
Abstract
Tourism contributes to mental health. We could: recognize, measure, value, and market those contributions; analyze components and design products to maximize mental health benefits; and use mental health benefits in tourism industry marketing and lobbying. If we measure benefits to health-research standards, then tourism could also gain commercial opportunities within the health sector. Currently, there are widely differing bodies of evidence within different tourism subsectors, reflecting historical research emphases. Music, museums, and shopping malls have been identified as therapeutic for some. Nature tourism therapies have been tested extensively, with a higher standard of evidence. Adventure tourism has been analyzed principally from a phenomenological perspective, indicating powerful psychological effects. Many mental health therapies require continuing behavioral change. Tourism research could contribute to these therapies, since it includes detailed data on the effects of program design and guiding, and individual personalities, interests, capabilities, motivations, experiences, emotions, and satisfaction.
Introduction
Recent research interest in tourism and mental health arises from a straightforward and fundamental premise: people pay for enjoyment. When tourists spend money and time on holiday travel, they expect to enjoy themselves. Enjoyment promotes wellbeing (Pyke et al. 2016; Smith and Diekmann 2017); wellbeing contributes to mental health (Yu, Smale, and Xiao 2021); and health has a substantial economic value. Historically, most tourism economics research has examined how discretionary spending by tourists generates financial inputs into travel, accommodation, and tourism activity products, enterprises, and destinations. The mental health perspective adds another financial element. Leisure tourists are investing in their own mental health, and this generates an independent set of economic contributions, through reduced healthcare costs, improved workplace productivity, and changes in social behaviors. There are also differences in geography and timing. Tourist spending contributes economically at destinations, as well as origins and en route; and principally, before and during the holiday concerned. Mental health gains, in contrast, generate contributions at tourist places of origin, and largely after holidays are over.
Tourism and health research and practice have complementary disciplinary emphases. Tourism research analyzes details of program and product design and setting, markets and marketing, including individual motivations, expectations, experiences, and satisfaction, because these are needed for profitability. It has not, historically at least, analyzed or compared clients’ mental health outcomes, because those have not been seen as relevant. From a tourism research perspective, a mental health lens can yield new insights and opportunities. Health research, in contrast, does focus principally on outcomes, with less emphasis on the details of program design and participation. Healthcare and health research, including mental health, are much larger fields than tourism. They do not currently consider tourism as mainstream mental health therapy; but this may change during post-pandemic recovery.
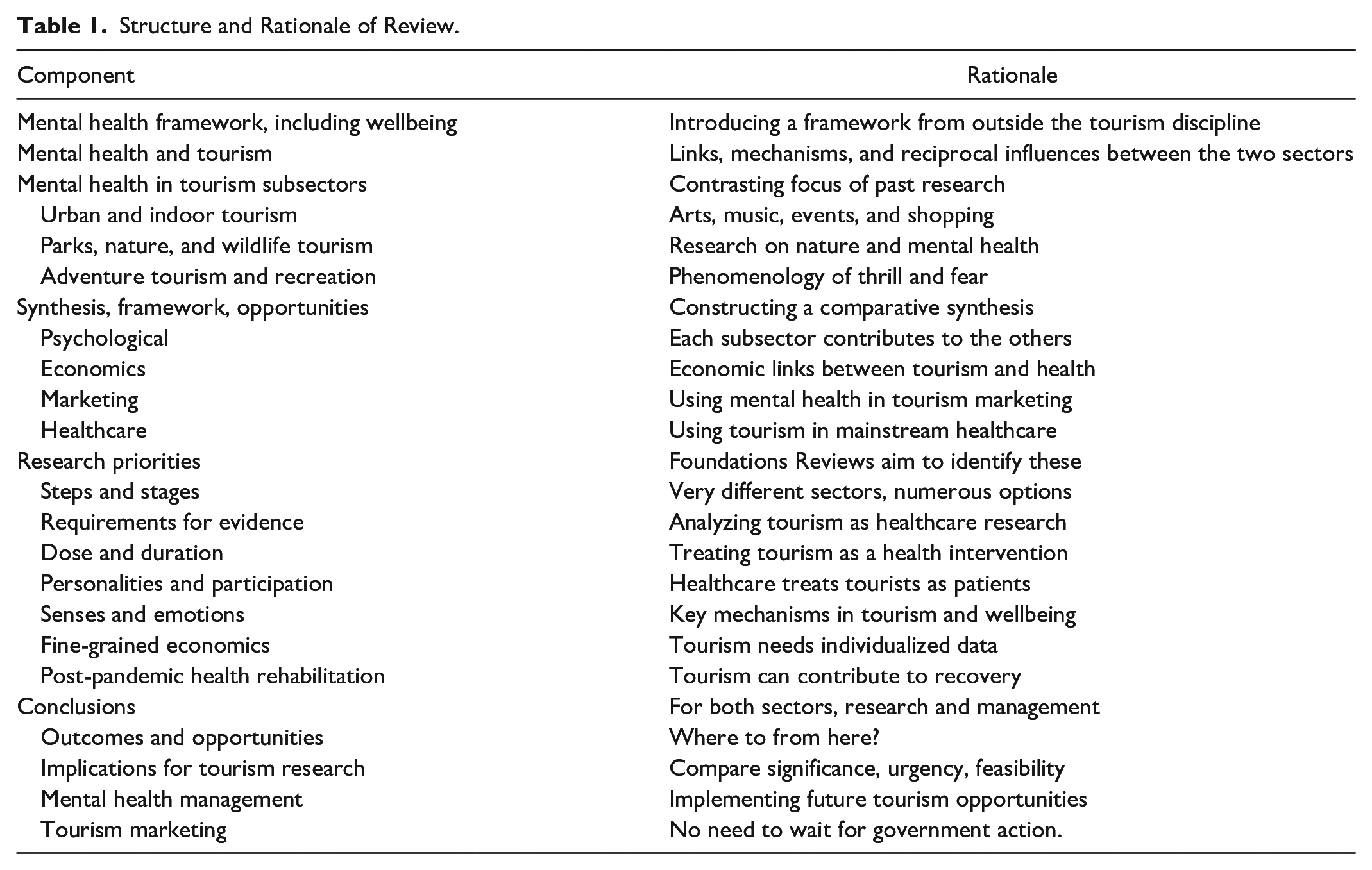
This Foundations review has three principal aims. First, to introduce a mental health research framework, and show how it is relevant in tourism. Second, to review published research across both tourism and health literature, so as to identify the principal linkages. Third, to identify the different emphases and gaps in research in three major tourism subsectors: urban and indoor; parks, nature, and wildlife; and adventure and outdoor recreation. This scope reflects the components of tourism where mental health outcomes depend most directly on the design of tourism products. Business travel, including conferences and events (MICE), is excluded, since it is not leisure travel and is not necessarily purchased with enjoyment in mind. Visiting friends and relatives (VFR) is also excluded, since its mental health outcomes are derived principally from family dynamics, not tourism. The structure of this review is summarized in Table 1. Its overarching goal is to provide a foundation for improved links between tourism and mental health, both in research and in practice.
Structure and Rationale of Review.
Theoretical Frameworks
Mental Health and Wellbeing: Definitions and Distinctions
A substantial component of tourism research has focused on wellbeing, so it is important to note that wellbeing is not the same as mental health (Berbekova, Uysal, and Assaf 2021; Buckley and Westaway 2020; Mehta, Croudace, and Davies 2015; Stewart-Brown 2013). Wellbeing is self-perceived, mental health is externally perceived (Buckley et al. 2019). Wellbeing is maintenance for people in good mental health; psychotherapies are repairs for people in poor mental health. Mental health includes clinical diagnosis and prescribed therapies; wellbeing does not. There are multiple scales intended to measure wellbeing, but only a single underlying construct. For mental health, in contrast, there are many fundamentally distinct parameters, for example, for cognitive capabilities cf emotional components. Countries routinely compile statistics on the economic costs of poor mental health, but not wellbeing. Measuring the mental health effects of tourism within the rigorous frameworks of health science and economics is more complex than measuring wellbeing.
Mental health has many different components: brain, nervous system, and sensory organs; senses, sensations, moods and emotions; and functions such as attention, cognition, memory, judgment, decision, and motor control. There is no single measure of mental health, and no criterion for perfect mental health: there are only population distributions, means, and norms for different parameters. Many aspects are difficult to measure unambiguously, and there are many psychological tests, intended to encapsulate different aspects. Any aspect of the mental health of any individual can fluctuate considerably, at either short or long timescales.
Poor mental health commonly implies that one or more mental functions, as measured by one or more tests, is below a standardized norm derived from population distributions. For example, a person who is anxious or depressed can be considered in poor mental health. Mental ill-health implies greater severity, usually involving a named psychological condition. There is a wide range of conditions and pathologies, defined formally in medical psychiatric manuals. Most mental conditions involve both neurological and biochemical components, but many of the mechanisms are poorly understood (Lynn and Bassett 2019).
Poor mental health can impose substantial social and economic costs, on: the individuals affected; their families and social contacts; and their employers, insurers, and national economies (Livingston et al. 2020; McDaid, Park, and Wahlbeck 2019). There are four main cost categories: direct healthcare costs, lost workplace productivity, costs of paid or unpaid carers, and costs of antisocial behaviors. Jointly, these costs amounted to ~10% of global GNP, prior to the onset of the COVID-19 pandemic. They are now substantially larger.
In developed nations, the proportions of populations suffering from poor mental health have increased during the COVID-19 pandemic in 2020 and 2021, from ~13% to ~40% (Kabasawa et al. 2021; US National Center for Health Statistics 2021), and up to 50% for women (Lindau et al. 2021; Panchal et al. 2021). Drivers include: livelihood losses (Egger et al. 2021); family health concerns; and social and nature deprivation due to lockdowns (Anderson 2021; Buckley and Brough 2021; Fancourt, Steptoe, and Bu 2021; Morse et al. 2020; Occhipinti et al. 2021; Spano et al. 2021; Tomasso et al. 2021).
The social context for mental health has changed considerably in recent years, especially in developed Western nations. Historically, in labor-intensive primary-production and manufacturing economies, only the more severe forms of mental ill health caused significant losses in economic productivity. Those individuals were excluded from the workforce, and in some cases were confined at home or in institutions. To be considered mentally unwell lead to severe negative social judgment, and mental health was a taboo topic of conversation. Currently, however, discussions of mental health are acceptable and encouraged. Mental health implications of any distressing or traumatic event, either personal or more widespread, are likely to be acknowledged and addressed. The importance of good mental health for workplace productivity, especially in professional and service economies, is understood. The economic costs of mental ill health are compiled routinely by national governments and multilateral medical commissions, as part of annual or regular economic statistics. In some countries, mental health resources are delivered by voluntary organizations. Individuals invest in maintaining and restoring their own mental health, by taking rests from mental effort, engaging in mental exercise, and consuming a mixed mental diet of challenging information, sensory impressions, and relaxing entertainment.
In addition to mainstream mental healthcare via government health agencies, insurance, and qualified psychologists and psychiatrists, there is a large industry operating under the name of wellness and lifestyle medicine. In sales, marketing, and corporate cross-ownership structure, this sector is linked to the spa, nutrition, cosmetics, beauty, and fashion industries. It packages and markets products for direct purchase by consumers, without qualified medical diagnosis or prescription. Its marketing terminology, however, and distribution and delivery mechanisms, often mimic mainstream healthcare.
Mental Health and Tourism: Linkages, Mechanisms, and Evidence
Many aspects of tourism research include mental components, at a wide variety of different scales. Smaller-scale frameworks consider tourist psychology at the scale of individual purchase decisions. These involve choice between competing accommodation, transport, or activities. They are driven by tourist motivations and tourism marketing, and they represent discretionary expenditure of time and money. Larger-scale frameworks analyze tourist goals across multiple decisions, either as expansions of affordances, improvements in wellbeing, or investments in mental health (Buckley and Akhoundogli 2020; Cooper and Buckley 2022).
The type, direction, intensity, and duration of the effects of tourism on mental health depend on destination, setting, product, activity, social context, and guiding; and on individual tourist life history, personality, and prior mental condition. Individual people differ greatly in personalities, psychological states, and life circumstances, and these differences may change when people are on holiday, compared to when they are at home. Different people prefer different destinations and activities, and mental health outcomes may differ for the same people between different activities, and for the same activity between different people.
There are perceived to be two principal obstacles to bringing tourism into mainstream mental healthcare: cost and evidence (Buckley, Brough, and Westaway 2018). The perception is that tourism products are too expensive to be prescribed as routine therapies. Many psychotherapies and mental-health chemotherapies, however, are more costly per capita than most tourism products. Consulting a psychiatrist in metropolitan USA, for example, costs typically US$400 per hour. Some mental health drugs (US National Institute of Mental Health [USNIMH] 2021) cost thousands or tens of thousands of dollars or euros per dose or course (Einarson et al. 2017), with sales in US$ billions p.a. Where health costs are paid via insurance or government, these costs are hidden. Pharmaceuticals are routinely compared using $/QALY, quality-adjusted life-years, and ICER, incremental cost-effectiveness ratios (Einarson et al. 2017). Only one study, however, has calculated $/QALY for a tourism-based intervention (Buckley et al. 2019). The perceived cost obstacle can thus be addressed by calculating $/QALY and ICER for tourism products, in the same way as for other therapies.
The evidence obstacle is harder to overcome. Legal approval of medical therapies requires evidence based on randomized controlled trials, RCTs. Participants are enrolled into an experimental panel, and allocated randomly between one or more treatments or interventions, or a placebo or control. At enrollment, participants do not know which group they will be in. In single-blind RCTs, they still do not know which group they are in, even once the experiment starts. In double-blind RCTs, neither the participants nor the researchers know which participants were allocated to which group, until the experiment is completed.
Since people can tell whether they are at home or on holiday, blind RCTs are not possible in testing the mental health outcomes of tourism. In addition, part of any tourism experience is the decision to pay for it, which cannot be allocated randomly between participants. Even if a research project pays for holidays, and allocates them randomly to some of the participants, a holiday may have different effects if it is free rather than full-cost. RCTs have been attempted for some analyses of outdoor recreation and education (Bielinis et al. 2019; Legrand and Mille 2009; Müller-Riemenschneider et al. 2020; Ryu et al. 2020; Sobko et al. 2020; Yen, Chiu, and Huang 2021). These include programs that adopt tourism-type business models, with individual discretionary purchases. There are also analyses using related designs such as randomized crossovers (Niedermeier et al. 2017).
There are other types of healthcare, such as psychological counseling, where blind RCT’s are not feasible, and alternative tests are accepted (Katz et al. 2019). This is also feasible for tourism. Experimental designs can include non-randomized controls (Levi et al. 2019; Wheatley 2021), but these are weaker. For some tests, matched-pair or twin-cohort studies are feasible (Bijnens et al. 2020). In large-scale representative population panels, some individuals experience an intervention, such as visiting parks, and some do not (Astell-Burt, Navakatikyan, and Feng 2020; Astell-Burt et al. 2022; Buckley et al. 2019). Some countries maintain permanent panels with millions of members (Chekroud et al. 2018; Hakulinen et al. 2019), but these must be screened for mental-health representativeness (Chauvenet et al. 2020), and none yet include measures of tourism activity (Buckley and Brough 2021).
Mental Health Research in Different Tourism Subsectors
Urban and Indoor Tourism
Research on tourism and mental health may usefully be considered in three main subsectors: urban and indoor; nature and outdoor; and adventure and sport. Across all these sectors, people take vacations to improve self-perceived wellbeing (Berbekova, Uysal, and Assaf 2021; Chen, Huang, and Petrick 2016; Chen and Li 2018; Chen, Petrick, and Shahvali 2016; Lengieza, Hunt, and Swim 2019; Pyke et al. 2016; Smith and Diekmann 2017; Uysal et al. 2016). This includes the roles of senses (Agapito 2020), including sounds (Gale et al. 2021), smells (Xiao, Tait, and Kang 2020), and tastes (Su and Zhang 2020). It also includes the role of emotions (Chen and Li 2018; González-Rodríguez, Díaz-Fernández, and Pacheco Gómez 2020; Hosany, Martin, and Woodside 2021; Volo 2021; Wang, Hou, and Chen 2021).
Therapeutic benefits of indoor attractions such as arts, music, and museums, have been analyzed extensively, but generally not in a tourism context (Bibb 2021; Van Hoven 2020; Wang, Mak, and Fancourt 2020). There is also a substantial literature on so-called retail therapy, the wellbeing effects of shopping (Craig, Fischer, and Lorenzo-Arribas 2018; Lee and Böttger 2017; Lee and Choi 2020; Rick, Pereira, and Burson 2014; Russell and Rogers 2019).
Parks, Nature, and Wildlife Tourism
Nature tourism, including parks and wildlife tourism, focuses on natural beauty, peace, tranquility, psychological restoration, and recovery. Nature tourism can improve attention, cognition, emotions, relaxation, and worldview (Akhoundogli and Buckley 2021; Buckley 2019b, 2020; Buckley and Westaway 2020, 2021; Cooper and Buckley 2022). Since poor mental health has high economic costs, parks and nature tourism have an economic value through tourist mental health, ~US$6 trillion p.a. worldwide (Buckley et al. 2019). This is 10 times direct parks and nature tourism expenditure, including time and travel costs and economic multipliers (Balmford et al. 2015), and influences the design of park tourism infrastructure (Buckley, Zhong, and Martin 2021). There are numerous recent reviews of mental health benefits of nature (Bratman et al. 2019; Derose et al. 2021; Kondo et al. 2020; Kotera, Richardson, and Sheffield 2022; Marselle et al. 2021; South, Kondo, and Razani 2020; Taye et al. 2021; White et al. 2021; Zhang, Zhang, and Rhodes 2021). As yet, however, there is no general model of the mechanisms by which particular nature tourism products and experiences contribute to the mental health of different individual tourists, and with what economic values to the tourists and tour operators.
From a health perspective, these aspects reflect the diagnosis, design, dose, and duration of nature tourism psychotherapies (Buckley, Brough, and Westaway 2018; Shanahan et al. 2016). Different activities (Pasanen et al. 2019; Svensson et al. 2019, 2021), for different durations (Bélanger et al. 2019; Chen, Zou, and Gao 2020; Labudek et al. 2021; Legrand and Mille 2009; Sanz-Remacha et al. 2021; White et al. 2019), in different environments (Biedenweg, Scott, and Scott 2017; Bielinis et al. 2019; Jarvis et al. 2020; White et al. 2021; Wyles et al. 2019), and countries (Buckley and Brough 2021; Tester-Jones et al. 2020; White et al. 2021) can improve mental health and wellbeing for people of different genders (Buckley and Westaway 2020, 2021; Doran, Schofield, and Low 2018); ages (Cleary et al. 2020; Engemann et al. 2020; Hartley et al. 2021; Jackson et al. 2021; Keith et al. 2021; Putra et al. 2021; Wharton 2020); interests and motivations (Roberts, Jones, and Brooks 2018); mental states or illnesses (Besser 2021; Tester-Jones et al. 2020); and personalities (Wang et al. 2017; White et al. 2016), especially nature connectedness (Martin et al. 2020; Richardson and McEwan 2018; Rickard and White 2021).
Mental health benefits of nature are improved by increased naturalness and ecosystem integrity (Høj et al. 2021; Reining, Lemieux, and Doherty 2021) and by increased biodiversity (Brock, Doremus, and Li 2021; Fisher et al. 2021; Gonçalves et al. 2021; Lindemann-Matthies and Matthies 2018; Methorst et al. 2020, 2021a, 2021b). They are also boosted by sensory experiences such as running water or birdsong (Ferraro et al. 2020; Zhu et al. 2020), or natural scents such as airborne terpenoids from some tree species (Kim et al. 2020); and by experiences evoking emotions (Ballantyne, Packer, and Sutherland 2011; Buckley 2020). There is also limited research on biochemical and hormonal responses (Jones, Tarter, and Ross 2021; Sobko et al. 2020). Most recently, this includes the effects of nature on DNA methylation, essential for cognitive function (Xu et al. 2021).
Adventure Tourism and Recreation
Adventure tourism provides thrill, exhilaration, excitement, and transformation (Buckley 2018a, 2018b, 2020, 2021; Hetland et al. 2019; Holmbom, Brymer, and Schweitzer 2017; Niedermeier et al. 2017; Svensson et al. 2019, 2021). It also involves physical exercise, which itself has powerful effects on mental health, at all ages (Bélanger et al. 2019; Chekroud et al. 2018; Dauwan et al. 2021; Maynou, Hernández-Pizarro, and Errea Rodríguez 2021; Müller-Riemenschneider et al. 2020; Neill et al. 2020; Remme et al. 2021; Smith and Merwin 2021; Yen, Chiu, and Huang 2021).
Adventure tourism includes destinations and activities worldwide, some motorized but most using gravity, wind, water, or human power. Some use fixed-site infrastructure, such as stadiums or ski lifts. Others involve mobile tour operators that provide equipment, guides, expertise, permits, technical training, local knowledge and logistics, and support and safety. Experiences range from high-volume entry-level products with lower risk, skill and price, and a substantial social component, to low-volume expert-level products with higher risk, skill and price, and fewer social interactions (Buckley 2007, 2012, 2016). Psychological benefits are more outwardly directed for the former, for example, through social contacts and capital; and more inwardly directed for the latter, for example, through self-esteem (Buckley 2018b).
During recent decades, historical perceptions of adventure tourists as pathological risk-takers, imposing costs on society, have been reversed. High-volume commercial adventure tourism for unskilled clients has shown that qualified guides with well-designed safety equipment and procedures can maintain risks at low levels. Acceptance as Olympic sports, and large-scale corporate endorsement, of adventure activities such as surfing, climbing and kayaking, has repositioned their practitioners as athletes rather than dropouts. Qualitative research on adventure participants has shown that they exercise socially admired personality traits such as careful judgment and advance preparation, and that adventure experiences generate positive psychological outcomes, some transformative (Hickman et al. 2018; Holmbom, Brymer, and Schweitzer 2017; Wharton 2020).
Advanced adventure tourism involves investment of time, money and effort in acquiring skill. For experiences that take decades to achieve, but last only for minutes or seconds, this indicates very high individual economic valuation of adventure experiences: thousands or potentially even millions of dollars per hour. Since very few individuals achieve these highest-level adventure goals, however, the economic value across entire populations is derived largely from lower-key activities with much milder mental health effects. As for previous studies of park tourism (Buckley et al. 2019), we could use large-scale panels, across single or multiple adventure activities and practice patterns, to identify associations with mental health and well-being, controlled for other causal factors.
Adventure tourism has advanced further than other subsectors in understanding the brain processes underlying mental health gains. This includes senses (Hickman et al. 2018), hormonal responses (Vrijen, van Roekel, and Oldehinkel 2018), emotions (Buckley 2016; Hetland et al. 2019), addictions (Buckley 2015; Heirene et al. 2016) and brainwave patterns (Bailey et al. 2019; Sacchelli et al. 2020). Cognitive perceptual and proprioceptive components operate at timescales down to tenths of a second (Buckley 2014, 2019a; Wittmann 2013), and there is a sawtooth relation between fear and thrill (Buckley 2016). Adventure tourism can lead to lifelong changes in worldview, such as a powerful appreciation for life, and the ability to overcome obstacles (Buckley 2021). There has been related research on mental health in sport (McHenry et al. 2021).
Synthesis, Framework, and Opportunities
Psychological Comparisons
The three subsectors examined above are compared in Table 2, which shows the different emphases of research to date, both in topics and in methods used. There are opportunities to examine additional topics, and apply alternative approaches, between the three subsectors. For example, the economic valuation approach based on quality-adjusted life-years, used to date only for nature tourism, would be equally applicable in other subsectors; and the detailed examination of short-duration psychological and neurological processes, addressed in adventure tourism, could also be applied more broadly. To bring tourism into the healthcare sector, there are also methodological approaches that merit greater emphasis across all tourism subsectors, such as the use of RCT’s where possible, and greater emphasis on strength-of-evidence design and assessment where RCTs are not feasible.
Relative Emphasis of Mental Health Research Across Tourism Subsectors.
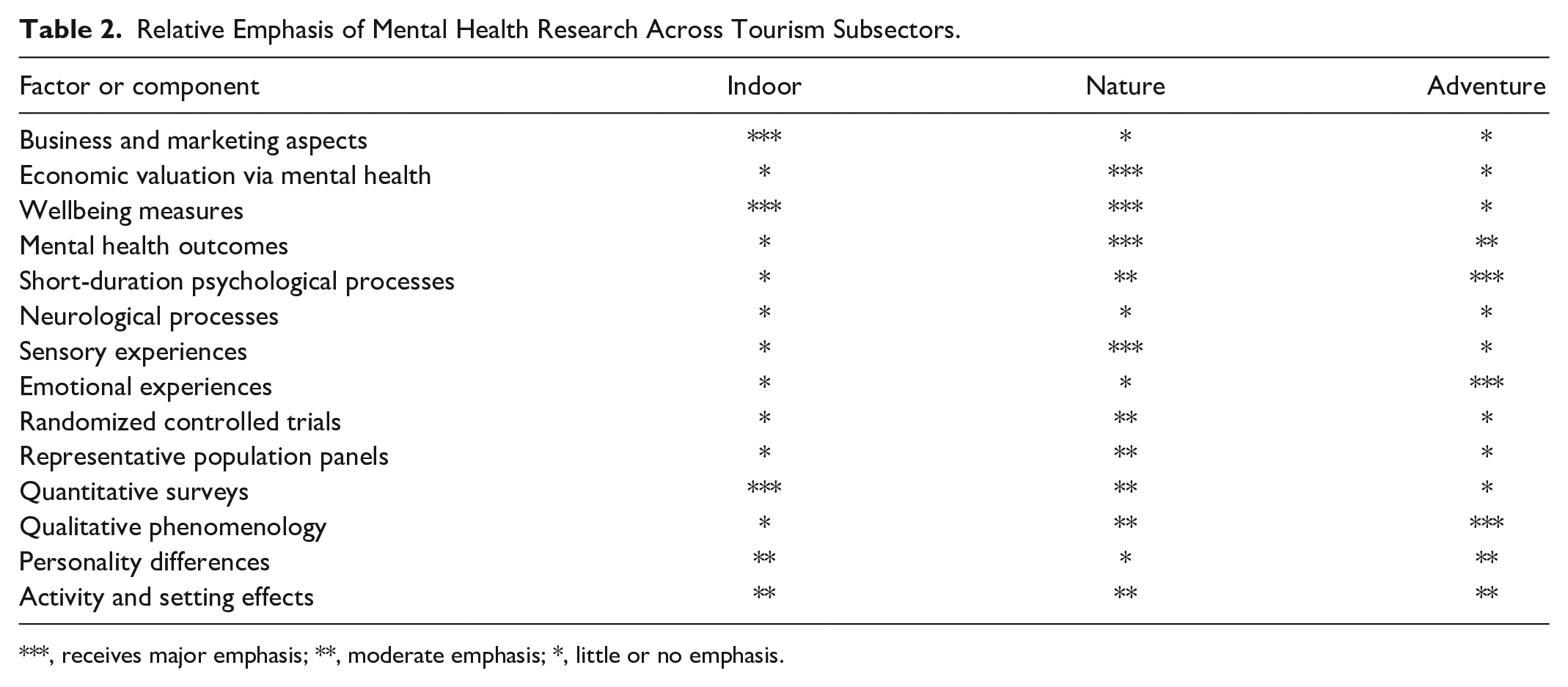
***, receives major emphasis; **, moderate emphasis; *, little or no emphasis.
There are also finer-scale differences between subsectors. For example, senses and emotions are studied increasingly in all three subsectors, but with different focus. In indoor tourism, the focus of research has been on marketing, using sensory measures to create emotional responses in retail establishments. In nature tourism, the focus has been on mental health maintenance and restoration, largely at low-key levels. In adventure tourism, the focus has been on intense psychological effects, which may drive lifestyle transformation for individuals, and repeat bookings for tourism enterprises. In nature, wildlife, and adventure tourism, guides are adept at emotional choreography, adjusting a routine program to the details of circumstances and tourist personalities so as to maximize their enjoyment and create long-lasting positive memories (Ballantyne, Packer, and Sutherland 2011).
Economic Linkages
The steps and stages leading to a tourist experience, and the psychological role and consequences of each for tourist mental health, are summarized in Figure 1. The connections from individual tourist experience to national economy, via mental health specifically, are summarized in Figure 2. These economic connections operate in parallel to tourism expenditure and economic multipliers, the more usual focus of tourism economics. They reflect the place and potential of tourism within the healthcare economy. By casting the psychological and wellbeing benefits of tourism within a healthcare framework, we can use health economics to calculate their financial values, whether at the fine scale of individual tourists and their households, or broader scales such as employers and nations.
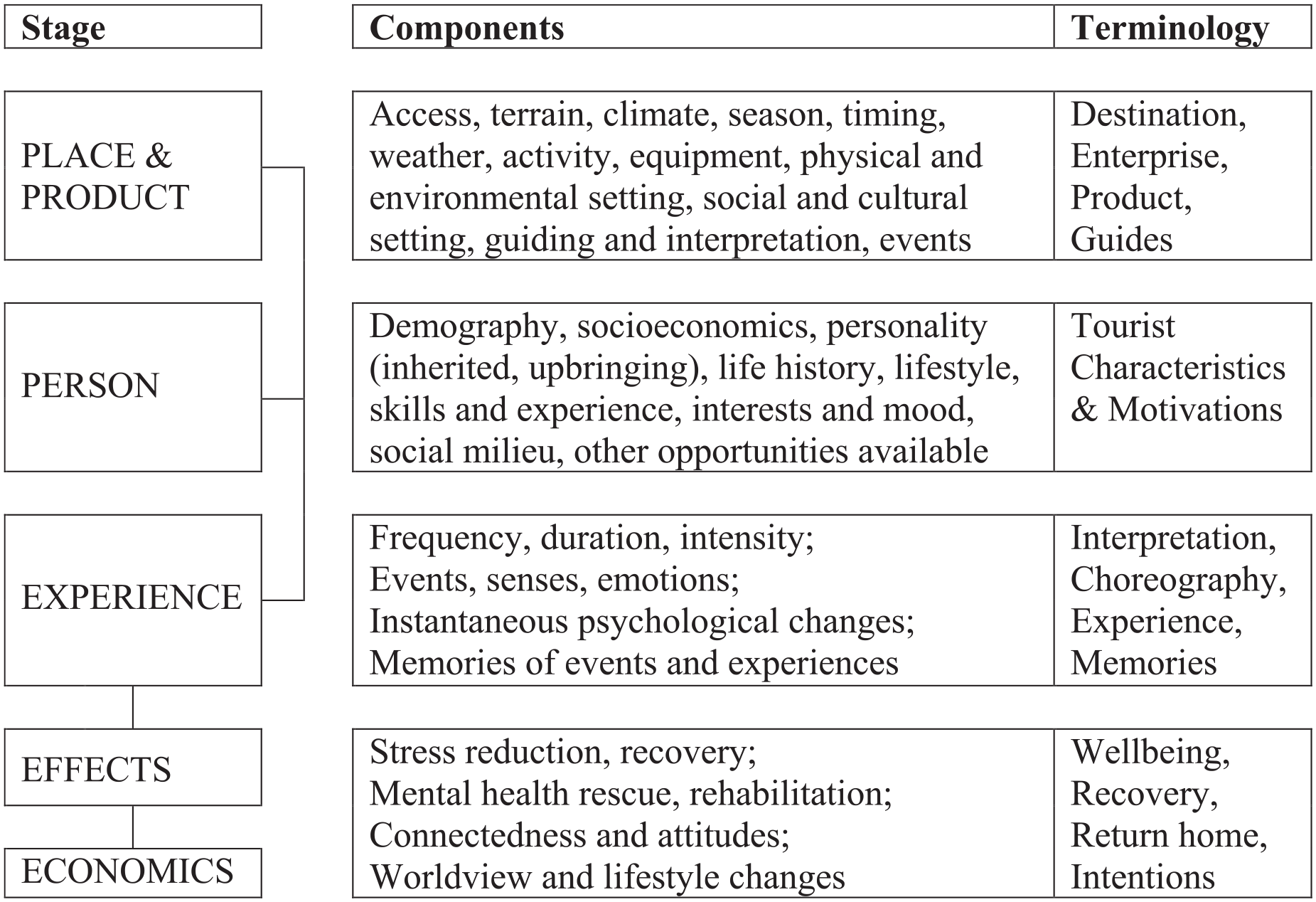
Tourism and mental health: theoretical framework.
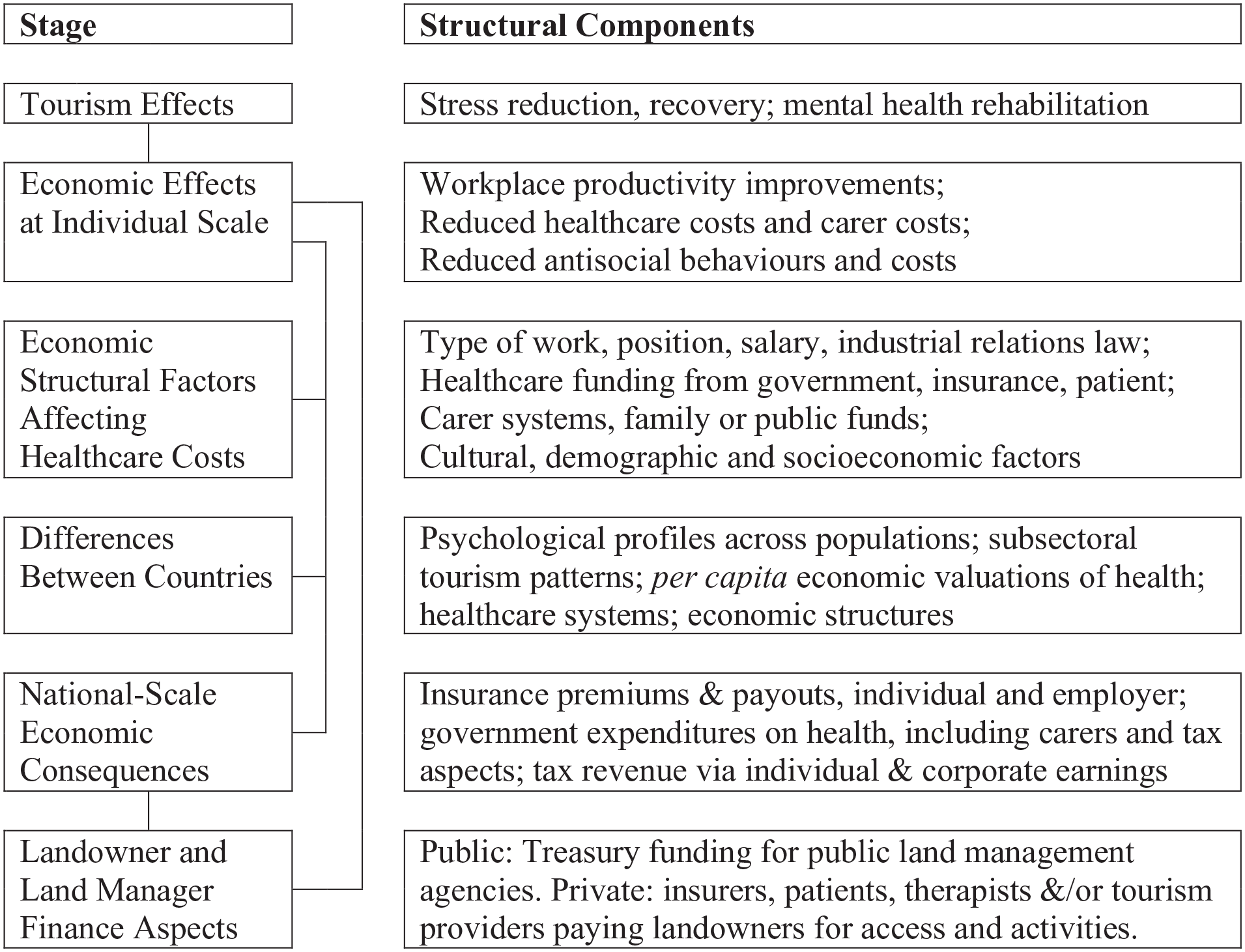
Tourism and mental health: post-experience economic linkages.
As noted at the outset, there are key distinctions in time and space between economic analyses of tourism expenditure, and those of healthcare effects. Expenditure takes place largely before and during a holiday or tourism experience, and largely in or en route to tourism destinations. Health benefits accrue largely after the holiday or tourism experience, and in the tourist country of origin. These temporal and geographical patterns in the economic contributions of tourism via mental health, remain to be analyzed (Buckley and Chauvenet 2021). In particular, a substantial component of international tourism involves tourists from wealthy developed nations, traveling on holiday to less wealthy, less developed nations. Economic analyses to date have focused on where payments are made and received, contributions to destination-country GNP and local resident communities, and transfers of foreign exchange both inward and outward, for example, through external purchases by in-country tourism enterprises to supply materials and consumables.
Where tourism experiences in developing nations contribute to the mental health of international tourists, however, there is another, hidden economic linkage, through the transfer of health benefits to countries of origin. Components of these benefits that accrue to, and are recognized by, the individual tourists themselves are reflected in the prices they are prepared to pay for tourism products. Components that accrue via reduced healthcare costs, improved workplace productivity, and improved public and private social behaviors, however, are effectively positive economic externalities for countries of origin. They represent an invisible economic export, via tourism, from less wealthy developing nations to more wealthy developed nations. These flows, if quantified, would contribute to the calculus of bilateral and multilateral aid, a longstanding component of global geopolitical influence.
Tourism Marketing
Tourism enterprises and destinations have already begun to include mental health benefits explicitly into marketing, especially since the COVID-19 pandemic (Cooper and Buckley 2022). We can anticipate that this will increase, and it will then be useful to test the success of marketing based on mental health, relative to other strategies. It may prove that mental health motivations appeal only to some market sectors. Given the new-found ability of digital matching strategies to analyze and target individual customers (Cooper et al. 2021), mental-health considerations can simply be added to digital marketing mixes.
Digital marketing technologies also provide new opportunities to measure psychological parameters more covertly, indirectly, or conveniently than in the past. There are two main components. The first includes technologies deployed via digital devices or online communications, to track and measure what tourists do or do not want, desire, appreciate, record, and talk about. These include a wide variety of analytics, based not only on keyboard and onscreen inputs, but now also on inbuilt infra-red eye-tracking, voice analysis, and facial emotion recognition (Buckley and Cooper 2021).
Retail salespeople have long used voice, pupil dilation, mannerisms, etc, to make covert judgments about customer interest in specific products. Online search, marketing, sales, and social media platforms can now do the same. The same technologies are also being deployed in online mental health counseling, for example, to measure agitation or relaxation. There seems to be no technical barrier to linking the two. It is already possible, for example, for tourism marketers to pay social media platforms to target ads to users who are both wealthy and in poor mental health. There are substantial ethical implications, but these may be ignored.
The second category includes technologies knowingly worn or carried by individual tourists, such as internet-connected phones, digital watches, cameras, and health and fitness trackers (Birenboim et al. 2019; Roberts and Helbich 2021). These can be used to analyze where tourists are, what they are doing, and what they are looking at, and to measure physiological parameters such as heart rate and skin conductance. Some of these measures are overt, but many are covert. We know from patents, at least to some degree, what they would be capable of, but we don’t always know what they actually do, from moment to moment.
Many of these devices produce continuous records from individual tourists, that are already used to analyze most-photographed attractions, infrastructure use patterns, etc. No doubt they will soon be adapted to record mental health measures as well. At present, these are possible only with relatively intrusive research-level equipment, such as mobile electrocephalographic (EEG) headsets that provide continuous records of individual brainwave patterns. Consumer-level mobile EEG headsets are already available, however, and could be fitted unobtrusively into ski and bike helmets, with local Bluetooth links to phones. Mental health measures could then be recorded contemporaneously with customer interest, satisfaction, or delight.
Tourism as Mainstream Mental Healthcare
There is a large commercial opportunity for tourism within mainstream healthcare. This approach also existed historically in some countries. For wealthier patients, doctors routinely recommended privately-funded grand tours or extended cruises, as antidotes for poor mental health. For the less wealthy, seaside bathing trips were suggested. National healthcare systems in developed nations now aim to include all citizens irrespective of socioeconomic status, albeit somewhat inequitably. Historically, these healthcare systems have emphasized clinical care over public health, hospital over home-based care, physical over mental health, and professional counseling and chemotherapies over lifestyle, nutritional, and nature-based approaches. All of these historical patterns, however, are changing rapidly at present.
The main focus to date has been in nature tourism (Buckley 2019b). There are examples in: China (China National Tourism Administration 2018; Zhao and An 2021); Japan (Kotera, Richardson, and Sheffield 2022; Oh et al. 2017); Italy (Doimo, Masiero, and Gatto 2021); UK (Bickerdike et al. 2017; Reeves et al. 2021; UK National Health Service [UKNHS] 2020); USA (Schmidt 2018); Chile (Cooper and Buckley 2022); and Australia (Buckley, Westaway, and Brough 2016; Buckley and Westaway 2020). Tourism designs maintain behavioral changes, needed for effectiveness (Brennan, Mulvey, and Costello 2021; Carey et al. 2019; Gillison et al. 2019; Hankonen 2020; Heino et al. 2021). There are also small-scale programs known as green prescriptions (Masterton et al. 2021; Patel et al. 2020; Robinson et al. 2020). These do not provide equipment, clothing, guides, physical fitness, or social support.
Research Priorities
Steps and Stages
A series of successive steps are needed for more widespread adoption of tourism in mental healthcare. 1. Demonstrating mental health outcomes, using methods accepted in health research. 2. Assembling detailed data on design, dose, duration, and response, relative to patient mental health symptoms and conditions. 3. Determining differences in effectiveness between individuals, for example, depending on personality, life history, and social situation. 4. Testing and comparing the detailed psychological mechanisms by which tourism experiences influence mental health, and measuring the multiple mental health parameters affected. 5. Designing and testing the various possible social levers, and individual motivational factors, that lead mental health patients to: (a) sign up for tourism therapies; (b) stay engaged and enrolled; and (c) continue relevant lifestyle or behavioral changes subsequently.
Requirements for Evidence
At least in developed nations, healthcare is strictly regulated, to avoid injury and liability caused by any negative side effects. Treatments and diagnostic tools are only legalized after approvals based on expert assessment of extensive evidence. The gold-standard evidence for health research relies on RCTs, but researchers cannot require randomly chosen participants to buy commercial tourism products. Alternatives are accepted where RCTs are not feasible and downside risks are low, as in tourism. RCT’s may not be suitable for testing long-term mental health interventions, where participants may be subject to external influences varying over time. Controls that compare treated cf untreated healthy participants, as well as treated cf untreated unhealthy participants, may be more important than randomizing treatment amongst unhealthy patients. This is feasible in tourism research.
Qualitative analyses have shown that taking part in tourism-type outdoor products and programs can yield powerful psychotherapeutic benefits for some participants (Buckley and Westaway 2020, 2021). They do not, however, show whether these effects are universal, widespread, or restricted. Most treatments are only applicable for particular patients. Healthcare practitioners need evidence and diagnostic tools to determine which patients should receive which treatments. We do not yet have that information for tourism, but there are no fundamental barriers to relevant research so as to expand that knowledge.
Dose and Duration
There is limited information to date on dose-response regimes for tourism-based mental health therapy, even for the simplest park-visit or walking-in-nature designs. These regimes include: design, that is, type of activity, place, and setting, solo or social, guided or unguided, etc; dose, that is, the length and intensity of each individual outdoor tourism experience; frequency, how often the experiences occur; and duration, the total elapsed time period for the entire program. Most nature-based workplace health interventions (Gritzka et al. 2020; Klotz, McClean, and Yim 2020), and local outdoor recreation programs, are short but frequent: 15–60 minutes, daily or weekly. To be effective, nature-based mental health programs need at least 120 minutes nature exposure per week (White et al. 2019). Programs range in duration from days to years, but many do not stipulate frequency or intensity.
Most commercial nature and adventure tourism products, in contrast, are continuous rather than intermittent, high intensity, with total duration from a few hours to a few weeks. The key question is hence whether brief, intense, choreographed, and highly memorable tourism experiences have more or less powerful effects on mental health, than longer, intermittent, and less intense recreational programs. As yet, there are apparently no tests. Such tests are entirely feasible technically, but only if commercial tour clients consent to take part.
Personalities and Participation
The roles of patient symptoms, personality, capability, lifestyle, and life history are also largely untested to date. People with different levels and types of physical and mental fitness are capable of different types of tourism activities, and likely to experience different mental health outcomes. Individuals who visit nature as children continue to do so as adults, but in developed nations, 30%–50% of individuals never visit national parks on their own (Boyd et al. 2018; Buckley et al. 2019). It remains unknown whether this is due to: unfamiliarity and lack of knowledge; lack of access, equipment or resources; or lack of enjoyment, even if guided. Some individuals face socioeconomic obstacles, overcome through public greenspace. Many, however, can afford nature tourism products that incorporate incentives such as enjoyment of nature, self-esteem through adventure, and social support through guided group products.
Research is also needed to differentiate between people who prefer passive contemplative outdoor experiences, and those who prefer more active adventures. These are not mutually exclusive; and the same individuals may enjoy different activities on different occasions or at different ages. Only some individuals, however, take part in adventure tourism activities. Are some individuals born as thrill-seekers; or do they acquire adrenalin addictions as part of their life history (Heirene et al. 2016)? If so, why do those individuals make that choice, what do they gain, and can we calculate its social and economic value?
Senses and Emotions
To answer these questions, we need research on what happens to our brains as we take part in these activities, and also as we learn the requisite skills. Sensory experiences seem to be the most basic mechanism, leading to emotional responses, which lead in turn to psychological recovery, rescue and rehabilitation, and in some case to sustained behavior change and/or lifestyle modification (Buckley 2020; Buckley and Westaway 2020, 2021). To date, however, these multiple mechanisms have not yet been studied jointly. There is a substantial literature on multi-sensory experiences in forest tourism, principally in Japan and China. Emotions have been studied for tourists in general, and adventure and wildlife tourists in particular; but rarely linked either to senses or mental health. The roles of senses and emotions in linking nature experience, individual personality, and mental health, is a priority for future research.
Fine-Grained Economics
We could calculate average economic values of mental health gains for tourists visiting national parks at different frequencies (Buckley et al. 2019). For marketing, however, we want to calculate financial returns on investment for individual clients purchasing particular holidays. For this, tourists from known countries of origin would need to complete brief psychological scales at the start and end of their holiday. That would allow us to calculate the economic value of their enjoyment, via improved mental health, during the holiday itself. To calculate that value over a longer timescale, however, after they had gone back to home and work, we should need follow-up surveys to track the time decay in self-perceived wellbeing (Gump et al. 2021; Yu, Smale, and Xiao 2021). We could also adjust for other influences using matched-pair controls. This would be a very interesting approach, but not at all easy to carry out in practice.
Post-Pandemic Mental Health Rehabilitation
The COVID-19 pandemic has led to severe mental health deterioration worldwide, and governments are seeking large-scale policy responses (Occhipinti et al. 2021). Tourism, and especially nature tourism, can play a significant role in recovery and rehabilitation. This is recognized within the parks and nature tourism industry, for example, in destination marketing. It is also recognized within the mental healthcare sector, and implementation strategies have adopted tourism-type business models. To date, however, none have enlisted the existing commercial nature tourism industry. This would seem to be a major opportunity for both tourism and mental health sectors, if the crossover can be achieved. It is also an opportunity for research in tourism and mental health.
Conclusions
Principal Findings
The principal finding is one of opportunity. There are powerful practical links between tourism and mental health, beneficial to both sectors. There are also strong overlaps in research, but these are rarely recognized, since the two fields use different terminologies and methodologies, and are published in different disciplines. We can compare the frameworks used in tourism and healthcare respectively, by considering each as an intervention in the healthy home life of the individuals concerned (Table 3).
Tourism and Health as Interventions: Comparing Terminology and Focus.
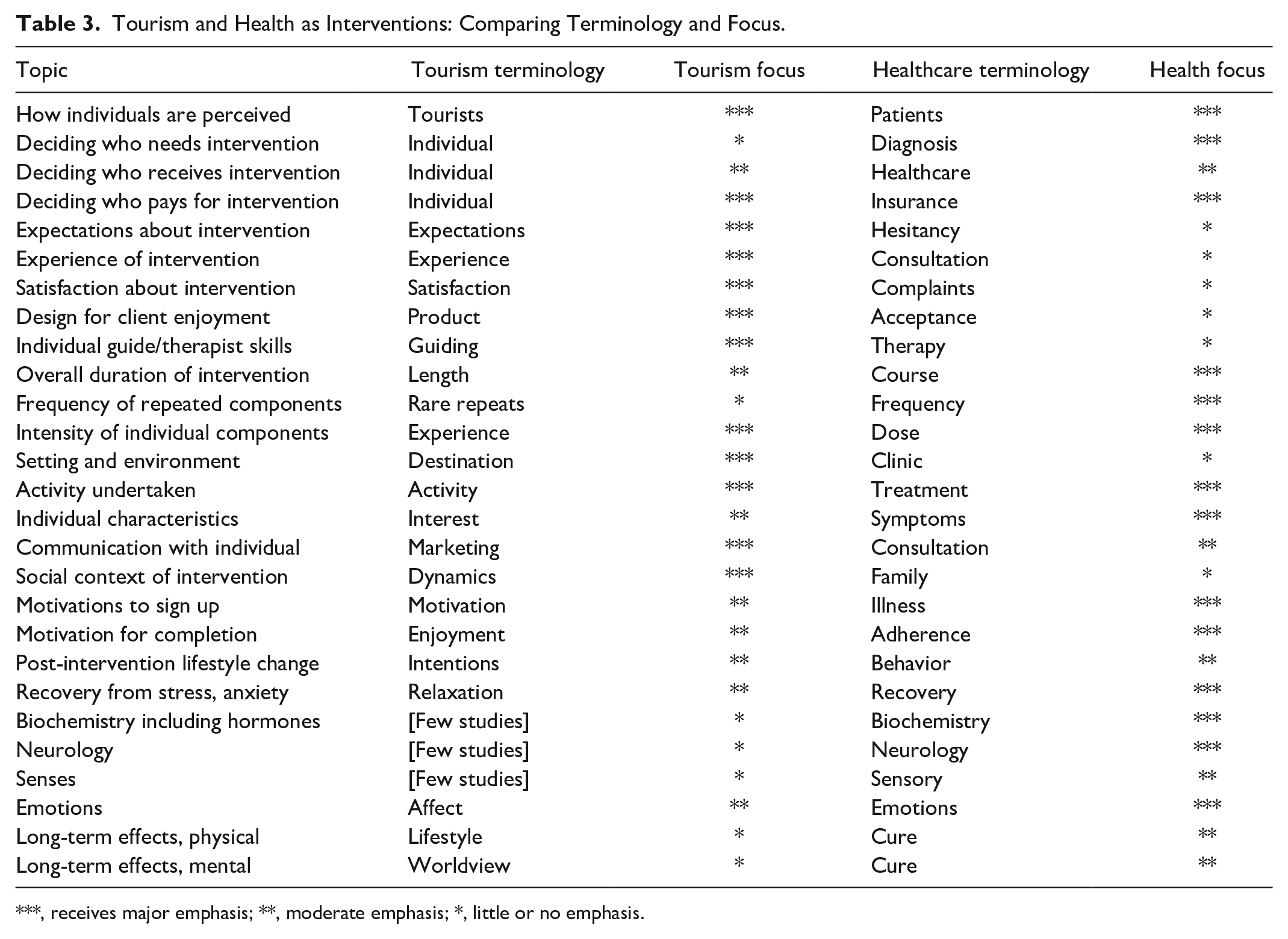
***, receives major emphasis; **, moderate emphasis; *, little or no emphasis.
This comparison shows that the two disciplines emphasize different stages in the intervention. There are thus opportunities for research to consider how to apply existing knowledge across disciplines. As outlined in Table 3, the healthcare sector focuses strongly on who receives interventions, whereas in tourism that is an individual choice. The tourism sector focuses strongly on enhancing positive experiences, whereas healthcare is only interested in avoiding severely negative experiences. In healthcare, aspects such as treatment dose, frequency, and duration are central to the intervention. In tourism, these are subsumed into product design. In tourism, the place where the intervention takes place, the destination, is a dominant component; whereas in healthcare, clinics are all treated as equivalent.
The details of actual activity, and the characteristics of the individual, are important in both tourism and healthcare. In tourism, communications with individuals are proactive, whereas in healthcare, they are largely reactive. In tourism, physiological responses have received little attention until recently, whereas in healthcare they are central. In healthcare, if a patient is cured, they cease to be a patient; but if their symptoms are merely managed, they remain as lifetime customers for treatments. In tourism, a tourist is always a potential future customer, and we are interested in how repeat clients differ from first-time clients.
Implications for Tourism Research
For tourism research, a mental health framework, connecting directly to health policy and economics, provides considerable advantages over a wellbeing framework, that addresses only individual self-perceptions. Mental health research approaches differ to date between indoor, nature, and adventure tourism respectively, and there are opportunities for greater exchange between subsectors. There is a torrent of new research in nature and mental health, but with little involvement yet from tourism. There is new recognition of the role of senses and emotions in tourism, and longstanding tourism research on motivations, expectations, experiences, satisfaction and intentions, highly relevant for mental health, but little utilized.
The role of tourism in mental health is a relatively new field, and there are many topics for further research. One overriding requirement is to adopt methods recognized within healthcare research, for the design and testing of dose-duration-response relationships. A second major focus is to compare differences between individuals, in life history, personality, participation, activity preferences, and cultural constraints and expectations. The third is to analyze differences in tourist experiences and psychological mechanisms, focusing on timescales, attention, senses, emotions, stress recovery, and memorability, in relation to terrain, ecosystem, weather, biodiversity, activity, frequency, duration, and social setting. Fourth is fine-grained economic valuation of mental health outcomes, to calculate financial return on investment for individual product purchases by individual tourists.
One priority for future research is to differentiate the effects of different components of the various tourism subsectors. How much of the mental health effects are due to setting and activity, how much to social and service components? For parks, nature, and wildlife tourism, for example, how important are naturalness, biodiversity, particular plant or animal species, specific animal behaviors such as displays, explanatory interpretation by skilled guides, or opportunities for close and extended observation; and how does relative importance differ between novice and experienced nature tourists? Similarly, in adventure tourism research, we could distinguish the mental health benefits of learning new adventure skills, from those of physical exercise; and we could analyze sensory and emotional components and memories, to determine to what degree they may add to learned mastery of physical skills.
Implications for Mental Health Management
We can examine how to engage commercial tourism enterprises, especially in nature tourism, in post-pandemic mental health recovery. As above, there is a large research literature that examines type and degree of nature exposure, individual demographic and socioeconomic parameters, and neighborhood and life history effects, for a wide range of physical and mental health conditions, across many different countries. There is much less research about the practical institutional mechanisms to deliver nature therapies; and less still about the opportunities for commercial tourism in mainstream mental healthcare.
Even though tourism products may be no more costly than counseling or chemotherapies, mainstream healthcare systems will not prescribe them until they are repackaged as mental health therapies, and their medical effectiveness and cost effectiveness analyzed rigorously. We therefore need practical trials of tourism programs with different types, frequencies, and durations of nature-based activities, to optimize designs for maximum effect; and institutional systems to bring nature and adventure tourism into mental healthcare systems.
Implications for Tourism Marketing
A substantial proportion of individual mental healthcare is funded privately by individuals, rather than by insurers or government; and private purchases are not subject to the same restrictions as government programs. For parks, nature, adventure, and wildlife tours, the most immediate opportunity is in marketing mental health benefits of existing products, if we can quantify effectiveness, duration, and economic values. We can use wildlife and adventure tourism as test cases, since guides routinely aim to choreograph memorable experiences for clients. This is reflected in the surge in domestic visitation to national parks during pandemic-related travel restrictions (Jones et al. 2021; McGinlay et al. 2020; Volenec et al. 2021). As international tourism re-opens post-pandemic, we can predict that tourism marketing will continue to increase its emphasis on mental health benefits. Hopefully, we shall soon be able to test this prediction.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.