
Abstract
Although the significance of travel health risks is well documented, the process through which people assess their vulnerability and ultimately take on preventive measures needs clarification. The purpose of this article is to better understand factors underlying travelers’ health risk perceptions and their protective behavior. Using the health psychology literature, a conceptual model that incorporates multilevel psychological constructs was tested with 830 Australian outbound travelers. Worry was an important antecedent to both travel health risk perceptions and risk-protective behavior. Perceived control over health-related risks was not positively associated with risk perceptions but was positively associated with risk-protective behavior. Sensation-seeking propensity was negatively associated with risk perceptions but positively associated with risk-protective behavior. Travel risk perceptions mediated the relationship between the antecedents and risk-protective behavior. Implications for the design of health communication for industry and government are outlined, and future research avenues are also proposed.
Introduction
Traveling and travel decision making involve a certain level of risk that needs to be recognized by both tourists and tour operators (Quintal, Lee, and Soutar 2010). Risk has been conceptualized as having two key elements: uncertainty and consequences (Conchar et al. 2004). The perspective on uncertainty has been the central focus of many tourism studies in recent years, which investigated a multitude of issues about risks involving various destinations (e.g., Fuchs and Reichel 2006; Lepp, Gibson, and Lane 2011), different forms of tourism (e.g., Boksberger, Bieger, and Laesser 2007; Cater 2006), and distinct market segments (e.g., Jonas et al. 2011; Lepp and Gibson 2003). Research in relation to consequences, on the other hand, has mainly centered on tourist information search and travel decision making as a result of risk assessment (e.g., Reisinger and Mavondo 2005; Sharifpour et al. 2014). The tourism literature has identified risk as a multidimensional phenomenon comprising a number of risk factors (Cheron and Ritchie 1982; Tsaur, Tzeng, and Wang 1997) that can be measured in terms of equipment, financial, political, physical, satisfaction, social as well as psychological dimensions (Kozak, Crotts, and Law 2007; Roehl and Fesenmaier 1992). Perhaps for apparent reasons, the bulk of the present research has focused on political and terror risks and less on health concerns (e.g., Floyd and Pennington-Gray 2004; Fuchs, Uriely, and Reichel 2013; Sonmez and Graefe 1998). Granted, the terrorism-related risk events generate deleterious impact on traveler’s psychological stress and behavior, but most, if not all, of these risk events are likely to be out of the individual’s control. Health and safety risks such as drug-taking, on the other hand, can be voluntary and prevented (Uriely and Belhassen 2006).
Although the existing literature has established the foundation for risk-related studies in tourism and enjoys widespread influence, it has become increasingly clear that the characteristics of individual travelers can have a significant impact on their risk assessment. One area where there is a clear need for greater understanding relates to traveler’s risk perception with respect to personal health and well-being, and its downstream consequences on health-preventative and protective behavior such as buying travel insurance or being vaccinated before traveling abroad. Studies across various contexts have typically found moderate to strong positive relationships between perceived risk and health-protective behavior (Schmiege, Bryan, and Klein 2009), but simultaneous investigation of these constructs in tourism is relatively limited. Intuitively, heightened health risk perception should encourage people to minimize or shift risks (Brewer et al. 2004; Uriely and Belhassen 2006), but anecdotal and research evidence suggests that this may not always be the case (e.g., Fuchs, Uriely, and Reichel 2013; Hajibaba et al. 2015; Uriely, Maoz, and Reichel 2007). The aim of this article is to better understand the factors which influence travel health risk perception, and to examine the relationship between risk perception and protective behavior in tourism.
We elect to focus on perceived risks that encompass health and personal safety hazards, such as traffic accidents and food poisoning, for several reasons. First, these risks are commonplace irrespective of destinations. If encountered, they are likely to have psychological, financial, and even social implications to the traveler as well as the healthcare system at the destination, and perhaps even the origin country. Second, tourists tend to be at higher levels of exposure to a range of health and safety hazards during a vacation than local residents because of a lack of destination familiarity or exercise of caution (McInnes, Williamson, and Morrison 2002; Page 2009). For example, research conducted in Australia indicated that about 50% of travelers reported some kind of illness when traveling overseas (Behrens 1997). Despite the potential costs associated with travel-related illness or injury, research consistently shows that many travelers journey abroad without precautionary measures (Hamer and Connor 2004; Jonas et al. 2011), possibly because of their low perceived risk susceptibility. Finally, though not entirely under one’s control, many of these risks can be prevented or their impact minimized through health-protective behaviors, such as immunization or insurance cover. Because of health risks’ potential influence on individuals’ well-being and host community safety (Wilks 2006), examining mechanisms that underlie risk perceptions can help provide useful insights to the design and development of travel health and safety communications, thereby reducing the possibility or impact of travel-related illness and injuries.
Literature Review
Perceived risk represents a central construct in many theories of health behavior and is often referred to as perceived probability, perceived likelihood, susceptibility, or vulnerability (Brewer et al. 2004). In line with Menon, Raghubir, and Agrawal (2008), we define travel risk perception as the negatively valenced likelihood assessment that an unfavorable event related to travel health and safety will occur over a specified time period. Past literature suggests that travel health risk perceptions are likely to vary according to individuals and their particular situations. Roehl and Fesenmaier (1992) were the first to investigate perceived risks associated with pleasure travel, and found the relationships between risk perceptions and travel behavior to be situation specific. Others have paid particular attention to travelers’ travel-specific and lifestyle variables (Fuchs and Reichel 2006; Maser and Weiermair 1998), and the influence of past experience (Larsen, Øgaard, and Brun 2011; Lerner et al. 2003; Sjöberg 1998). More recently, Fuchs, Uriely, and Reichel (2013) demonstrated that tourists’ risk perceptions correlated with their political orientation. A number of personal factors have also been found to influence the level or nature of individuals’ risk perceptions, including tourist’s sociodemographic makeup (Floyd and Pennington-Gray 2004; Tsaur, Tzeng, and Wang 1997), culture (Reisinger and Mavondo 2005, 2006), and psychographic factors such as novelty seeking and sensation seeking (Lepp and Gibson 2008; Pizam et al. 2004; Sharifpour, Walters, and Ritchie 2013). Research in the area of travel medicine, on the other hand, has predominantly considered the relationship between travel patterns, travel destinations, and the type of health advice sought including travel vaccine uptake (e.g., Hamer and Connor 2004; Wilder-Smith et al. 2004; Zwar and Streeton 2007).
The aforementioned literature mainly investigated perceived risk in relation to specific destinations (e.g., the Middle East). Such investigation provides insight into travelers’ behavior within a specific context and could assist with destination marketing. However, this makes it impossible to derive insights into travelers’ general propensity to risks that may frame their travel decision making and, more importantly, their readiness to carry out preventative measures before departure. Recently, there have been calls to better understand travelers’ psyche in order to determine their general risk predisposition irrespective of types of crises, so as to allow the development of effective travel health and safety communications (Hajibaba et al. 2015). Given the probability of health risks such as getting infectious diseases or falling ill while traveling is common to all destinations, it is reasonable to examine traveler’s general health risk perceptions irrespective to their travel destinations.
The literature also recognizes the value of integrative models to examine travel risk perception in order to advance theory development and improve current analysis of risk (Williams and Baláž 2015). Efforts to develop a model incorporating cognitive, affective, and motivational factors as predictors of individual risk perception and behavior have been limited in tourism literature. In addition, existing research has predominantly approached the issue from the perspective of potential travelers considering travel during a specified period, and only a handful of studies have included actual travelers who were on their way to the final destination (e.g., Fuchs, Uriely, and Reichel 2013). Findings from prior studies often have been based on case studies (e.g., Sharpley, Sharpley, and Adams 1996) or focus group research (e.g., Peattie, Clarke, and Peattie 2005), which can overlook the correlation among constructs and have limited generalizability.
Following the calls to conduct systematic, theoretically driven research into travel risk perceptions before developing strategies to manage the travel-related risks (Williams and Baláž 2015), we aim to integrate the widely studied concept of perceived risk and constructs from models of health behavior into a broader theoretical framework. Informed by the conceptual framework related to health risk perceptions (Menon, Raghubir, and Agrawal 2008), the current research simultaneously examines the effects of multilevel psychological factors on individuals’ travel risk perceptions and their behavioral outcomes. Specifically, it explores the impact of motivational factors such as sensation-seeking propensity, affective factors such as worry, and cognitive factors such as perceived control in an outbound travel context with actual travelers, rather than potential travelers. To our knowledge, this is one of the first studies to provide an integrative analysis of the psychological mechanisms that underlie travel risk perceptions with actual travelers. Understanding risk perceptions from individual traveler’s perspective is important for policy makers and tourism operators for both risk prevention (i.e., preemptive) and risk management (i.e., responsive).
Conceptual Framework
We propose a conceptual model (Figure 1) that explores the dynamics among individual travelers’ psychological and sociodemographic factors and examines their interplay with travel risk perception and protective behavior. Specifically, our purpose is to integrate the widely studied concepts of worry, perceived control over the risk, and sensation-seeking propensity into a broader theoretical framework
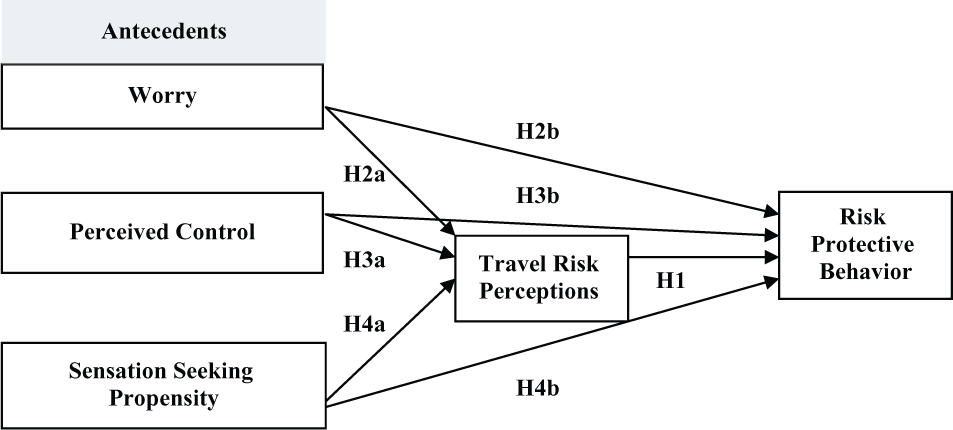
Conceptual model and constructs.
Several empirical studies in health psychology have found positive association between risk perceptions and health protective action, such that higher perceived risk of harm should encourage people to take action to reduce their risk (e.g., being vaccinated, precautionary sexual behavior) (e.g., Brewer et al. 2004; Weinstein et al. 2007). Kreuter and Strecher (1995) noted that by increasing perceived stroke risk among smokers, intention to quit smoking significantly increased. Specifically, increased age was associated with more realistic risk perceptions, and higher education levels also predicted less biased risk perceptions. Similarly, Bull, Kreuter, and Scharff (1999) found that individuals who received tailored communication relating to their health assessment were more likely than those receiving standard materials to increase their physical activities of daily living, presumably because the material raised perceptions of personal risk. In a tourism context, research found that travelers to Zimbabwe who had higher malaria risk perceptions were more likely to have undertaken precautions (Laver, Wetzels and Behrens 2001). An Australasian study also found that higher levels of health risk perception lead to higher levels of pre-travel health advice (Wilder-Smith et al. 2004). From the preceding discussion, the degree to which a traveler believes that he or she is at risk should affect decisions to engage in protective behaviors. Travelers with higher travel risk perceptions are likely to have greater involvement in protective behaviors.
Hypothesis 1: Travel risk perception is positively related to protective behavior.
Worry
Emotion is an affective antecedent that is hypothesized to trigger changes in cognition and action; therefore, a growing literature in psychology has considered the interplay of emotions and risk perceptions (Lerner et al. 2003). Rundmo (2002) suggests that affective dimensions act as the best predictors of risk estimates, and it is likely that the most salient affective element that influences risk perceptions is worry. Worry is described as an affective response to a threat and, naturally, for many who think about a risk source, there are feelings of worry and concern (Schmiege, Bryan, and Klein 2009). While worry is related to anxiety, they have been demonstrated as independent constructs (Davey et al. 1992). Worry may be understood as negative affect and relatively uncontrollable chains of thought related to future uncertainties and imagined catastrophes (e.g., What if I become ill while traveling?) (Larsen, Brun, and Øgaard 2009; Borkovec et al. 1983). Anxiety, on the other hand, is associated with poor problem-solving confidence and considered to result in poor psychological outcomes (Davey et al. 1992).
As worry exacerbates vulnerability, it is linked to unconstructive outcomes such as anxiety and depressive symptoms (Hong 2007). For example, worriers tend to perceive less confidence in their coping abilities and solutions and engender anxiety by worrying about almost everything (Hong 2007). However, worry can serve constructive functions by keeping individuals aware of potential threats and motivating them to discover ways of avoiding possible problems (Watkins 2008). This suggests that worry can implicate mental coping as well as adoption of adaptive behaviors that reduce anticipated negative outcomes. As such, worry is considered as an antecedent of risk perception and protective behavior.
Worry has been found to predict an interest in reducing one’s health risks and is positively related to health-protective behavior such as mammography screening (Diefenbach, Miller, and Daly 1999), influenza vaccination (Chapman and Coups 2006) and quit attempts among cigarette smokers (Dijkstra and Brosschot 2003). McCaul and Mullens (2003) suggested that worry motivates self-protective behavior because it keeps an issue salient. The experience of worry may add a cognition to one’s storehouse of reasons to take protective actions, thus motivating attempts to manage the aversiveness of worrying. Worry matters because it organizes thoughts, focuses actions, and arouses coping strategies concerning stressful situations, and thus helps prioritize risks (Peters et al. 2006).
Worry has also been studied in tourism to predict travel behaviors. Fischhoff et al. (2004) investigated travelers’ vulnerability by asking about their travel concerns that led to feeling at risk, their worries about other travel problems, and their attitudes toward risk. Results revealed that worry played a significant role in people’s willingness to travel to various places and their cancellation decisions, suggesting that worry may affect choices even among people who have generally consistent beliefs or emotions. Larsen et al. (2009) developed a scale for measuring tourist worries. Their Tourist Worry Scale was tested in three different samples and findings suggested that the more risky tourists perceived destinations to be, the more they worried. Bergstrom and McCaul (2004) investigated the impact of worry as a determinant of decision making, examining the willingness of college students to fly to New York City or Washington DC, and their beliefs on the likelihood and severity of new terrorist occurrence after 9/11 terrorism. Worry was found to be the strongest indicator of willingness to travel for self as well as others. Together, existing literature shows that worry influences travelers’ information processing of risks and subsequent behaviors.
In a similar vein, Dolnicar (2005) examined the relationship between fear and risk perceptions. Tourists were categorized into groups based on the level of fear they experience with regards to travel. The author identified four fear segments: low-fear, overseas sceptics, thrill seekers, and high-fear group. The thrill seekers gave a lower rating on risk dimensions related to overseas travel, while scoring average on social and general risk items and scoring high on thrill and excitement. The overseas sceptics group believed that terrorism and contagious diseases are more likely to occur and held more doubts about the benefits associated with the novelty and adventure of traveling to exotic places. In contrast, the high-fear group consistently rated risk factors higher than the average, and the low-fear group consistently rated the risk items lower than the average. The findings implied a direct relationship between travelers’ negative affect and risk perceptions. We follow the path of previous research and propose that worry can serve a constructive purpose in a travel context. Travelers who express higher level of worry are likely to display higher travel risk perceptions and protective behavior.
Hypothesis 2a: Worry is positively related to travel risk perception.
Hypothesis 2b: Worry is positively related to risk-protective behavior.
Perceived Control over Risk
Perceived control can be conceptualized as command over the outcome and is commonly defined as a belief about one’s ability to influence outcomes and to prevent negative events (Nordgren, Van Der Plight, and Van Harreveld 2007). In general, people are motivated to maintain control over their environment even though the control is merely a self-generated feeling or perception (Helgeson 1992). Gaining a sense of control over future events gives a feeling of invulnerability and allows one to believe that victimization is manageable (Helgeson 1992). Research evidence from health psychology supports a negative relationship between perceived control and risk perception, such that the greater the perceived control over the outcome of an event, the lower one’s personal risk estimate (Welkenhuysen et al. 1996). Ruthig et al. (2008) examined whether perceived control predicted older adults’ estimates of their risk for a future health problem, namely, a hip fracture. They found that stronger control perceptions were associated with lower risk estimates, even when participants’ age, gender, income, and physical health were statistically accounted for. The effects of perceived control also differed as a function of risk attribution, in that the negative relationship between perceived control and risk estimates was stronger when implied risk was low (vs. high) and when the cause was deemed controllable (vs. uncontrollable) (Ruthig et al. 2008). The authors concluded that perceived control reduced pessimistic risk estimates, which in turn, could lead to decreased anxiety and depression while bolstering engagement in protective health behavior.
In tourism, Jonas et al. (2011) identified three distinctive groups of perceived health risks based on the level of control individuals assumed to have on the occurrence of these events. The first group included risks that were environmentally induced such as water quality, food safety, and disease infection. The second group comprised semi-controlled risks including physical injuries and safety of extreme adventure facilities, which were categorized by travelers as medium-level health risk factors. The third group contained risks related to sexually transmitted diseases and drug use, which were deemed fully controllable by the traveler. These findings unveiled travelers’ perceived vulnerability to certain risks, suggesting perceived control as an important determinant of travel health risk perception. In line with prior research, we propose that the level of control one assumes to have can influence perception and behavior. Specifically, perceived control over outcomes and events might reduce anxiety while increasing perceived invulnerability, which in turn lowers risk perception and risk-protective behavior.
Hypothesis 3a: Perceived control is negatively related to travel risk perception.
Hypothesis 3b: Perceived control is negatively related to risk-protective behavior.
Sensation-Seeking Propensity
An individual traveler’s personality provides the impetus for risk taking. One personality trait that is inherently intertwined with perception of risk is sensation-seeking propensity. It is a personality trait in which individuals are considered to vary in their ability to tolerate sensations of all types (Pizam et al. 2004). People with the desire for novelty and intense sensory stimulation show a willingness to take risks for the sake of such experience (Zuckerman 1979). In the tourism literature, sensation seeking has been found to be positively correlated with participation in high-risk recreational activities, dislike of structured and formal situation, and tendency toward disinhibition (Galloway 2002; Pizam et al. 2004). For example, high sensation seekers are more likely to be adventure travelers (Gilchrist et al. 1995) and seek out travel experiences that provide a greater degree of novelty (Lepp and Gibson 2008) compared with low sensation seekers. High sensation seekers were also found to visit parks more often to camp, be more likely to attend interpretive programs, and enjoy a broad range of more challenging activities during their park visits than low sensation seekers (Galloway 2002). Overall, travelers’ sensation-seeking propensity encapsulates their tendency to try out novel experiences and willingness to tolerate uncertainty.
Accordingly, sensation seeking has been linked to risk taking, and tourists are said to assess risks differently depending on their preference for familiarity or novelty (Reisinger and Mavondo 2005). Zuckerman (1979) showed that low sensation seekers displayed a higher level of anxiety toward risks; in contrast, high sensation seekers reported a positive arousal by the associated risk. Similarly, Pizam, Reichel, and Uriely (2001) revealed that high sensation seekers were more inclined to travel independently and engage in risky vacation activities. Notwithstanding, there have been debates about whether sensation seeking influences travelers’ risk perceptions and risk-taking behaviors (Lepp and Gibson 2008). Pizam et al. (2004), for example, argued that individuals who took risks deliberately and were not informed on the potential losses were not necessarily motivated by sensation seeking. In other words, some sensation seekers do not undertake activities that might be considered as risky.
By and large, the existing literature acknowledges that risk taking and sensation seeking are related but different constructs (Pizam et al. 2004). Studying Israeli student backpackers, Fuchs (2013) found that travelers share common perceptions of some risk events regardless of their sensation-seeking propensity. While high sensation seekers might be less concerned about socially oriented threats such as crowded and commercialized places, they were equally concerned about risks and incidents involved in backpacking activities. Fuchs’s (2013) study highlighted the complexity of the relationship between sensation seeking and travel risk perception, implying that high sensation seekers might simply have higher tolerance for certain risks. Furthermore, through applying the four independent scales of sensation seeking, Fuchs (2013) found differences based on the type of experience sought and the types of risk they were likely to confront during their trip. The findings have implications for both understanding the influence of sensation seeking and a comprehensive measurement of the trait through measuring the subdimensions. Recently, in a study to understand and profile crisis-resistant travelers, Hajibaba et al. (2015) concluded that crisis-resistant tourists do not necessarily perceive risks differently; rather, they might have a higher threshold or tolerance for risks and thus may not postpone or cancel their trips. Building on the existing literature, we propose that travelers with high sensation-seeking propensity might show a lower level of perceived risk and risk-protective behavior because of their willingness to participate in adventurous activities and their higher risk tolerance threshold.
Hypothesis 4a: Sensation-seeking propensity is negatively related to travel risk perception.
Hypothesis 4b: Sensation-seeking propensity is negatively related to risk-protective behavior.
Consistent with our conceptual framework and the central positioning of travel risk perceptions in the framework, we propose that the influence of the antecedents on risk-protective behavior can be mediated through risk perceptions.
Hypothesis 5: Travel risk perception mediates the relationship between the antecedents (worry, perceived control, and sensation-seeking propensity) and risk-protective behavior.
Contextual Differences
Past research on travel risk perceptions acknowledges that risk is context specific and dependent on the travel location (Roehl and Fesenmaier 1992); thus the choice of holiday destination can affect travelers’ perceived risk. For instance, from a list of 50 countries respondents believed that Canada, New Zealand, Switzerland, Sweden, and Australia were the five safest countries (Sönmez and Graefe 1998). In contrast, Iraq, Somalia, Libya, Lebanon, and Syria were identified as the five riskiest countries to visit (Sönmez and Graefe 1998). Asia and North America were perceived to be riskier driven by the frequency and severity of natural disasters, while South America, Africa, the Middle East, and Asia were perceived to be risky for the outbreak of infection disease (Kozak et al. 2007).
The further the traveler’s home country is from their destination, the less knowledge about the new environment is likely to be available (Sousa and Bradley 2006), and thus the more likely he or she is to feel that the destination’s culture, history, and heritage are distinctively different (McKercher and du Cros 2003). This can create a feeling of cultural distance between the origin and destination country, potentially increasing risk perceptions. Researchers have argued that cultural distance could impact on individual’s perception or “psychic distance” (Sousa and Bradley 2006). Clearly, greater cultural distance renders learning more difficult and could hinder interaction among people, which might lead to misinterpretation and misunderstanding (Manev and Stevenson 2001) and increasing risk perceptions. Crotts (2004) suggested that greater cultural distance between international visitors and the culture of host country should increase the likelihood of visitor’s engagement in risk reducing behaviors. Strategies used to reduce perceived risk might include spending more time in planning their trips, use of travel packages, use of travel agents and tour operators, traveling in a larger group, and booking shorter trips. Therefore, it is important to consider the destination context when designing travel risk studies, and this is particularly important when studying outbound travelers who are traveling to many different countries.
Research Design and Methods
Design and Measurement
To test our hypotheses, we conducted a survey on a sample of outbound travelers who were Australian citizens or permanent residents. We distributed surveys to travelers who were waiting to board international flights at the departure lounges of a major international airport. Participants first responded to background questions about their sociodemographic characteristics, main travel destinations, trip purpose, and length of stay. These questions allowed for benchmarking against Australian Bureau of Statistics (ABS) data to ensure the sample was representative of outbound travelers. The remainder of the survey questions related to the key constructs in the model.
Risk perceptions were measured by assessing the likelihood of potential travel health and safety risks occurring when traveling overseas on a seven-point Likert-type scale (1 = extremely unlikely to 7 = extremely likely). Based on previous research (Page 2009), seven risk events were identified, including high likelihood/relatively minor health and safety risks such as general travel well-being; moderate likelihood and impact risks such as crime and transport accidents; and finally major impact risks with low likelihood such as natural disasters and epidemic diseases. Risk-protective behaviors were identified from a number of travel sources including the Australian Department of Foreign Affairs and Trade smartraveler website 1 and information provided by The Travel Doctor, 2 a travel medicine provider. A total of four risk reduction measures were presented and respondents indicated the frequency that they have carried out these activities in the past, including the current trip. Items were measured on a five-point Likert-type scale (1 = almost never to 5 = almost always) adapted from Hoorens and Buunk (1993). Items included seeking travel advice, registration of their contact details with the Australian government, seeking health advice, and taking out travel insurance.
Worry associated with the seven potential risks outlined above was measured on a single-item, seven-point Likert scale (1 = not at all worried to 7 = extremely worried) adapted from Larsen et al.’s (2009) tourist worry scale. In line with Rotter (1966), perceived control over risk was measured using a single-item, seven-point Likert-type scale (1 = not at all controllable to 7 = completely controllable), asking respondents how much control they felt they had over the seven potential travel-related risks. Sensation-seeking propensity was measured using the eight-item Brief Sensation Seeking Scale (BSSS) (Hoyle et al. 2002), which has been adapted from Zuckerman’s (1979) sensation-seeking scale and previously validated in tourism (Eachus 2004; Litvin 2008). Finally, we measured destination context to check if this has an impact on the proposed relationships. Travelers indicated the destination where they were planning to spend the majority of their trip. Individual destinations were combined into regions following the United Nations World Tourism Organization regions to assess whether the statistical models would be different based on travel destination.
Sampling and Procedure
The departure lounges of a major international airport were used to collect the data for several reasons. First, travelers at the departure lounges would have just carried out travel risk assessment and preventive measures, if any. Thus, these travelers should be able to provide reflective responses with little bias. Second, as travelers were asked to recall behaviors that occurred only recently and thus should still be salient in memory, the method addresses the limitations related to memory recall of a distal past behavior. Third, the research site prevents the limitations usually associated with measuring just behavioral intentions of prospective travelers as it measures actual travelers at their point of depart.
We adopted a self-administered survey method. The questionnaire was initially piloted in a representative sample of 52 people to ensure clarity, reliability, and validity. The data collection was planned based on flight departures to the main outbound destinations by checking flight schedules and matching these with the timing of fieldwork. We surveyed 864 Australian citizens and permanent residents in the departure lounges during December 2011 and January 2012. On the basis of the Australian Bureau of Statistics outbound travel data for the December/January period, we estimated a target population of approximately 1 million travelers during this peak travel period (ABS 2012). Owing to missing data, a total of 830 useable surveys were collected during this period. Thus, based on the target population, this sample would provide us with results confident to a ±4% margin of error at the 95% confidence level.
Results
Sample Profile
With respect to sociodemographics the average age of respondents was 39.6 years; 54.3% were male and respondents were either married or had de facto partners (54.3%). Approximately 41% of respondents had completed a university degree as their highest qualification. A total of 69.8% did not have any children living at home.
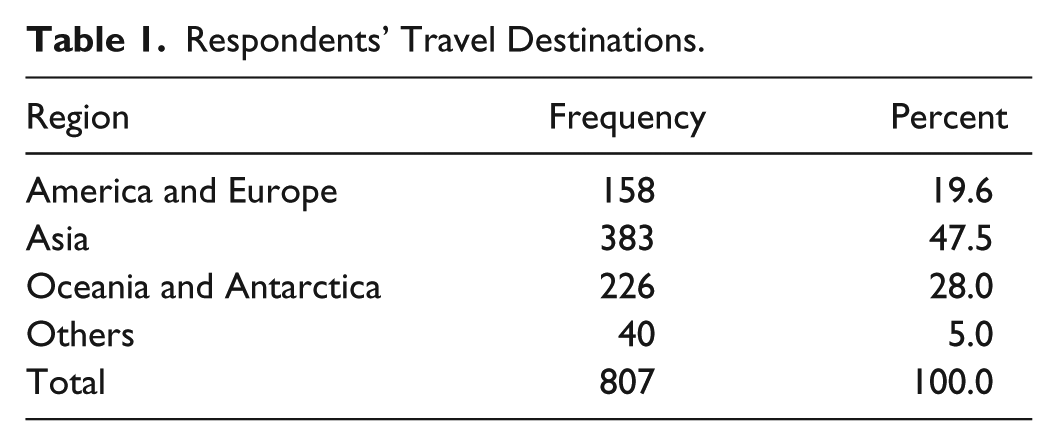
The top 10 outbound destinations accounted for 69.0% of the sample compared to 67.9% of the Australian Bureau of Statistics (ABS) data for the period. New Zealand and Indonesia were the top two outbound destinations for the sample and Australian travelers generally during the survey period. Respondents were planning on staying overseas for a median duration of 14 days, compared with 15 days based on the ABS data for the study period. Approximately 81% were traveling independently for the purposes of holiday (56%), visiting friends and relatives (22%), and business (13%). This also compares favorably with data from the ABS for the period. Table 1 demonstrates the regions and the number of respondents in each category. Most respondents were traveling to Asia (47.5%), followed by Oceania (28%) and America and Europe (19.6%).
Respondents’ Travel Destinations.
The First Stage: The Measurement Model
This study utilized structural equation modeling (SEM) to test the model and the relationships between variables. As suggested by previous literature, we employed a two-step approach to structural equation modeling to ensure reliability and adequacy of the measurement model before examining the structural model and the hypothesized relationships (see Bagozzi and Yi 1988).
The constructs under investigation were subjected to a series of exploratory factor analyses (EFA) to identify and confirm their multidimensionality. Therefore, travel risk perception, risk-protective behavior, worry, perceived control, and sensation-seeking propensity were subjected to a principal components analysis with Oblimin rotation. A one factorial solution was identified for travel risk perception, worry, and risk-protective behavior. Sensation-seeking propensity, however, loaded on two factors that appeared to be consistent with previous research findings using the BSSS (Sharifpour, Walters, and Ritchie 2013). Two items of sensation-seeking propensity were further removed from the scale as they had a low reliability.
Perceived control was loaded on two factors, represented with two items with cross loadings. Dropping these two items was not recommended as it would lead to factors with as few as two items, in addition to reducing the theoretical strength of the measure. Therefore, the factorial structure of perceived controllability was further examined via confirmatory factor analysis. Cronbach’s alphas for all the factors were all satisfactory and above 0.7, except for one factor of sensation-seeking propensity (0.45), which might be related to the inherent weakness of factors having as few as two items (Worthington and Whittaker 2006). These assured the reliability of scales as well as consistency between responses. In addition to the reliability analyses, the Bartlett test of sphericity and the Kaiser-Meyer Olkin (KMO) measure of sampling adequacy was also performed. For all the constructs, the Bartlett test was significant at 0.000 and the KMO score achieved greater than 0.6, indicating the adequacy of the sample size as well as the existence of the latent factors. Table 2 presents the factor analysis and reliability results of these constructs.
Factor Analysis of all Measurement Items.

Items with cross loadings.
The final measurement models for all the constructs were further examined via confirmatory factor analysis using AMOS 21. The χ2 for the travel risk perception, worry, and perceived control measurement models were significant. However, with improvements made to the initial measurement models, the respecified CFA measurement models suggested a good fit with all the indices above the suggested cut-off points. Table 3 shows the indices results for all the CFA measurement models. These modifications included dropping an item (general travel health and well-being) from the travel risk perception measurement model, as it suggested low reliability. There were also two negative error variances related to the second-order models of sensation-seeking propensity and perceived control. These problems are generally due to the small number of observed variables associated with the latent constructs (Kolenikov and Bollen 2012). In the sensation-seeking propensity measurement model, we respecified the model as a unidimensional construct, which provided a better fit to the data and eliminated the negative error variance. In the perceived control model, negative error variance issue was rectified by constraining the latent factor loadings to one (Kolenikov and Bollen 2012).
Fit Indices Results of CFA Measurement Models.
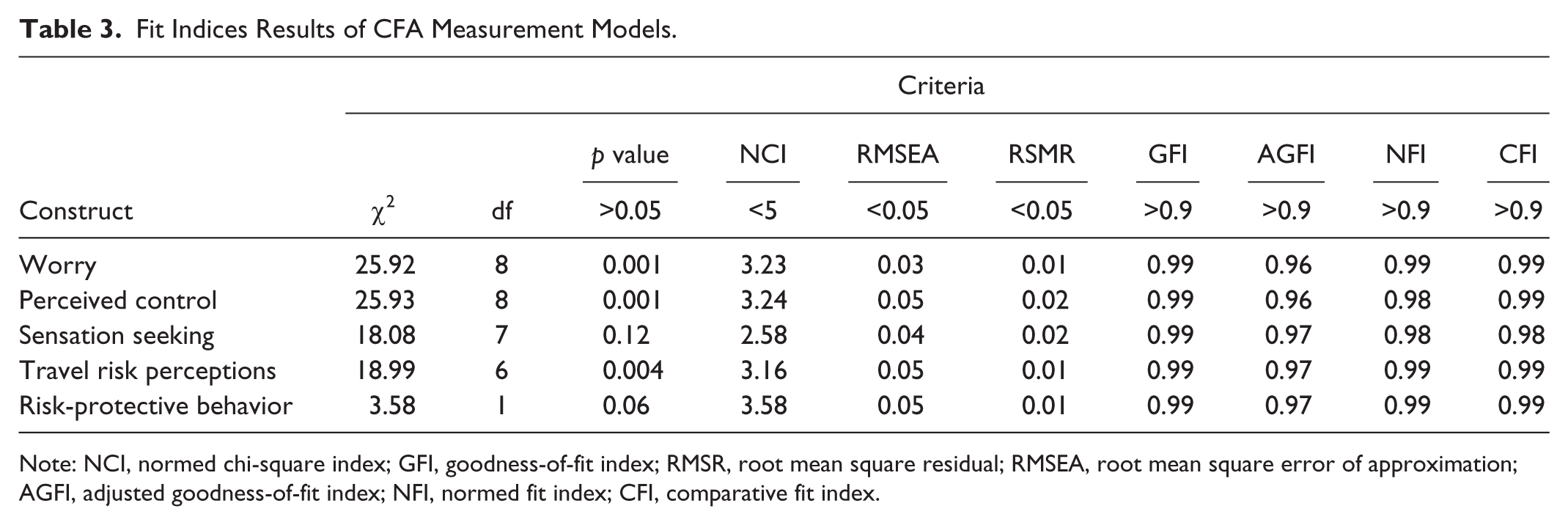
Note: NCI, normed chi-square index; GFI, goodness-of-fit index; RMSR, root mean square residual; RMSEA, root mean square error of approximation; AGFI, adjusted goodness-of-fit index; NFI, normed fit index; CFI, comparative fit index.
The Second Stage: The Structural Model
Achieving confidence in the good fit of all the measurement models and their factorial structure, the structural equation path was designed in AMOS 21. The structural model included a second-order exogenous variable of perceived control, endogenous variables of protective behavior and travel risk perceptions, and two exogenous variables of worry and perceived control.
Assessment of the structural model
According to Bagozzi and Yi (1988), it is necessary to assess the structural model from three different standpoints of “primary fit criteria,” “overall model fit,” as well as “fit of internal structure of the model” that addresses an examination of composite reliability and convergent and discriminant validity. Table 4 shows the results of these assessments. Most tests are satisfactory, confirming the adequacy of the structural model.
Results of Assessment of the Structural Model.
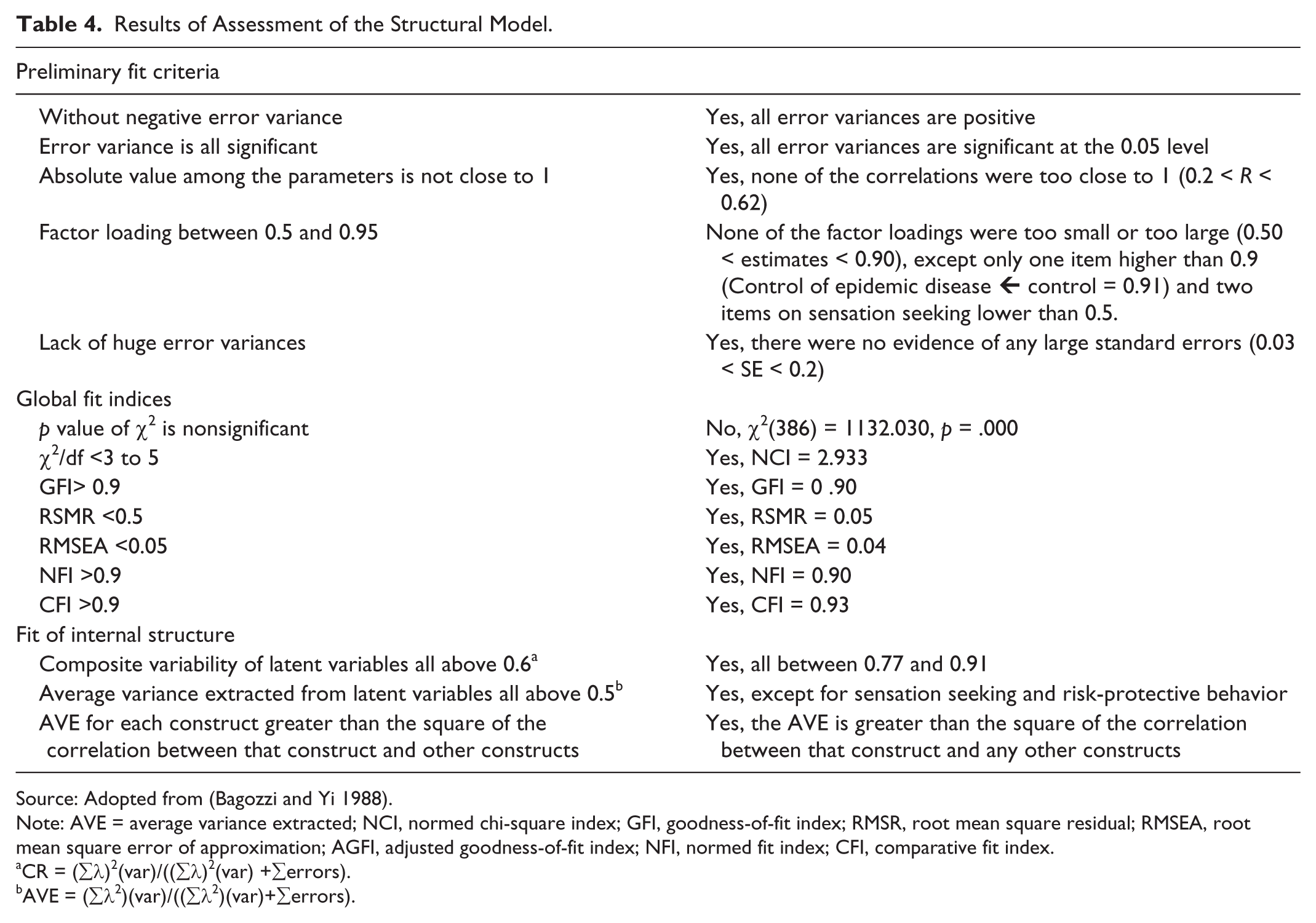
Source: Adopted from (Bagozzi and Yi 1988).
Note: AVE = average variance extracted; NCI, normed chi-square index; GFI, goodness-of-fit index; RMSR, root mean square residual; RMSEA, root mean square error of approximation; AGFI, adjusted goodness-of-fit index; NFI, normed fit index; CFI, comparative fit index.
CR = (∑λ)2(var)/((∑λ)2(var) +∑errors).
AVE = (∑λ2)(var)/((∑λ2)(var)+∑errors).
Among the three assumed covariances between the independent variables of worry, sensation seeking, and control, only the positive association between worry and sensation seeking was significant, and therefore the other two covariances were removed from the model. This was further confirmed with the weak correlation between control and worry as well as control and sensation seeking. The covariance estimates and correlation between these three variables are shown in Table 5.
Covariances and Correlations between Antecedents.

To account for contextual differences, individuals were classified into four categories based on the region they were traveling to (see Table 1). The next step in the SEM analysis was to ensure the created measurement model demonstrates a good fit across all the regions to consider whether the same measurement model can be used across all regions. In other words, this analysis initially tested the influence of the destination and whether travel destination context should be considered in our data analysis. The baseline model was created and it revealed adequacy of the goodness-of-fit statistics across all the groups for the configural model (X2/df = 1.817, comparative fit index [CFI] = 0.91, root mean square error of approximation [RMSEA] = 0.03). Therefore, the next step was to test measurement invariance and to ensure that the measurement model does not show significant differences between the destination groups. Using the automated Multiple Group analysis function in AMOS, the factor loadings were constrained so that the invariance in measurements could be identified. Goodness-of-fit results from this test of invariant factor loadings again provided evidence of a good-fitting model (χ2/df = 1.79, CFI = 0.91, RMSEA = 0.03). The model comparison revealed a nonsignificant difference between the unconstrained and the measurement weight model (constrained factor loadings), with a Δχ2 = 60.076, p = 0.08, and a ΔCFI = 0.001, meeting the recommended cut-off criterion of 0.01. These results demonstrated that factor loadings operated similarly across the three groups and thus the measurement model could be implemented for all the groups. In this study the destination context, measured by destination traveled to, had no influence on the model.
Assessment of the hypothesized relationships
Table 6 presents the summated results of the hypothesized paths. The significant paths of the best-fitting model and the CR values are depicted in Figure 2.
Summarized Results of the Hypothesized Paths.


Significant paths of the final model.
The results support Hypothesis 1 as there was a significant change in the level of risk-protective behavior from travel risk perceptions (β = 0.173, t = 1.092, p = 0.050). Hypotheses 2a and 2b were both supported, as a higher level of worry was associated with a higher level of travel risk perception (β = 0.516, t = 13.545, p < 0.001) and a higher level of protective behavior (β = 0.279, t = 3.521, p < 0.001). Hypothesis 3a was not supported as there was no evidence of a significant change in travel risk perceptions because of a higher level of perceived control. However, an increase in perceived control was associated with a higher level of risk-protective behavior (β = 0.239, t = 2.547, p = 0.03), suggesting a positive relationship. Thus, hypothesis 3b was not supported as the relationship was in an opposite direction to that hypothesized. The findings supported hypothesis 4a as a higher level of sensation-seeking propensity was associated with a lower level of perceived risk, while hypothesis 4b was not supported as sensation seeking was associated with a higher level of protective behaviour (β = 0.177, t = 2.488, p = 0.013).
This study employed the bootstrapping method to investigate the mediation effect of risk perception in the structural model. Bootstrapping is becoming a popular method of testing mediation as it has advantages over other methods (see MacKinnon, Lockwood, and Williams 2004; Preacher and Hayes 2008). Table 7 presents the bootstrap estimates based on 2,000 bootstrap samples, at a 95% bias-corrected percentile. The results indicated significant indirect paths between worry and protective behavior as well as between perceived control and protective behavior. The results also suggested that travel risk perception partially mediates the relationships between tourists’ sensation-seeking propensity and risk-protective behavior. Given the indirect effect is estimated to lie between a confident interval that does not contains zero, alongside the significant direct effect between sensation-seeking propensity and protective behavior, it is concluded that the indirect effect is significantly different from zero at p <0.05. Thus, the relationship between sensation seeking and protective behavior is partially mediated by risk perceptions (Preacher and Hayes 2008), supporting Hypothesis 5.
Bootstrap Results to Test the Significance of Mediation Effect (Indirect Effects).
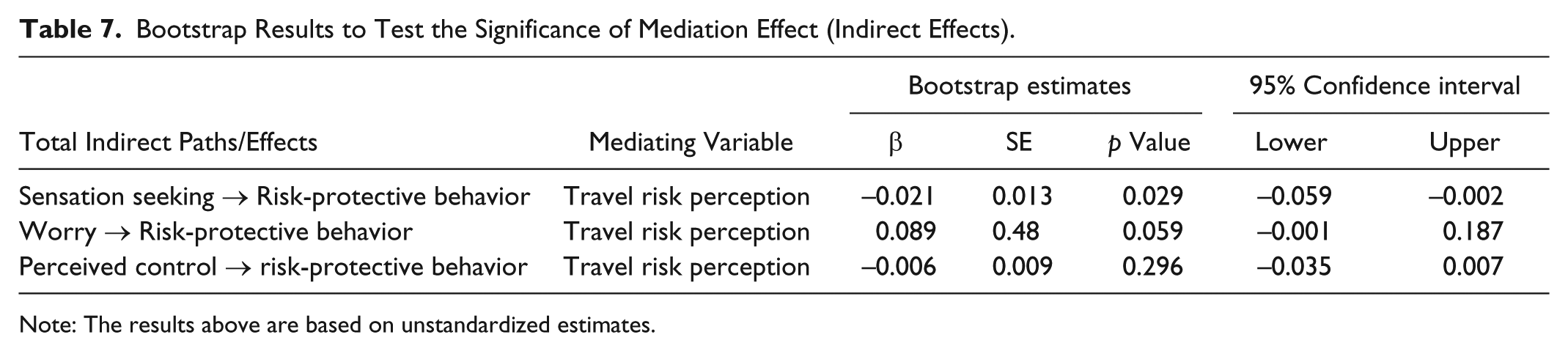
Note: The results above are based on unstandardized estimates.
Discussion
This study represents one of the few to simultaneously examine the psychological factors underlying travelers’ health risk perceptions and their protective behavior. It addresses the relationships among motivational (sensation-seeking propensity), affective (worry), and cognitive (perceived control over risk) factors, as well as their roles in influencing health risk perceptions and travelers’ protective behaviors. Specifically, the study demonstrates that travel health risk perceptions mediate the relationship between the antecedents and risk-protective behavior. This research contributes both theoretically and practically, through an analysis of data gathered from actual travelers rather than those intending to travel in the future.
One of the most significant findings relates to the proposed relationship between perceived risk and worry and how these two constructs influence behavior. The results reveal that individuals’ level of worry plays a significant role in determining their travel health risk perceptions. Specifically, the more worried individuals are about potential risk events, the higher their level of perceived travel risk. Consistent with prior research findings (Rundmo 2002), worry represents a significant dimension of “affect,” which predicts risk estimates and may not depend on cognition. The finding also concurs with Zajonc’s (1980) proposition that emotions are likely to precede cognition and thus influence cognitive judgements.
Sjöberg (1998) noted that worry and risk perception are statistically two independent constructs and hence the way individuals experience risk can be different to their experience of worry. Peters et al. (2006) further suggested that when considering different risks, the level of worry about that risk influences both the way it is perceived and how it is prioritized. Similarly, our study reveals an association between risk and worry, suggesting that worry as an affective dimension is extremely important in influencing both cognition (travel risk perceptions) and behavioral outcomes (risk-protective behavior). Findings from the mediation analysis further show that worry motivates protective behavior through increased health risk perceptions. This finding is consistent with Watkins’s (2008) proposition that worry not only keeps an individual aware of potential threats but also motivates behavior adaptation. It further reinforces the observation that worrisome thoughts enable people to seek out solutions and prepare them for negative outcomes (Hong 2007). Because worrying keeps an issue salient (McCaul and Mullens 2003) and motivates information-seeking and problem-focused solving (Davey et al. 1992), it is considered to be a constructive process in response to potential threats.
Our finding is somewhat different to Reisinger and Mavondo’s (2005) study, which found that perceived risk caused anxiety. We did not include anxiety in our conceptualization, as the present study focused on the antecedents of travelers’ health risk perceptions. As discussed previously, worry predicts anxious and depressive symptoms (Hong 2007). Intuitively, worry may influence risk perception, and risk perception may generate anxiety. Future research should consider testing the relationship among worry, risk perception, anxiety, and protective behavior directly. Subsequently, we also suggest that a much deeper understanding of other affective antecedents is required, such as fear, terror, or panic, and how these specifically influence travel risk perceptions and risk-protective behavior.
Contrary to our expectation, the findings suggest that perceived control is positively related to risk-protective behavior. The mediation analysis further indicates that perceived control influences protective behavior through risk perception. This result contradicts Jonas et al.’s (2011) study which found that travelers associated lower levels of risk perception with health risks that are deemed fully controllable, such as sexually transmitted diseases and drug abuse–related risks. One possible explanation is that an individual’s awareness of protective behavior options can play a role in their perceived efficacy of control over risk events. As Jonas et al. (2011) suggest, respondents in the study may have had lower risk perceptions and felt these types of risk were more controllable because they came from a low health risk–taking sample and understood how to control these risks. It should be noted, however, that Jonas et al. (2011) did not actually measure perceived control; they merely inferred this from their findings by categorizing perceived health risks into three types: difficult to control environmental components (food safety), partially behaviorally controllable (physical injuries), and fully behaviorally controllable (impacts of drug use). Our results suggest that although individuals attribute a specific level of control with a variety of negative health and safety events, it may not necessarily result in changes to the level of travel risk perceptions they associate with these events, if they are not aware of how they can safeguard themselves. Thus, knowledge of the preventative options may be an important factor associated with perceived control and protective behavior (Peters et al. 2006; Weinstein 1989) and should be investigated in future research.
Another possible explanation of our findings relates to our measures of travelers’ perceived control. The respondents might have misinterpreted our question “how much control do you feel you have over travel related risks” as volition or control over exposure to risks, rather than command over outcomes. Consistent with the study by Nordgren et al. (2007), when travelers believe they have control over risk exposure, their voluntary risk appraisal heightens risk perception, which in turn increases risk-protective behavior. It is recommended that future studies apply Rotter’s (1966) locus of control construct or the primary or secondary control components of control (Klein and Helweg-Larsen 2002). Similarly, Bandura’s (1977) self-efficacy construct could be used in future studies, as research on the interplay between self-efficacy and risk is not conclusive and further research has been encouraged (Breakwell 2007).
According to our findings, sensation seekers are more tolerant toward potential travel health risks. This finding appears to support previous findings that sensation seekers are able to account for their consequences and take informed risks; thus they might not engage in activities that might be considered as high risk (Pizam et al. 2004). Although sensation-seeking propensity is negatively related to travel health risk perception, it is positively related to protective behavior, adding new insights into the current literature that has focused on sensation-seeking propensity and tourist behavior at the destination (Lepp and Gibson 2008; Pizam et al. 2004; Sharifpour, Walters, and Ritchie 2013). However, we should note that we used the brief sensation seeking scale and were unable to examine the influence of the subdimensions of sensation seeking as Fuchs (2013) recommends because of the complex nature of the construct. Our analysis further reveals that health risk perception partially mediates the relationship between sensation-seeking propensity and protective behavior. This finding implies that without knowing the availability of precautionary measures, high sensation seekers would simply play down the possibility of potential threats. However, when they are prompted to consider preventative measures or given options to protect themselves, their susceptibility to risks is highlighted and potential threats or risk become salient. This finding underlines the importance of including solutions, not just problems, in travel risk communications, especially when targeting high sensation seekers. In other words, communications that highlight potential health risks must also provide means to effectively minimize or neutralize these risks. Extending further research to include other personality dimensions, such as novelty seeking, venturesomeness, and egocentrism, is also recommended in future studies (see Breakwell 2007) to deepen our understanding of how personality influences risk cognition and behavior.
A key outcome from our research is the downstream consequence of affective and cognitive factors. An understanding of what influences behavior is important, as ultimately governments and industry would like travelers to take precautionary activities prior to travel, such as taking out travel insurance or seeking health advice. Worry was found to have a strong influence on individuals’ protective behaviors. Previous research has also shown a strong correlation between coping strategies and worry (MacGregor 1991), although this strong relationship appeared to exist only for the events individuals assumed to have a high control over. For risk events seen as uncontrollable, worrying was not likely to improve individuals’ ability to manage them (MacGregor 1991). This phenomenon was also reflected in the results of our study, where we found a positive relationship between perceived control and protective behavior. This observation provides additional support to prior research findings that people with a higher level of worry would report a higher likelihood of pursuing protection strategies (MacGregor 1991). Studies have found that the more individuals assumed controllability in preventing risks, the more likely they were to engage in protection strategies (Klein and Helweg-Larsen 2002; Peters et al. 2006). Similarly, as suggested by Peters et al. (2006), worry is an emotional factor and “prepares us for stressful situations by arousing coping strategies” (MacGregor 1991, p. 316). Therefore, the affective component of worry alongside perceived control appears to be an important determinant when it comes to risk-protective behavior.
Importantly, our results reveal that individuals on average indicate neither a high level of perceived travel health risk nor worry about potential risks, with the average level of risk and worry ranging between 2.31 and 3.41 out of a maximum of 7.00. This appears to support previous research suggesting that individuals tend to avoid destinations associated with a high level of risk and these places would have been eliminated from the list of alternatives prior to actual travel (Lepp and Gibson 2008; Sharifpour et al. 2014). In other words, a low level of risk perceptions and worry may not have been found if we had examined potential travelers and their risk perceptions on prospective travel destinations. The research also discovered that destination context did not change the statistical models and findings from the study, despite previous research indicating that travel risks are destination specific (Roehl and Fesenmaier 1992). Finally, there was a direct but small relationship between travel risk perceptions and risk-protective behavior. This relationship may be complex as perceived risk may not only influence protective behavior, but in return protective behavior could also influence perceived risk (Brewer et al. 2004). Some studies have also found associations weaker than expected or even negative links between increased risk perceptions and protective behavior (Van Der Pligt 1998). Future research is required to further clarify the relationship between these constructs and to consider factors that could potentially mediate this relationship.
Taken together, our study aims to investigate the factors that influence travel risk perceptions and protective behavior. It extends the existing literature by focusing on health and safety risks that are commonplace irrespective to destinations. To this end, our conceptual model integrates a range of psychological factors that are often examined separately, with their interplay being overlooked in previous studies. By simultaneously incorporating affective, cognitive, and motivational factors, we demonstrate that worry, an affective antecedent, trump other factors in contributing to a traveler’s health risk perception and protective behavior.
Managerial Implications and Limitations
Our findings offer important implications to the government and tourism industry stakeholders. Although levels of worry are overall low, they do appear to strongly influence travel risk perceptions and risk-protective behavior. Consequently, future travel health and safety communications may need to focus on fear arousal to stimulate concern and worry. Increasing the level of worry among potential travelers, perhaps through public announcement ads or education materials, would lead to higher level of risk perception, which in turn should influence travelers’ protective behaviors Communications which feature vivid images of potential threats to traveler’s well-being, such as transmittable disease or physical injury, may be effective.
Owing to the importance of perceived control, agencies should communicate the ease of undertaking protective measures and highlight the fact that although travelers cannot stop risks (such as crime or natural disasters), they can take actions to either reduce their chances of these negative events occurring or reduce the damage these events may cause. Our findings also shed light on the importance of disclosing potential risks associated with a destination to travelers. Increasing self-efficacy or the perceived confidence of travelers’ ability to take control should, according to this research, lead to increased protective behaviors.
The present research is not without its limitations. Although the sample was representative based on outbound travelers, the model can be tested in other contexts such as other countries to enhance the generalizability of the findings. Some constructs had measurement items that had lower levels of internal reliability (i.e., sensation seeking). This required some re-specification to the measurement model. It is recommended that the full sensation seeking scale should be used in the future, so that the influence of the four independent dimensions on health risk perceptions and protective behavior can be examined (Fuchs 2013). The discussion above identified key avenues for future research, including further investigations to explore the role of affective antecedents (such as fear, anxiety, and panic), motivational factors beyond sensation seeking (such as personality types), as well as self-efficacy and its relationship to perceived control and behavioral outcomes. Associations between the antecedents should also be examined as relationships may be complex (Breakwell 2007). The results did show relationships only between worry and sensation seeking and not between the other antecedents. Sensation seeking is a personality trait that may influence other antecedents such as self-efficacy or locus of control. A more detailed investigation into the psychology of travel risk and protective behavior is strongly recommended in the future. It is hoped that the research outlined in this article has made an initial contribution to this broader research agenda.
Footnotes
Acknowledgements
We would like to acknowledge the support of the Brisbane Airport Corporation for providing airport access, and Dr. Jie Wang for assisting with the data collection.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was funded by a Collaboration and Industry Engagement Fund (CIEF) grant from the University of Queensland.