus disease (COVID-19) may cause long-lasting adverse consequences after acute recovery, including functional limitations and reduced work capacity. Individuals with long-lasting complications of COVID-19 are known as long-haulers. There is a knowledge gap on how COVID-19 complications affect return-to-work (RTW) efforts. We aimed to describe the challenges that long-haulers encounter when returning to work from the perspectives of rehabilitation professionals. In this study, four certified rehabilitation counselors and four rehabilitation physicians in U.S. outpatient rehabilitation centers participated in focus groups. Participants discussed challenges in working with long-haulers, including personal attributes, post–COVID-19 symptoms and complications, uncertain recovery and unpredictable outcomes, limited health care accessibility and support, and unsupportive work environments. Participants provide individualized services to meet long-haulers’ diverse needs as they do for all persons with disabilities, although they expressed uncertainty due to the variable disease course and risk of infection. Modifying workplace policies, especially gradual RTW, were frequently mentioned accommodations. The findings highlight the RTW issues of long-haulers. We provide recommendations on increasing awareness of the challenges and job accommodations of long-haulers.
Approximately 28 million people ages 18 to 64 years were diagnosed with COVID-19 between February 2020 and February 2021 in the United States (Centers for Disease Control and Prevention [CDC], 2020). Of that number, the CDC attributes 16% or 460,234 deaths to COVID-19 as the underlying cause (Andrenelli et al., 2020). While most people recover from COVID-19, a significant number can have long-term symptoms lasting weeks or even months that may require comprehensive rehabilitation services. One study estimated that between 10% and 87% of patients experience COVID-19–related symptoms 2 months after diagnosis (Rubin, 2020); in the United States specifically, nearly 3 million individuals still experience long-term symptoms from this illness (Ceravolo et al., 2020). Hereafter, we use “long-haulers” to describe people who experience long-lasting complications of COVID-19 (del Rio et al., 2020). Long-haulers experience persistent symptoms long after the typical recovery course.
The lasting sequelae of COVID-19 include significant physical and cognitive limitations. Physical impairments can include persistent fatigue, impaired lung function, myocardial injury, muscle deconditioning, various pain symptoms, and damage to the central nervous system (Del Rio et al., 2020; Pincherle et al., 2020; Rubin, 2020, 2021; Tenforde et al., 2020). Cognitive difficulties can include “brain fog,” prolonged confusion, decreased mental processing, memory problems, and impaired concentration (Pincherle et al., 2020; Rubin, 2020, 2021). Seizures and major mood disorders can also occur months after onset (Del Rio et al., 2020).
These persistent symptoms may significantly hinder community and vocational reintegration in individuals. In August 2020, a group of young and previously healthy long-haulers met with officials from the World Health Organization to discuss their experiences with the debilitating residual symptoms from COVID-19 (Sacks, 2020). Many struggled to work and maintain daily routines for months after their initial diagnosis. Specific difficulties include forgetting to complete household chores and completing self-care activities due to fatigue (Sacks, 2020), failing to exercise or maintain motor activities (Garrigues et al., 2020), word-finding difficulties (Prakash, 2020), need for excessive sleep and breaks (Prakash, 2020), depression and loneliness due to social distancing (Galea et al., 2020), and feelings of hopelessness when experiencing unpredictable and seemingly endless symptoms (Davis et al., 2020).
Long-haulers also report challenges in return-to-work (RTW) efforts. Many had to reduce work schedules (Davis et al., 2020), lost connections due to workplace social distancing (Galea et al., 2020), and faced termination due to extended time away from work. (Prakash, 2020). Unfortunately, while there is an urgent need for health care professionals to provide early rehabilitation and vocational services (Galea et al., 2020), there is no guideline for rehabilitation services focused on improving functional capacities for long-haulers (Law & Scott, 2020).
Identifying specific job accommodations tailored to long-haulers is an essential approach to minimize the negative consequences of persisting complications. However, most of the current literature regarding COVID-19 focuses on recognizing the job accommodations to help people with disabilities (PWD) maintain employment during the pandemic, such as teleworking and providing workspace modifications with a universal design to allow PWD to meet hygiene protocols (Adams et al., 2021; Sheppard-Jones et al., 2021; U.S. Equal Employment Opportunity Commission, 2020). There is a dearth of studies investigating job accommodations to support long-haulers RTW. Although the Job Accommodations Network (JAN) provides guidance for employers to support long-haulers (Batiste, 2021), it does not investigate whether the job accommodations address long-haulers’ diverse needs from the perspective of clinicians.
COVID-19 survivors have an increased risk of long-term disability due to neurological and cardiopulmonary impairment (Centers for Disease Control and Prevention, 2020; Couzin-Frankel, 2020; Sacks, 2020). While new therapies targeting these symptoms are under development (Bij de Vaate et al., 2020; Rubin, 2020), there is currently a paucity of treatment options to address these long-term impairments. The guidelines for managing COVID-19 suggested by the National Institutes of Health focus on pharmacologic interventions but not rehabilitation efforts for independent living nor support for RTW (National Institutes of Health COVID-19 Treatment Guidelines Panel, 2020). There is also a dearth of scientific literature and high-quality primary studies regarding the lingering symptoms and long-term effects of COVID-19 (Andrenelli et al., 2020; Gutenbrunner et al., 2020); therefore, studies on the impacts of rehabilitation for COVID-19–related disability are warranted (Galea et al., 2020; Gutenbrunner et al., 2020; Pincherle et al., 2020; Singh et al., 2020).
Few studies have investigated the challenges long-haulers experience in work environments. Furthermore, there is no research on what job accommodations and supports in the workplace address the needs of long-haulers. The novelty of the long-term recovery process from COVID-19 and the need to provide targeted job accommodations to allow long-haulers to RTW has become a key focus in the field of rehabilitation medicine and vocational rehabilitation. Learning from the rehabilitation professionals who are supporting long-haulers RTW can provide valuable information that fills knowledge gaps and provides practical guides for vocational rehabilitation. In this research, we targeted vocational rehabilitation counselors and physicians at outpatient rehabilitation centers because they gained early experience in helping people with disabilities return to work. We also described professionals’ experience of providing vocational services for long-haulers. The research aimed to:
Identify the challenges persons recovering from COVID-19 encounter when returning to work from the perspective of physicians and vocational rehabilitation counselors;
describe rehabilitation professionals’ experiences in working with long-haulers who RTW; and
describe the job accommodations that are helpful in returning to work.
Method
Participants
Participants were recruited at the outpatient and vocational rehabilitation (VR) clinics affiliated with a Midwestern U.S. rehabilitation center that actively provides services to individuals with COVID-19 long-term symptoms. The Institutional Review Board at Northwestern University reviewed and exempted the protocol (STU00213991). Investigators contacted potential participants at the outpatient and VR clinics via email. Eligibility criteria included individuals who are (a) licensed rehabilitation physicians or certified rehabilitation counselors (CRCs) and (b) have experience serving individuals recovering from COVID-19. We recruited all of the CRCs in the VR center affiliated with a rehabilitation hospital. The physicians were recruited from an outpatient rehabilitation center that serves people with disabilities living in the community. Because there were few VR centers and rehabilitation hospitals accepting long-haulers at the time when we recruited participants, the sample size was determined by the number of people who responded to our recruitment emails and who qualified for the study. Due to the difficulty of recruiting participants, we did not purposefully match participants on demographic characteristics and we were not able to select participants from diverse demographic backgrounds.
Procedures
Due to the COVID-19 pandemic, we conducted all research activities via virtual meetings, online surveys, and emails. First, we obtained participants’ consent and collected their background information through REDCap (Harris et al., 2009), a secure web application for online data collection. Second, we used Cisco WebEx, HIPAA-compliant telecommunication software, to host virtual focus groups. Both focus groups lasted around 90 min with 10 min for last comments and member reflections. The focus groups were held between December 2020 and January 2021. We developed a focus group guide to facilitate the discussion (the appendix). The moderator of the focus groups was a co-author with 40 years of experience designing and conducting qualitative research. A professional service transcribed the focus group recordings. We masked personal identifying information in the transcripts to assure confidentiality.
The research team consisted of a professor with a clinical psychology background (senior author), a post-doctoral fellow with graduate training in occupational therapy (first author), three CRCs with extensive job placement experience (fifth, sixth, and seventh authors), a medical student (third author), and three research assistants (second, fourth, and eighth authors).
Data Analysis
Being a qualitative investigation, the research team conducted a content analysis based on the transcripts of the focus groups (Bazeley, 2013). We used the NVivo Software (version 12) to categorize the codes and create conceptual themes (QSR International, 2018). As Bazeley (2013) suggests, we developed a codebook to address the three research aims. To develop the codebook, five researchers listened to the audio recordings and independently made reflective listening notes to capture the key points of a focus group. The five researchers noted: (a) the salient or important themes to capture, (b) the topic or themes that related to the researcher’s experience as a CRC, (c) the challenges of RTW after COVID-19, and (d) the job accommodations mentioned in the focus group. The first author then incorporated the five reflective listening notes and developed the first version of the codebook. All authors met to discuss and revise the codebook. We refined the codebook as we analyzed the focus group transcripts. We organized the codebook to reflect the study aims: (a) challenges encountered in a RTW, (b) health care professionals’ experience in helping long-haulers RTW, and (c) the job accommodations or resources helpful to support long-haulers who are recovering from COVID-19.
Next, four researchers coded transcripts by labeling text with codebook entries. Two authors coded each transcript independently. The fifth coder, a CRC, then reviewed, compared, and integrated the codes for each transcript. All coders met to resolve discrepancies and reach consensus. After reconciling discrepancies, all authors met to review the results, discuss ways to present the results, and interpret the findings.
Study Credibility and Trustworthiness
We used three strategies to achieve and protect the research rigor: (a) Participant self-reflection—at each focus group, we asked one participant to sit in the group silently and observe the discussion. At the end of each focus group, the participant summarized the discussion, reflected the salient themes addressed in the focus group, and facilitated self-reflection with other participants. (b) Double coding—we had two coders independently code the data. The coders met with a third coder to develop a consensus on analysis. (c) Member check—we invited focus group participants to review the analytic summary and provide feedback to ensure the results accurately represent their perspectives.
Results
Participants
We scheduled separate focus groups for the two professions. We recruited four CRCs and four attending physicians at the outpatient centers. Table 1 shows participant characteristics. Most participants were White (n = 7) and female (n = 7). One participant reported her race as “Other,” and one participant was male. Mean age was 52.8, and most had decades of experience in providing rehabilitation for people with physical disabilities. Physicians reported treating 10 to 29 patients recovering from COVID-19; most of their patients were retired and not seeking to RTW. For each physician participant, less than five of their patients with COVID-19 intended to RTW. In contrast, CRCs had served 5 to 10 or more long-haulers recovering from COVID-19 who intended to RTW, with only 3 long-haulers successfully doing so with VR assistance thus far. Others (a) were still managing long-hauler complications and symptoms, (b) were engaged in rehabilitation services, (c) decided not to RTW due to long-term disability, or (d) were looking for new jobs. Counselors reported a wide range of employment history in the long-haulers they worked with, including executive assistant, school aide, radiology technician student, emergency medicine physician, pharmacist, factory worker, supervisor, bagger, business owner, janitor, police officer, truck and limousine driver, sales representative, and therapist.
Characteristics of Participants.
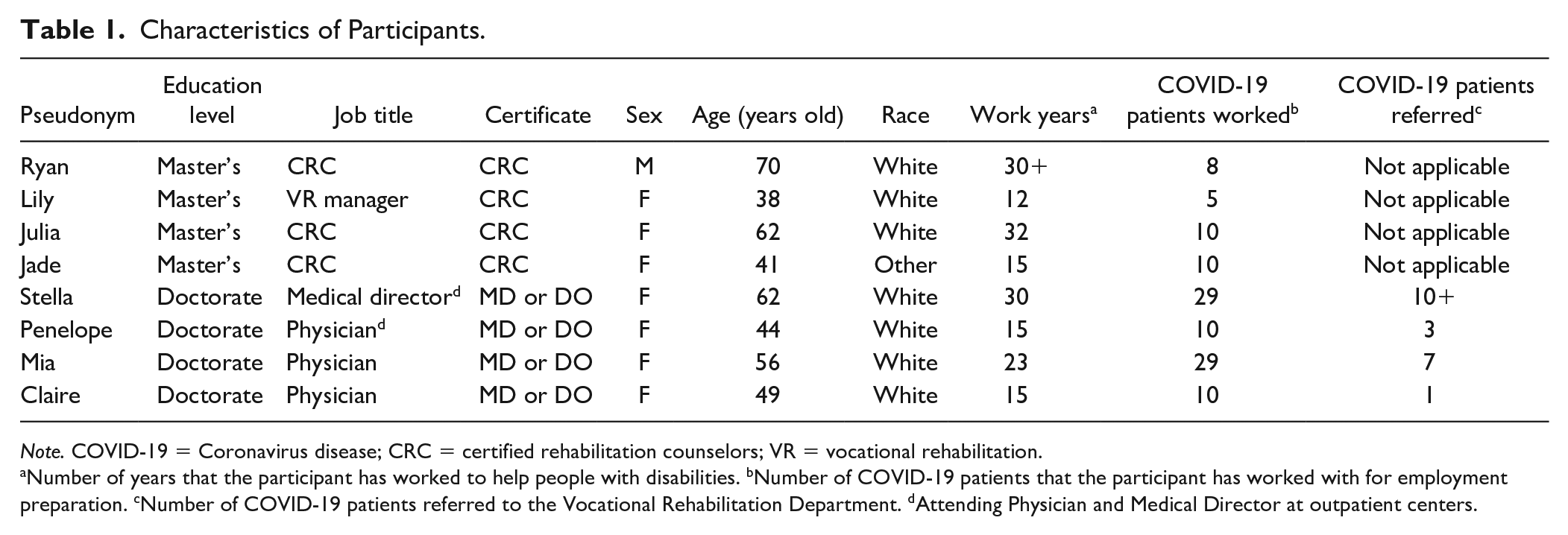
Note. COVID-19 = Coronavirus disease; CRC = certified rehabilitation counselors; VR = vocational rehabilitation.
Number of years that the participant has worked to help people with disabilities. bNumber of COVID-19 patients that the participant has worked with for employment preparation. cNumber of COVID-19 patients referred to the Vocational Rehabilitation Department. dAttending Physician and Medical Director at outpatient centers.
Aim 1: Challenges Encountered in RTW
Focus group participants described various challenges that patients encountered in vocational reintegration. We categorized them as attributes of persons recovering from COVID-19, post-COVID-19 symptoms and complications, uncertain COVID-19 recovery and unpredictable outcomes, limited health care accessibility and support, and unsupportive work environment.
Attributes of persons recovering from COVID-19
Age is an issue in employment independent of COVID-19. Many patients had difficulty returning to work or finding a new job because they had reached or neared retirement age, although some of them were employed full-time prior to their illness. Many long-haulers were unable to return to their usual job responsibilities, and many reported significant financial pressures and concerns about wage loss. Some long-haulers who were not hospitalized told their outpatient physicians that they were unable to access VR support because they were either unaware of the long-term complications of COVID-19 or did not know about the existence of VR. Participants also mentioned fear and how it negatively influences long-haulers’ readiness to RTW. Julia, a CRC, shared, I think a reinfection. A lot of the ones [people recovering from COVID-19] I talked to are really afraid of getting sick again. I think it must’ve just been a horrid experience for the people we saw. They were alone. On ventilators, probably terrified. And not knowing if they were going to live or not.
In addition, focus group participants reported that patients who were referred to VR may not adhere to the program suggestions. Lily, a CRC, described, [The client recovering from COVID-19] was not following our overall recommendations, which is a prime example of an individual who is struggling with the new reality of his current situation. . . . He wanted to be that provider for his family, so he was going to figure out how to make it work.
Post–COVID-19 symptoms and complications
Another prominent issue was the variability of post–COVID-19 symptoms, which complicated recovery and delayed RTW. While cognitive delays and physical deconditioning were common sequelae, participants also reported comorbid conditions such as Guillain-Barré, paralysis, paresthesia, strokes, and other ischemic injuries. Participants mentioned the mental and emotional consequences of COVID-19 infection, especially amid the financial burden posed by the pandemic; typical manifestations were depression, fear of reinfection, and concerns about unemployment.
Uncertain COVID-19 recovery and unpredictable outcomes
Beyond the diverse symptoms complicating the rehabilitation approach, there was also uncertainty in the recovery trajectory. Unclear prognosis created distress, as patients could not anticipate improved function. This ambiguity prevented CRCs from communicating RTW schedules with employers. As Julia, a CRC, stated, We run into situations with employers, who maybe want to know: when will they [people recovering from COVID-19] be back? We don’t know, we don’t have any way of projecting, if it’s going to get better or not. [About the client who worked in the factory], I have no idea what to expect for her future. It’s hard to tell her what to expect. That’s hard for her. She doesn’t know. She has three kids, and she wants to take care of them. She’s always worked. But we just have no idea what direction to go.
Limited health care accessibility and support
Physicians mentioned that insurance plans frequently do not include mental health coverage, despite Congress’ passage of the Mental Health Parity and Addiction Equity Act of 2008. They observed their patients having difficulty accessing VR services due to a lack of transportation support during the pandemic. Certified rehabilitation counselors stated that medical professionals sometimes overrode their suggestions. Lily, a CRC, stated, [The client recovering from COVID-19] had a laundry list of recommendations. However, they just had their neurologist give them a full duty release to return to work despite our recommendations.
Unsupportive work environment
Employers often complicated the VR process. Employers wanted to know the long-term consequences of COVID-19 on their employee’s ability to perform job duties, which was difficult to estimate, given the paucity of research. Many long-haulers were unable to RTW due to the physical demands of their job. While some employers were willing and able to provide accommodations, many were not. One physician said, There are certain jobs that will not accommodate the patients and say, “if you can’t do X, Y, and Z, you can’t come back to work.”
Aim 2: Rehabilitation Professionals’ Experience of Helping Long-Haulers RTW
Table 2 shows the strategies that participants reported to support workers recovering from COVID-19 to return to employment. They reported no novel approaches or strategies. Due to the variety of symptoms, most focus group participants stated that they provided individualized services to meet patients’ diverse needs, as they do for all persons with disabilities. However, participants expressed uncertainty in working with patients with COVID-19 due to the unknown disease course and risk of infection. Stella, a physician, stated,
Strategies That VR and Physicians Used to Help Long-Haulers.
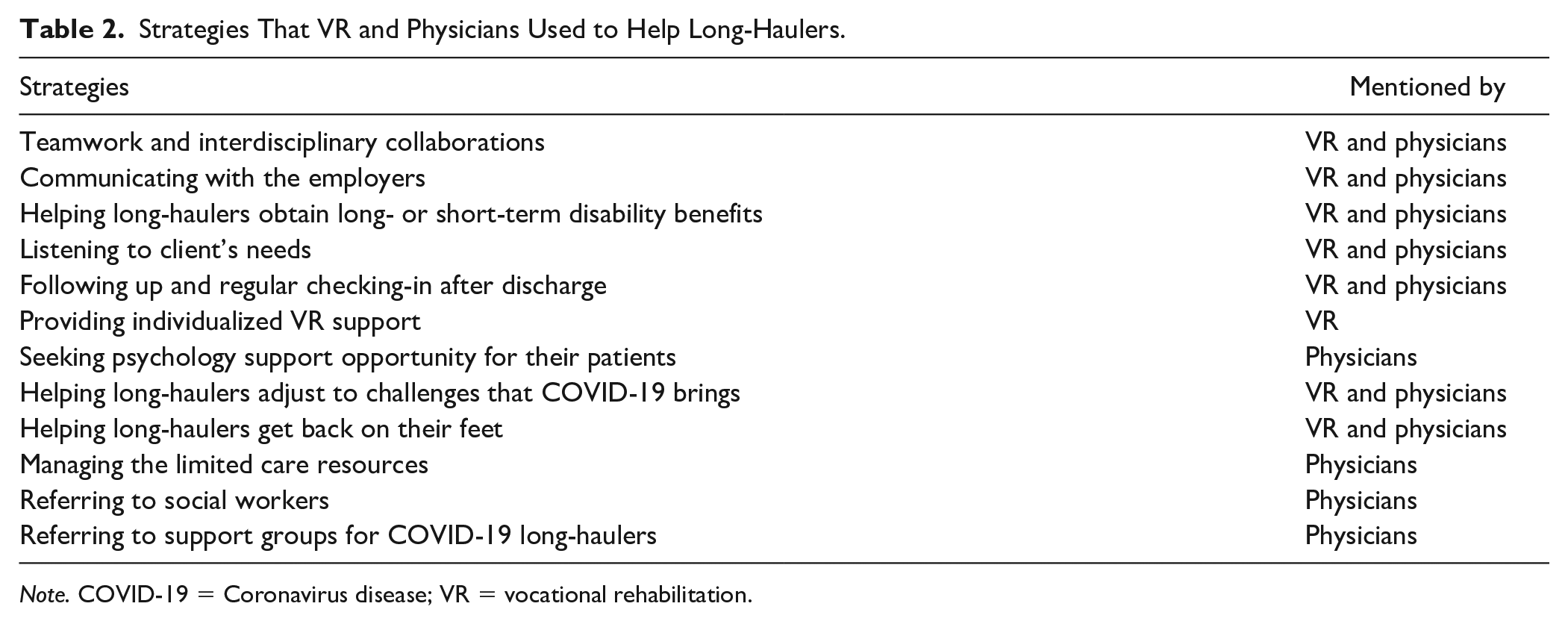
Note. COVID-19 = Coronavirus disease; VR = vocational rehabilitation.
Initially, therapists were scared to work with them [patients recovering from COVID-19] . . .when we were first opening up our clinic and we got the first COVID-19 patient, everybody was a little hesitant. We took care of them and we did all the appropriate protocols, but I think that there was a bit of fear in caring for these patients because the diagnosis was so unknown.
Some participants shared their fear of approaching patients with suspicious symptoms: I had a patient come into the clinic. They called me to see a toe that was infected, and all of a sudden, he starts coughing this deep cough. I literally went back. I could not look at his toe, which was bad. I’m like, “You have to leave the clinic and get tested for COVID right now.” And, as he’s going down, he’s coughing and coughing. And, I was completely . . . I reacted, probably overreacted. I am now vaccinated and I have my mask, but it was like he was untouchable. “Get out of the clinic. You’re going to expose everybody. You’re going to get everybody sick.”
The physician reported feeling guilty for rejecting patients with COVID-19–like symptoms, as Stella shared: It was so bad. I think he was hurt. He felt bad, and then I felt bad.
The participants suggested learning more about the short- and long-term symptoms of COVID-19 and the recovery trajectory for long-haulers. They also stressed the importance of offering psychological support for patients recovering from COVID-19.
Aim 3: Job Accommodations or Resources That Are Helpful in RTW
Job accommodations
Table 3 lists the job accommodations CRCs and physicians used when helping long-haulers RTW. We used the typology developed by Wong et al. (2021) to categorize job accommodations. Modifying workplace policies, especially gradual RTW, was the most frequently mentioned accommodation. Participants mentioned other job accommodations, including flexible scheduling, modifying job responsibilities, and modifying architecture or workplace environment, to support long-haulers who experienced fatigue, pain, and memory loss. However, many post–COVID-19 patients had to investigate using time off options and insurance policies instead of RTW using job accommodations. Jade, a CRC, shared,
Job Accommodations Used With Post-COVID Patients.

Note. COVID = Coronavirus disease; VR = vocational rehabilitation.
I think about one gentleman in particular, where he was a janitor at a university and incurred a stroke because of COVID. And, he’s unable to do the physical parts of the job. So he ended up applying for workmen’s comp, and it got approved.
Policy modification
Participants from both focus groups stated that long-haulers applied for workers’ compensation, short- and long-term disability, and other insurance benefits. While some employers modified company sick leave policies to accommodate employees’ COVID-19–related disability during the pandemic, there were others who did not. For employers without proactive COVID-19 policies, employees had to use their personal time off until they could work full-time. Both the physician and the CRC participants agreed that proactive employment policies would be helpful to address the RTW needs of long-haulers. As stated by Julia, a CRC, I’ve been impressed with the employers who had COVID leaves. I think being aware of the fact that this is something that we don’t know all the information about it and what’s happening. And, the employers who have been flexible about giving people the time that they need, although I’d like to see that with other groups we work with as well. That would be nice if there were more proactive leave policies.
Resources for regaining employment
Referring long-haulers to the state Division of Rehabilitation Services and suggesting that they apply for Social Security Disability Insurance were additional resources mentioned by CRCs and physicians. Participants mentioned support groups as a resource to help long-haulers deal with disability and navigate the unfamiliar journey of recovery. As Julia, a CRC, shared, I have another client who was also depressed. He was a part of three different COVID support groups. One at [the outpatient center]. And, then he had found two [other support groups] on his own that he participated in. He found that very helpful to talk to other people who were experiencing the same kinds of uncertainties.
Results of Member Check
After we completed the qualitative analysis, we emailed a two-page summary of the findings to participants and asked them to provide feedback. Four of eight participants responded, and all of them stated that the results represented their experiences. Examples of their comments are: “It seems that you covered what we discussed with you very well,” and “The summary is reflective of my experience.”
Discussion
This qualitative study provides novel and clinically relevant information about the challenges experienced by persons recovering from COVID-19 when RTW, including personal attributes, post–COVID-19 symptoms and complications, uncertain COVID-19 recovery and unpredictable outcomes, limited health care accessibility and support, and unsupportive work environments. To help long-haulers RTW, we found that although rehabilitation professionals adopted the same approaches as they used for people with other disabilities, they expressed uncertainty in working with long-haulers due to the unknown disease course and risk of infection. The rehabilitation professionals shared the job accommodations and resources that are helpful for long-haulers to manage their long-lasting symptoms and emotional needs in the workplace, such as gradual RTW, flexible scheduling, and support groups. Finally, the participants suggested that providing proactive employment policies would be helpful to address the RTW needs of long-haulers. The findings highlight the RTW issues of long-haulers. We provide recommendations on increasing awareness of long-haulers’ needs when returning to work. Strengths of this study include the clinical importance of the topic, extensive collaboration with CRCs, and rigorous data analysis procedure.
Unknown COVID-19 Recovery Limits Service and Support Provision
Participants of this study described the unpredictability of COVID-19 recovery, which presented major challenges in the RTW process. Given the novelty of the disease, there is a paucity of long-term (more than one year) data on permanence and severity of symptoms and functional limitations. In addition, COVID-19 symptoms can affect every major organ system, often in unpredictable and debilitating ways (Davis et al., 2020; Leung et al., 2020). As a result, physicians and CRCs cannot provide a definitive prognosis to patients and their employers, creating tension and uncertainty for all. Ambiguity regarding prognosis limits patients’ ability to adjust to a new life and leaves employers uninformed about the duration or permanency of job accommodations.
Considerations When Supporting Long-Haulers to Return to Work
Because nearly one-fourth of COVID-19 survivors experience symptoms after 5 weeks (Davis et al., 2020), the disease burden is substantial and requires thoughtful consideration when planning VR services. Vocational rehabilitation services serve people with disabilities who experience many of the same challenges that long-haulers do during the pandemic. For instance, both long-haulers and individuals with disabilities may have worsening mental health or neurologic conditions, increased difficulties with activities of daily living, and difficulty accessing health care and physical therapy (Lebrasseur et al., 2021). As a result, VR strategies used for individuals with disabilities may translate well to long-haulers. The variability and unpredictability of long-hauler symptoms require an individualized, multidisciplinary effort from rehabilitation medicine specialists, physical and occupational therapists, social workers, CRCs, and mental health providers given the profound physical and psychiatric sequelae (Leung et al., 2020; Mendelson et al., 2021). In addition, individuals with COVID-19 may face undue stigma due to unknown or misinformed transmissibility data, drawing parallels to HIV-related stigma from the 1980s. As such, stigma reduction interventions from that era may inform modern-day efforts for COVID-19.
Policy Modifications and Guidance for Employers During the COVID-19 Pandemic
Americans With Disability Act (ADA) and amendments
Employers are grappling with policies related to accommodating individuals who RTW after COVID-19. The ADA amendments broadened coverage in 2008 and specified that temporary impairments can qualify as disabilities (Dill, 2020). This Act increases the likelihood that long-haulers will meet the definition of disability (Office of Disability Employment Policy, 2008). Consequently, CRCs should consider the chronicity of illness experienced by long-haulers in the context of the legal protections provided by the ADA and the Family and Medical Leave Act (FMLA).
Guidance from CDC
The CDC developed guidance for businesses and employers on emerging workplace policies related to COVID-19 (CDC, 2021). Among their suggestions is identifying a workplace coordinator, whose job is to manage COVID-19–related concerns. The CDC also recommends that companies implement flexible sick leave and supportive practices to assist employees’ RTW. The recommendations include non-punitive sick leave policies and provide guidance for the use of the FMLA or the Families First Coronavirus Response Act. Most states have passed COVID-19 specific laws and expanded coverage for worker’s compensation (Phillips, 2020). However, the scope of coverage varies widely from state to state (Sams, 2020).
Regulations for disease control and confidentiality protection in workplace
Numerous concerns about the Health Insurance Portability and Accountability Act as it relates to COVID-19 have arisen since the WHO’s declaration of a pandemic in March 2020. Hamilton (2020) cautions that employers must offset the need to keep their workforce safe while safeguarding the privacy of the infected employee and adhering to privacy laws. The ADA would typically limit an employer’s ability to ask health-related questions of their employees. However, the Equal Employment Opportunity Commission has determined that the ADA should not interfere with employers who are following the advice of the CDC and has supported the policy of informing employees of any workplace exposure in an effort to decrease the spread of the disease (U.S. Equal Employment Opportunity Commission, 2020). Employers must be aware of their employee’s COVID-19 diagnosis. Employers are also required to comply with regulations regarding confidentiality and the prevention of workplace stigma for employees diagnosed with COVID-19.
Resource from job accommodations network
The JAN recently published a list of accommodations specific to people with impairments resulting from COVID-19 (Batiste, 2021). One example, relevant to persons experiencing dyspnea, is to use alternative masks, allowing removal of mask when appropriate, reducing physical exertion, reducing workplace triggers, allowing time for medical treatment, job restructuring, developing a plan of action to deal with sudden exacerbations, and allowing telework. Job Accommodations Network also recommends that employees use an interactive process to determine if employees will continue to need job accommodations for ongoing COVID-19–related impairments.
Implications for Clinical Practice to Serve Long-Haulers
Clinical implications include using an individualized interdisciplinary approach with rehabilitation counseling support, job assessment, and identification of specific job accommodations when assisting RTW after COVID-19. Certified rehabilitation counselors are an invaluable resource to other rehabilitation professionals, workers recovering from COVID-19, and employers regarding legislative and accommodations resources. Certified rehabilitation counselors should monitor long-haulers’ symptoms and modify job accommodations as the person’s functioning changes. Rehabilitation counseling professionals working with long-haulers should collaborate closely with physicians and allied health clinicians to support RTW efforts due to the changing nature of this chronic disease.
Implications for Future Research
The job accommodations identified in this study are summarized in Table 3. These are the salient job accommodations reported by the focus groups and are not intended to be all-inclusive list. Further research is warranted as long-haulers return to the workforce. Research should focus on COVID-19 long-haulers who can report the specific challenges they encountered in reentering the workforce with COVID-19–related impairments and the job accommodations they found to be helpful. As more information becomes available on the length and permanency of impairments from COVID-19, future research may be able to identify the specific job accommodations needed by long-haulers.
Strengths and Limitations of the Research
The strength of this study is that it addresses the importance and urgency of recognizing the RTW experiences for COVID-19 long-haulers and strategies used by service providers to assist them. These service providers included highly experienced rehabilitation medicine physicians and vocational rehabilitation counselors currently treating COVID-19 long-haulers. The main limitation is the small sample size of focus group participants, all of whom worked in a Midwestern rehabilitation hospital, limiting the generalizability of findings. As there were few rehabilitation professionals working with long-haulers at the time when we collected the data, we were not able to recruit participants from diverse backgrounds, including race and gender. Our study sample reflects the limited number of VR professionals who work with COVID-19 survivors and temporary closures among VR centers during the pandemic. Finally, we only included outpatient physicians and CRCs in the study. Thus, the findings may not be representative of other health care professionals working with COVID-19 long-haulers or long-haulers themselves. To describe the experience of RTW for long-haulers, future research should investigate long-haulers’ firsthand experience of receiving VR services and include health care professionals from diverse backgrounds. As the RTW process is optimized by a multidisciplinary approach, recruiting a larger sample size with a greater variety of health care specialists and long-haulers would be beneficial in future research.
Conclusion
This study provides new information about the challenges experienced by long-haulers and the experiences of rehabilitation professionals in assisting in their RTW. While the VR fundamentals and job accommodations for long-haulers often remain the same as for all people with disabilities, this research highlights the unique needs of this population. Future research should follow long-haulers over extended periods to monitor their recovery, overall functioning, and ability to maintain employment. This study provides recommendations on increasing awareness of long-haulers’ unique challenges, clinical implications, and the specific accommodations needed to address their needs. COVID-19 may require revision of the ADA’s definition of temporary disability and clarifying the length of time a condition must last before an individual qualifies as a person with a disability.
Footnotes
Appendix
Summary of Focus Group Guides.
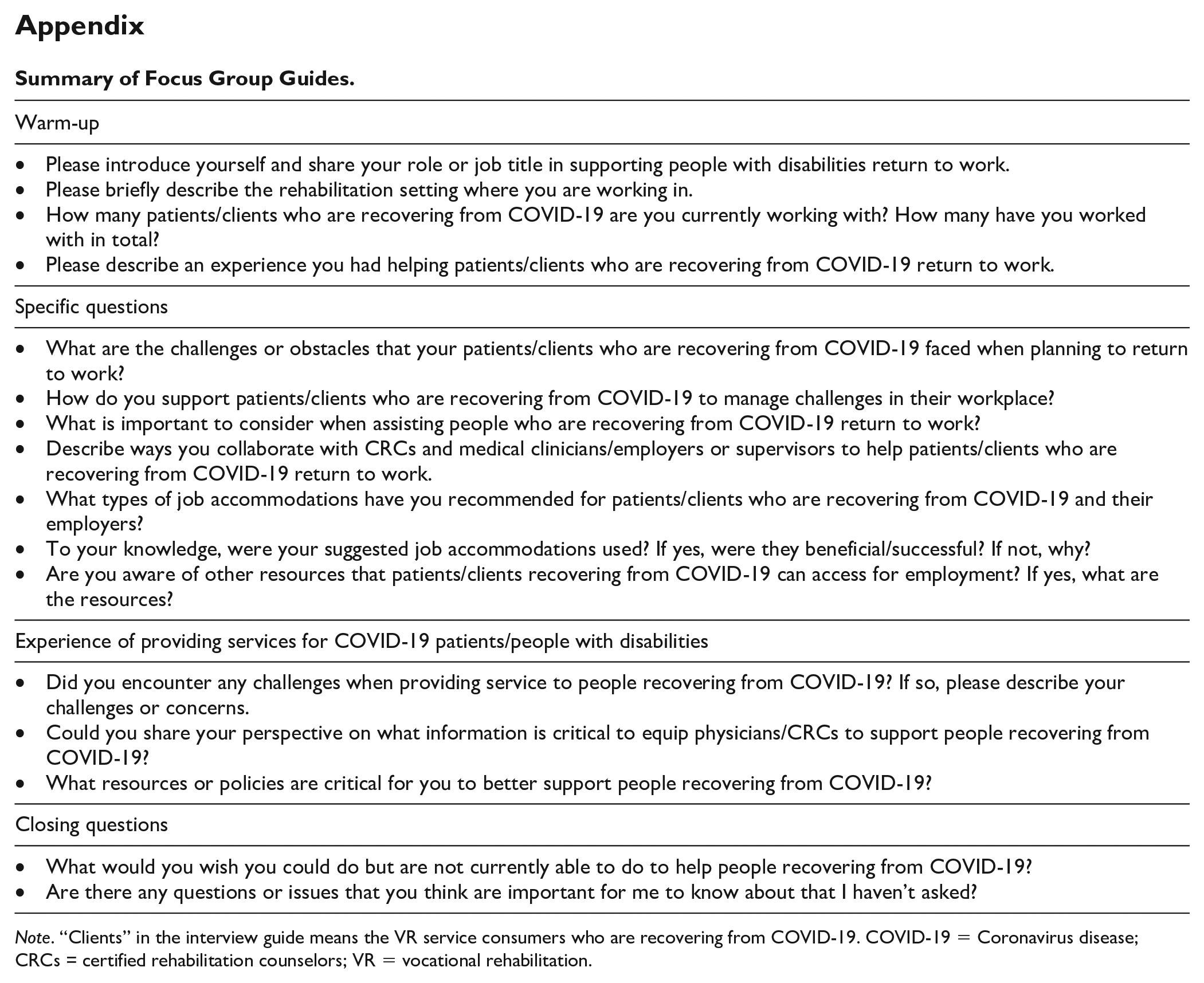
| Warm-up |
| • Please introduce yourself and share your role or job title in supporting people with disabilities return to work. • Please briefly describe the rehabilitation setting where you are working in. • How many patients/clients who are recovering from COVID-19 are you currently working with? How many have you worked with in total? • Please describe an experience you had helping patients/clients who are recovering from COVID-19 return to work. |
| Specific questions |
| • What are the challenges or obstacles that your patients/clients who are recovering from COVID-19 faced when planning to return to work? • How do you support patients/clients who are recovering from COVID-19 to manage challenges in their workplace? • What is important to consider when assisting people who are recovering from COVID-19 return to work? • Describe ways you collaborate with CRCs and medical clinicians/employers or supervisors to help patients/clients who are recovering from COVID-19 return to work. • What types of job accommodations have you recommended for patients/clients who are recovering from COVID-19 and their employers? • To your knowledge, were your suggested job accommodations used? If yes, were they beneficial/successful? If not, why? • Are you aware of other resources that patients/clients recovering from COVID-19 can access for employment? If yes, what are the resources? |
| Experience of providing services for COVID-19 patients/people with disabilities |
| • Did you encounter any challenges when providing service to people recovering from COVID-19? If so, please describe your challenges or concerns. • Could you share your perspective on what information is critical to equip physicians/CRCs to support people recovering from COVID-19? • What resources or policies are critical for you to better support people recovering from COVID-19? |
| Closing questions |
| • What would you wish you could do but are not currently able to do to help people recovering from COVID-19? • Are there any questions or issues that you think are important for me to know about that I haven’t asked? |
Note. “Clients” in the interview guide means the VR service consumers who are recovering from COVID-19. COVID-19 = Coronavirus disease; CRCs = certified rehabilitation counselors; VR = vocational rehabilitation.
Author Note
Jasin Wong is now affiliated with National Tsing Hua University, Taiwan.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This research was supported by the National Institute on Disability, Independent Living, and Rehabilitation Research (NIDILRR) (Grant Number: 90RTEM0001).