
Abstract
This study examined the mediating role of psychological inflexibility in the relationship between resilience and marriage satisfaction among parents of children with developmental disabilities in a Turkish sample using Bayesian structural equation modeling (BSEM). Data were collected from 420 participants using the Acceptance and Action Questionnaire-II, the Connor-Davidson Resilience Scale, and the Marriage Life Scale. Results supported the hypothesized model with adequate fit (PPP = .48), with psychological inflexibility partially mediating the relationship between resilience and marriage satisfaction. Resilience was negatively associated with psychological inflexibility (β = −.73, 95% CI [−0.78, −0.68]), and psychological inflexibility was negatively related to marriage satisfaction (β = −.31, 95% CI [−0.40, −0.22]). The indirect effect of resilience on marriage satisfaction through psychological inflexibility was significant (β = .23, 95% CI [0.16, 0.30]). Gender differences were examined, with results suggesting similar structural patterns across genders, though males showed slightly higher levels of resilience and marriage satisfaction. The findings highlight the importance of psychological inflexibility as a mechanism through which resilience influences marriage satisfaction in parents of children with developmental disabilities.
Keywords
The global prevalence of developmental disabilities and their socioeconomic impact on families has become a significant public health concern. According to the Global Burden of Disease Report 2017, the financial burden of disabilities among children and adolescents increased by 4.3% between 1990 and 2015 (Olusanya et al., 2018). Data from the Centers for Disease Control and Prevention (2024) indicate that approximately 15% of children between the ages of 3 and 17 years are affected by conditions such as autism spectrum disorder, Down syndrome, cerebral palsy, and intellectual disabilities (Boyle et al., 2011). These figures underscore that developmental disabilities are lifelong conditions that profoundly impact the quality of life, financial resources, and emotional stability of the entire family unit. In this context, the emergence of a developmental difference—often contrary to parental expectations—creates a profound psychological impact and leads to significant distress (A. W. Cheng & Lai, 2023; Sharma et al., 2021). Parents of children with developmental disabilities (PCDDs) consistently report higher levels of depression, anxiety, and stress compared to parents of typically developing children, while exhibiting lower levels of hope and subjective well-being (Gur & Reich, 2023; Ma et al., 2023). This adaptation process, often referred to as psychological adjustment, requires parents to reshape social relationships, make critical career sacrifices, and reorganize financial resources (Turnage & Conner, 2022). Scholars have examined this complexity through various theoretical lenses, including the grief model, chronic sorrow, and the ABCX model of family stress (McCubbin & Patterson, 1983), all of which highlight the arduous nature of long-term adaptation.
Beyond individual adjustment, these challenges exert significant pressure on the marital subsystem. Research consistently demonstrates that PCDDs experience higher rates of marital discord and divorce due to increased caregiving demands and chronic emotional strain (Anchesi et al., 2023; Chan & Leung, 2020). However, there is a growing recognition that the shared experience of raising a child with special needs can also strengthen marital bonds through collaborative problem-solving and a sense of shared purpose (Eren-Kanbir & Akşit, 2020; Manor-Binyamini, 2016). Consequently, understanding the specific factors that contribute to marital satisfaction in this population is essential for developing effective family-based interventions.
Furthermore, these relational dynamics are deeply embedded within cultural frameworks. In collectivist cultures—such as Türkiye, the Middle East, and parts of Asia—the experience of disability involves different social markers than in individualistic Western societies. Factors such as family honor, social stigma, and gender roles fundamentally shape the parental experience (Papadopoulos et al., 2013). For instance, while extended family can provide vital support, it can also serve as a distinct stressor (Kağıtçıbaşı, 2007). Similarly, religious beliefs often dictate the meaning attributed to the disability; viewing the child as a “spiritual test” or a “gift” can facilitate positive religious coping and enhance resilience (Güleç-Aslan, 2017). These nuances necessitate culturally sensitive approaches rather than “one-size-fits-all” intervention strategies.
In light of these complexities, although current intervention programs target distress reduction, many fail to address the lifelong nature of the adaptation process. This gap highlights the importance of “psychological resilience”—the ability to adapt and thrive despite adversity (Lu et al., 2022). Resilience acts as a protective factor that buffers the negative effects of caregiving on family well-being (Gagat-Matuła, 2022). Therefore, examining how resilience interacts with variables such as marital satisfaction within a specific cultural context is vital for advancing the field of rehabilitation counseling and promoting long-term family flourishing.
Resilience and Marital Satisfaction
In academic literature, the concept of resilience has been defined in multiple ways. Aburn et al. (2016) noted existing explanations revolve around “overcoming challenges,” “adaptation,” “experience,” “good mental health,” and “bouncing back.” The common thread is confrontation with difficult events and responses during this process (Ma et al., 2023). Connor and Davidson (2003) defined resilience as characteristics including internal resources, environmental support mechanisms, and coping strategies helping individuals adapt to stressful events.
PCDD resilience has been widely discussed (Broll et al., 2025; Ma et al., 2023; Widyawati et al., 2023). Studies have highlighted risk factors influencing resilience, including disability type, chronicity, symptom severity (Flores-Buils et al., 2025), and child’s age (Ekas et al., 2015). Protective factors include social support (Broll et al., 2025), time since diagnosis, locus of control, cognitive appraisal, and spirituality (Ekas et al., 2015). In the Turkish context, spirituality often acts as a significant cultural buffer; the perception of the child’s disability as a “divine test” or “fate” can foster a sense of purpose, thereby enhancing psychological endurance (Güleç-Aslan, 2017).
A significant factor influencing PCDD resilience is perceptions regarding marital life. Marital satisfaction serves as a protective factor (Gagat-Matuła, 2022; Güçlü & Hürmeydan, 2024; Zoromba et al., 2024). Positive marriage perceptions enable parents to stand stronger against challenges and derive life satisfaction (Seligman & Csikszentmihalyi, 2014). Literature reports PCDDs tend to perceive marital relationships negatively (Golan-Bayazy & Gur, 2024; Markodimitraki et al., 2024). PCDDs often reorganize lives, focusing on children’s needs after diagnosis, altering role definitions between spouses (Daks & Rogge, 2020). In Turkish society, where traditional gender roles are prevalent, the caregiving burden falls disproportionately on mothers, which may lead to emotional exhaustion and a sense of isolation within the marriage (Türk et al., 2025). Many parents confine marital relationships within parenting role boundaries, negatively impacting marital satisfaction. Compared to parents of typically developing children, PCDDs exhibit lower marital satisfaction and higher divorce rates (Anchesi et al., 2023).
However, limited literature shows family relationships can strengthen following a child’s disability (Eren-Kanbir & Akşit, 2020; Manor-Binyamini, 2016). This strengthening is often observed in collectivistic cultures where the “Family Model of Emotional Interdependence” (Kağıtçıbaşı, 2007; Mayer et al., 2012) provides a theoretical framework for understanding these dynamics. Unlike the Western model of independence, this model suggests that while economic dependence decreases with urbanization, emotional interdependencies remain core to the family unit. In the context of PCDDs, this manifests as a ‘related-autonomous’ self-construal, where parents maintain high levels of intimacy and psychological loyalty to the extended family. This interdependence functions as a socio-emotional safety net; the psychological burden is not confined to the marital dyad but is shared across a communal network, which can prevent the erosion of marital satisfaction and foster collective resilience (Kağıtçıbaşı, 2007). Better understanding of this phenomenon and its relationship with resilience is needed.
However, simply identifying a relationship between resilience and marital satisfaction is not enough to guide intervention. To develop effective counseling strategies, it is essential to understand the underlying mechanisms that link these two constructs (Jo et al., 2024). An increasing amount of research in rehabilitation and counseling psychology highlights psychological flexibility as a key factor in this process (Golan-Bayazy & Gur, 2024; Whittingham et al., 2019). In this context, examining psychological inflexibility provides a deeper understanding of how PCDDs manage caregiving stress while maintaining marital satisfaction. This concept, which is central to Acceptance and Commitment Therapy (ACT), provides a model for understanding how individuals can handle distress and still engage in meaningful, values-driven actions. Specifically, psychological inflexibility acts as the mechanism through which caregiving-related distress permeates the marital bond. For PCDDs, ‘cognitive fusion’ with negative thoughts about their child’s future or ‘experiential avoidance’ of the pain associated with disability can lead to emotional withdrawal from their spouse. By applying the ACT framework, we can see that marital satisfaction is not merely threatened by the external stress of a child’s disability, but by the internal rigidities—such as an inability to remain present or a struggle with difficult emotions—that prevent couples from supporting one another. Thus, connecting ACT to these constructs allows for a targeted understanding of how fostering psychological flexibility can preserve the ‘parenting-marital’ balance and enhance overall family resilience.
Psychological Inflexibility Model
ACT aims to help individuals live meaningful, enriched lives (S. C. Hayes, 2022; S. C. Hayes et al., 2012). Psychological flexibility encompasses being present, defusion, and acceptance, while inflexibility involves experiential avoidance, cognitive fusion, and dysfunctional behaviors. Ruiz et al. (2024) define psychological inflexibility as inability to engage in behaviors aligned with valued purposes or modify existing behaviors.
Although psychological inflexibility and resilience belong to different theoretical frameworks, they are conceptually connected through their influence on adaptive functioning. While resilience reflects a positive adaptive ability, psychological inflexibility can act as a significant obstacle to this process. Recent reviews suggest that psychological inflexibility may be an important element of resilience (Jo et al., 2024; Meyer et al., 2019). Studies show that psychological inflexibility is linked to distress among PCDDs (X. Cheng et al., 2021; Golan-Bayazy & Gur, 2024; Sairanen et al., 2018; Whittingham et al., 2019), and this distress is associated with resilience levels (Ma et al., 2023). Improving resilience in PCDD populations could help reduce psychological inflexibility.
Psychological inflexibility emerges as noteworthy in marital relationships. A meta-analysis revealed it associates with individuals being less supportive, empathetic, and compassionate toward partners (Daks & Rogge, 2020). Golan-Bayazy and Gur (2024) found significant relationships between psychological inflexibility and marital quality in parents of autistic children. Understanding dynamics between PCDD resilience and marital satisfaction is essential. While high resilience may influence marital satisfaction, psychological inflexibility could determine whether this influence is positive or negative. Gender differences in psychological distress (Bitsika et al., 2013) warrant investigation in these relationships.
The Present Study and Model Specification
Based on the theoretical framework and empirical evidence reviewed above, we developed a mediation model to examine the relationships among resilience, psychological inflexibility, and marriage satisfaction in parents of children with developmental disabilities (PCDDs). The model specification was guided by the following theoretical reasoning: First, resilience was positioned as the independent variable because it represents a stable adaptive capacity that enables individuals to cope with adversity (Connor & Davidson, 2003). In the context of PCDDs, resilience reflects the internal and external resources parents draw upon when facing caregiving challenges (Ma et al., 2023; Widyawati et al., 2023).
Second, psychological inflexibility was specified as the mediator based on Acceptance and Commitment Therapy (ACT) theory, which posits that psychological inflexibility—characterized by experiential avoidance and cognitive fusion—acts as a barrier to adaptive functioning (S. C. Hayes et al., 2012). We theorized that resilient parents would exhibit lower psychological inflexibility because resilience facilitates acceptance of difficult experiences and engagement in value-driven behaviors (Jo et al., 2024; Meyer et al., 2019). This aligns with research showing that resilience is associated with adaptive coping strategies that are core components of psychological flexibility (Hu et al., 2015).
Third, marriage satisfaction was specified as the outcome variable because it represents a critical indicator of family adaptation and well-being among PCDDs (Gagat-Matuła, 2022; Güçlü & Hürmeydan, 2024). Previous research has established that psychological inflexibility negatively impacts relationship quality through reduced empathy, support, and emotional availability (Daks & Rogge, 2020; Golan-Bayazy & Gur, 2024). Thus, our model proposes that resilience influences marriage satisfaction both directly (through enhanced coping and relational resources) and indirectly through reducing psychological inflexibility (which removes barriers to emotional connection and value-consistent behavior in marital relationships).
Furthermore, demographic variables like age and marriage duration influence both resilience and marital satisfaction (S. C. Hayes et al., 2012; Kapikiran & Acun-Kapikiran, 2016). Despite these influences, psychological flexibility’s mediating role is theorized to persist across demographic differences, as its adaptive function transcends these variations. Studies using structural equation modeling show psychological flexibility predicts relational outcomes even when controlling for confounding variables (Fledderus et al., 2010). Consequently, age and duration of marriage were included as control variables in the current study to ensure a more rigorous test of our hypotheses. Gender was also examined as a grouping variable to test whether these structural relationships are consistent across mothers and fathers. Based on the theoretical framework and empirical evidence reviewed, we propose the following hypotheses:
Method
Participants and Procedure
After receiving approval from the institutional review board [Protocol no: 60724], participants were recruited through special education centers, parent support groups, and online communities for parents of children with developmental disabilities (PCDDs) between January and June 2023. Individuals interested in participating were provided with information about the study’s purpose, procedures, confidentiality, and voluntary nature. Upon giving informed consent, participants completed a demographic questionnaire and three measurement scales, either on paper or online. The scales were presented in a counterbalanced order to control for order effects, and completing all measures took approximately 20–25 minutes. No compensation was offered for participation. The final sample included 420 married individuals with PCDDs living in various regions of Türkiye at the time of the study. The sample consisted of 315 females (75%) and 105 males (25%), with ages ranging from 23 to 50 years (M = 36.33, SD = 5.62), and an average marriage duration of 11.81 years (SD = 5.08, range: 0–35 years). All participants had at least one child with developmental disabilities.
Measures
Connor-Davidson Resilience Scale (CD-RISC)
The CD-RISC (Connor & Davidson, 2003; Turkish adaptation by Karaırmak, 2010) was used to measure resilience. The scale consists of 25 items rated on a 5-point Likert scale ranging from 0 (not true at all) to 4 (true nearly all of the time). Sample items include “I am able to adapt to change” and “I can deal with whatever comes my way.” While the original scale identified five factors, the Turkish adaptation found a three-factor structure: “personal competence and tenacity,” “tolerance of negative affect,” and “spiritual orientation.” However, as recommended by Karaırmak (2010), we used the total score as a unidimensional measure of resilience. Total scores range from 0 to 100, with higher scores indicating greater resilience. The original scale demonstrated good internal consistency (Cronbach’s α = .87) and test–retest reliability (r = .89). The Turkish adaptation showed excellent internal consistency (Cronbach’s α = .92). In the current study, the Bayesian reliability coefficient (McDonald’s ω) was .92, 95% CI [0.90, 0.94].
Acceptance and Action Questionnaire-II (AAQ-II)
The AAQ-II (Bond et al., 2011; Turkish adaptation by Yavuz et al., 2016) was used to measure psychological inflexibility. The scale consists of 7 items rated on a 7-point Likert scale ranging from 1 (never true) to 7 (always true). Sample items include “My painful experiences and memories make it difficult for me to live a life that I would value” and “I worry about not being able to control my worries and feelings.” The scale is unidimensional, with higher scores indicating greater psychological inflexibility. Total scores range from 7 to 49. The original scale demonstrated good internal consistency (Cronbach’s α = .84) and test–retest reliability (r = .81). The Turkish adaptation showed similar psychometric properties (Cronbach’s α = .84, test–retest r = .85). In the current study, the Bayesian reliability coefficient (McDonald’s ω) was .88, 95% CI [0.85, 0.91].
Marriage Life Scale
The Marriage Life Scale (Tezer, 1996) was used to measure marriage satisfaction. The scale consists of 10 items rated on a 5-point Likert scale ranging from 1 (strongly disagree) to 5 (strongly agree). Sample items include “I think my marriage is a very meaningful relationship” and “I feel that I have made the right decision to marry my spouse.” The scale is unidimensional, with higher scores indicating greater marriage satisfaction. Total scores range from 10 to 50. Items 2, 4, and 5 are reverse-scored. The original scale demonstrated good internal consistency (Cronbach’s α = .91 for women and .88 for men) and test–retest reliability (r = .85). In the current study, the Bayesian reliability coefficient (McDonald’s ω) was .87, 95% CI [0.84, 0.90].
Data Analysis
A Bayesian structural equation modeling (BSEM) approach was employed to test the hypothesized mediation model. The hypotheses were tested through the following analytical steps: H1 and H4 were tested by examining the direct path coefficients in the structural model, with H4 specifically including age and marriage duration as control variables. H2 was tested through Bayesian mediation analysis, examining the indirect effect of resilience on marriage satisfaction through psychological inflexibility. H3 was tested through multigroup analysis, including measurement invariance testing (configural, metric, scalar, and strict) and comparison of path coefficients and latent means across gender groups. BSEM was chosen over traditional frequentist SEM because it provides more accurate estimates for small to moderate sample sizes (B. Muthén & Asparouhov, 2012; van de Schoot et al., 2014), offers greater flexibility in model specification (Depaoli & van de Schoot, 2017), provides parameter estimates with uncertainty quantification through posterior distributions (Gelman et al., 2013; Kruschke et al., 2012), is more robust to violations of normality (Yuan & MacKinnon, 2009), and allows for more nuanced interpretation using credible intervals rather than p-values (Kruschke & Liddell, 2018; van de Schoot et al., 2021). Prior to analysis, we tested assumptions for Bayesian SEM. Mardia’s coefficients showed significant deviations from multivariate normality (multivariate skewness = 4.72, multivariate kurtosis = 3223627.67), justifying the use of Bayesian estimation. Unlike frequentist maximum likelihood estimation, Bayesian estimation using MCMC sampling does not rely on the assumption of multivariate normality of observed variables (B. Muthén & Asparouhov, 2012; van de Schoot et al., 2014). Non-informative default priors in Mplus were used to allow the data to drive the posterior estimates. The common method bias assumption was also satisfied, as indicated by Harman’s single factor score, which was determined to be less than 50% (Spector & Brannick, 2009). No missing values were detected, and the sample size (N = 420) was adequate for BSEM analysis.
The analysis was conducted in sequential steps. First, descriptive statistics and correlations were calculated. Second, scale reliability was assessed using McDonald’s omega, more appropriate than Cronbach’s alpha when tau-equivalence is violated (Dunn et al., 2014). Third, a measurement model was tested to confirm factor structure and evaluate measurement invariance across gender. Fourth, a structural model examined direct and indirect effects, focusing on psychological inflexibility’s mediating role between resilience and marriage satisfaction. Non-informative (diffuse) default priors in Mplus were used for all parameters, allowing the data to primarily drive the posterior estimates (Asparouhov & Muthén, 2010). The use of non-informative priors is appropriate when researchers do not have strong prior knowledge about parameter values and want results to be data-driven (Depaoli & van de Schoot, 2017; van de Schoot et al., 2014).
Model fit was evaluated using posterior predictive p-value (PPP), Deviance Information Criterion (DIC), Widely Applicable Information Criterion (WAIC), and Leave-One-Out Cross-Validation Information Criterion (LOOIC) (Gelman et al., 2014; Vehtari et al., 2017). PPP values near .5 indicate a good fit, while lower DIC, WAIC, and LOOIC values indicate better-fitting models (Spiegelhalter et al., 2002). Measurement invariance was assessed by comparing models with increasingly stringent equality constraints across gender, with DIC differences less than 10 indicating invariance (Asparouhov & Muthén, 2010). For mediation analysis, direct and indirect effects were estimated with 95% credible intervals. The proportion of the total effect mediated was calculated as the ratio of indirect effect to total effect (Preacher & Kelley, 2011). The Bayesian approach provides more accurate estimates of indirect effects, particularly with non-normal sampling distributions (Yuan & MacKinnon, 2009). Gender differences were examined by comparing path coefficients, with differences considered statistically credible if the 95% credible interval for the difference excluded zero.
Age and marriage duration were included as control variables, given their potential influence on psychological inflexibility, resilience, and marriage satisfaction (S. C. Hayes et al., 2012; Kapikiran & Acun-Kapikiran, 2016). These variables were regressed on all latent variables, with effects evaluated using standardized regression coefficients and 95% credible intervals. Multiple software packages were used: IBM SPSS Statistics 27.0 (IBM Corp., 2020) for initial data screening and descriptive analyses; OMEGA macro (A. F. Hayes & Coutts, 2020) for reliability analyses; Mplus 8.6 (L. K. Muthén & Muthén, 1998–2021) for primary BSEM analyses using the BAYES estimator with two MCMC chains (100,000 iterations each, 50,000 discarded as burn-in); and R 4.1.2 (R Core Team, 2021) with various packages for supplementary analyses and visualizations, including lavaan (Rosseel, 2012), blavaan (Merkle & Rosseel, 2018), bayesplot (Gabry & Mahr, 2021), ggplot2 (Wickham, 2016), and semPlot (Epskamp, 2015). Convergence was assessed using potential scale reduction factor (PSRF < 1.1; Gelman & Rubin, 1992) and visual inspection of trace plots. Mplus and R codes generated from AI models Grok 3 and Claude Sonnet 3.7.
Results
Descriptive Statistics and Correlations
Table 1 presents the means, standard deviations, and correlations among the study variables. The latent variable correlations were as expected, with psychological inflexibility negatively correlated with both resilience (r = −.73, 95% CI [−0.78, −0.67]) and marriage satisfaction (r = −.51, 95% CI [−0.58, −0.43]), and resilience positively correlated with marriage satisfaction (r = .50, 95% CI [0.42, 0.58]). Both age and duration of marriage showed significant correlations with the main study variables, justifying their inclusion as control variables in the model.
Means, Standard Deviations, and Correlations Among Study Variables.
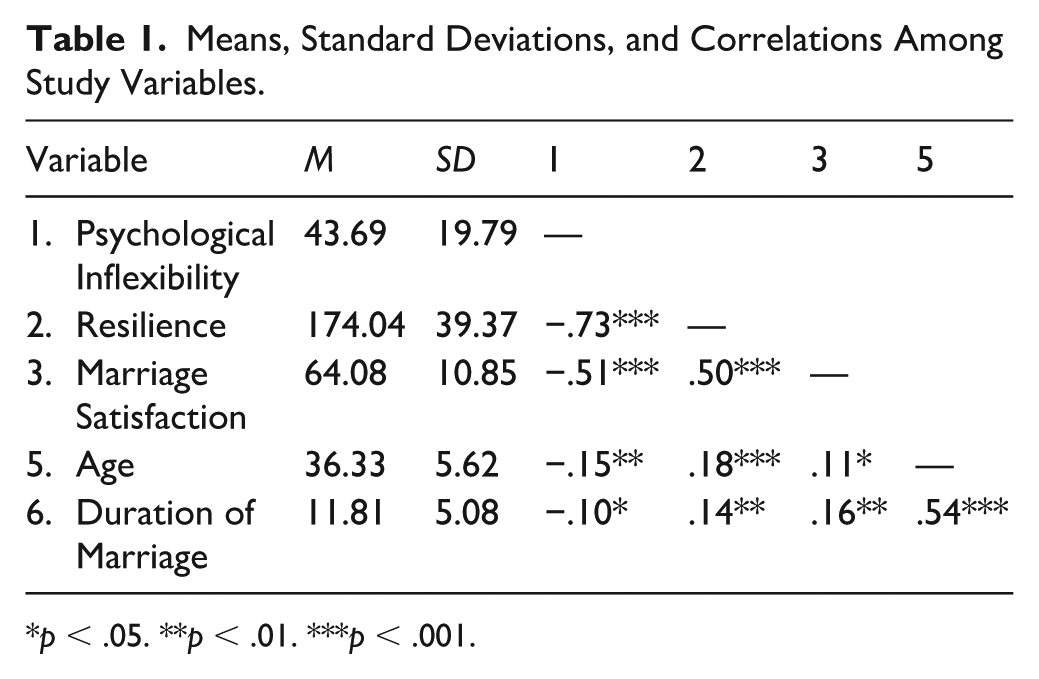
p < .05. **p < .01. ***p < .001.
Measurement Model
The Bayesian measurement model demonstrated excellent fit with a posterior predictive p-value of .52, which is close to the ideal value of .50 (see Table 2). All factor loadings were significant, with standardized values ranging from .62 to .79 (see Table 2).
Bayesian Structural Equation Model Fit Indices.
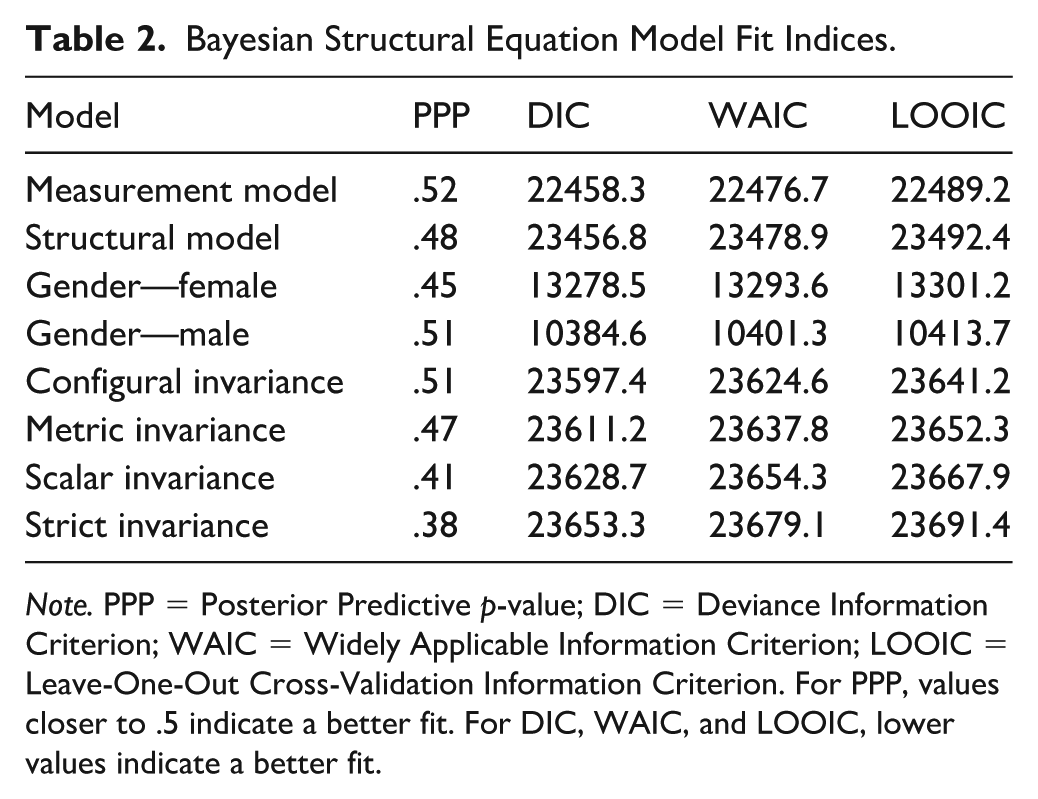
Note. PPP = Posterior Predictive p-value; DIC = Deviance Information Criterion; WAIC = Widely Applicable Information Criterion; LOOIC = Leave-One-Out Cross-Validation Information Criterion. For PPP, values closer to .5 indicate a better fit. For DIC, WAIC, and LOOIC, lower values indicate a better fit.
Tests of measurement invariance across gender groups supported partial invariance up to the scalar level. The configural invariance model (same factor structure) had a posterior predictive p-value of .51. The metric invariance model (equal factor loadings) had a posterior predictive p-value of .47 with a DIC difference of 13.8 from the configural model, which is not substantial. The scalar invariance model (equal intercepts) had a posterior predictive p-value of .41 with a DIC difference of 17.5 from the metric model, which is also not substantial. However, the strict invariance model (equal residual variances) had a posterior predictive p-value of .38 with a DIC difference of 24.6 from the scalar model, which is potentially problematic. Therefore, we concluded that partial measurement invariance up to the scalar level was supported, allowing for valid comparisons between gender groups on latent means and relationships.
Structural Model
The Bayesian structural equation model examining the mediating role of psychological inflexibility in the relationship between resilience and marriage satisfaction showed adequate fit (posterior predictive p-value = .48). Figure 1 presents the standardized path coefficients for the structural model. Resilience was negatively associated with psychological inflexibility (β = −.73, 95% CI [−0.78, −0.68]). Psychological inflexibility was negatively related to marriage satisfaction (β = −.31, 95% CI [−0.40, −0.22]), and resilience had a positive direct effect on marriage satisfaction (β = .32, 95% CI [0.24, 0.40]).

Structural model with standardized path coefficients.
The Bayesian structural equation model examining the mediating role of psychological flexibility in the relationship between resilience and marriage satisfaction showed adequate fit with a posterior predictive p-value of .48 (see Table 2). Table 3 presents the standardized direct, indirect, and total effects with their 95% credible intervals. Also presents the standardized path coefficients by gender.
Standardized Direct, Indirect, and Total Effects with 95% Credible Intervals.
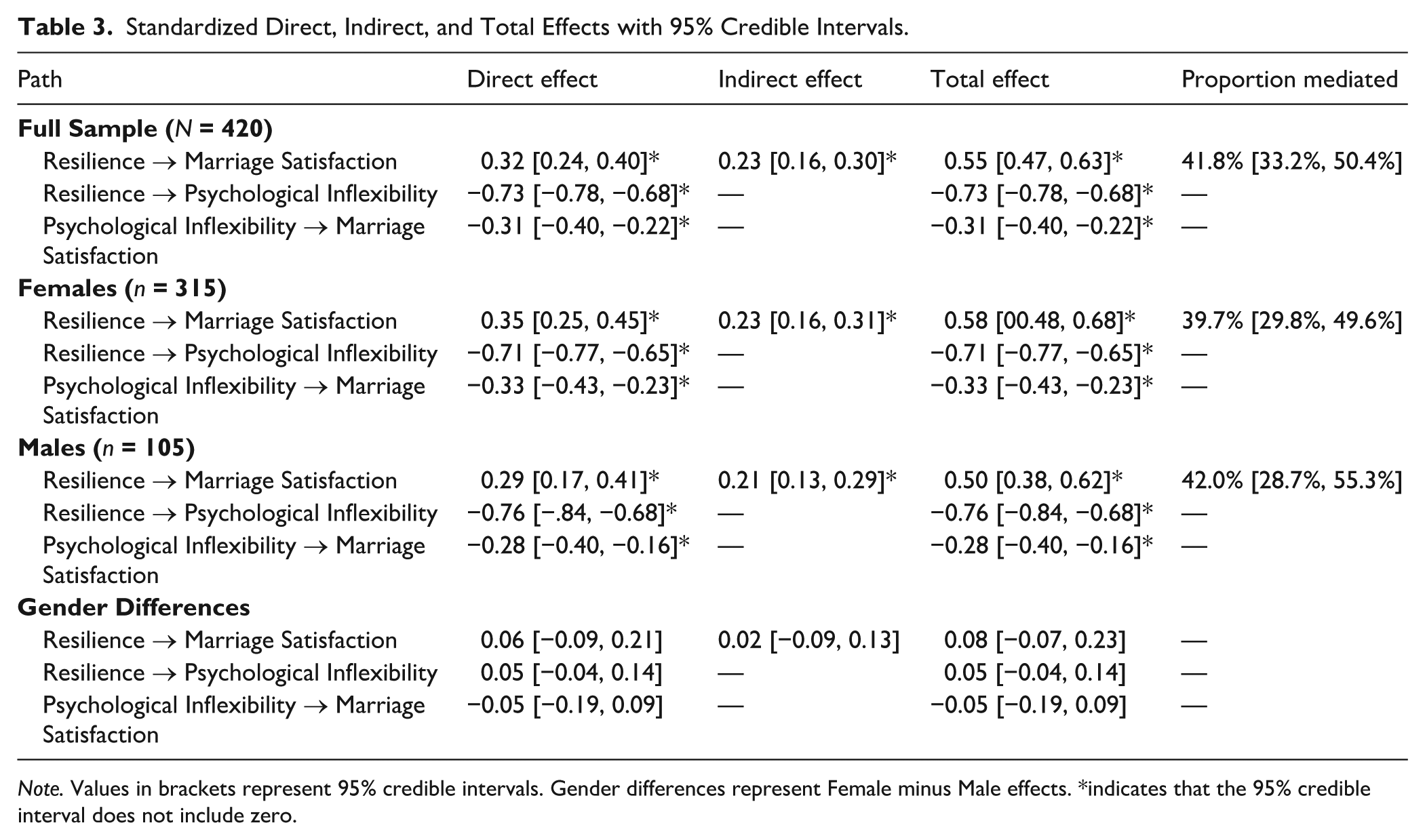
Note. Values in brackets represent 95% credible intervals. Gender differences represent Female minus Male effects. *indicates that the 95% credible interval does not include zero.
Resilience was negatively associated with psychological inflexibility (β = −.73, 95% CI [−0.78, −0.68]), indicating that individuals with higher resilience tend to exhibit less psychological inflexibility (or greater psychological flexibility). Psychological inflexibility was negatively related to marriage satisfaction (β = −.31, 95% CI [−0.40, −0.22]), suggesting that individuals with greater psychological flexibility tend to report higher levels of marriage satisfaction. In addition, resilience had a positive direct effect on marriage satisfaction (β = .32, 95% CI [0.24, 0.40]). The explained variance (R²) was substantial for both endogenous variables: psychological inflexibility (R² = .56, 95% CI [0.51, 0.61]) and marriage satisfaction (R² = .38, 95% CI [0.32, 0.44]).
Bayesian mediation analysis revealed a significant indirect effect of resilience on marriage satisfaction through psychological flexibility (indirect effect = 0.23, 95% CI [0.16, 0.30]). The total effect of resilience on marriage satisfaction was 0.55 (95% CI [0.47, 0.63]), with approximately 42% of this effect being mediated by psychological flexibility. The Bayesian mediation test provided strong evidence for mediation, with P(Indirect effect > 0) = 1.00.
Gender Differences
Analysis of gender differences indicated that the structural relationships were generally similar across gender groups. The indirect effect of resilience on marriage satisfaction via psychological flexibility was .23 (95% CI [0.16, 0.31]) for females and .21 (95% CI [0.13, 0.29]) for males, with the difference not being statistically credible (difference = 0.02, 95% CI [−0.09, 0.13]). Similarly, the total effect was 0.58 (95% CI [0.48, 0.68]) for females and 0.50 (95% CI [0.38, 0.62]) for males, with the difference not reaching statistical credibility (difference = 0.08, 95% CI [−0.07, 0.23]). Analysis of latent means by gender, with females as the reference group, indicated that males had slightly lower psychological inflexibility (standardized difference = −0.18, 95% CI [−0.32, −0.04]), higher resilience (standardized difference = 0.22, 95% CI [0.08, 0.36]), and higher marriage satisfaction (standardized difference = 0.15, 95% CI [0.01, 0.29]).
Control Variables
When controlling for age and duration of marriage, both variables showed some influence on the model variables. Age was positively associated with resilience (β = .14, 95% CI [0.05, 0.23]) and negatively with psychological inflexibility (β = −.12, 95% CI [−0.21, −0.03]), but its relationship with marriage satisfaction was not statistically credible (β = .08, 95% CI [−0.01, 0.17]). Duration of marriage was positively related to marriage satisfaction (β = .13, 95% CI [0.04, 0.22]) and resilience (β = .11, 95% CI [0.02, 0.20]), but its relationship with psychological inflexibility was not statistically credible (β = −.07, 95% CI [−0.16, 0.02]).
Discussion
This study examined the mediating role of psychological inflexibility in the relationship between resilience and marriage satisfaction among PCDDs using Bayesian structural equation modeling. The results supported the hypothesized model, indicating that psychological inflexibility partially mediates the relationship between resilience and marriage satisfaction.
In the Turkish cultural context, these findings are consistent with the “Family Model of Emotional Interdependence” (Kağıtçıbaşı, 2007), where psychological flexibility serves as a vital internal mechanism within close-knit family structures. Specifically, our results align with recent empirical evidence from Turkey indicating that psychological resilience is a significant predictor of marital adjustment among parents of children with disabilities (Eren-Kanbir & Akşit, 2020). Furthermore, researchers have highlighted that for Turkish parents, psychological flexibility acts as a protective bridge that prevents caregiving-related distress from eroding relationship quality (Güleç-Aslan, 2017). By establishing this mediating link, the current findings provide a foundation for the more detailed thematic discussions presented in the following subsections.
Relationship Between Resilience and Psychological Inflexibility
Relationship Between Resilience and Psychological Inflexibility The current study has revealed a strong negative relationship between resilience and psychological inflexibility. This finding aligns with previous research suggesting that resilient individuals are more likely to adapt to challenging situations and accept difficult thoughts and feelings without allowing them to unduly influence their behavior (Kashdan & Rottenberg, 2010). While consistent with existing theory, the use of a Bayesian approach provides robust evidence, confirming this crucial relationship within the specific context of PCDDs. The current study has revealed a strong negative relationship between resilience and psychological inflexibility. This finding aligns with previous research suggesting that resilient individuals are more likely to adapt to challenging situations and accept difficult thoughts and feelings without allowing them to unduly influence their behavior (Kashdan & Rottenberg, 2010). While consistent with existing theory, the use of a Bayesian approach provides robust evidence, confirming this crucial relationship within the specific context of PCDDs. Particularly, it has been observed that PCDDs who exhibit dysfunctional behaviors and behavioral inflexibility lack positive coping skills when faced with challenging life conditions (X. Cheng et al., 2021; Daks & Rogge, 2020; Lobato et al., 2022; Reich et al., 2025; Scherer et al., 2019).
In fact, most PCDDs are forced to leave behind a significant portion of their existing life roles and reshape their roles around the diagnosis from the moment they confront their child’s condition. This process can be laden with depression, anxiety, and stress for many parents (Ülker Tümlü et al., 2017; A. W. Cheng & Lai, 2023; Sairanen et al., 2018; Sharma et al., 2021; Whittingham et al., 2019). On the other hand, there are also parents who, despite experiencing similar psychological distress, continue their lives with positive outcomes (Eren-Kanbir & Akşit, 2020; Manor-Binyamini, 2016). We can interpret this situation as PCDDs with resilience exhibiting less psychological inflexibility in adapting to the new life. Within the framework of the “Family Model of Emotional Interdependence,” resilient Turkish parents often utilize their extended family networks as a buffer against psychological rigidity (Kağıtçıbaşı, 2007). In this context, resilience may foster psychological flexibility by enabling parents to reframe negative experiences, such as caregiving stress, into opportunities for growth (Meral et al., 2021). In addition, the cultural perception of the child’s condition as a “divine test” (imtihan) can facilitate the acceptance of difficult emotions and reduce cognitive fusion (Güleç-Aslan, 2017). Furthermore, a meta-analytic review by Hu et al. (2015) found that resilience is consistently associated with adaptive coping strategies, such as acceptance and problem-focused coping, which are core components of psychological flexibility. This suggests that resilience may not only reduce psychological inflexibility but also enhance the capacity to engage in value-driven actions, a hallmark of psychological flexibility (S. C. Hayes et al., 2012). The current findings may also provide a new perspective on the ongoing debates in the literature regarding whether the concepts of resilience and psychological flexibility/inflexibility are processed similarly or differently.
Psychological Inflexibility and Marriage Satisfaction
The negative relationship between psychological inflexibility and marriage satisfaction suggests that individuals who are less psychologically inflexible tend to report higher levels of marriage satisfaction. This finding is consistent with previous research indicating that psychological flexibility is associated with better relationship outcomes (Daks & Rogge, 2020). In addition, there are studies in the literature demonstrating that psychological inflexibility predicts parental burnout, depression, anxiety, and stress (Lobato et al., 2022; Reich et al., 2025; Whittingham et al., 2019).
PCDDs who can accept their challenging circumstances and remain committed to valued actions may be better able to maintain satisfying marital relationships despite the additional stressors they experience. Building on this, low psychological inflexibility may enhance marital satisfaction by fostering emotional regulation and reducing conflict escalation, as flexible individuals are more likely to respond to relational stress with mindfulness and acceptance rather than avoidance or reactivity (X. Cheng et al., 2021; Golan-Bayazy & Gur, 2024). In the context of parents of children with special needs, this ability to manage relational stress is particularly critical, given the heightened demands of caregiving (Güçlü & Hürmeydan, 2024). The relationship between psychological inflexibility and marital satisfaction in Turkish society is inextricably linked to the collectivist nature of the culture. Turkish families often operate within dense social networks where the ‘perceived gaze’ of the extended family and the community plays a significant role (Kağıtçıbaşı, 2007). For PCDDs, the social stigma or ‘elalem ne der’ (what would others say) concern can increase psychological inflexibility by forcing parents to hide their struggles or maintain a facade of a ‘perfectly functioning family.’ This need for social approval often functions as a source of psychological distress in the Turkish context (Karaşar & Öğülmüş, 2016). Parents who can bypass this social pressure through psychological flexibility—accepting their reality rather than avoiding social judgment—are likely to experience higher marital quality by focusing on their core values rather than external societal expectations. Moreover, low psychological inflexibility may promote marital satisfaction by enhancing communication and emotional intimacy, as individuals who are psychologically flexible are more likely to express vulnerability and empathy, thereby fostering deeper relational bonds (Cordova et al., 2014). This is especially relevant for PCDDs, who often face unique emotional challenges that necessitate mutual understanding and support within the marital relationship.
Mediation Effect
The significant indirect effect of resilience on marriage satisfaction through psychological inflexibility suggests that psychological inflexibility serves as a mechanism through which resilience influences marriage satisfaction. Specifically, resilience appears to reduce psychological inflexibility, which in turn promotes marriage satisfaction. This mediation effect accounted for approximately 42% of the total effect of resilience on marriage satisfaction, indicating a partial mediation. The direct effect of resilience on marriage satisfaction remained significant, suggesting that resilience also influences marriage satisfaction through other mechanisms not included in the current model. For example, resilient individuals may be more adept at seeking and utilizing social support from their spouse, which can directly enhance marital satisfaction (Gagat-Matuła, 2022). This suggests that interventions targeting reducing psychological inflexibility may not only enhance individual well-being but also strengthen family relationships. In addition, the mediating role of psychological inflexibility might be influenced by cultural coping mechanisms prevalent in Turkey, such as ‘sabır’ (patience/endurance) and ‘tevekkül’ (resignation to fate). While resilience in the Turkish context is often bolstered by these spiritual or fatalistic beliefs, the findings suggest that if this ‘patience’ turns into rigid avoidance or emotional suppression (psychological inflexibility), it ceases to protect marital satisfaction. Therefore, for Turkish PCDDs, resilience contributes to marital health only when it promotes an active, flexible acceptance of the situation rather than a passive or rigid endurance.
Gender Differences
The analysis of gender differences revealed that the structural relationships were generally similar across gender groups, with no statistically credible differences in the indirect or total effects. However, analysis of latent means indicated that males had slightly lower psychological inflexibility, higher resilience, and higher marriage satisfaction compared to females. These findings suggest that while the processes linking resilience, psychological inflexibility, and marriage satisfaction may be similar across genders, there may be differences in the levels of these variables. Specifically, female PCDDs may experience greater challenges in maintaining resilience and psychological inflexibility, potentially due to societal expectations and caregiving responsibilities. This finding is consistent with broader gender role research, which suggests that women often bear a disproportionate burden of caregiving responsibilities, leading to higher levels of stress and emotional exhaustion (Sharma et al., 2021). In the specific context of Turkish culture, these gender differences can be further understood through the lens of traditional gender roles and the ‘intensive mothering’ phenomenon. In Turkey, mothers are often culturally constructed as the primary caregivers and the ‘glue’ that holds the family together, especially in the face of disability (Gökçek & Boyacığlu, 2024; Kaş-Alay & Kaçan, 2024; Öztürk & Alemdar, 2023). This cultural expectation may impose a disproportionate emotional labor on mothers, leading to higher levels of psychological inflexibility as they struggle to suppress their own needs to meet the demands of their child and spouse. Furthermore, the Turkish cultural concept of ‘fedakârlık’ (self-sacrifice), while traditionally idealized in motherhood, may inadvertently act as a precursor to experiential avoidance, where mothers feel culturally inhibited from expressing their own distress to maintain family harmony. This caregiving burden may reduce women’s capacity to maintain psychological flexibility, as they may become more entrenched in experiential avoidance as a coping mechanism (Levin et al., 2014). The literature on PCDDs also indicates that mothers may experience greater psychological distress and burnout compared to fathers (Sharma et al., 2021), evaluate their marriages more negatively (Chan & Leung, 2020), and take on more responsibilities (Tümlü & Akdoğan, 2019). All these findings are consistent with the findings of the current study.
However, the lack of significant gender differences in the structural relationships suggests that the mechanisms through which resilience and psychological inflexibility influence marriage satisfaction are relatively universal across genders. This universality highlights the potential applicability of psychological inflexibility interventions for both male and female parents. Nonetheless, future research should explore whether gender-specific stressors, such as societal expectations around masculinity and emotional expression for men, might influence the pathways differently in larger or more diverse samples.
Practical Implications
The findings of this study offer several critical implications for rehabilitation counseling practice, emphasizing that psychological inflexibility serves as a significant barrier to the positive effects of resilience on marital satisfaction among parents of children with developmental disabilities (PCDDs).
At the clinical level, these results underscore the necessity of systematically assessing psychological inflexibility during the intake process. While formal couple-based therapy may often fall outside the professional scope of rehabilitation counseling, practitioners can significantly enhance relational stability through an integrative individual approach. Rehabilitation counselors should consider blending established Cognitive-Behavioral Therapy (CBT) frameworks—which focus on identifying and restructuring maladaptive thought patterns—with Acceptance and Commitment Therapy (ACT) modules, such as mindfulness and values-based action. By utilizing CBT to address specific caregiving stressors and ACT to reduce experiential avoidance, counselors can help parents ‘unlock’ their inherent resilience. This hybrid individual intervention allows the parent to maintain personal well-being and indirectly improves dyadic adjustment, ensuring that the primary support system remains stable and functional without necessitating formal family therapy.
Furthermore, the study highlights the need for gender-sensitive and family-focused programming. Given the observed differences in latent means, practitioners should prioritize targeted support for female caregivers, who may face disproportionately higher caregiving burdens and emotional strain. Resilience-building programs based on positive psychology (Seligman et al., 2006) should be integrated into broader family support services. These programs, such as specialized stress management training or peer support groups, can be tailored to the unique systemic needs of PCDDs, ensuring that marital health is addressed as a core component of family resilience rather than an isolated outcome.
Finally, from a professional development and systemic perspective, these findings suggest that the training curricula for rehabilitation counseling professionals should be expanded. Comprehensive training modules should incorporate ACT techniques and resilience-building strategies as standard components of disability support services. By adopting this holistic approach, rehabilitation settings can ensure that marital satisfaction is integrated alongside vocational, social, and community participation goals. Ultimately, fostering an environment that addresses the intersection of individual psychological flexibility and relational health will enhance the overall quality of life and long-term adaptation for families navigating the challenges of developmental disabilities.
Limitations and Future Directions
This study has several limitations. The cross-sectional design prevents causal inferences, emphasizing the need for longitudinal research to examine the temporal order of variables and capture dynamic changes as parents adapt to their children’s evolving needs. Reliance on self-report measures may introduce common method bias and social desirability bias; future research should include observational measures of marital interactions and objective indicators of psychological adjustment. The study did not investigate specific aspects of the special needs context, such as the type and severity of the child’s disability or the availability of social support, which may influence outcomes. The sample consisted entirely of parents living in Türkiye, which could limit the applicability of the findings to other cultural and geographic settings. The gender distribution was uneven, with more mothers participating than fathers, potentially affecting the results. Although the study controlled for age and marriage duration, other contextual factors like socioeconomic status, cultural background, and access to healthcare services may also impact the relationships among variables. Moreover, Bayesian SEM requires careful consideration of prior specifications; future studies should examine how different prior distributions affect model outcomes.
Conclusion
The Bayesian SEM results support the hypothesized mediation model, indicating that psychological inflexibility partially mediates the relationship between resilience and marriage satisfaction in PCDDs. These relationships were generally consistent across gender groups, though males showed slightly higher resilience and marriage satisfaction levels compared to females. The findings highlight the importance of psychological inflexibility as a mechanism through which resilience influences marriage satisfaction in this population and suggest potential targets for interventions aimed at supporting the marital relationships of PCDDs within rehabilitation counseling practice and training.
Footnotes
Ethical Considerations
This study was approved by the ethics committee of Anadolu University (Protocol No. 60724)
Patient Consent
All study participants provided informed written consent prior to study enrollment.
Funding
This research has been financially supported as part of the Publication Incentive Project at Anadolu University [ID 2105E128].
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data are available on request from the author.
Permission to Reproduce Material From Other Sources
The authors give permission to reproduce material from other sources.
Declaration of Generative AI
The authors used ChatGPT and Qwen 2.5 for the English translation and editing of the manuscript.