
Abstract
This study aims to develop and test a theoretical model that predicts individuals’ intention to engage in medical tourism. Structural equation modeling (SEM) was performed to test the study hypotheses by using data collected from 246 US residents. The study results indicated that perceived benefits were positively, and perceived barriers negatively, associated with attitude, and perceived barriers had a negative impact on perceived behavioral control. The study results further revealed that attitude, perceived behavioral control, and subjective norm positively influenced individuals’ intention to engage in medical tourism. Finally, a significant moderating effect of perceived severity was found on the relationships between perceived benefits and attitude, perceived barriers and attitude, and attitude and behavioral intention. The findings of the study offer valuable theoretical contributions and practical implications in the context of medical tourism.
Keywords
Introduction
Emerging as a new type of alternative tourism, medical tourism has involved individuals traveling to another country with the purpose of obtaining non-emergency health care services. As a part of medical tourism, people either travel from developing countries to highly developed countries for medical treatment that is not available or legal in their home country, or they travel overseas from highly developed countries to developing countries to obtain medical care because of the low cost and relatively short wait times (Johnston et al. 2011). The globalization of health care and other factors such as advanced health care technologies and skills in host countries, the explosion of complex communication and transportation technologies, and the inclusion of a vacation element in which a patient might enjoy the local environment while seeking health care treatment have made medical tourism one of the fastest growing and most profitable tourism sectors in the world (Fortune Business Insights 2018; Seow et al. 2017; Fetscherin and Stephano 2016). The market size of the medical tourism industry, which was $45 to $100 billion in 2017 and is expected to grow to 25% annually in the coming decade (Medical Tourism Magazine 2016; Patients Beyond Borders 2018), and many countries, especially Asian countries including Singapore, Thailand, and India, have reached a notable position in the international medical tourism market (Moghavvemi et al. 2017; Zarei and Maleki 2018). Nearly 16 million patients travel internationally every year and spend an average of $3,800 to $6,000 per visit on healthcare costs and other related costs, including cross-border and local transport, inpatient stay, and accommodations (Patients Beyond Borders 2018).
Medical tourism has quickly gained mainstream acceptance by Americans as well and more Americans are expected to travel internationally to obtain health care services. In 2017, for example, approximately 1,400,000 Americans traveled outside the United States for medical care (Patients Beyond Borders 2018). This is due to various reasons including the rising cost of health care in the United States (Probasco 2019); the aging American population of age 65 and older, which is estimated to reach 87 million by the year 2050 (US Census Bureau 2015); and the growing number of Americans lacking health insurance (DeMicco 2017). Other factors such as a shortage of care personnel in the health care system, long wait times for treatments, lack of doctors and specialists in the United States (Lee, Han, and Lockyer 2012), and the higher cost of treatment accompanied with low-quality care (Zolfagharian et al. 2018; Yu, Lee, and Noh 2011) also were factors for Americans to seek medical treatment abroad. Furthermore, improved standards of care and the proven safety records of health care services in developing countries also play a crucial role in motivating Americans to travel internationally to receive medical care (Zolfagharian et al. 2018).
Medical tourism involves both the “willingness to travel” and “willingness to be treated” as core processes in the new global market of health travel and captures both the health sector element and the wider economic impact of such travel (Lunt and Carrera 2011). While there is a lack of consensus among researchers regarding a unified definition of medical tourism (Bolton and Skountridaki 2017), researchers do agree that medical care and travel are the two components of medical tourism. On the other hand, other researchers argue that the vacation elements of medical tourism are merely the conduit toward securing medical care (Drinkert and Singh 2017), and it is primarily the health rather than the tourism aspect (Lovelock and Lovelock 2018). Prior research in the context of medical tourism has mainly focused on its development (Momeni et al. 2018; Chuang et al. 2014), conceptualization (Ghosh and Mandal 2018), impacts on host destinations (Snyder et al. 2013; Lunt et al. 2014), and community well-being (Suess, Baloglu, and Busser 2018). A number of studies also focused on the factors affecting the choice of medical tourism destination such as the low cost of treatment at the host destination (Zolfagharian et al. 2018), accessibility (Connell 2006), favorable currency exchange rates (Tang and Lau 2017), and service quality of medical facilities (Han and Hyun 2015). However, to the authors’ best knowledge, there has been no studies that investigated individuals’ medical tourism decision-making process from a social psychological health behavior perspective, which leaves a gap in the conceptualization and modeling of health-related behavior in medical tourism.
Health-related behavior and the guiding concepts for influencing it are complex and are often informed by more than one theory (Earp and Ennett 1991). As highlighted by Sirakaya and Woodside (2004), a single theory is likely to explain a specific aspect of decision making in a given context, but multiple theories, when used together, can better predict or explain a broader range of decision-making processes across different contexts. In this regard, the present study incorporates the health belief model (HBM) (Rosenstock 1974), and the theory of planned behavior (TPB) (Ajzen 1985) to predict factors that influence Americans’ intention to engage in medical tourism. The integration of HBM and TBP is considered in the study since both of the theories focus on understanding the behavioral intention of a person before he or she engages in the actual behavior. HBM and TBP are also recognized as two social psychological theories that are used extensively to understand a wide range of health-related behaviors (e.g., Kamran et al. 2014; Roncancio et al. 2015), which also justifies the integration of these two theories. In addition, because of the complexity posed by the involvement of health and travel related behavior in medical tourism, the integration of HBM and TPB may better predict medical tourists’ behavior from the perspectives of both the patient and the tourist. Thus, by integrating the HBM and the TPB, the current study aims to develop and test a theoretical model to examine individuals’ intention to engage in medical tourism. More specifically, this study investigates the impact of perceived benefits and perceived barriers on attitude and the influence of perceived barriers on perceived behavioral control. Furthermore, the impacts of attitude, perceived behavioral control, and subjective norm on individuals’ intention to engage in medical tourism are analyzed. Finally, the moderating role of perceived severity on the proposed relationships is examined. The findings of the current study offer valuable theoretical contributions in the context of destination marketing literature in general and medical tourism literature in particular. It is further believed that this study offers several practical implications and suggestions not only for destination marketers and decision makers but also for healthcare service providers and medical tourism facilitators in developing an effective marketing strategy by providing a better understanding of potential medical tourists’ expectations and their decision-making process.
Theoretical Foundation
Health Belief Model
The HBM introduced by Rosenstock (1974) is one of the most widely used conceptual models for understanding individuals’ health-related behaviors (Green and Murphy 2014). The HBM attempts to predict health-related behavior in terms of certain belief patterns, which specifically include two classes of variables including (1) the psychological state of readiness to take specific action and (2) the extent to which a proposed behavior is believed to be beneficial in reducing the threat (Rosenstock 1974). The psychological state of readiness is determined by individuals’ perceived threat of vulnerability or susceptibility to a health condition and the severity of that health condition. Perceived susceptibility is individuals’ beliefs about the likelihood of experiencing a condition or a disease, and perceived severity refers to the beliefs a person holds regarding the seriousness of the illness or disease (Champion and Skinner 2008; Rosenstock 1974).
According to the HBM, the acceptance of susceptibility and severity of disease alone is not enough to explain individuals’ intentions to engage in a behavior. Individuals’ behavior also depends on perceived benefits of the behavior as well as the barriers to engage in such behavior. In other words, individuals’ beliefs about the susceptibility and severity of a condition and the benefits and the barriers of the course of action available to them in reducing the susceptibility to or severity of the condition will determine if individuals will take action to reduce the threat posed by the condition (Champion and Skinner 2008).
Researchers have investigated individuals’ health-related behavior by utilizing the HBM in different settings including but not limited to mental health help-seeking behavior (e.g., O’connor et al. 2014), adherence to medications (e.g., Kamran et al. 2014), disease prevention, and early disease detection (e.g., Hajian et al. 2011; Guvenc, Akyuz, and Açikel 2011). A study conducted by Kim and Zane (2016) applied HBM to examine how perceived severity of symptoms, perceived susceptibility to mental health problems, perceived benefits of treatment, and perceived barriers to treatment influenced intentions to seek help among a sample of 395 Asian American and 261 White American students experiencing elevated levels of psychological distress. The study results indicated that Asian Americans in distress had relatively lower intentions to seek help compared with White Americans, and perceived benefits partially accounted for differences in help-seeking intentions. Perceived severity and barriers were related to help-seeking intentions in both groups. Salari and Filus (2017) used HBM to examine factors related to parental intention to participate in parenting programs. The results indicated that, for both mothers and fathers, perceived program benefits were positively associated with intention to participate in parenting programs. In addition, perceived barriers had a negative impact on intention to participate only for mothers and perceived self-efficacy had a positive impact on intention only in the sample of fathers. No significant relations were found between intention to participate and perceived child problem susceptibility and severity. In another study, Mehta, Sharma and Lee (2014) investigated factors affecting human papillomavirus (HPV) vaccine acceptance among college male students. The study results demonstrated that self-efficacy for taking the vaccine, perceived barriers, and perceived severity were significant positive predictors of vaccine acceptability (Mehta et al. 2013).
Theory of Planned Behavior
The TPB is proposed by Ajzen (1985) as an extension of the theory of reasoned action (TRA) (Fishbein and Ajzen 1975). According to TBP, individuals behave in a certain way if they think that such behavior will result in a particular outcome that they value, that their important referents will value and approve of the behavior, and that they have the required resources, abilities, and opportunities to perform such behavior (Lam and Hsu 2006; Ajzen 1985). More specifically, TBP hypothesizes that an individual’s actual execution of certain behavior is mainly a function of his or her behavioral intention, which is jointly predicted by three antecedents, including attitude about the behavior, subjective norm, and perceived behavioral control. Thus, behavioral intention is a linear regression function of attitudes, subjective norms, and perceived behavioral control (Ajzen and Fishbein 1980).
Attitude is an individual’s personal convictions and feelings toward the behavior (Ajzen and Fishbein 1980). Attitude can be defined as a favorable or unfavorable predisposition, shaped by learning and experience, which allows an individual to react in a consistent way toward a certain behavior, product, or service (Lam and Hsu 2006). According to the TBP, when a person has a positive attitude toward the behavior, then his or her intention to engage in that behavior will also be positive and vice versa. Subjective norm refers to “social pressure to perform or not to perform the behavior in question” (Ajzen 1991, p. 188). Subjective norm is considered as an individual’s perception of how the others who are most important to him or her would think of the behavior. TPB also postulates that perceived behavioral control is an important determinant of the target behavior. Perceived behavioral control refers to the perceived difficulties when carrying out a certain behavior (Ajzen 1991). According to the TPB, perceptions of having control over the external resources (e.g., knowledge, ability, time) to perform a behavior play an important role on engaging in that specific behavior.
TBP is one of the most extensively used psychological models that explains and predicts human behavior. Prior researchers have extensively used TPB to explain tourist behavior in different contexts (e.g., Lam and Hsu 2006; Quintal, Lee, and Soutar 2010; Sparks and Pan 2009). TBP has also been used in the context of health behavior in different settings such as drug use (e.g., Zemore and Ajzen 2014), alcohol consumption (e.g., Haydon, Obst, and Lewis 2018), dietary behaviors (e.g., McDermott et al. 2015), cancer screening (e.g., Roncancio et al. 2015), adherence in chronic illness (e.g., Rich et al. 2015), and exercise behavior (e.g., Gomes et al. 2018).
Hypotheses Development
As previously mentioned, this study integrates the HBM and the TPB to develop and test a theory-based model that empirically investigates the antecedents of Americans’ intention to engage in medical tourism. In this regard, this study examined the impacts of perceived benefits and perceived barriers on individuals’ attitude toward medical tourism and the impact of perceived barriers on individuals’ perceived behavioral control. In addition, the impacts of attitude, perceived behavioral control, and subjective norm on individuals’ intention to engage in medical tourism were investigated. Finally, the moderating role of perceived severity on the proposed relationships was examined. Perceived susceptibility is not included in the proposed model since the current study specifically focuses on behavioral intentions of individuals who currently have chronic conditions, a disease, an illness, or other health problems.
The Impacts of Perceived Benefits and Perceived Barriers on Attitude
In the context of HBM, perceived benefits are individuals’ beliefs regarding the benefits of an action such as the benefits of treatment in reducing the threat of a disease as well as non–health-related perceptions such as financial savings that are gained by engaging in the behavior (Champion and Skinner 2008). The benefits of medical tourism have been examined in prior medical tourism research in different settings; however, there has been a limited number of studies that have conceptualized perceived benefits as a research construct and empirically examined its impact on individuals’ attitude and behavioral intention toward medical tourism. Cost savings (Crooks et al. 2011; Hanefeld et al. 2015), access to high-quality care and services (Mason and Wright 2011), expedited and timely access to health care (Mason and Wright 2011; Turner 2007a, 2007b), and opportunity for luxurious vacation (De Arellano 2007) are identified as major factors that influence individuals’ behavior to engage in medical tourism.
The rapid growth and improvement of medical infrastructure and systems in developing countries have resulted in overall low healthcare costs. In contrast, the steadily rising healthcare costs within the developed countries such as the United States have made the medical services more attractive in developing countries (Yu and Ko 2012), which, consequently, has increased the demand for medical tourism. In this regard, the difference in healthcare costs between the home and host countries has been identified as one of the major benefits of medical tourism in prior studies (e.g., Hanefeld et al. 2015; Ramamonjiarivelo, Martin, and Martin 2015). Another important factor that motivates individuals to travel abroad for medical tourism is long wait times for certain procedures in their home country or the unavailability of those procedures in their national health care system (Heung, Kucukusta, and Song 2010). In the United States, there is developing proof that long wait times to see a doctor have become the norm in many parts of American medicine not only for those patients with private insurance, but also for those with Medicaid and Medicare. For instance, a study conducted by Merritt Hawkins, a physician staffing firm, surveyed five types of doctors’ offices in terms of wait times. The study results indicated that the waits varied greatly by market and specialty. Patients waited an average of 29 days nationally to see a dermatologist for a skin examination, 66 days to have a physical examination in Boston, and 32 days for a heart evaluation by a cardiologist in Washington, DC (Rosenthal 2014). Medical tourists can also be pulled toward destinations that have hospitals and medical facilities that are renowned for the quality of service, care, and facilities they offer (Crooks et al. 2011). In fact, a study conducted by the Medical Tourism Association (2013) indicated that medical tourists cited expertise and qualification of the doctors as the most important factor in choosing a healthcare facility. Finally, factors that motivate individuals to engage in medical tourism may be different from those for leisure tourism since medical tourists are more concerned with medical factors, whereas leisure travelers are mostly interested in destination attributes (Ye et al. 2008). On the other hand, medical tourism is a combination of medical services and the tourism industry (Yu and Ko 2012), and people travel long distances to obtain medical services while vacationing. In this regard, medical tourists may consider the opportunity of combining their desired medical service with a vacation as one of the benefits of engaging in medical tourism. In the present study, based on the aforementioned discussion, the perceived benefits construct is conceptualized as a combination of lower cost, less wait time, better quality of medical care, and the opportunity to combine medical service with a vacation.
In HBM, even if individuals believe that a behavior is effective in reducing the threat of a disease, the action may still seem expensive, inconvenient, or unpleasant to them (Rosenstock 1974). In this regard, perceived barriers play an important role on shaping individuals’ attitudes toward the behavior and their intention to engage in such behavior. Perceived barriers refer to the negative externalities of an action, which may act as impediments that are related to the undertaking of the behavior (Champion and Skinner 2008). In the context of leisure and tourism, perceived barriers (barriers and constraints are used interchangeably) are defined as constraints that prevent tourists from visiting a specific destination (Huang and Hsu 2009). Prior literature demonstrated that tourists do not travel to participate in any leisure-related activities because of intrapersonal, interpersonal, and structural constraints (Crawford and Godbey 1987). Intrapersonal constraints are individual psychological conditions and characteristics that influence individuals’ preferences such as lack of interest, anxiety, and lack of skill. Interpersonal constraints are the social interactions or relationships between individuals’ characteristics, which result from the unavailability of other people such as family members and friends. Structural constraints are associated with the external factors such as inconvenient facilities, time limitations, and lack of knowledge (Zhang et al. 2012).
In this study, perceived barriers to medical tourism are considered in the context of the aforementioned three dimensions (i.e., intrapersonal, interpersonal, and structural). Since medical tourism involves traveling to another country to receive nonemergency medical treatment with the opportunity to combine the desired medical service with a vacation, it is logical to expect that medical tourists may experience similar types of barriers as might regular tourists. For instance, as structural barriers, language, or not having enough time due to job and/or family commitments; as intrapersonal barriers, feeling anxious about engaging in medical tourism due to security and risk concerns; and as interpersonal barriers, having no travel companions and disapproval from family and friends may prevent individuals to travel to a foreign country to receive medical treatment.
Positive or negative beliefs about certain behavior and an evaluation of the outcome of that specific behavior determines one’s attitude regarding the behavior, and the belief in benefit or barrier determines expectancy about the outcome (Quine, Rutter, and Arnold 1998). In this regard, HBM’s perceived benefit and perceived barriers constructs can be considered as subjective cost and benefit analysis, which impact the attitude component of TBP (Quine, Rutter, and Arnold 1998). Prior tourism research has confirmed that attitudes are closely associated with potential tourists’ beliefs and perceptions about the benefits and the barriers (F. Wang, Deng, and Petrick 2018; Lam and Hsu 2006). In the context of medical tourism, similar relationships can be expected. Therefore, while the higher level of perceived benefits may increase individuals’ favorable attitude toward medical tourism, the higher level of perceived barriers may cause individuals to form negative attitudes toward medical tourism. Hence, based on the aforementioned discussion, the following hypotheses are proposed:
Hypothesis 1: Perceived benefits of engaging in medical tourism is positively associated with individuals’ attitude toward medical tourism.
Hypothesis 2: Perceived barriers of engaging in medical tourism is negatively associated with individuals’ attitude toward medical tourism.
The Impact of Perceived Barriers on Perceived Behavioral Control
As previously mentioned, perceived behavioral control (PBC) refers to the perceived difficulties and control when performing a specific behavior. PBC was included in the original theory of reasoned action in an effort to assess perceived barriers and constraints that limit individuals’ ability to execute a behavior. More specifically, the inclusion of PBC as an antecedent of behavioral intention in the TPB was in response to criticisms that the theory of reason action was based on the assumption of perfect volitional control over behavior and thus failed to consider perceived constraints that restrict individuals’ ability to perform a desired action (Alexandris and Stodolska 2004; Dawson et al. 2001).
According to Ajzen and Driver (1992), PBC is positively associated with the amount of resources an individual believes that he or she possesses and is negatively related with the number of barriers that he or she perceives to experience. Prior studies that utilized TPB demonstrated that perceptions of having control over the external resources and barriers to perform a behavior play an important role on engaging in that specific behavior (Lee, Han, and Lockyer 2012; M. F. Chen and Tung 2014). However, it is important to note that PBC is operationalized in a more generic way, and it is a broader concept than perceived barriers since PBC not only influences the intentions but also affects actual behavior (Alexandris and Stodolska 2004). Therefore, relating PBC with only external enabling or hindering aspects, as proposed by previous TBP studies, may not be sufficient to understand the actual barrier or constraint factors that prevent individuals to engage in the behavior; thus, a better understanding of the concept PBC is required by examining its antecedents. This issue may be particularly crucial in medical tourism settings since various barriers exist that may limit potential medial tourists’ control over their behavior. For example, lack of knowledge, time constraints, or lack of a travel companion may influence individuals’ perceived behavioral control toward medical tourism since these factors are not under the individuals’ control. Therefore, we examined perceived barriers as the antecedent of PBC. Based on the discussion provided above, the following hypothesis is proposed:
Hypothesis 3: Perceived barriers of engaging in medical tourism is negatively associated with individuals’ perceived behavioral control.
The Impacts of Attitude, Subjective Norm, and Perceived Behavioral Control on Behavioral Intention
According to TBP, when individuals have a more positive attitude toward the behavior, have a high level of perceived behavioral control, and have positive subjective norms, then their intention to engage in that behavior will also be positive and vice versa. As previously mentioned, numerous empirical studies have investigated the relationships between the three TPB constructs and travel intentions in tourism contexts (Choo et al. 2016; Park, Hsieh, and Lee 2017; Duarte Alonso, Sakellarios, and Pritchard 2015). In the context of medical tourism, similar relationships can be expected. For instance, if individuals have favorable attitudes toward medical tourism and believe that the outcome of the medical tourism activity will be satisfactory, they may have positive behavioral intention to engage in medical tourism. In the same vein, others’ (i.e., friends and family) opinions may play an important role on individuals’ intention to participate in medical tourism since participating in medical tourism is a serious health-related decision. More specifically, individuals who consider engaging in medical tourism may expect that people who are important to them (i.e., friends and family) would approve of their behavior. Finally, having required resources, knowledge, and ability to engage in medical tourism play an important role on individuals’ behavioral intentions. For instance, although an individual has a positive attitude toward medical tourism, if he or she does not have control over the resources (e.g., financial resources, time), knowledge (e.g., information about medical tourism), and ability (e.g., access, overall health condition) for traveling abroad to receive medical treatment, then his or her intention to engage in medical tourism will be lower.
Even though TPB has not been extensively utilized in the context of medical tourism, the positive impacts of attitude, subjective norm, and perceived behavioral control on behavioral intention to engage in medical tourism have been confirmed through a few prior studies. One study conducted by Martin, Ramamonjiarivelo, and Martin (2011) demonstrated that all three TPB constructs significantly influenced individuals’ behavioral intention to engage in medical tourism, with attitude being the strongest predictor followed by subjective norm, and perceived behavioral control, respectively. Another study conducted by Lee, Han, and Lockyer (2012) demonstrated that attitude, subjective norm, and perceived behavioral control positively influenced Japanese tourists’ intention to travel to Korea to receive medical treatment. Therefore, based on the discussion provided above, the following hypotheses are proposed:
Hypothesis 4: Attitude toward medical tourism is positively associated with intention to engage in medical tourism.
Hypothesis 5: Perceived behavioral control about medical tourism is positively associated with intention to engage in medical tourism.
Hypothesis 6: Subjective norm about medical tourism is positively associated with intention to engage in medical tourism.
Perceived Severity
In healthcare literature, the utilization of health services is identified as a complex phenomenon, which is dependent upon many factors (e.g., availability, cost, and health beliefs of individuals), and perceived severity is found to be an important factor in explaining utilization of health services (Chakraborty et al. 2003). In the context of HBM, perceived severity refers to the beliefs a person holds regarding the seriousness of illness or disease (Champion and Skinner 2008; Rosenstock 1974). According to the HBM, seeking medical care is positively associated with perceived severity of illness, and this relationship has been confirmed in prior literature in different settings (Cerkoney and Hart 1980; Turkington, Dempster, and Maguire 2018; King 1982).
Even though it has not been investigated in the context of HBM, the positive impact of perceived severity of a health condition is found to be positively associated with individuals’ behavioral intention to engage in medical tourism. For instance, a study conducted by Reddy, York, and Brannon (2010) investigated factors influencing Americans’ intentions to travel abroad for medical treatment and found that the nature and severity of the health condition played an important role in individuals’ decision to consider medical tourism. In addition to the direct relationships between perceived severity and behavioral intention, perceived severity may also play a moderating role on the proposed relationships in this study. To the authors’ best knowledge, the moderating role of perceived severity has not been investigated in prior literature. However, it can be expected that the impacts of perceived benefits and perceived barriers on attitude and the impacts of attitude, perceived behavioral control, and subjective norm on individuals’ intention to engage in medical tourism may differ based on individuals’ perceptions about the severity of illnesses or health conditions. Hence the following hypothesis is proposed:
Hypothesis 7: Perceived severity of the disease or the condition positively moderates the relationship between perceived benefits and attitude (hypothesis 7a), perceived barriers and attitude (hypothesis 7b), perceived barriers and perceived behavioral control (hypothesis 7c), attitude and intention to engage in medical tourism (hypothesis 7d), perceived behavioral control and intention to engage in medical tourism (hypothesis 7e), and subjective norm and intention to engage in medical tourism (hypothesis 7f).
The conceptual framework in Figure 1 concisely illustrates Hypotheses 1–7f.
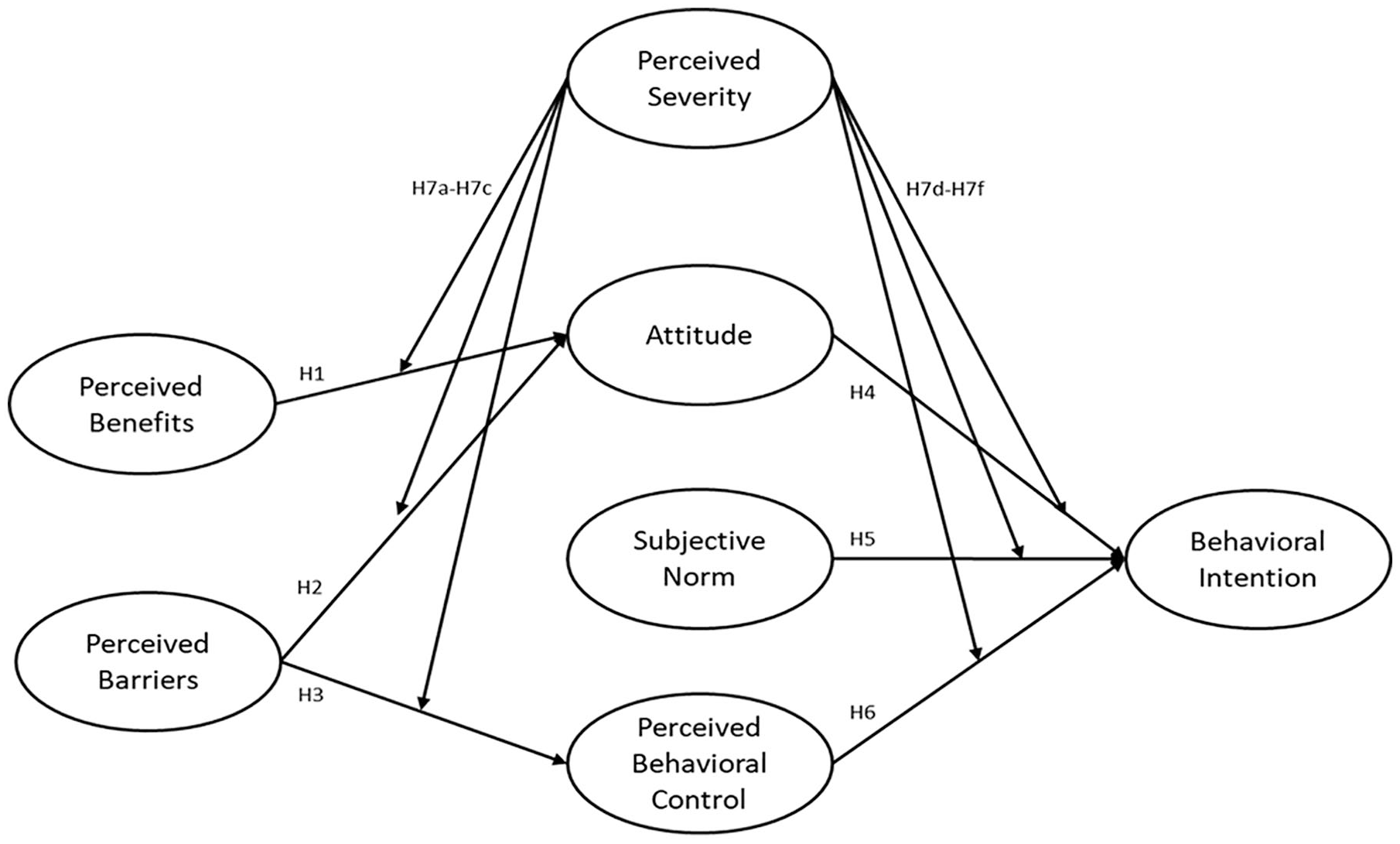
Research model.
Methodology
Survey Instrument
All of the study scales except perceived benefits were adapted from prior research. More specifically, perceived barriers was measured using a total of 12 items adapted from Nyaupane, Morais, and Graefe (2004), Nyaupane and Andreck (2008), and Fleischer and Pizam (2002). Attitude was measured using a three-item scale measure adapted from Ajzen and Fishbein (1980) and Ajzen (1991). Subjective norm was adapted from Venkatesh et al. (2003) and measured with three items. Perceived behavioral control was measured with three items adapted from Wu and Chen (2005), and behavioral intention was adapted from Davis, Bagozzi, and Warshaw (1992) and measured with three items. Perceived benefits scale was developed by the researchers based on prior medical tourism literature. All of the survey items were measured on a five-point Likert-type scale ranging from 1 = strongly disagree to 5 = strongly agree. Perceived severity was measured with one question asking the respondents to indicate the severity level of the health condition (i.e., the primary condition that affects them the most) that they have. A five-point scale was used to measure perceived severity (i.e., 1 = not severe, 2 = mild, 3 = moderately severe, 4 = severe, and 5 = very severe). A pilot test was conducted to evaluate the clarity and comprehensiveness of the questionnaire. Thirty questionnaires were distributed to graduate students and faculty members. After the pilot test and informal discussions with faculty members, some modifications were made, and the scales were slightly revised to reflect the context of the study.
Sampling and Data Collection
The target population of this study was American adults who currently have a chronic condition, disease, illness, or health problem that requires medical care, who are aware of the possibility of getting medical treatment in a foreign country, and who are interested in traveling to a foreign country to receive medical treatment for the health condition that they currently have. A web-based self-administered questionnaire was utilized to collect the empirical data of the study. An online panel survey company (i.e., Qualtrics) was hired for the data collection procedure. The link of the survey was provided to the marketing company, and the marketing company distributed the survey to randomly selected panel members. Online panel survey technique has many advantages such as reducing social desirability bias and increasing access to a larger population (Hung and Law 2011). In addition, online panel surveys have been seen to be appropriate when rapid responses are required and when hard-to-find quota sampling is needed (Lugtiga, Dasb, and Scherpenzeela 2014). Furthermore, response rates and the quality of responses are significantly high in general in panel surveys since the survey takers are offered a financial reward in return for participating in the survey (Lugtiga, Dasb, and Scherpenzeela 2014).
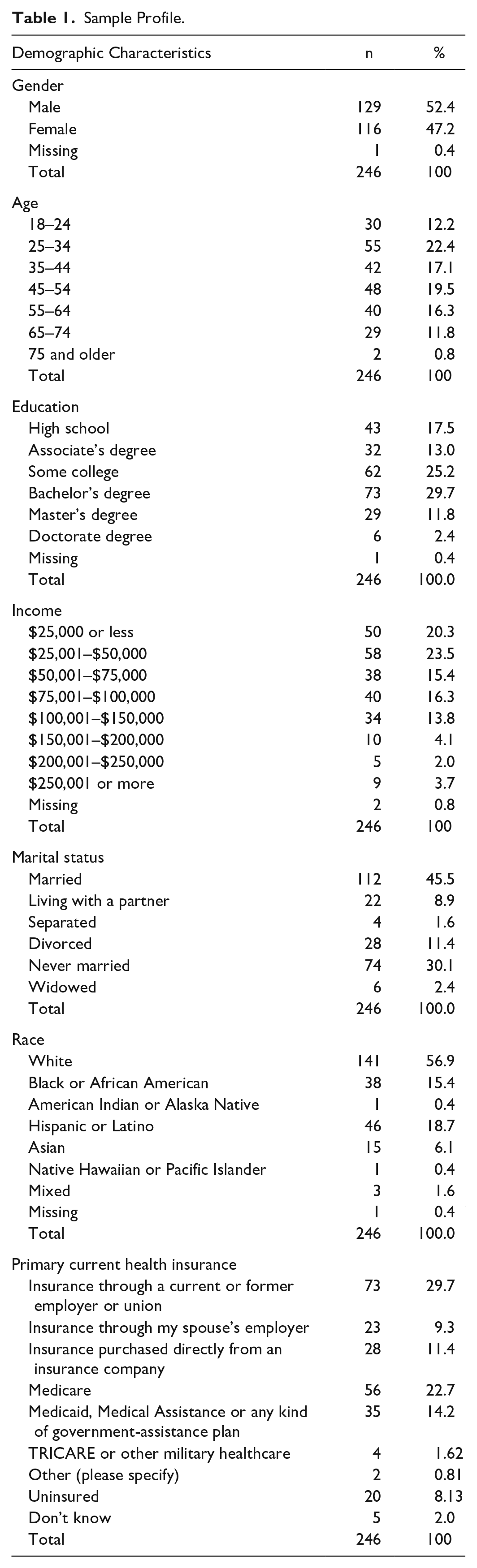
Three screening questions (i.e., Are you aware of the possibility of getting medical treatment in a foreign country? Do you currently have any chronic condition, disease, illnesses, or health problem that requires medical care? and Are you interested in traveling to a foreign country to receive medical care for the chronic condition, disease, illness, or health problem that you currently have?) were used to ensure that only respondents who are qualified to be part of the sample of the study participated in the survey. The web-based survey was conducted in July 2018. A total of 246 responses were gathered. The key demographics (see Table 1 for the full sample profile) indicated that nearly 52% of the respondents were male, and 36% of the participants were between the ages of 35 and 54 years. Approximately 30% of the participants had earned a bachelor’s degree, and around 24% of participants had a household income of $25,001–$50,000. Forty-six percent of the participants were married, and a majority (57%) of the participants declared their ethnicity as white. Around 30% of the participants had insurance through their former or current employer, 23% of the respondents had Medicare, and 8% of the respondents were uninsured.
Sample Profile.
Data Analysis
Prior to data analyses, the data were checked for normality. Variables showed normal distribution based on a visual inspection of histograms and box plots. All of the skewness and kurtosis values were within the acceptable range of ±2 (George and Mallery 2010). The multicollinearity check showed that tolerance values were above 0.2 for all of the constructs, indicating that there were no multicollinearity issues. In the first step of data analysis, an exploratory factor analysis (EFA) was conducted to identify underlying dimensions associated with perceived barriers and perceived benefits. As the second step, a first-order confirmatory factor analysis (CFA) was performed to evaluate the overall measurement model. Factors derived from the EFA and the TBP constructs (i.e., attitude, perceived behavioral control, subjective norm) were included in the CFA. The perceived barriers construct was conceptualized as a second-order construct (C. C. Chen and Patrick 2016; Wang, Deng, and Petrick 2018). Therefore, a second-order CFA was performed by conceptualizing perceived barriers as a second-order construct. To test the proposed theoretical model and the study hypotheses, a structural equation modeling (SEM) was used.
Finally, to examine the moderating effect of severity on the structural model, a multigroup moderation test (pairwise comparison) was conducted using AMOS. Multiple-group comparison involves splitting the data set into groups based on a categorical variable and estimating separate models for each group. More specifically, the use of multigroup comparisons is to determine if relationships hypothesized in a model will differ based on the value of the moderator. A multigroup moderation was utilized to analyze how the proposed relationships among the constructs vary across the three severity groups including low (n= 43), moderate (n=83), and high severity (n=120).
Results
Exploratory Factor Analysis
An exploratory factor analysis was conducted to identify the underlying dimensions of the perceived barriers and perceived benefits constructs. Principal axis factoring with varimax rotation was applied as the extraction method. The Kaiser-Meyer-Olkin test, which evaluates the measure of sample adequacy (MSA), was above the 0.5 minimally accepted level (MSA = 0.874), and the overall significance of the correlation matrix was less than α = 0.001, with a Bartlett test of sphericity value of 1991.240. Items with factor loadings equal to or greater than 0.5 were retained in the data analysis. In addition, variables that had eigenvalues equal to or above 1 were evaluated as significant. One intrapersonal item (i.e., my overall health condition is a concern for traveling to a foreign country to receive medical treatment), and one structural barrier item (i.e., language would be a major problem for me to travel to a foreign country to receive medical treatment) were removed from the data analysis since they had factor loadings less than 0.5. The results of the EFA yielded a four-factor model, explaining 73% of the variance. The first factor (interpersonal barriers) explained 40.3% of the variance, the second factor (intrapersonal barriers) explained 15.9% of the variance, the third factor (structural barriers) explained 10.1% of the variance, and the fourth factor (perceived benefits) explained 7.2% of the variance. To evaluate the reliability of the measurement scales, Cronbach’s alpha was utilized. The scales’ alpha coefficient values ranged from 0.71 to 0.93. Based on the recommended benchmark value (i.e., 0.70), the scales are considered reliable and can be used for further analysis (Nunnally 1970).
Measurement Model
The overall first-order measurement model was initially evaluated before the second-order measurement model and testing the structural model. Constructs derived from the EFA (i.e., interpersonal, intrapersonal, and structural barriers, and perceived benefits) and the TBP constructs, namely, subjective norm, perceived behavioral control, attitude, and behavioral intention were included in CFA analysis. The results demonstrated an acceptable model fit with a significant chi-square statistic (chi-square = 432.393, df = 271) and with other fit indices including root mean square error of approximation (RMSEA = 0.049), goodness-of-fit index (GFI = 0.90), comparative fit index (CFI = 0.96), normed fit index (NFI = 0.91), and incremental fit index (IFI = 0.96) (Hair et al. 1998). Composite reliability (CR) was used to examine the reliability of the measurement scales. The CR values of all dimensions were higher than the suggested value of 0.8, providing evidence for reliability (Nunnally 1970; Fornell and Larcker 1981) (Table 2).
Measurement Model Results.
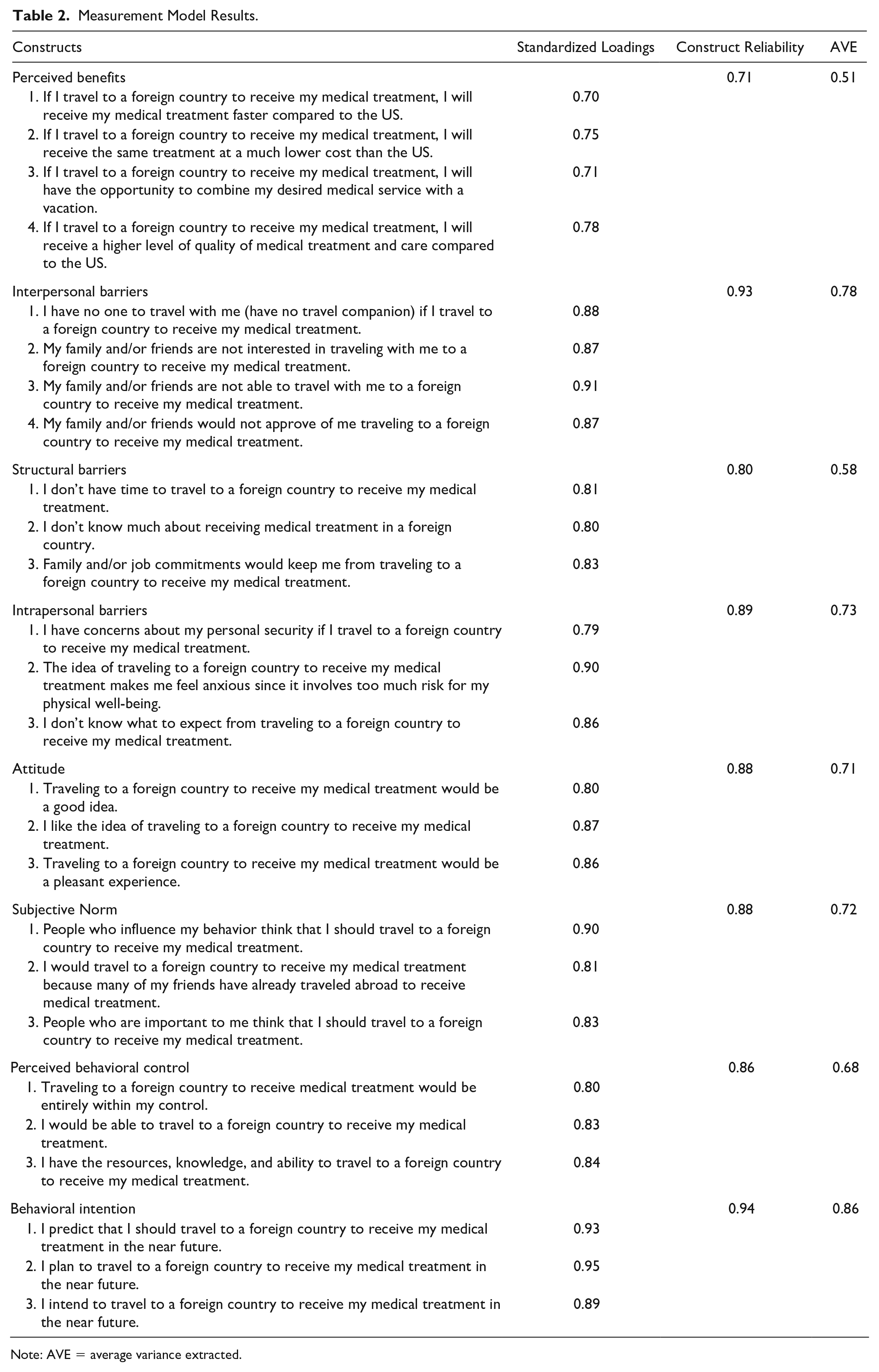
Note: AVE = average variance extracted.
Average variance extracted (AVE) values were analyzed to evaluate the convergent validity. As presented in Table 3, the AVE values for all eight factors were above the suggested value of 0.5, thus indicating good convergent validity (Fornell and Larcker 1981). The comparison of square roots of AVEs with the correlation between variables was utilized to assess the discriminant validity. The results demonstrated that the square roots of AVE values were more than the correlations between two factors, thus confirming a satisfactory discriminant validity.
Discriminant Validity Matrix.
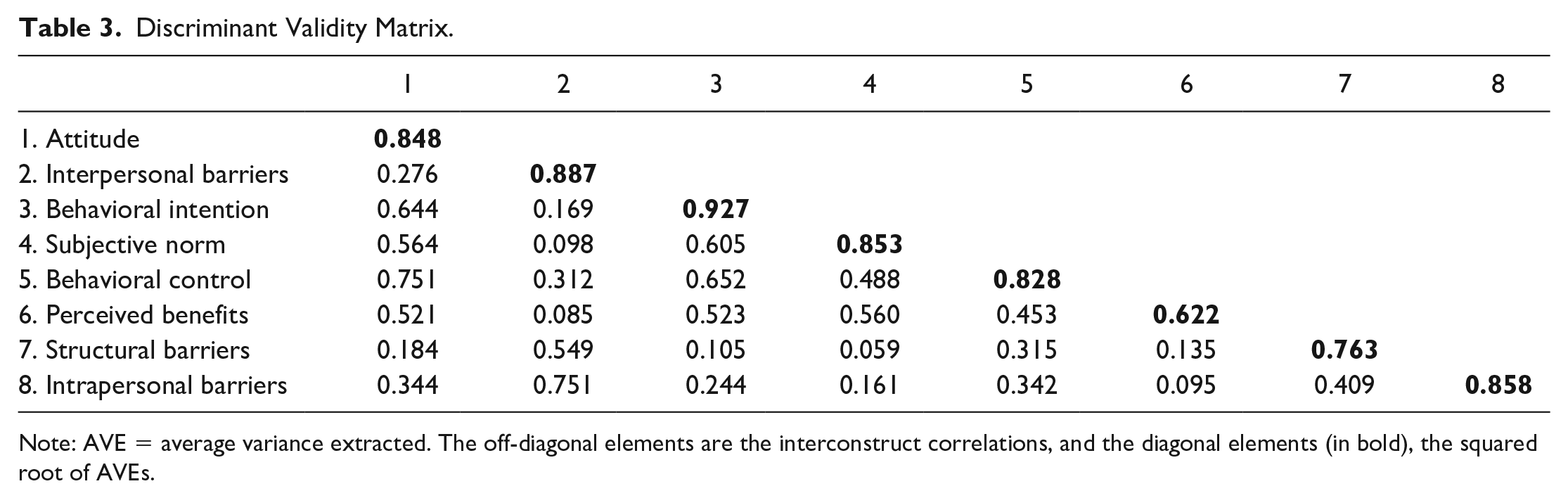
Note: AVE = average variance extracted. The off-diagonal elements are the interconstruct correlations, and the diagonal elements (in bold), the squared root of AVEs.
In terms of second-order factor analysis, the results indicated a good model fit as well with a significant chi-square statistic (chi-square = 460.740, df = 281) and with other fit indices (RMSEA = 0.051, GFI = 0.90, CFI = 0.96, NFI = 0.90, and IFI = 0.96). The second-order measurement model also demonstrated good convergent and discriminant validity (Table 4). Based on the standardized factor loadings, it can be stated that interpersonal barriers had the highest impact on developing perceived barriers construct followed by intrapersonal barriers and structural barriers (Table 4).
Second-Order Measurement Model Results.
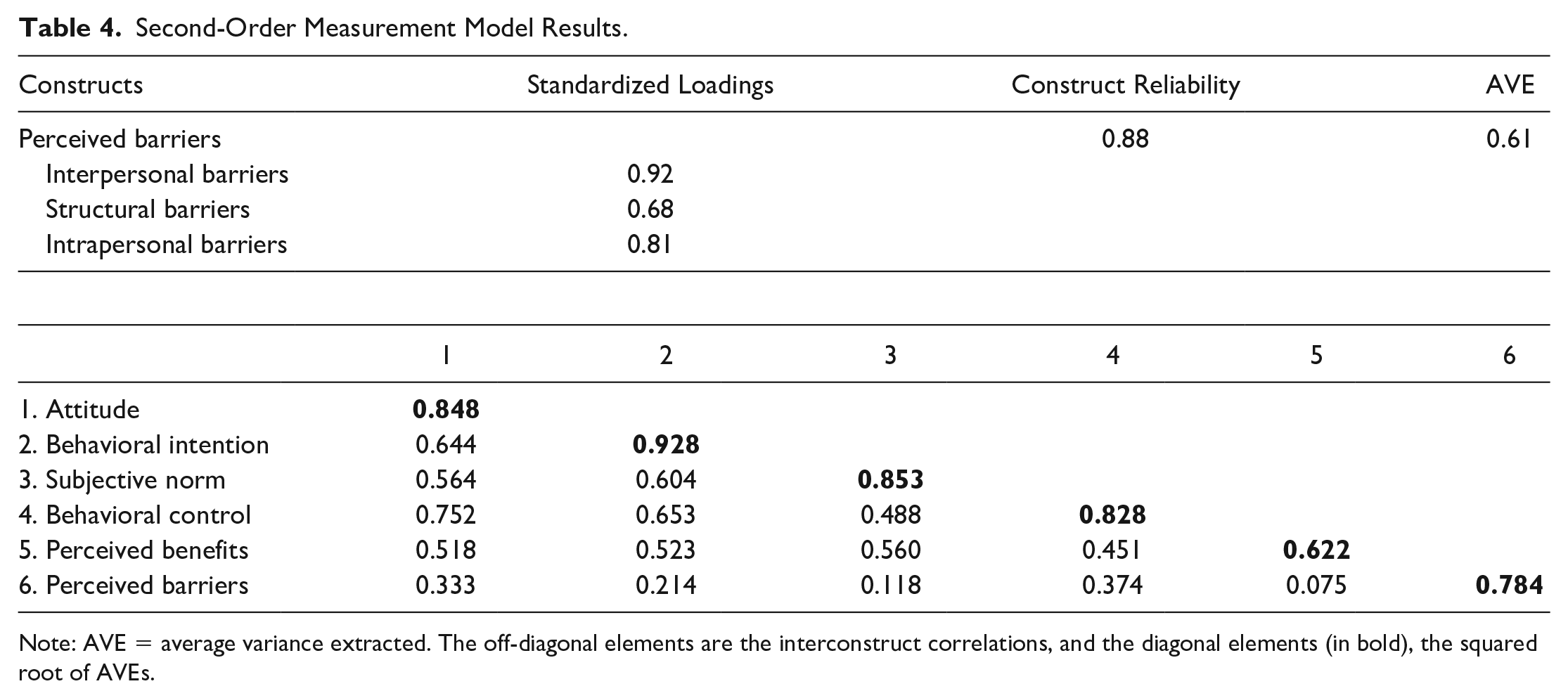
Note: AVE = average variance extracted. The off-diagonal elements are the interconstruct correlations, and the diagonal elements (in bold), the squared root of AVEs.
Structural Model Analysis
SEM analysis was conducted to test the study hypotheses. The results indicated a good model fit. The chi-square to degrees-of-freedom ratio was equal to 2.1, which fell below the cut-off point of 3. Other fit indices were all acceptable values (RMSEA = 0.067, GFI = 0.90, CFI = 0.92, NFI = 0.90, and IFI = 0.93) (Hair et al. 1998). The results indicated that hypotheses 1 to 6 were supported in their proposed directions (Figure 2, Table 5). More specifically, the study results indicated that perceived benefits had a positive (hypothesis 1), and perceived barriers a negative (hypothesis 2), impact on attitude; perceived barriers had a negative impact on perceived behavioral control (hypothesis 3); attitude (hypothesis 4), behavioral control (hypothesis 5), and subjective norm (hypothesis 6) positively influenced behavioral intention. In addition, the variance explained was 48% for attitude, 27% for perceived behavioral control, and 47% for intention to engage in medical tourism.

Results for structural modeling analysis.
Hypotheses Test Results (Moderation Hypotheses Are Excluded).

***p < 0.01; **p < 0.05; *p < 0.10.
In terms of the moderating role of perceived severity, the results demonstrated a significant moderating effect of perceived severity on the relationships between perceived benefits and attitude (hypothesis 7a), perceived barriers and attitude (hypothesis 7b), and attitude, and behavioral intention (hypothesis 7d), indicating a partial support for hypothesis 7. More specifically, the results indicated that the positive impact of perceived benefits on attitude was stronger for the high-severity group than it was for the low severity group; the negative impact of perceived barriers on attitude was stronger for the high-severity group than it was for the low-severity group, and the positive impact of attitude on behavioral intention was stronger for the high-severity group than it was for the low-severity group (Table 6).
The Moderating Effect of Perceived Severity.
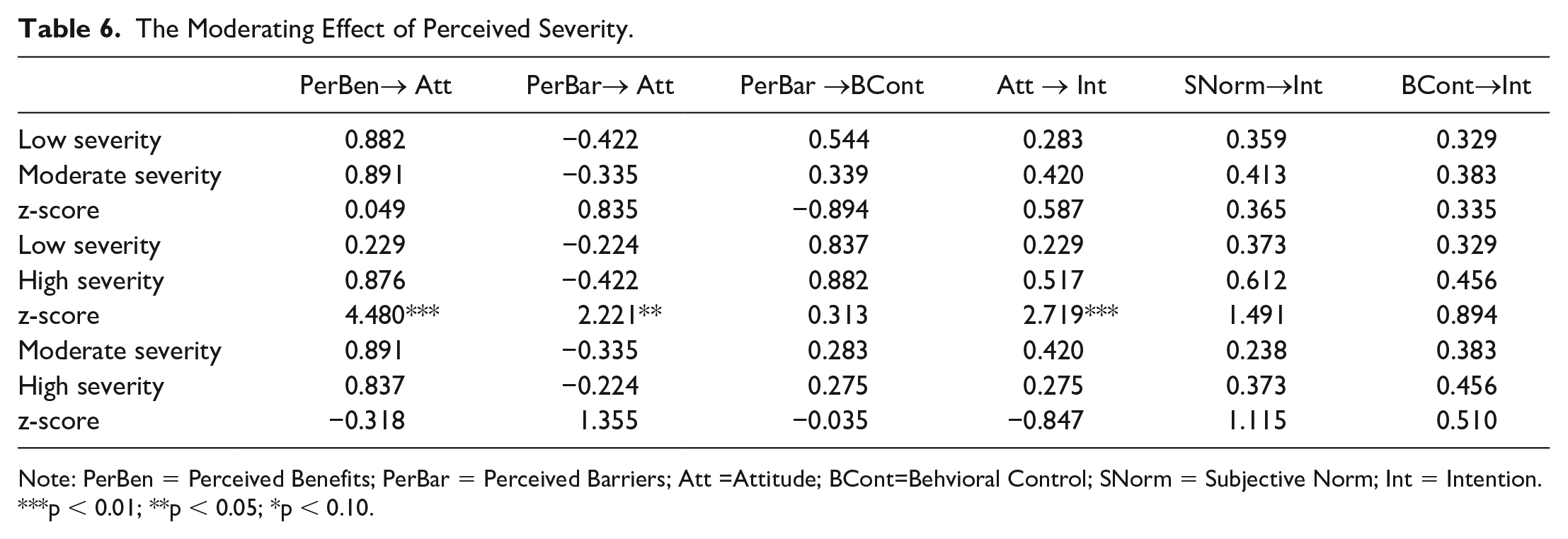
Note: PerBen = Perceived Benefits; PerBar = Perceived Barriers; Att =Attitude; BCont=Behvioral Control; SNorm = Subjective Norm; Int = Intention.
p < 0.01; **p < 0.05; *p < 0.10.
Discussion and Conclusions
By incorporating HBM and the TPB, this study developed and tested a theoretical model to examine individuals’ intention to engage in medical tourism. The study results related to hypotheses 1 and 2 indicated that perceived benefits was positively, and perceived barriers negatively, associated with individuals’ attitude toward medical tourism. Consistent with prior studies (Reference), these results demonstrate that both barriers and benefits constructs are important factors in forming individuals’ opinions about medical tourism. However, prior studies generated inconsistent findings in terms of the strength of the impact barriers and benefits on individuals’ attitude and behavioral intention (e.g., Wang, Deng, and Petrick 2018). The present study findings illustrated that perceived benefits (hypothesis 2: Beta = 0.557) had a stronger impact on attitude than did perceived barriers (hypothesis 1: Beta = -0.350). This result suggests that perceived benefits is a more critical factor than is perceived barriers in terms of individuals’ attitudes toward medical tourism.
With respect to hypothesis 3, the study results revealed that perceived barriers was negatively related to perceived behavioral control (hypothesis 3: Beta = −0.449). Prior studies confirmed the negative effect of perceived barriers on travel behavior (e.g., Wang, Deng, and Petrick 2018). This study further identified a significant explanation of the negative effects of barriers on behavioral control suggesting that individuals with high barriers tend to believe that traveling to a foreign country to receive medical treatment is not entirely within their control. In regard to hypothesis 4, attitude was found to be significantly associated with individuals’ intention to engage in medical tourism (hypothesis 4: Beta = 0.281). This result supports previous medical tourism studies (Martin, Ramamonjiarivelo, and Martin 2011) indicating that attitude is a positive predictor of intention. More specifically, the results suggest that positive attitudes held by individuals will have a positive influence on their intention to engage in medical tourism. The research findings related to hypothesis 5 indicated that subjective norm was a significant predictor of behavioral intention (hypothesis 5: Beta = 0.27). In accordance with the findings of previous studies (Lee, Han, and Lockyer 2012), the results illustrate that individuals who are interested in medical tourism are affected by others’ thoughts and tend to behave in accordance with others’ expectations. In terms of hypothesis 6, the study results further revealed that perceived behavioral control was positively associated with individuals’ intention to engage in medical tourism (hypothesis 6: Beta = 0.34). In fact, perceived behavioral control had the strongest impact on behavioral intention followed by attitude and subjective norm. These results indicate that if individuals believe that they do not have the necessary resources and knowledge regarding medical tourism and if they believe that traveling to a foreign country to receive medical treatment is not entirely within their control, then they tend not to engage in medical tourism. These findings were inconsistent with other medical tourism studies (Martin, Ramamonjiarivelo, and Martin 2011; Lee, Han, and Lockyer 2012), which failed to find significant relationships between behavioral control and intention. Finally, study findings revealed that hypothesis 7 was partially supported indicating that perceived severity moderates the relationships between perceived benefits and attitude, perceived barriers and attitude, and attitude and behavioral intention. The findings suggest that perceived benefits and perceived barriers had a stronger impact on attitude, and attitude had a stronger impact on behavioral intention for individuals who believe that the severity level of their disease is high than it did for those who believe that it is low.
Theoretical Implications
The results of this study provide several theoretical contributions in the context of destination marketing literature in general and for medical tourism literature in particular. As previously mentioned, this study incorporated the HBM and the TPB to examine individuals’ intention to engage in medical tourism. Instead of linking perceived benefits and barriers directly to behavioral intention, we examined their association with the components of the TPB. To the authors’ best knowledge, this is the first study that contextualized and incorporated the HBM and the TPB in a predictive model, which provides a comprehensive theoretical foundation that illuminates how individuals’ behavioral intentions toward medical tourism form. The study model explained 47% of the variance in individuals’ intention to engage in medical tourism confirming that integrating the HBM and the TPB is appropriate for medical tourism research.
As mentioned before, perceived barriers have not been previously investigated to understand individuals’ attitude and behavioral intention in the context of medical tourism. The findings of this study indicated that perceived barriers was a significant predictor of attitude. Therefore, this research demonstrated the applicability of barriers in medical tourism indicating that it is an important and valid concept in medical tourism research. In addition, perceived barriers predicted a significant and relatively high proportion of the PBC construct (27%), and the PBC had the strongest impact on behavioral intention followed with attitudinal and normative components of TPB, respectively. As previously mentioned, PBC was added to the original theory of reasoned action in an effort to consider perceived barriers and constraints that restrict individuals’ attitude to perform a desired behavior. The study results demonstrated that linking PBC with only external facilitating or hindering factors, as proposed by previous TBP studies, may not be adequate to understand the actual barrier or constraint factors that prevent individuals to engage in the behavior. Therefore, it is believed that the present study findings demonstrate that integrating perceived barriers in TBP could contribute to a better understanding of the concept of PBC and its antecedents.
Finally, this study is also one of the first studies that incorporated and empirically tested the severity of disease as a moderating construct in a medical tourism context. As previously mentioned, prior studies have confirmed the applicability and importance of the severity of illness in health-related decision making in different contexts (Conner and Norman 2005; Janz and Becker 1984; Weinstein 2000). The findings of this study demonstrated that the applicability of the severity of illness is extended as a moderator construct that interacts with the antecedent factors that affect individuals’ intention to engage in medical tourism.
Managerial Implications
While providing valuable theoretical contributions, the findings of the study also deliver several practical implications not only for destination marketers and decision makers but also for healthcare facilities and medical tourism service providers such as medical tourism travel agencies. By identifying factors affecting individuals’ medical tourism engagement, various parties in the medical tourism industry can develop and implement a more comprehensive and effective marketing strategy to encourage a more favorable perception of medical tourism for potential tourists. For instance, the study results suggest that medical tourism facilitators should increase potential tourists’ understanding of the benefits of medical tourism. In this regard, medical tourism facilitators in host countries should publicize the availability of equal or a higher level of quality medical care in their countries. Information about the specific facilities including but not limited to excellent service records, reputations, specializations, and accreditations should be disseminated through different channels including social media and digital marketing. In addition, potential medical tourists should be informed about the lower cost and shorter waiting time (compared with that of the United States) for the medical procedures. More specifically, educational sessions or seminars should be organized to inform and educate potential medical tourists on the availability of sound medical treatments, the lower cost, less wait time, and quality of medical tourism services available in host countries. In addition, although individuals engage in medical tourism primarily because of their health conditions, this study suggests that a vacation is an important side benefit of medical tourism. Therefore, potential medical tourists should also be informed and educated about the availability and ability to vacation while visiting the host country for medical treatment.
The study results revealed that perceived barriers was negatively associated with attitude and PBC, and PBC had a negative impact on individuals’ intention to engage in medical tourism. These results suggest that efforts should be made to assist potential medical tourists in negotiating the barriers that prevent them from engaging in medical tourism. For instance, in terms of intrapersonal barriers, strategies of reducing perceived risk, security concerns and anxiety may boost the confidence level of potential tourists to travel to a foreign country to receive medical treatment. Medical tourism facilitators should work with healthcare providers in the United States to ensure that the tourists are able to receive postoperative care to treat possible side effects and postoperative complications after they return to their home country. In addition, local government and law enforcement organizations in host countries should work with medical tourism service facilitators to provide a safe and secure environment for medical tourists during their medical treatment. To reduce the structural barriers, medical tourism facilitators should educate and inform potential tourists about medical tourism with consistent and accurate information. In addition, employers and insurance companies should develop policies (e.g., paid leave) that provide individuals with a sufficient amount of time to travel to a foreign country to receive medical treatment. In order to reduce the negative impact of interpersonal barriers, medical tourism facilitators should communicate promotional activities (e.g., discounted airfare and accommodation, promoting the tourism attractions in the host countries) to increase awareness and create interest among the family members and friends of the potential medical tourists. Recognizing the role of subjective norm in potential medical tourists’ decision making, it is crucial for medical tourism facilitators to adopt an inclusive marketing strategy that targets not only potential medical tourists but also the people around them, including their relatives and friends. For this purpose, informative and promotional materials should be sent to the relatives and friends of the potential tourists to increase their knowledge and create a positive perception about medical tourism so that they can be involved in the decision-making process. Finally, the current study findings indicated that Americans show strong intention to engage in medical tourism for treatment related to various health conditions, and the severity level of these conditions have a moderating role on the relationships between perceived benefits, attitude, and behavioral intention. Therefore, customized marketing strategies with highlights on availability of treatments and specialists are required to target this specific market of individuals with health conditions and who believes that their condition is severe. In conclusion, understanding factors that influence individuals’ intention to engage in medical tourism is crucial for effective destination management, especially for destinations that are trying to position themselves as a medical tourism destination. In this context, the findings of this study deliver a better understanding of potential medical tourists’ expectations and their decision-making process. Equipped with this information, medical service providers and destination decision makers will be able to create effective marketing strategies to attract more customers through product differentiation, thereby creating a continual, competitive advantage.
Limitations and Future Research
The current study offers several theoretical contributions and practical implications in the context of medical tourism. However, this study is subject to several limitations, and future research is required to validate the findings of the study. The data of the study were collected from US residents only. Future research that collects data from other countries may offer valuable information for comparing cultural differences in medical tourists’ behavioral intentions. This was a perception-based study, where the data were collected from individuals who were interested in engaging in medical tourism. Data collected from actual medical tourists who had prior experience in traveling abroad to receive medical treatment may produce more valid findings. A nonprobability sampling technique, namely, convenience sampling, was used to select the sample from the population. The respondents self-reported their health condition by indicating if they had a chronic condition, disease, or other health problem at the time they participated in the survey. This limits the generalizability of the findings of the study to the general population. Future studies that use probability sampling techniques with some form of random selection would provide more generalizable findings.
Even though integration of HBM and TPB was successful in predicting Americans’ intention to engage in medical tourism, future research may use different theoretical frameworks to investigate the impact of other antecedents on individuals’ intention to engage in medical tourism. For example, future studies that investigate the impact of other factors such as availability and the cost of US health insurance, wait time in the United States getting treated without traveling, perceived risk and perceived cost of traveling abroad for receiving a medical treatment, and perceived value on behavioral intention would provide a deeper understanding of how individuals’ medical tourism decision forms. In addition, this study did not consider respondents’ individual differences or past experiences. In this regard, follow-up studies that examine individuals’ behavioral intentions based on their individual difference characteristics such as individuals’ health insurance coverage plans, frequency of traveling to a foreign country, past medical tourism experience, and demographic characteristics including age, gender, marital status, education level, income, and race may provide further insights. Finally, this study did not examine if participants’ behavioral intentions vary based on the type of the health condition or disease they had. Individuals’ intention to travel to a foreign country to receive medical treatment may differ based on health condition or disease-related factors such as the availability of treatment in the United States, potential delay in getting treatment, and expected out-of-pocket expense for the treatment in the United States vs. abroad. Therefore, future studies that consider the above-mentioned factors may provide different findings.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.