
Abstract
Objectives
On the 125th anniversary of the first recognised publication on polymyalgia rheumatica, a review of the literature was undertaken to assess what progress has been made from the point of view of the epidemiology of this disease and whether such studies have advanced our knowledge of its aetiopathogenesis and management.
Methods
The authors searched Medline and PubMed using the search terms ‘polymyalgia rheumatica’, ‘giant cell arteritis’ and ‘temporal arteritis’. As much as possible, efforts were made to focus on studies where polymyalgia and giant cell arteritis were treated as separate entities. The selection of articles was influenced by the authors’ bias that polymyalgia rheumatica is a separate clinical condition from giant cell arteritis and that, as yet, the diagnosis is a clinical one.
Results
This review has shown that, following the recognition of polymyalgia as a distinct clinical problem of the elderly, the results of a considerable amount of research efforts investigating the populations susceptible, the geographic distribution of these affected populations and the associated sociological and genetic elements that might contribute to its occurrence, polymyalgia rheumatica remains a difficult problem for the public health services of the developed world.
Conclusions
Polymyalgia rheumatica remains a clinical enigma and its relationship to giant cell arteritis is no clearer now than it has been for the past 125 years. Diagnosing this disease is still almost exclusively dependent on the clinical acumen of a patient’s medical attendant. Until an objective method of identifying it clearly in the clinical setting is available, uncovering the aetiology is still unlikely. Until then, clear guidelines on the future incidence and prevalence of polymyalgia rheumatica and the public health problems of the disease and its management, especially in relation to the use of long term corticosteroids, will be difficult to provide.
Keywords
Epidemiological considerations
Prevalence of, and population susceptibility to, polymyalgia rheumatica
Polymyalgia rheumatic (PMR) is a very common problem amongst the ageing populations of western society. This is especially true of those of Nothern European and especially of Scandinavian origin. It is likely that, within these populations, it is the most common inflammatory disease of the elderly.1–7 This contrasts with a significantly lower incidence and prevalence in some areas of southern Europe such as northern Italy, northwestern Spain and Israel.1,8–10. The increased, and apparently increasing, incidence within all populations is also seen in the migrant descendants of these northern European populations in North America, where similar climatic conditions prevail as in their countries of origin.1,11–13 It should be pointed out that the majority of these studies do not distinguish between PMR and giant cell arteritis (GCA) or include both conditions in reaching their outcomes and conclusions. These variations in geography and populations have been attributed, in part, to an association between the diagnosis of PMR and several specific tissue type antigens, HLA DRB1*0401, HLA DRB1*0403 and HLA DRB1*0404, although not all series agree on the specific variant of the epitope most associated, and the genetic susceptibility to these diseases is not uniform.13–17 In a study done in northwestern Spain, the study of TNF alleles suggests that susceptibility to PMR and GCA is inherited differently. 18 As might be anticipated if this genetic link is real, there have been reports of a familial increase in incidence of PMR and GCA.19,20
A Viking link?
The geographic distribution of PMR in Europe is of itself interesting. The largest pool of patients, as noted above, is in the Scandinavian countries, but its prevalence in other areas of the continent corresponds remarkably well with the Viking invasions that occurred around the end of the first millennium AD.
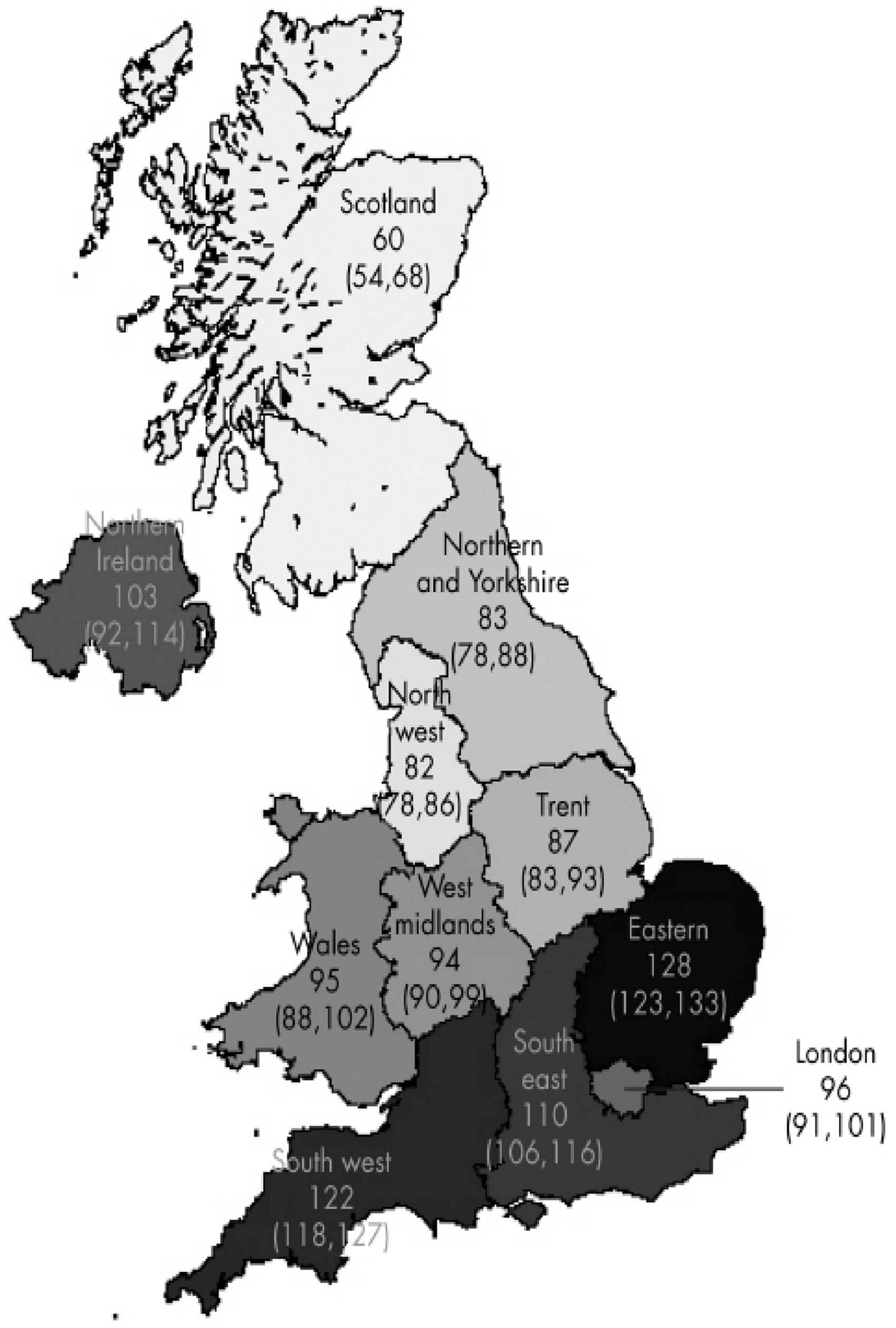
Scotland, where Bruce reported the disease for the first time, the eastern part of England and northern France were the major targets of the Viking Long Ships, and the subsequent settlement of these regions by these Scandinavian warriors, but Northwestern Spain and Northern Italy around the headwaters of the Rhine also suffered from these invaders (Figure 1). Apart from the Scandinavian countries, these are the areas of Europe from which most of the papers on PMR and GCA in the current reference list originate. The maps showing the distribution of the disease in the UK in the paper by Smeeth and his colleagues (Figures 2 and 3) show that PMR and GCA are concentrated in the part of England that was under Viking rule longest and which was known as the Danelaw (Figure 4).
21
Whether this coincidence of geography offers any further insight into the aetiology of PMR is, at present, unknown.
Extent of Viking invasion and settlement in Europe between the 6th and 11th centuries AD. (Reproduced from Google Maps – open access). Age standardised incidence ratios for PMR by region with 95% CIs. Copyright© 2006 BMJ Publishing Group Ltd & European League Against Rheumatism. (Reproduced by permission of Dr L Smeeth and the publishers of the Annals of the Rheumatic Diseases). Age standardised incidence ratios for TA by region with 95% CIs. (Reproduced by permission of Dr L Smeeth and the publishers of the Annals of the Rheumatic Diseases). Area of the UK, known as the Danelaw, that was settled and ruled by Viking invaders from the 9th to the 11th centuries AD. (Reproduced from Google Maps – open access).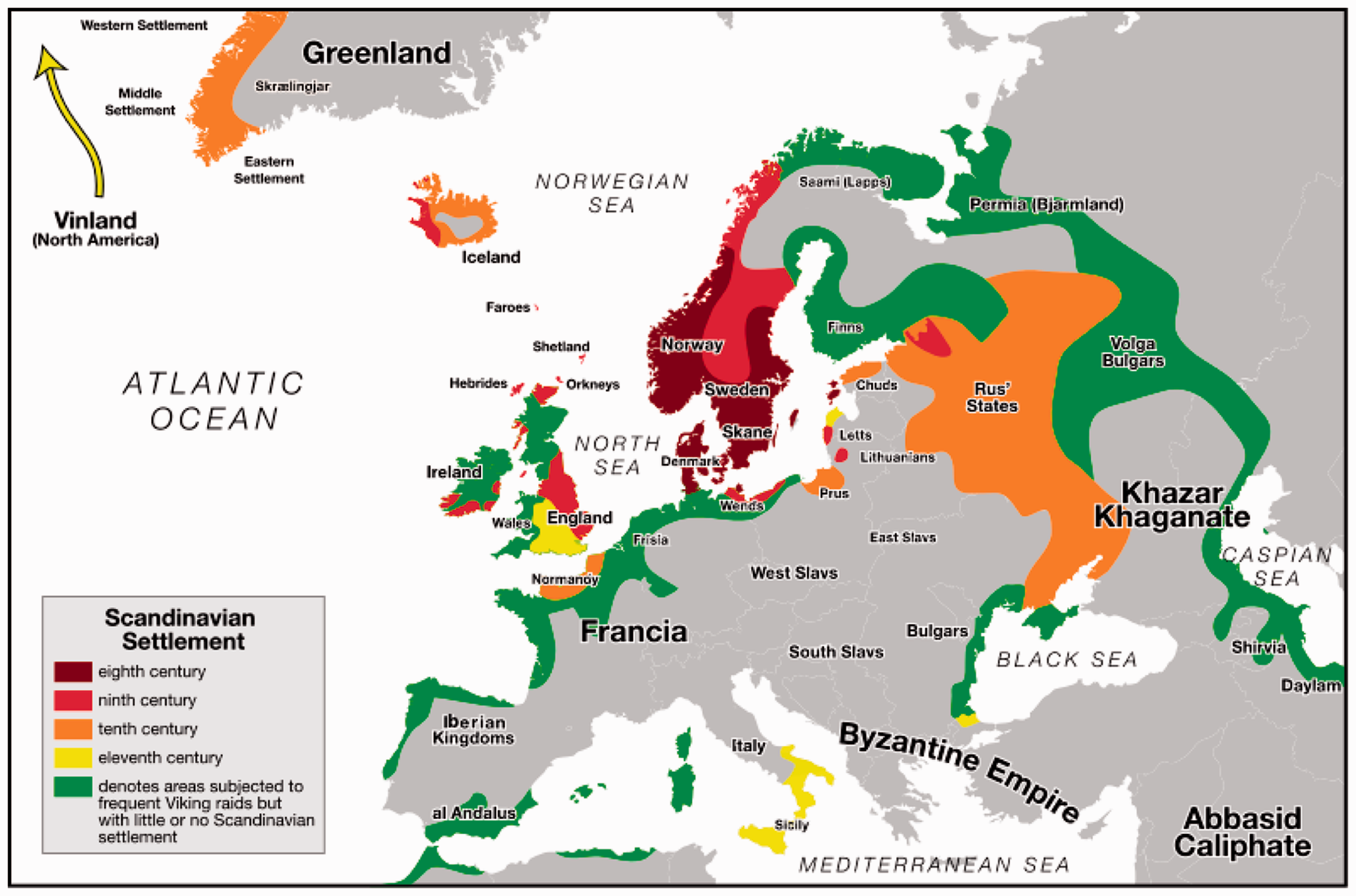


Seasonality
Based on the evidence of the varying seasonal incidence of PMR noted in their study population over a three-year period during which peaks of incidence were noted, a Danish group suggested that infection might be aetiological in PMR, but to date this has not been confirmed. 2 Significant seasonal clustering of both PMR and GCA cases in Britain and Italy, has been reported in addition to those from the Scandinavian countries.22–25 However, the seasons differed, being summer for the British patients and winter for those in Italy, and such clustering has not been universally found.21,26,27 In particular, none has been reported in North America. 28 A number of infectious agents have been considered as potentially aetiological in this, but to date none of these has proven likely in all cases.29–32
Climate vs geography
It would be of interest to know whether the ethnic preponderance of northern Europeans developing PMR persists under very different climatic conditions where seasonal exposure to infectious agents is likely to be markedly different. No reported studies of incidence or prevalence of PMR were found originating from Australasia where this comparison could be made most easily because there has been similar immigration from Europe as that into North America. There are reports that suggest PMR and GCA are common in Australia, but the ethnic origins of these patients has not been provided in sufficient detail to make a meaningful comparison to Europe or North America.12,33,34 The first author has encountered a number of cases of PMR in his practice in the tropical Caribbean islands. These have been almost exclusively in expatriate retirees from North America and the UK who are elderly people of northern European ethnicity and who have spent most of their lives in the colder climates where PMR is most common. Thus, it is not possible to determine from these subjects whether it is race or climate that is the more significant influence on the incidence of PMR. An Australian study is likely to be more meaningful.
Racial influence
There also seems to be a racial predilection for PMR and GCA. Although it has been suggested that the Arab physician Ali Ibn Isa described the diagnosis and treatment of GCA in the 10th century AD, the reported incidence in Arab and Asian populations is much lower than that for Caucasians.35–39 Imai suggested that the apparent lower prevalence in Japan could be due to lack of awareness of the disease among the members of the Japanese medical profession, but even when this potential source of error is taken into consideration, the incidence of PMR seems to be much lower in ethnic Japanese.37,39,40
In all populations in the developed world, however, with the demographic shift towards more advanced age, the overall numbers of patients with PMR have shown a marked increase and this trend is likely to continue in the near future.1,15
Differential diagnosis of PMR
As has been emphasised, PMR is essentially a clinical diagnosis. It is necessary that care is taken to exclude and/or monitor for other disorders. The most frequent disorder that is likely to present as PMR is of course GCA. 41 However, a number of other patients, when followed up over time, are likely to be suffering from rheumatoid arthritis (RA).42–45 There are also patients with underlying malignancies who present with symptoms mimicking PMR. Patients with solid tumours are not likely to show a significant response to glucocorticoids treatment and, as in the large series of patients reported by Gonzalez-Gay, a careful clinical history will often reveal atypical features in the musculoskeletal complaints of patients with such malignant diseases.41,44,45
Giant cell arteritis: clinical comparisons
It is important to note that the same population and ethnic factors discussed above for PMR also apply to GCA, and the inter-relationship of PMR with this disease remains very close.1,11 As discussed earlier, it is not clear whether these two conditions are different manifestations of the same disease, and there are many patients who clearly show features of both. This has meant that the studies of both have suffered. Many contributions to the literature are directed to one or other disorder, but many do not make this distinction and conclusions reached about one condition are extrapolated without sufficient evidence to the other.1–4,11,26,46–50 As much as possible, this review has focussed on PMR but not all the evidence considered is derived from studies specific to PMR. About 15% of PMR sufferers can be shown to have GCA or biopsy evidence of this pathology, whether or not they have symptoms, and about 50% of GCA patients have symptoms of PMR.11,36,51 GCA patients frequently have florid clinical signs of the active arteritis, notably, scalp tenderness, visibly inflamed temporal or facial arteries or tissue infarction of the scalp, the tongue or the central nervous system.1,37,39,47,51–54 Arteriography and Doppler ultrasound examination of the arteries show abnormalities in a high proportion of patients with GCA.55–59 In addition, in GCA, there are clear and well-defined histopathological changes in almost all patients affecting the medial coat of some of the extra-cranial, mid-sized, elastic artery branches of the aortic arch.35,47 In contrast, PMR patients have a dearth of objective clinical or pathological changes attributable to the disease.60–62 This lack of objective signs of specific anatomical involvement in PMR remains the most striking difference between PMR and GCA, and an area of ongoing concern and research.
Course and prognosis of PMR
Because of the marked overlap between PMR and GCA, it is important to investigate all patients with PMR for symptoms and/or signs of GCA as, untreated, this carries a significant risk of blindness in one or both eyes.37,53 Although rarer, it is also a cause of disability and even mortality from cerebrovascular and cardiovascular ischaemic complications.51,54 For this reason, when evidence of GCA is present, or where any doubt that GCA exists in the patient, treatment of the arteritis takes precedence in view of the serious prognosis should vascular occlusion result. Loss of vision is occasionally due to impairment of the vertebro-basilar circulation rather than to direct involvement of the ophthalmic arteries.51,63
At least 80% of PMR patients show no evidence of GCA 64 and, unlike GCA, PMR generally has a benign prognosis in the long term. Bruce emphasised this and was not a little surprised at encountering a rheumatic disease in the elderly where full recovery was the rule. 65 This feature of PMR continues to hold throughout all reported series, although the time to recovery in individual patients does show considerable variation.35,61,66–69 Recovery from a disease where a generalised inflammatory response is a constant feature is suggestive of an infectious aetiology and many authors have sought such an infectious cause for PMR.70,71 Perhaps the newer techniques of viral isolation and culture might be a useful approach to PMR at this time. 72
Clinical care of PMR
It was a family practice physician, William Bruce, who first reported his efforts to alleviate the pain and stiffness of PMR in the Spa at Strathpeffer. Appropriately, the treatment of PMR, in most countries where the prevalence is high, has remained the responsibility of primary care physicians and family doctors.12,73–75 Patients with PMR provide the largest group of patients on long-term corticosteroid treatment in such countries, and the management of this treatment and the prevention of long-term side effects are best addressed in the community this way.46,47 A recent study suggested that general practitioners were much closer than specialist rheumatologists to patients goals and objectives in their assignment of treatment priorities in PMR. 76
Recent advances in our understanding of the biochemical pathways of inflammation have led to a growing number of new therapies for inflammatory diseases such as RA and ankylosing spondylitis. To date, where these have been used in PMR, very little advantage over the traditional treatment has been recognised. Methotrexate does not seem to ameliorate the symptoms significantly and does not shorten the course, although it may reduce the dose of corticosteroid needed to maintain renission.77–79 Biologics therapy has also been tried, but the outcomes have not yet justified any major change in clinical practice.80–84 This may change as the biology and specific actions of these monoclonal antibodies to specific molecules of the inflammatory pathways become clear. Recent case reports suggest that tocilizumab may be helpful in controlling the symptoms of PMR and may reduce the exposure to glucocorticoids, but further trials are needed before this treatment can be said to offer significant advantages over current practice. 85 As the biology and specific actions of these monoclonal antibodies (or the ‘biosimilar’ drugs currently entering the market) become clear, biologics treatment may change clinical management of PMR in the future. 86
Diagnostic/classification criteria for PMR
A number of attempts to provide clinicians with assistance in the diagnosis of PMR by establishing lists of reliable criteria have been made.22,28,87–89 These criteria, perforce, focus on the characteristic clinical features of proximal pain and stiffness and on the acute phase markers that are usually markedly elevated in this disorder.42,48,87,90,91 The dramatic response to corticosteroids has been included as a criterion for the diagnosis, but for the most recent EULAR/ACR criteria, this was excluded as being insufficiently discriminating of the disease, perhaps because there is no clear definition of what exactly this ‘response’ entails.92,93 The more recent evidence from imaging with MRI and ultrasound, that synovitis, bursitis or tendinitis of the proximal musculoskeletal structures is present in a very high percentage of patients with PMR has stimulated some investigators to include imaging techniques in these criteria. 94 All of these criteria which are more properly termed classification criteria rather than diagnostic allow research studies to focus on very homogeneous groups of patients in whom the level of diagnostic certainty is high. However, from the point of view of the clinician treating patients, they leave the problem of excluding from treatment a large number of sufferers where there is a very high probability of PMR. It is not possible or desirable to exclude this group which has been estimated to be about 30% or more of all PMR patients.45,61
Conclusion
Polymyalgia rheumatica remains an enigma, 125 years after its first recognisable description in a medical publication. Over the last half century, the amount of research effort in elucidating the aetiology of this disorder and of its relationship to giant cell arteritis has been prodigious. It is now known that it is more common in women than in men; there is a dramatic response to corticosteroids; there is clear evidence of synovitis, bursitis and tendinitis in the proximal limb girdles; and there is a genetic and racial element to susceptibility to PMR. Apart from these few additional facts, almost nothing has been added to the astute clinical observations about the disease by Bruce in 1888. The treatment has changed little in more than half a century and the newer methods of altering inflammatory responses and pathways have not yet proven to influence the outcome of PMR. Whether patients with PMR would consider exposure to the cold water of the Strathpeffer spring preferable to the exposure to oral prednisone for a prolonged period of time has not been established.
Footnotes
Funding
Dr P Rooney was supported by a sabbatical stipend awarded by St George’s University School of Medicine.
Declaration of conflicting interests
None declared.