
Abstract
While travel for physical well-being has long been a practice, medical tourism is an emerging phenomenon characterized by medical care combined with holiday-making activities. The medical tourism industry has rapidly grown due to exponential growth in the number of medical tourists worldwide. Despite this upsurge in practice, less research attention has been devoted to exploring the experience and perceptions of medical tourists toward the wide range of services available to them at medical destinations. This article conceptualizes a construct called “medical tourism experience” and develops a scale that measures it. A rigorous scale development procedure is employed, and four studies are conducted. Seven dimensions of this construct are explored, namely, treatment quality, medical service quality, medical tourism expense, medical tourism infrastructure, destination appeal, destination culture, and ease of access. The results reveal considerable opportunity for marketers and policy makers to increase the attractiveness of medical destinations and gain sustainable competitive advantages.
Introduction
The following scenario, although hypothetical, is not uncommon: Minati Ghosh, a senior administrative officer in a retail bank in New York, was suffering from osteoporosis (a medical condition characterized by fragile and brittle bones due to loss of tissue), which resulted in bone decay in her left knee and impeded her movement. She consulted several doctors in New York, and they suggested a partial knee replacement surgery that would cost her approximately $40,000. Due to this enormous expenditure, Minati decided to go to India to her relatives and undergo the surgery at a low-cost hospital specializing in orthopedic-related treatments located in a town called Manipal. She traveled to India, and the surgery was successfully conducted at a considerably lower cost ($7200, including medicines). After the doctors advised her to walk, she also had a brief yet refreshing tour of nearby places around Manipal with her family. Minati returned to New York three months later in an extremely satisfied state of mind and boastfully shared the experience with her colleagues.
Similar situations occur in the lives of medical tourists who travel to different places, typically across international borders, with the dual purpose of obtaining affordable but good quality medical treatment and holiday making (Connell 2006, 2013; Fetscherin and Stephano 2016). Prior studies reveal that the medical tourism industry has recently and rapidly boomed, predominantly because of the availability of affordable health care technologies (Connell 2013), cheaper transportation facilities (Fetscherin and Stephano 2016), and an augmented level of promotion by hospitals and countries as medical tourism destinations (Moghavvemi et al. 2017; Saadatnia and Mehregan 2014). To cite a real-life example, at the well-known Bumrungrad hospital in Bangkok, “some 40 percent of [the approximately one million patients] are expatriates, tourists, or medical travelers from 190 different countries” (Patients Beyond Borders 2012, 1). Allied Market Research (2017) estimates that the medical tourism industry is expected to grow from $61 billion in 2016 to $165 billion by the end of 2023 at a compounded annual growth rate of 15 percent.
As the number of medical tourists increases globally at a rapid pace, it becomes increasingly important for policy makers and marketers, including hospitals, government bodies, and travel agencies, to explore and measure tourists’ overall experience of their medical tours (Connell 2013; Fetscherin and Stephano 2016). Understanding this experiential aspect of medical tourism is particularly important for several reasons. First, emotional and experiential reactions often prevail among tourists (Otto and Ritchie 1996), including medical tourists (Connell 2006), which may shape their satisfaction level and post-tour decisions, such as whether to visit the medical destination again and whether to spread positive or negative word of mouth to their peers (Connell 2013). Second, medical tourism is an amalgamation of different types of services (Connell 2006; Debata et al. 2015), which means that measuring medical tourists’ experience would facilitate multiple service providers in accurately evaluating their service quality/standards. Third, marketers and policy makers would be able to identify the diverse set of attributes that contribute to a satisfying (or unsatisfying) experience of medical tourists. In turn, the marketers and policy makers would be able to attract potential medical tourists by focusing on all or some of these attributes, refine their quality for better service delivery, and eventually increase inbound patient volume and revenue.
Despite this pragmatic need, little research attention has been devoted to exploring and measuring the experiential reactions of medical tourists in a scientific manner. Although several studies have examined medical service quality in general (e.g., Ali, Basu, and Ware 2018; Guiry and Vequist 2011; Johnson and Russell 2015; Murfin, Schlegelmilch, and Diamantopoulos 1995) and service quality in medical tourism in particular (e.g., Debata et al. 2015; Manaf et al. 2015; Wang 2012), the measurement instruments used in these studies fail to evaluate the diverse nature and subtle nuances of a complex service category, such as medical tourism. For example, the study conducted by Manaf et al. (2015) used a scale that measured dimensions pertaining only to the medical treatment component, such as medical staff quality, supporting services quality, and administrative service quality while completely discounting the tourism component. Similarly, Guiry and Vequist (2011) administered the traditional SERVQUAL scale to measure expectations and perceptions of medical tourists toward health care facilities only. As Connell (2013, p. 2) justly points out, “other than in nomenclature ‘tourism’ has largely been absent from formal discussions of international medical travel,” and it is important for academicians to pay more attention to conducting studies that firmly integrate the polarized aspects of ‘medical care’ and ‘tourism.’ In line with this research agenda, Fetscherin and Stephano’s (2016) study is one of the few to conceptualize and develop a measurement instrument called a “medical tourism index” comprising four factors: country environment, tourism destination, medical tourism costs, and facility and services. However, this instrument is targeted toward exploring the attractiveness of a country as a medical tourism destination and not the experiential reactions of medical tourists per se.
The present study addresses this research gap by conceptualizing a construct called “medical tourism experience” (henceforth MTEX) and developing a scale to measure it. Employing this approach, this study intends to strike a fine balance between the dual aspects of medical care and tourism and to provide new insights to earlier research by employing an experience-focused approach. The article begins with a brief review of the literature on medical tourism and tourist experience followed by a grounded theory approach as suggested by Rossiter (2002). Next, a modified scale development process is undertaken using Churchill’s (1979) methodology. The article later proceeds to develop a conceptual framework that examines the effect of MTEX on two nomologically related variables, namely, medical tourist satisfaction and medical destination loyalty. Lastly, the study concludes by providing salient academic and managerial implications of the MTEX scale.
Literature Review
Medical Tourism
Travel for physical well-being and medical care has long been common practice. Individuals used to travel to spas and health care centers in various parts of Europe during the 18th century, while such destinations as Harley Street in London have been popular international centers of medical care since the 19th century (Connell 2006). What is fairly new as a practice is the emergence of a distinct niche called medical tourism, which is characterized by combining medical care with holiday making (Balaban and Marano 2010; Burkett 2007; Connell 2006, 2013). Regrettably, the current literature is ambiguous as to “what” comprises medical tourism. Many researchers interchangeably use this concept with similar ones, such as health tourism, wellness tourism, vacationing patients, and medicated tourists (Balaban and Marano 2010; Connell 2006, 2013; Fetscherin and Stephano 2016; Hoz-Correa, Muñoz-Leiva, and Bakucz 2018). Such a practice is prevalent probably because there is a continuum that exists from medical tourism, involving medical care and relaxation/holiday making, to more compelling travel situations characterized by major treatments and critical surgeries (Connell 2013).
Because of a growing number of studies in this field, the definitional muddle has gradually begun to fade. Connell (2006, p. 1094) clearly defined medical tourism as a situation “where people often travel long distances to overseas countries to obtain medical, dental and surgical care while simultaneously being holidaymakers.” Heung, Kucukusta, and Song (2010, p. 236) also conceptualized it as a “vacation that involves traveling across international borders to obtain a broad range of medical services. Medical tourism usually includes leisure, fun and relaxation activities, as well as wellness and health-care service.” It is also argued that medical tourism may not be restricted to international travel but also includes situations wherein patients travel to any destination, even within the same nation, with the dual purposes of availing themselves of technically proficient health care services at a competitive price and experiencing pleasurable travel (Chuang et al. 2014; Tham 2018; Yu and Ko 2012).
Extant scholarly works suggest that several factors prompt medical tourists to travel, such as quality of treatment (John and Larke 2016; Wu, Li, and Li 2016), high cost at home (Moghavvemi et al. 2017), as well as unavailability of treatments and lack of insurance (Borman 2004), faster access to medical care facilities (Abubakar and Ilkan 2016), intent to avoid long waiting lines (Snyder, Crooks, and Turner 2011), and cultural proximity between nations (Esiyok, Çakar, and Kurtulmusoglu 2017; Liu and Chen 2013). Inspired by the economic literature, Crompton (1992) further categorized these factors into “push” and “pull.” The push factors focus on the demand side of medical tourism and are mostly consumer- or patient-related, such as sociodemographics (age, income, gender) and health (health status, insurance status). On the other hand, the pull factors emphasize quality of medical facilities and services (quality of medical care, reputation of doctors, accreditation), country environment (country image, stability of economy), and the health care and tourism industry of the country (popular tourist destination, health care costs).
Medical tourism regions are often segmented by inflow of patient traffic from different continents (Tham 2018). By far the largest outbound market is the USA, while Mexico has the highest number of inbound medical tourists (Tore 2016). The Asia-Pacific region, typically in such countries as India, Malaysia, Singapore, and Thailand, is also estimated to be one of the fastest-growing markets for medical tourism (Fisher and Sood 2014). These emerging countries have often been found to deliberately link medical care to tourism and boost attractions for inbound patients (Alsharif, Labonte, and Lu 2010; Connell 2006). However, one major obstacle that marketers (e.g., hospitals, tourism bodies and corporations) often face is to convince distant potential tourists that “medical care in relatively poor countries is comparable with that available at home, in outcome, safety and even in dealing with pain thresholds” (Connell 2006, p. 1094). A twofold strategy may be adopted by marketers to mitigate this problem: (1) first evaluate medical tourists’ experiential reactions to the range of services consumed by them and (2) enrich their perceptions by improving service quality and fixing prevalent service exceptions. One main rationale behind developing the MTEX scale in the present research is to help marketers and policy makers measure the experience of medical tourists and to do away with the perceptual fallacies of potential medical tourists, as mentioned above.
Tourist Experience
In general, tourism and leisure experience is conceptualized as “the subjective mental state felt by the participants” (Otto and Ritchie 1996, p. 166). Researchers also claim that tourist experience is a component of tourists’ psychological environment (Otto and Ritchie 1996), an instrument to describe the meaning of various leisure- and tourism-related events and activities (Mannell and Iso-Ahola 1987), and an essential cognitive or symbolic representation of travel (Nash and Smith 1991). Simply stated, tourist experience is the subjective personal reactions and feelings experienced while consuming leisure or tourism-related services that determine tourists’ nature of evaluation and degree of satisfaction with those services (Otto and Ritchie 1995, 1996).
Existing studies reveal that experience exerts a profound influence on tourists’ cognitive, affective, conative, and behavioral reactions toward a destination and its attributes (Jensen, Lindberg, and Ostergaard 2015; Kim 2014; Kim, Hallab, and Kim 2012; Otto and Ritchie 1995, 1996; Ritchie and Hudson 2009), which explains why one should scrutinize the experiential reactions of tourists, including medical tourists. For example, experience has been found to affect tourists’ sense of well-being, satisfaction, and loyalty toward a destination (Saayman et al. 2018), memory (Kim 2010; Kim, Hallab, and Kim 2012), arousal (Kastenholz et al. 2018), word-of-mouth and future intention to travel (Ali, Ryu, and K. Hussain 2016), service fairness and consumption-related emotions (Su and Hsu 2013), intention to recommend a destination (Hosany and Witham 2010), and a host of other consumer-related variables. Several scholarly attempts have also been made to measure tourism experience by exploring its salient dimensions in a variety of consumption contexts (Kim 2014; Otto and Ritchie 1996; Pijls et al. 2017). For example, Otto and Ritchie (1996) explored six dimensions of service experience in tourism, namely, hedonic, interactive, novelty, comfort, safety, and stimulation, and validated them in three service consumption contexts: airlines, hotels, and tours and attractions. In another rigorous empirical study, Kim (2014) developed a scale called “memorable tourism experience” which includes dimensions such as local culture, activities and special events, hospitality, infrastructure, destination management, accessibility, quality of service, physiography, place attachment, and superstructures. The author concluded that these dimensions are typically related to destination attributes and have a tremendous impact in shaping tourists’ semantic and autographic memory.
Despite this research emphasis in exploring various structural aspects of experiential reactions, less attention has been devoted to date to measuring medical tourists’ experience of the array of services received by them at medical destinations. Although many researchers have adapted the well-known SERVQUAL scale to evaluate service standards in medical tourism (Debata et al. 2015; Guiry and Vequist 2011; Manaf et al. 2015; Wang 2012), most of these attempts have failed to integrate the polarized service components of medical care and tourism concurrently in the same framework. One study that stands out was conducted by Fetscherin and Stephano (2016), whereby a country-based performance measure called a medical tourism index was developed. The authors explored dimensions such as country environment, tourism destination, medical tourism costs, and facility and services. However, close scrutiny of this research reveals the following two aspects: (a) the index measures attractiveness of a country as a medical tourism destination instead of the experiential reactions of medical tourists, and (b) the scale may be administered to any medical tourists irrespective of whether they have already traveled or are yet to travel to the destination. In other words, this index is not intended to capture the intricacies of medical tourists’ experience from a post hoc standpoint and thus does not fill the research gap mentioned earlier.
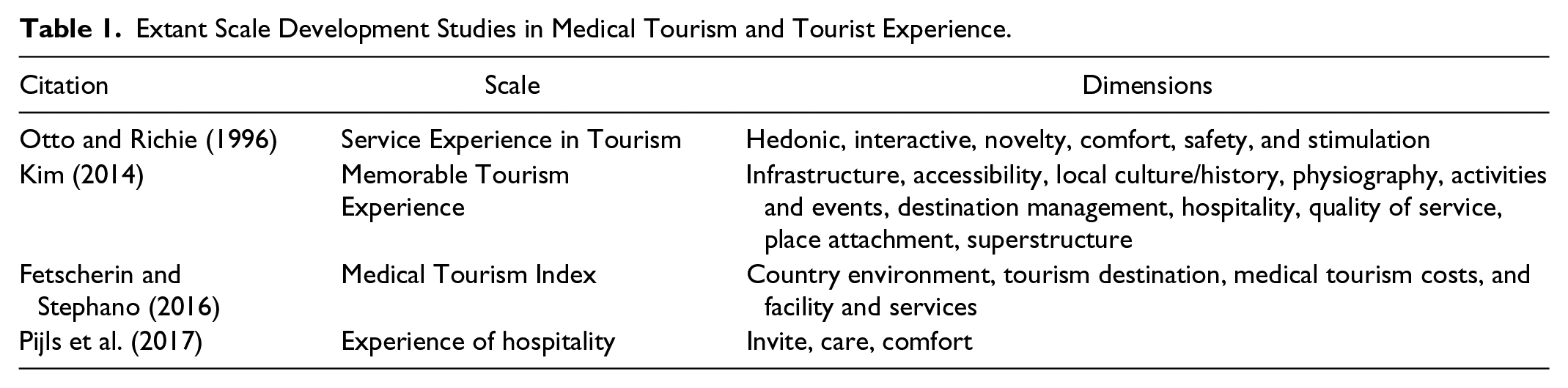
The present research intends to fill this research void by conceptualizing a construct called MTEX and developing a scale that measures it. This scale would measure medical tourists’ experiential reactions about services related to medical care and tourism already received by them at specific medical destinations. This study also aims to complement prior studies on medical tourism by employing an experience-focused perspective. This research is highly important regarding the economic success of multiple service stakeholders at medical destinations. A good starting point was to conduct a thorough literature search in these two fields and review relevant scale development works, which facilitated the identification of baseline dimensions of the construct (see Table 1).
Extant Scale Development Studies in Medical Tourism and Tourist Experience.
Scale Development and Validation Process
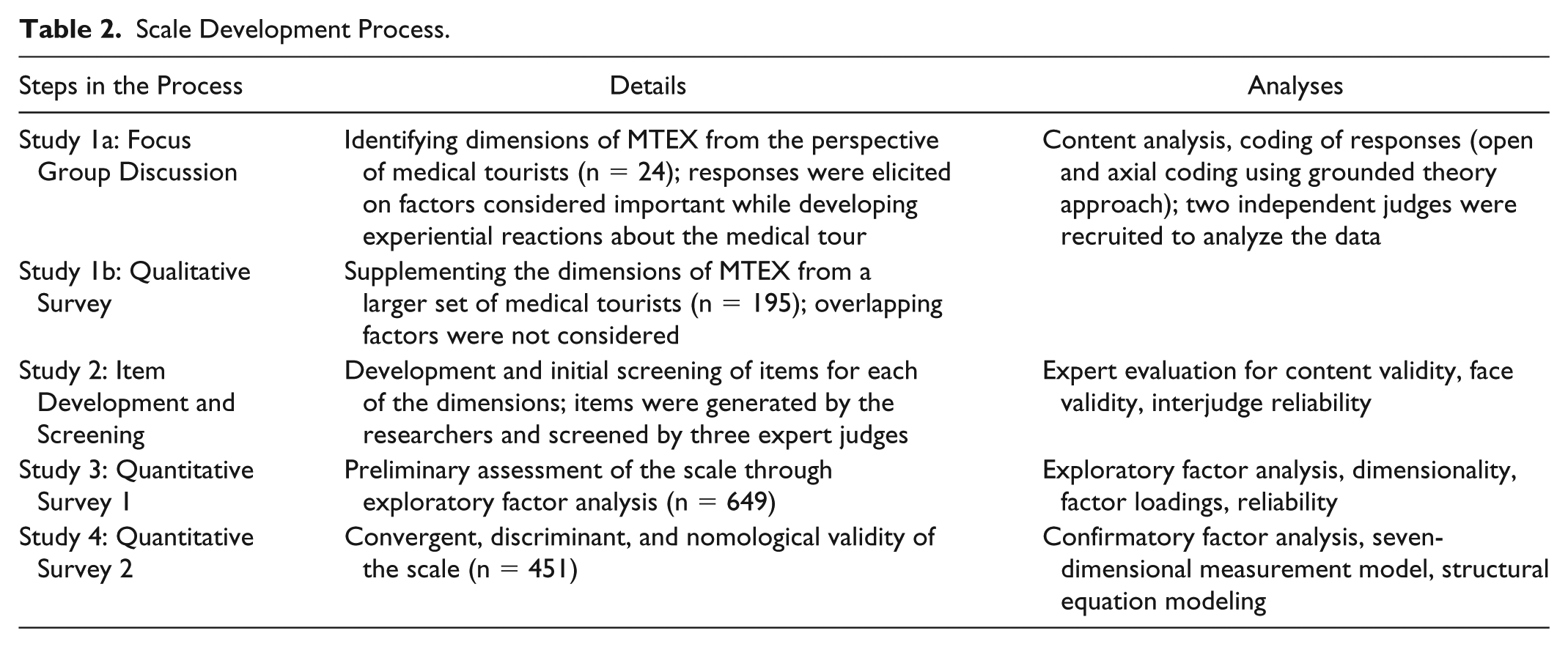
The scale development process incorporated a grounded theory approach (Rossiter 2002; Spiggle 1994) to explore the baseline dimensions of MTEX using the following two sources: (a) an exhaustive review of the literature on medical tourism and tourist experience as mentioned above, and (b) a series of qualitative studies (one focus group discussion, one qualitative survey). While the literature survey helped in identifying the existing dimensions of experience in the context of the hospitality and tourism industry, data from the focus group discussions and qualitative survey were analyzed and coded (open and axial) based on grounded theory principles. This was subsequently followed by an exhaustive item generation procedure, expert review to achieve face validity of the items, data collection and exploratory analysis of the dimensions, and one scale validation study (see Table 2).
Scale Development Process.
Study 1a: Identification of Baseline Dimensions of MTEX through Focus Group Discussions
The focus group discussion included a sample of participants who recently visited (within one month or less) various destinations within or outside India for medical tourism. For all the studies conducted, outside destinations included Turkey, Thailand, Singapore, the Czech Republic, and Israel to name a few. This time frame was chosen to ensure that the participants recalled their true experience without encountering the problems of telescoping, a situation where an individual compresses time by recalling events as occurring more recently than they actually happened (Malhotra 2008). Twenty-four participants (mean age = 44.9 years; 14 men, 10 women; visited outside India = 7, visited within India = 17) recruited through a market research agency for a cash award of Indian National Rupee 500 each were distributed in equal numbers (n = 8) in three discussion panels. This heterogeneous sample facilitated the researchers in capturing a diverse range of experiential reactions, which increased the external validity of the construct. Discussion questions were directed toward exploring various factors considered important in shaping or forming the experience of their medical tourism activity. Some salient questions were as follows: (1) What was your experience on your recent medical tour? (2) Are you satisfied with the medical tour? If so, why? If not, why? (3) What are the things you think are important in forming your overall experience about the medical tour?
Discussion sessions were audiotaped, transcribed, and analyzed using QDA Miner to identify the MTEX dimensions, which included the following stages: first, keywords related to dimensionality were identified and categorized into various dimensions by two independent judges unfamiliar with the research context. This categorization process used open and axial coding principles of grounded theory (Charmaz 2014; Spiggle 1994). Second, interjudge reliability was generated using Cohen’s Kappa (Cohen 1960) formula. The coefficient of agreement between the judges reached 91%. Lastly, the researchers authenticated the dimensions by reconfirming the interpretation of the judges. An example of this coding process is provided below:
The judges identified a dimension called ‘medical tourism expense’ after reading the following transcript:
What things are important in helping you develop your medical tourism experience?
“I think the expenditure incurred by my family is most important to be considered here. The treatment expenses were quite affordable. In fact, the overall cost of staying in the city fit pretty well in our budget. Food costs were also decent. Initially, I had some doubt about whether the expenditure budget would be sufficient for the treatment and the holiday tour. It did fit nicely. Overall we had a nice tour.” (Respondent no. 17, female, age 35 years).
Study 1b: Identification of Baseline Dimensions of MTEX through Qualitative Survey
An open-ended survey was conducted to supplement the MTEX dimensions generated through focused group discussion. The same market research agency was reappointed, and data were collected and analyzed from a sample of 195 participants (mean age = 46.2 years; 116 men, 79 women; visited outside India = 24, visited within India = 171). The questionnaire, sample selection criteria, and coding process by the judges were same as earlier. Cohen’s Kappa measuring interjudge reliability was 93%.
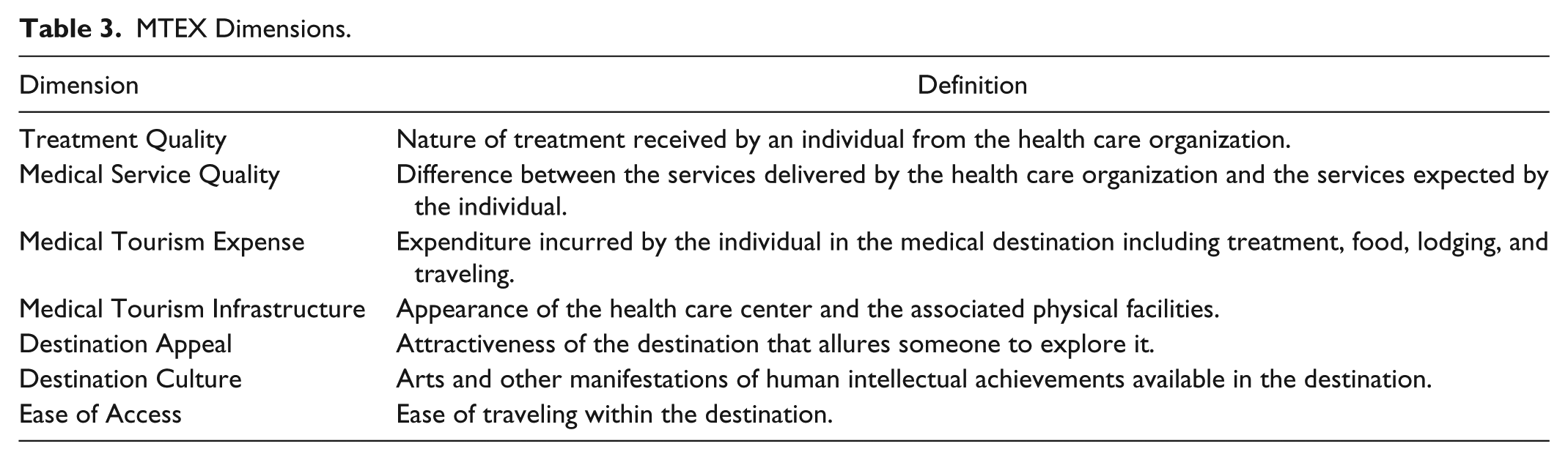
Eventually, reconciliation of dimensions from the literature review, focus group discussions, and the qualitative survey resulted in identifying seven dimensions of MTEX with their construct definitions as suggested by Rossiter (2002). At this point, MTEX was conceptualized as the collective meaning gathered by a medical tourist while traveling, availing treatment, and holiday making in a medical destination (see Table 3).
MTEX Dimensions.
Study 2: Item Development and Screening through Expert Reviews
Fifty-seven items for seven MTEX dimensions were subsequently generated and subjected to face validity by three experts appointed for the study. These experts were marketing faculty members of a major south-Indian university, had a fair amount of knowledge of travel- and tourism-related research, and were very well acquainted with the scale development process in general. Following DeVellis’s (2003) method, items were then reviewed for similarity, relevance, and ambiguity with respect to one of the seven MTEX dimensions. The researchers then analyzed expert ratings using ANOVA and identified whether an item was statistically less relevant than other items belonging to a particular dimension. At the conclusion of the entire process, the researchers were left with a reduced pool of 43 items.
Study 3: Preliminary Assessment of the Scale—Scale Purification, Reliability, and Dimensionality
The same agency was again contacted for another phase of data collection using a survey. Sample selection criteria were identical with the previous studies, except that the time frame was increased to three months in order to capture a larger range of respondents. The questionnaire had (a) 43 items of MTEX; (b) demography-related items such as age, gender, education, income, occupation, and designation; and (c) respondent screening questions. Responses on the MTEX items were elicited on a five-point Likert-type scale (1 = strongly disagree, 5 = strongly agree). Out of 889 survey responses, researchers reached a usable sample size of 649 (mean age = 45.3 years; 387 men, 262 women; visited outside India = 130, visited within India = 519) after screening for completed responses, sample relevance, and poor response quality.
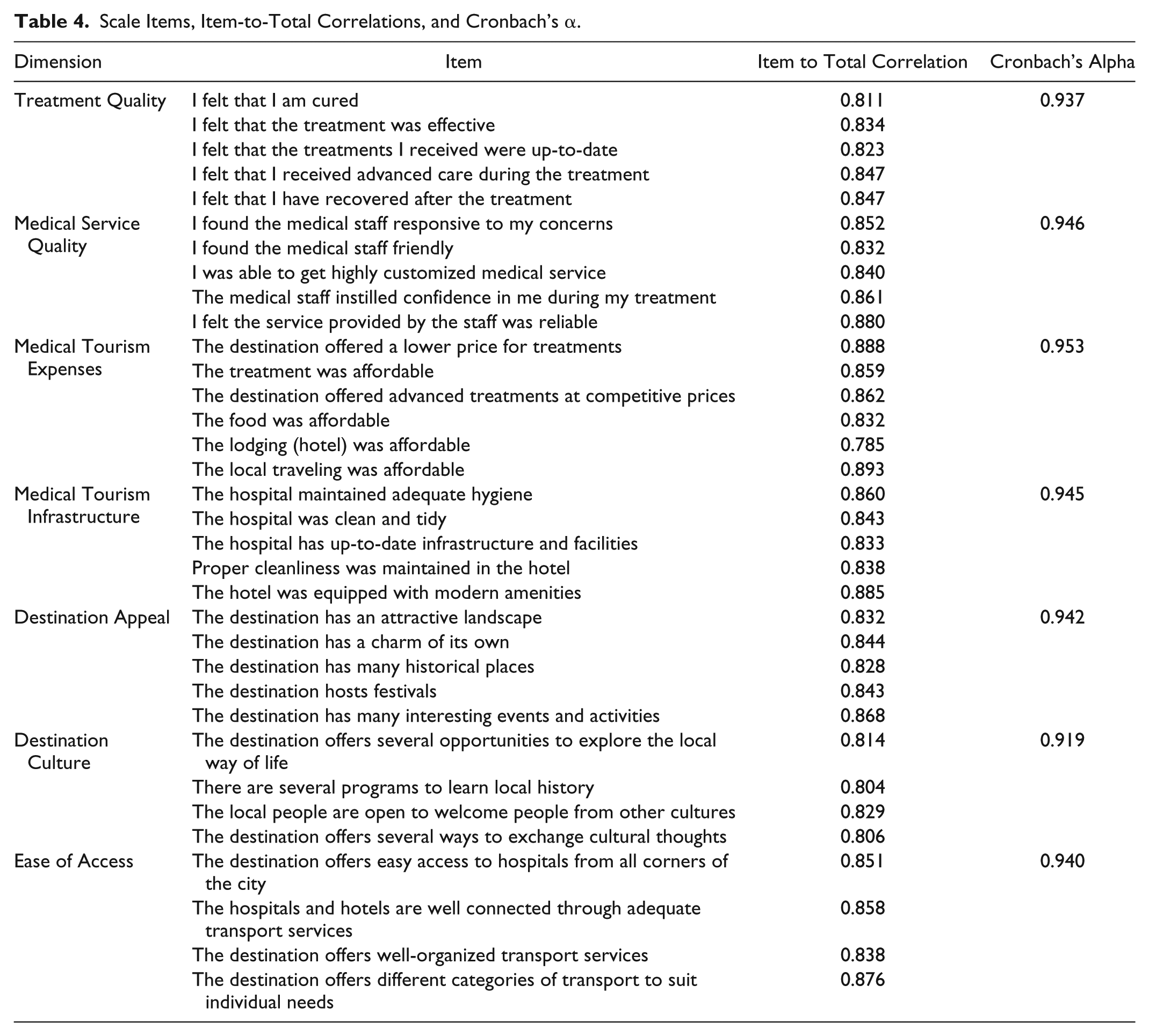
To identify the factor structure of MTEX, a principal component analysis (PCA) was conducted followed by an orthogonal rotation (Varimax). A seven-component solution was obtained after using the following factor extraction criteria: (a) eigen value > 1, (b) factor loading score of each component > |0.50|, (c) Scree plot (all components with sharp descent were retained), and (d) meaningfulness of the extracted components (Churchill 1979; Nunnally 1978). Five items had low factor loading (less than 0.50 on the corresponding components), and four items had high cross-loading. These nine items were dropped, and PCA was performed again with the remaining 34 items, which resulted in a meaningful seven-factor solution. All the items loaded on relevant factors as expected with no cross-loading. These seven dimensions of MTEX explained approximately 81.92% of the total variance. For each of the seven dimensions, the α coefficient met Nunnally’s (1978) criterion of α > 0.60 and reflected a high level of internal consistency or reliability (see Table 4). A confirmatory factor analysis was subsequently conducted to assess the validity of the scale, the results of which are presented in the next study.
Scale Items, Item-to-Total Correlations, and Cronbach’s α.
Study 4: Validation of the MTEX Scale
Convergent and Discriminant Validity
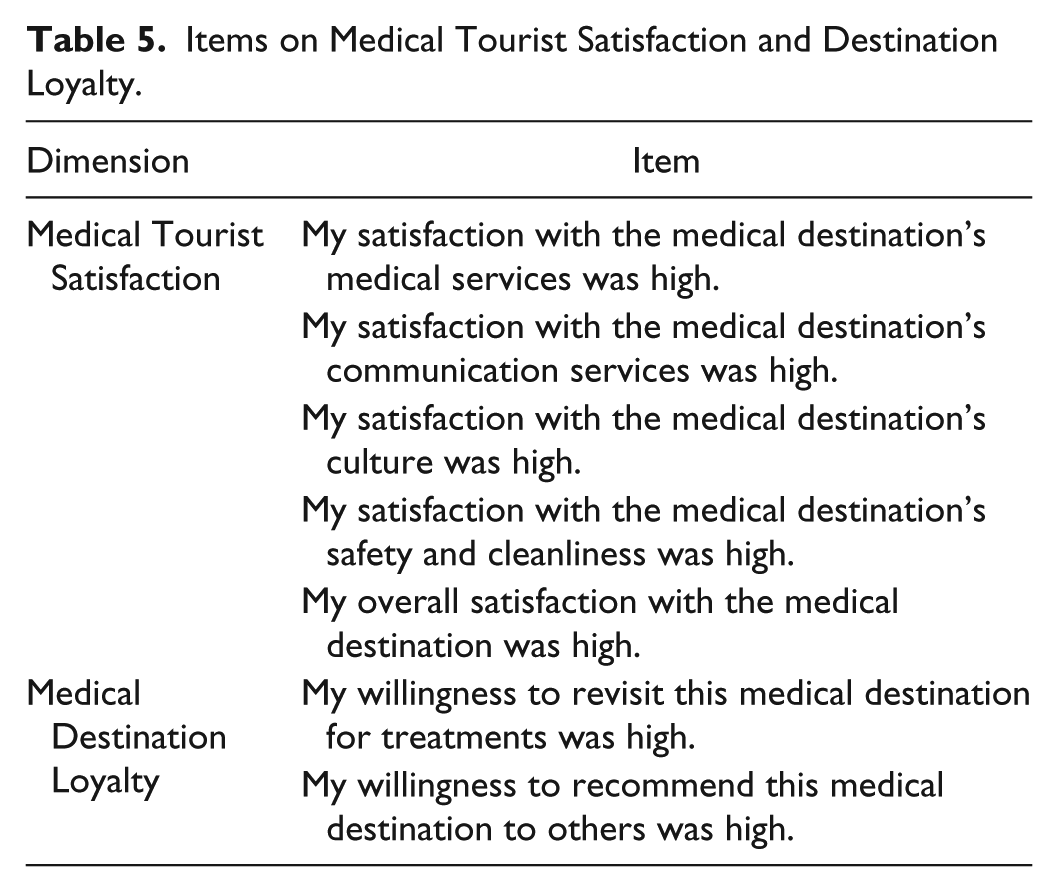
Data using a survey were collected by the same market research agency to validate MTEX as a sound theoretical construct. The target sample was same as that of Study 3. The questionnaire included (a) 34 items of MTEX; (b) five items on medical tourist satisfaction and two items on medical destination loyalty adapted from Chi and Qu (2008) (see Table 5) required in assessing the nomological validity of MTEX; and (c) items to capture demographic and medical tour–related information. Responses to the MTEX items were elicited using a five-point Likert-type scale (1 = strongly disagree, 5 = strongly agree). Out of 559 survey responses, a usable sample size of 451 was reached (mean age = 41.4 years; 298 men, 153 women; visited outside India = 39, visited within India = 412) after screening for completed responses, sample relevance, and poor response quality.
Items on Medical Tourist Satisfaction and Destination Loyalty.
First, a second-order confirmatory factor analysis (CFA) was conducted using AMOS 20.0. Examination of how the data fit the CFA model was performed using a set of goodness-of-fit indices, namely, the parsimony comparative fit index (PCFI), goodness-of-fit index (GFI), and normed fit index (NFI) (Hu and Bentler 1999). PCFI (0.939), GFI (0.925), and NFI (0.955) revealed high goodness of fit, as all these values were more than 0.90. The chi-square statistic was statistically significant: χ2=536.87, DF = 527, p < 0.01 (χ2/DF = 1.019). In addition, root mean square error of approximation (RMSEA) was 0.007, which was below the approved cut-off of 0.50. These results indicated that data collected for Study 4 sufficiently fit the measurement model.
Next, the reliability of the MTEX dimensions was confirmed using the composite reliability index, which was found to be higher than the recommended level of 0.60 (Bagozzi and Yi 1988). The average variance extracted (AVE) for each dimension was also higher than the recommended level of 0.50 (Hair et al. 1998) (see Table 6).
Composite Reliability and AVE of the Dimensions.
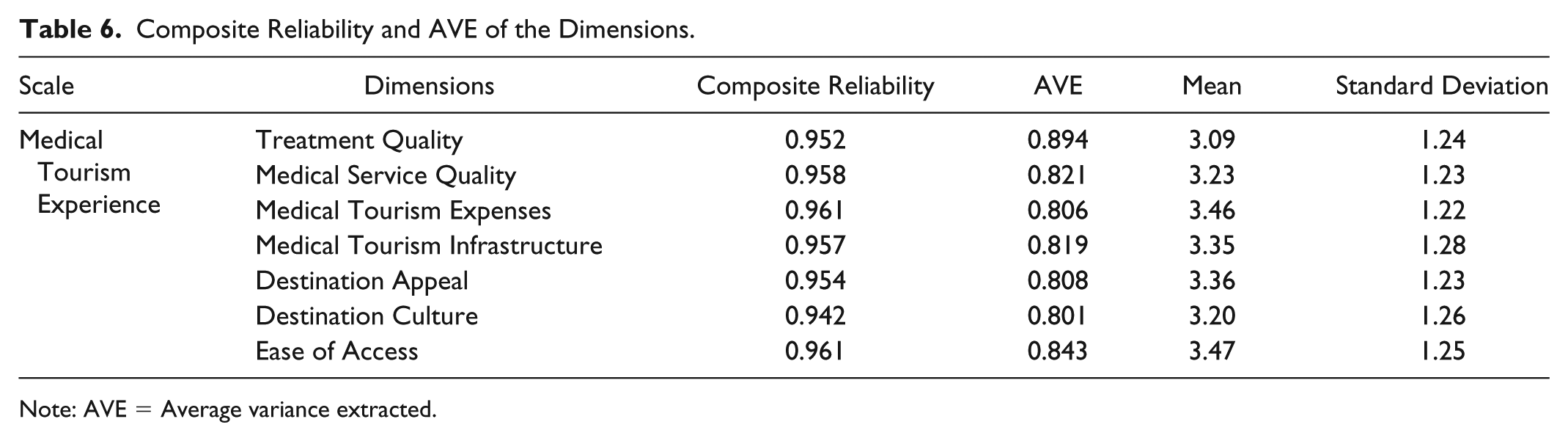
Note: AVE = Average variance extracted.
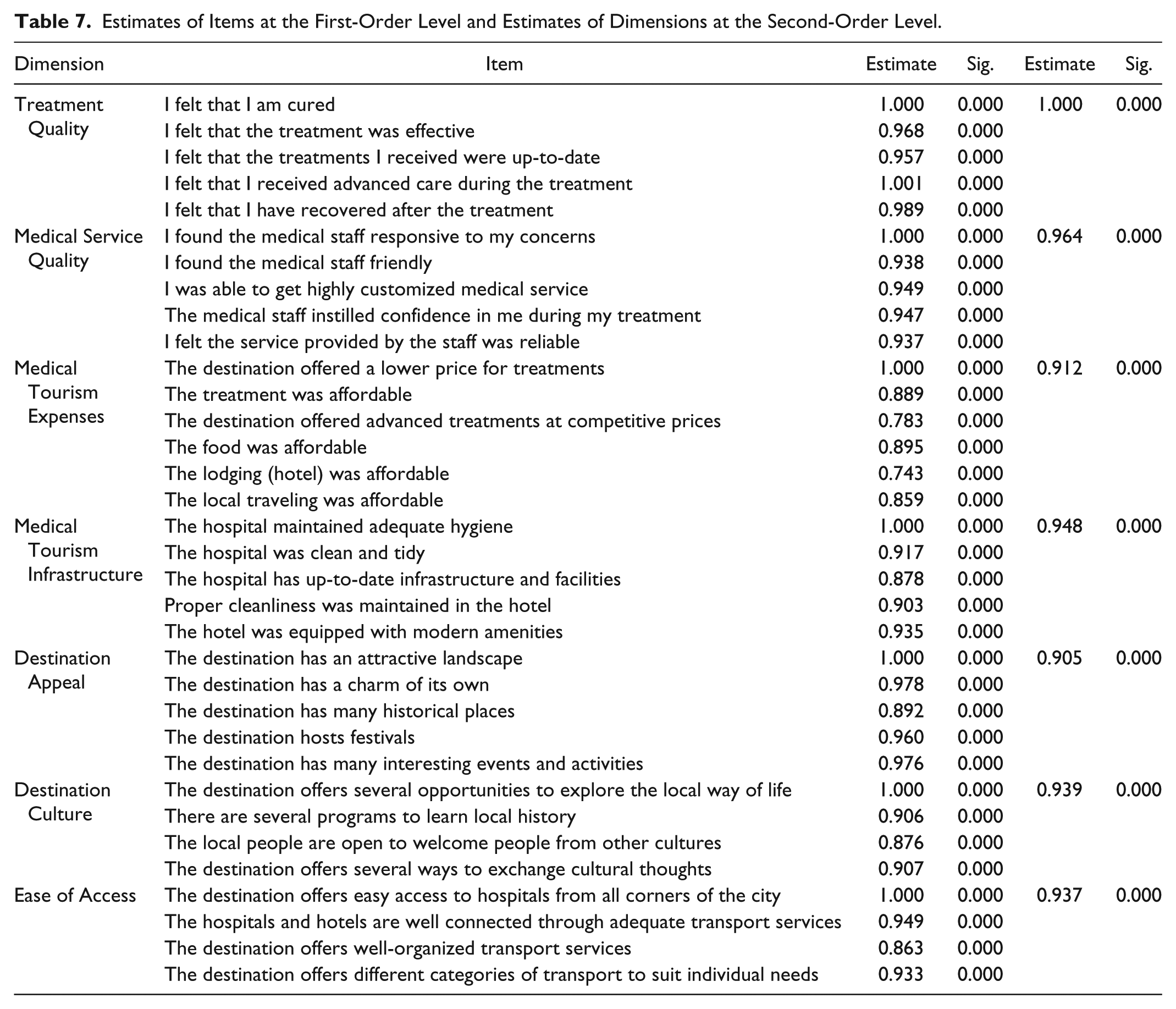
Lastly, the convergent and discriminant validity of MTEX was examined. The second-order CFA mentioned earlier empirically validated two things: (a) whether the 34 items of MTEX measured seven dimensions of MTEX and (b) whether these seven dimensions belonged to MTEX statistically. The results revealed that at a first-order level, all 34 items significantly loaded (p < 0.01) on the corresponding constructs. More importantly, at a second-order level, these seven dimensions significantly loaded (p < 0.01) on MTEX. These results met the criteria suggested by Fornell and Larker (1981) and Bagozzi and Yi (1988) and confirmed the convergent validity of the scale (see Table 7). Discriminant validity was examined by comparing the AVE of each construct to the shared variance (squared correlation) between the construct and all other variables. For each such comparison, the AVE exceeded all combinations of shared variance (see Table 8). Hence, discriminant validity of the webcare quality scale was also confirmed.
Estimates of Items at the First-Order Level and Estimates of Dimensions at the Second-Order Level.
Composite Reliability, AVE, and Correlations.
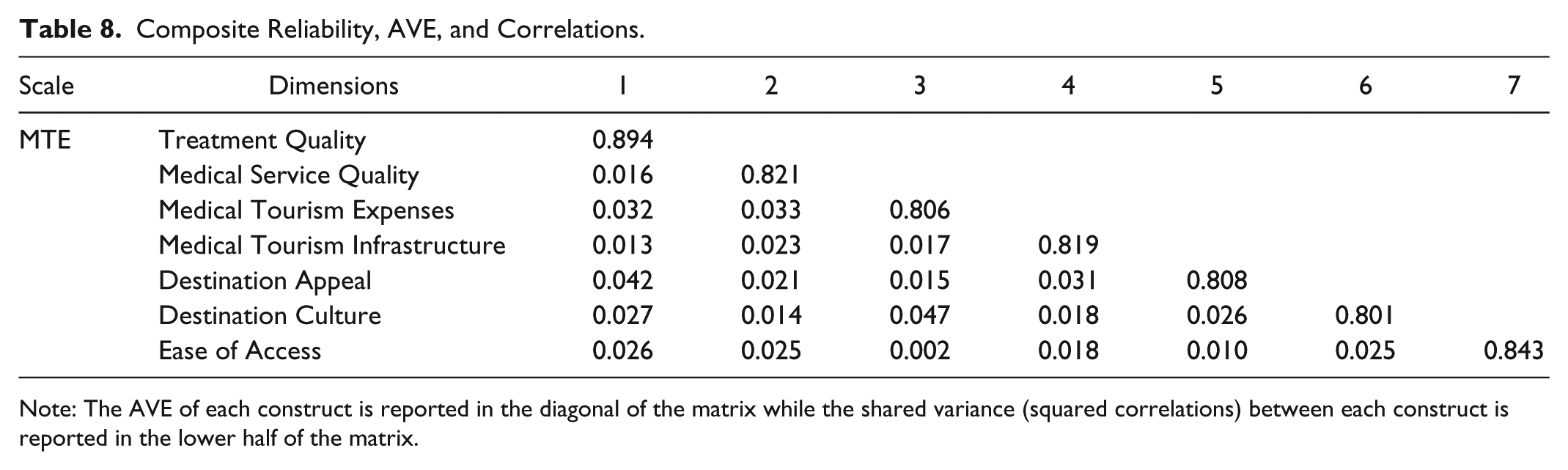
Note: The AVE of each construct is reported in the diagonal of the matrix while the shared variance (squared correlations) between each construct is reported in the lower half of the matrix.
Nomological Validity
To assess the nomological validity of MTEX, two theoretically related constructs were identified from prior studies, namely, medical tourist satisfaction and medical destination loyalty. The definitions of these constructs were then adapted to fit the present research context. Following Heung and Cheng (2000), medical tourist satisfaction was conceptualized as a medical tourist’s evaluation of services availed in the medical destination in comparison to their perceived expectations. Satisfaction resulted if performance exceeded expectations; otherwise it resulted in dissatisfaction. Similarly, based on the definition provided by Toyama and Yamada (2012), medical destination loyalty was conceptualized as the intention of medical tourists to revisit the medical destination and to recommend it to their peers and relatives. Thus, the following hypotheses were developed:
Hypothesis 1: MTEX positively affects medical tourist satisfaction.
Hypothesis 2: MTEX positively affects medical destination loyalty.
To test these hypotheses, data were subjected to a second-order structural equation modeling in which empirical linkages between MTEX and these variables were established (see Figure 1). The results revealed that the estimated model fit the data reasonably well: PCFI = 0.928, GFI = 0.917, NFI = 0.943, RMSEA = 0.037, with χ2 =1073.28, DF = 533, p < 0.01 (χ2/DF = 2.01). As predicted, the effect of MTEX was positive and statistically significant on both the dependent variables: medical tourist satisfaction (path coefficient = 0.56, p <0.01) and medical destination loyalty (path coefficient = 0.47, p < 0.01). This finding supported hypotheses 1 and 2, and the nomological validity of MTEX was also established.
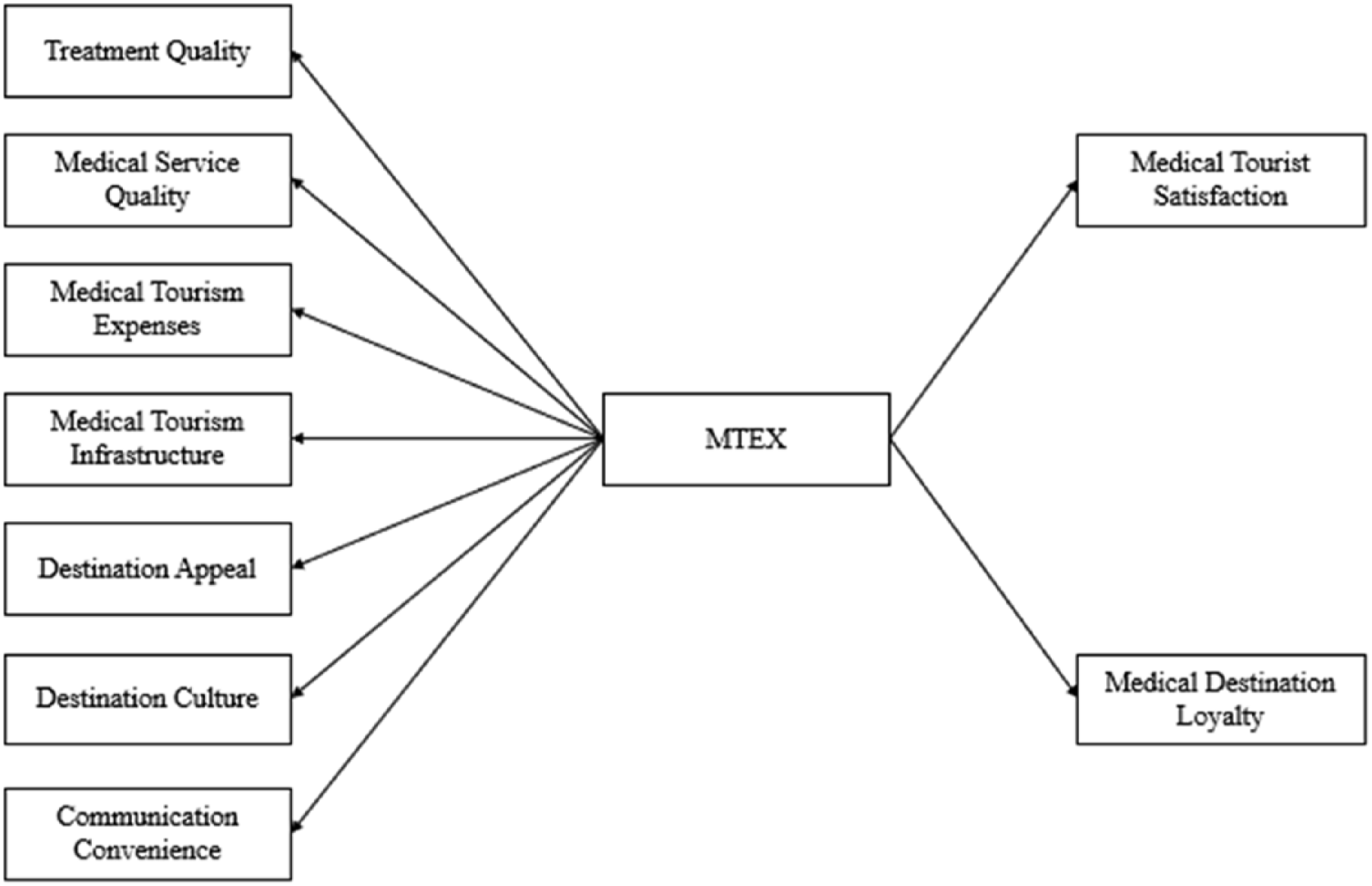
Conceptual framework for nomological validity.
Lastly, since consumption experience has been found to positively affect consumer satisfaction in earlier studies (Saayman et al. 2018; Otto and Ritchie 1995, 1996), it was interesting to investigate whether salience of the MTEX dimensions on medical tourist satisfaction varied between satisfied versus dissatisfied respondents. To examine this relationship, respondents were categorized into two groups (low satisfaction and high satisfaction) based on a median split of the variable, medical tourist satisfaction. Prior to the median split, mean medical tourist satisfaction scores across five items for all respondents were calculated (lowest score = 1.00, highest score = 5.00, median score = 3.00). Respondents with scores lower and higher than 3.00 were categorized into low (n = 218) and high (n = 196) medical tourist satisfaction groups, respectively. Respondents with scores exactly equal to 3.00 (n = 37) were removed from the analysis. A multiple regression analysis was then conducted with medical tourist satisfaction as the dependent variable and the MTEX dimensions as the independent variables. Results revealed that both the regression models were statistically significant (FModel1 = 20.36, p < 0.001; FModel2 = 17.42, p < 0.001) (see Table 9). It was also revealed that as the satisfaction level decreased, salience of dimensions (βs) related to medical care, that is, treatment quality, medical service quality, medical tourism expenses, and medical tourism infrastructure increased, while the weightage of dimensions (βs) related to holiday making, that is, destination culture, destination appeal, and ease of access decreased. In addition, another comparative analysis was conducted in which the effects of the MTEX dimensions were compared between Indian and international tourists using two multiple regression models in which medical tourist satisfaction was the dependent variable and the MTEX dimensions were the independent variables. The first model was run on the data collected from the tourists who traveled within India, while the second model included data collected from tourists traveling to international destinations. Results revealed no significant difference in the R2 and beta coefficients between these models (F < 1.00, n.s.). This increased the generalizability of the MTEX construct.
Multiple Regression Results.
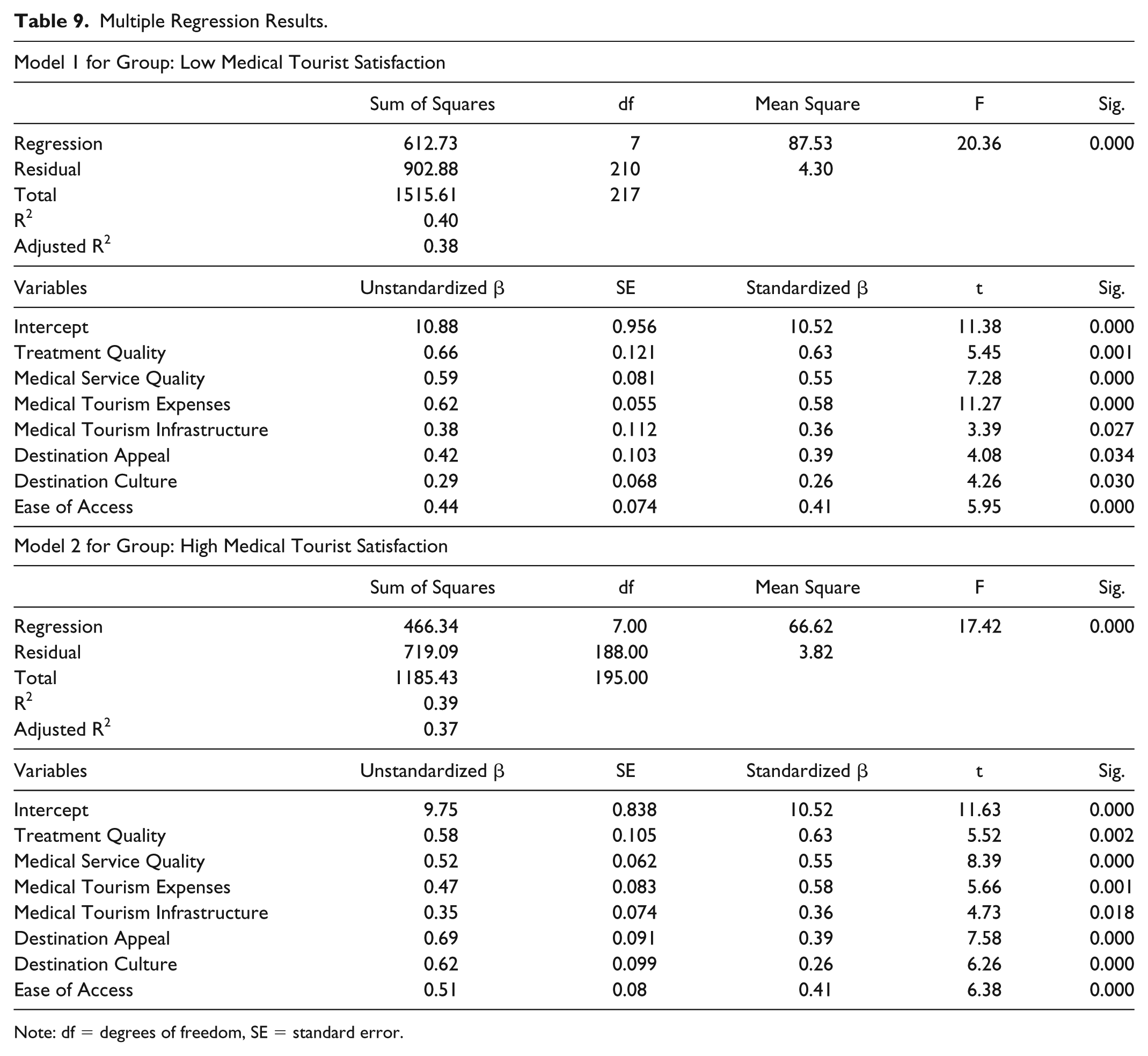
Note: df = degrees of freedom, SE = standard error.
Discussion and Implications
Traveling to distant places, typically across international borders, in search of good quality health care services has been common practice for decades. In recent times, medical tourism has grown exponentially as a phenomenon characterized by polarized travel purposes: obtaining medical care and relaxation or holiday making. When the industry gradually began to grow in the 21st century, there were selected hospitals and countries that promoted the concept of medical tourism. Today, medical tourism is an approximately $100 billion industry, with 6 million medical tourists actively engaged in medical tourism who travel globally to seek better medical treatment and simultaneously participate in tour-related activities.
Despite this remarkable size and growth, empirical insights into constructs that explore the experience and perceptions of medical tourists regarding a large range of services received at medical destinations remain scant. This article attempts to fill the gap in medical tourism literature by conceptualizing a construct called MTEX, which measures the post-consumption experience of medical tourists regarding their entire travel, medical treatment, and holiday-making activities. A grounded theory approach as suggested by Rossiter (2002) and Spiggle (1994) is used to explore baseline dimensions of MTEX from three sources: (a) prior studies dealing with experiential reactions of tourists, including medical tourists; (b) focus group discussions; and (c) a qualitative survey. Subsequently, a rigorous multistep scale construction procedure is adopted from Churchill (1979), which involves a large sample of medical tourists who have recently completed their medical tours in various destinations. Seven dimensions of MTEX, namely, treatment quality, medical service quality, medical tourism expense, medical tourism infrastructure, destination appeal, destination culture, and ease of access, comprising 43 items, are explored and empirically validated. At a second-order level, MTEX is found to positively affect two nomologically related constructs, that is, medical tourist satisfaction and medical destination loyalty. More interestingly, it is found that dimensions related to medical care (i.e., treatment quality, medical service quality, medical tourism expenses, and medical tourism infrastructure) compared to holiday making (destination appeal, destination utility, and ease of access) have a more positive effect on satisfaction when medical tourists are less satisfied than when they are more satisfied. In other words, the former set of dimensions is more critical to affecting satisfaction of those who are less satisfied compared with the more satisfied medical tourists. In contrast, confidence in the latter set of dimensions on satisfaction is greater when tourists are more (as compared to less) satisfied.
The implications of developing the MTEX scale are pertinent to both research and practice. From an academic perspective, the present study makes numerous contributions. First, it provides a new research direction in medical tourism literature by integrating tourists’ experience in medical care services and relaxation/holiday-making activities. Prior studies are mostly scattered and do not systematically capture experiential reactions of medical tourists. For example, Kim (2014) developed a scale called “memorable tourism experience,” which consists of many destination-specific attributes. However, most of these attributes are relevant in the overall tourism context and fail to capture the subtle nuances of a complex service category such as medical tourism. Therefore, this article is a step toward bridging the gap by offering salient insights into medical tourists’ post-consumption perceptions of services ranging from medical care to tours and relaxation. Second, while many studies in medical tourism have investigated the factors affecting the selection of a particular medical destination, the present research complements these works by analyzing the experience of medical tourists in these destinations. This study also takes a step forward and empirically demonstrates that positive experience leads to higher levels of satisfaction and loyalty toward medical destinations. Third, the body of knowledge already available on the application of SERVQUAL dimensions in medical tourism will benefit immensely from the present research findings. Although researchers have already conceptualized medical tourism service quality and its dimensions related to medical care services, this study brings into focus tourists’ own perceptions, not only of medical care services but also of such attributes as destination appeal, culture, and ease of access. The scale also signals the need to conduct a series of studies that move beyond the health care perspective and encompass a more holistic understanding of medical tourism. Lastly, the scale developed in this study contributes to the wide array of available studies on postconsumption experience. To this body of knowledge, which investigates the process of seeking value from experience after consuming a product or service, this study adds fresh insights into the dimensions of experience in an emerging service sector such as medical tourism. In addition, this research enables academicians to appreciate how experiential value dimensions vary with the change in consumption contexts from one product/service category to another.
From the perspective of marketers and policy makers, this article makes several contributions. First, national and local government authorities, managers of travel agencies, and hospital owners may administer the MTEX scale to outbound medical tourists and probe more deeply into their experience, level of satisfaction, revisit intention, and propensity to share positive word of mouth. Second, administration of this measurement instrument empowers marketers and policy makers to precisely evaluate their service standards. For example, if a medical tourist is not satisfied with the quality of treatment, his or her evaluation will be promptly evidenced in the respective items of the scale. In turn, the concerned hospital authority may precisely track the exact problem and work immediately to rectify or improve it. Third, companies that provide bundled medical tourism packages may concentrate their marketing efforts on specific dimensions in order to achieve a sustainable competitive advantage. For example, a bundled package that includes affordable yet high-quality treatment, cheap air fare, decent lodging arrangements, and a compulsory posttreatment tour to local places has an immense likelihood of being rated high in the MTEX scale. This also ensures that medical tourists are highly satisfied, share their positive experience with others, and return to the same medical destination (same country and same health care organization) if and when necessary. Fourth, this article offers numerous opportunities for policy makers, specifically local government, to attract potential medical tourists through activities such as hosting festivals, renovating worn-out historical locations, prompting cultural exchanges, and collaborating with reputed hospitals. Strategic endeavors such as these will draw the attention of medical tourists because destination appeal is an important aspect of holiday making and helps develop favorable experiences among medical tourists. Fifth, medical destinations with open cultures often become prime candidates in offering medical services. Medical destinations must, therefore, make appropriate efforts to promote their local culture and to attract and retain medical tourists. Random yet positive encounters with residents will help medical tourists become familiar with the destination culture. Furthermore, their friendliness and hospitality may make them feel comfortable in a new location. Such things are vital for delivering satisfying MTEX. Lastly, the scale can be further utilized to compare the capacity of medical destinations to deliver a favorable experience. Hence, random surveys of medical tourists will help destination marketers to understand their respective performances in each of the seven dimensions. This would help them prioritize destination attributes and develop promotional campaigns based on top-rated attributes or dimensions.
Limitations and Future Research
While a rigorous empirical procedure was employed to develop the scale, there are some limitations in the present study. First, as it was conducted in the context of a developing nation such as India, its findings may have limited generalizability. As mentioned earlier, medical tourists’ perceptions toward treatment outcome and safety are more negatively biased when the medical destination is a developing nation rather than a developed one. Future cross-cultural studies should be conducted to test the generalizability of the instrument and drop/add country-specific dimensions if necessary. Second, the majority of the survey participants traveled within the country, that is, India. Though it is now a known fact that cross-country travel is not a necessary condition for medical tourism, future research is needed to examine whether the same set of MTEX dimensions shape the experience of those who travel globally for medical tourism purposes. Third, the nature or critical aspect of the treatment, which may interact with the experiential reactions or perceptions of medical tourists, was not captured in the scale development process. Data were collected from a large group of medical tourists who traveled to avail themselves of treatment for a variety of health-related issues. This homogeneity in the sample, although it increases the applicability of the instrument, ignores the fact that the degree of importance of each scale dimension may be dependent on the medical tourists’ health conditions. When the treatment is less critical, such dimensions as destination appeal, culture, and ease of access may play a more important role in overall experience formation. However, for more serious health-related treatments, such dimensions as treatment quality, medical service quality, and medical tourism expenses may increase in degree of importance. Therefore, future researchers should classify medical tourists into groups according to the critical nature of their treatments, administer the scale separately to each group, and explore whether and to what extent the weighting of each scale dimension varies based on criticality of treatment.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.