
Abstract
Most studies of the early origins of adult health rely on summing dichotomously measured negative exposures to measure childhood misfortune (CM), neglect, adversity, or trauma. There are several limitations to this approach, including that it assumes each exposure carries the same level of risk for a particular outcome. Further, it often leads researchers to dichotomize continuous measures for the sake of creating an additive variable from similar indicators. We propose an alternative approach within the structural equation modeling (SEM) framework that allows differential weighting of the negative exposures and can incorporate dichotomous and continuous observed variables as well as latent variables. Using the Health and Retirement Study data, our analyses compare the traditional approach (i.e., adding indicators) with alternative models and assess their prognostic validity on adult depressive symptoms. Results reveal that parameter estimates using the conventional model likely underestimate the effects of CM on adult health outcomes. Additionally, while the conventional approach inhibits testing for mediation, our model enables testing mediation of both individual CM variables and the cumulative variable. Further, we test whether cumulative CM is moderated by the accumulation of protective factors, which facilitates theoretical advances in life course and social inequality research. The approach presented here is one way to examine the cumulative effects of early exposures while attending to diversity in the types of exposures experienced. Using the SEM framework, this versatile approach could be used to model the accumulation of risk or reward in many other areas of sociology and the social sciences beyond health.
Keywords
Introduction
A key idea of life course epidemiology is that early life experiences influence health and well-being in later life through a set of biological, psychological, and social mechanisms (Barker et al. 2002; Ben-Shlomo and Kuh 2002; Elder, Johnson, and Crosnoe 2003; Ferraro, Shippee, and Schafer 2009; Miller, Chen, and Parker 2011; Shonkoff, Boyce, and McEwen 2009). Empirical studies have consistently documented that childhood misfortune (CM) raises the risk of multiple negative outcomes in adulthood such as chronic disease (Morton, Mustillo, and Ferraro 2014), disability (Rose, Xie, and Stineman 2014), depression (Kessler and Magee 1993), and well-established negative health behaviors such as smoking (Anda et al. 1999; Bowen 2010; Davis et al. 2014; Friedman et al. 2015; Kessler and Magee 1993; Pavela and Latham 2016; Rose et al. 2014). These findings also contribute to the evidence base for theoretical advances in life course epidemiology (Ben-Shlomo and Kuh 2002) and cumulative inequality (Ferraro and Shippee 2009).
Despite these empirical and theoretical advances, there remains a fundamental and neglected question of how to measure accumulated negative exposures. Empirical studies have used different approaches to measure negative childhood exposures, but an underlying procedure—adding indicators—is widely used. The purpose of this article is to systematically examine this practice and compare it to an innovative modeling approach to assess the way negative exposures during early life influence health and well-being. Central to our task is to demonstrate the limitations of the widely used approach and the strengths of this new approach that enables us to evaluate both the differential and cumulative impact of CM on health. Additionally, recent theoretical developments in life course research conceptualize human developmental trajectories as a product of two life course processes involving the accumulation of both risks and resources (Ferraro and Morton 2018). Although early life disadvantages can accumulate to shape health outcomes, the accumulation of resources and protective factors may attenuate or counteract the consequences of early disadvantage. We will illustrate that our new approach can be applied to study the impact of both cumulative processes and the interaction of the two in influencing health outcomes.
Additive Approaches to Cumulative CM
CM is used here as an umbrella term covering a wide range of negative childhood experiences from contextual disadvantage, which may not be seen by the child as adverse, to traumatic experiences in different life domains. Different lines of research, often originating in different fields, use a variety of terms, such as childhood adversity, disadvantage, and trauma, in some cases referring to very specific types of childhood experiences and in other cases covering a broader set of experiences. Given that very few studies actually assess the respondent’s perceived level of adversity, Morton, Markus, and Kenneth (2012) proposed a hierarchical framework with misfortune as the most encompassing term to describe (1) negative exposures, (2) adversity involving “distress or harm,” and (3) trauma as “the most vexing adverse conditions” (p. 980). Low parental education, parental substance abuse, and physical abuse are examples of these three categories, respectively.
This conceptual hierarchy, reflecting the severity of harm, is also manifested in research examining specific childhood exposures such as abuse (Felitti et al. 1998; Springer et al. 2003; Wegman and Stetler 2009), low socioeconomic status (SES; Galobardes, Lynch, and Smith 2004; Hayward and Gorman 2004; Warner and Hayward 2006), and health problems (Haas 2007; Haas, Krueger, and Rohlfsen 2012). By contrast, some studies reveal that the sheer number of negative exposures, regardless of severity, harms adult health (Davis et al. 2014; Felitti et al. 1998; Finkelhor, Ormrod, and Turner 2007). Some scholars, however, balk at the notion of adding all types of misfortune into a global measure (Kelly-Irving and Delpierre 2019; O’Rand and Hamil-Luker 2005).
Negative childhood exposures rarely occur in isolation, as they are often clustered (Jacobs et al. 2012; Kessler et al. 2010). For instance, children living in poverty are at greater risk of exposure to dysfunctional parenting and trauma. The clustering of CM has thus triggered scholarly interests in the cumulative impact of multiple negative experiences in particular domains. Indeed, the notion of early-life accumulation of misfortune has gained prominence among social scientists and life course epidemiologists who have put forth concepts such as “risk clustering” and/or “risk accumulation” to depict the fact that co-occurring disadvantageous events/experiences can combine to impact later-life health status (Ben-Shlomo and Kuh 2002).
Much of the current understanding of the cumulative health impacts of CM has grown out of four related but distinct bodies of work on (1) adverse childhood experiences (ACEs), (2) cumulative childhood trauma, (3) additive CM, and (4) cumulative childhood SES disadvantage. Studies in these areas have consistently documented a positive association between the number of adverse childhood exposures and health risks in adulthood, a pattern that many refer to as a “dose–response” relationship (Friedman et al. 2015). Although studies in these four bodies of literature focus on different aspects of CM and use slightly different operational definitions and measures for CM, most construct some type of index of CM by summing indicators of misfortune or perhaps domains of misfortune in some fashion.
A review of these four bodies of literature reveals that there are two main practices for adding CM indicators. The first and most common is to add all available epistemic indicators for childhood negative exposures to construct an overall score for cumulative CM. For example, the Adverse Childhood Experiences study uses an ACE score that sums dichotomous exposure indicators for eight different types of childhood adversity (Anda et al. 1999; Dong et al. 2003; Felitti et al. 1998; Hillis et al. 2000). Most cumulative trauma studies focus on the sum of individual traumatic events (Briere, Kaltman, and Green 2008; Cloitre et al. 2009; Follette et al. 1996; Ogle, Rubin, and Siegler 2014; Suliman et al. 2009). Similarly, in the childhood SES literature, studies tend to measure the cumulative effect of low SES exposure by adding up different types of socioeconomic adversities and/or time units of poverty exposure (Cohen et al. 2004, 2010; Montez and Hayward 2014; Pollitt, Rose, and Kaufman 2005). This simple additive approach is parsimonious and conveys the idea of a dose–response relationship between CM and health outcomes, but it does so at the expense of treating all CMs equally or all time periods equally. That is, studies using this approach alone cannot determine whether one type of CM has more of an impact than another or whether one time period is more impactful than another. To overcome this limitation, some scholars use the epistemic indicators separately (Hayward and Gorman 2004), but this approach cannot assess the cumulative impact and can become unwieldy with a large number of indicators, especially if they are correlated.
The second approach is to cluster closely related childhood adversities into a few preconceptualized life domains and then sum up indicators within those domains and, possibly, sum across domains as well. For example, two recent studies organized dozens of indicators of CM into five domains: infectious disease, chronic disease, impairment, SES, and risky parental behavior. Each domain was created by adding the dichotomous (Kemp et al. 2018) or trichotomous indicators (Kemp et al. 2018; Smith et al. 2019). Compared to the first approach, this approach represents a more refined effort to distinguish the unique impact of CM in different life domains, but this approach fails to capture the dose–response relationship like the first approach. In an attempt to do both, a study of the cumulative impact of CM on risk of acute myocardial infarction classified 16 items of CM into four domains: SES, household structure, maltreatment, and poor health and summed the four domains (0–4; Morton et al. 2014). The logic of this approach is to compare results derived from domain-specific and summed CM. These widely adopted additive approaches have been useful tools for assessing the cumulative burden of CM and may serve as an effective screening tool to identify young people in need of intervention. At the same time, we identify several limitations of these approaches that constrain research advances.
Limitations of Additive Approaches
The summed score approach for measuring cumulative CM rests on two assumptions. First, the additive approaches described above assume that each misfortune or domain carries the same level of risk for a particular outcome. That is, each indicator carries equal weight in a summed score. Second, they assume that each misfortune or domain carries the same risk for every outcome. Although the summed score can have a different association with different outcomes, the individual elements therein cannot have distinct relationships with different outcomes. Both assumptions are hard to sustain in light of empirical evidence. Studies have revealed that different CM domains do not have the same impact on particular health outcomes. For example, maltreatment in childhood carries greater risk of acute myocardial infarction in later life than do childhood SES and childhood health (Morton et al. 2014).
There is also evidence that interpersonal traumas (e.g., assault or abuse) in childhood are more likely than noninterpersonal traumas (e.g., accident or natural disasters) to cause psychiatric problems in later life (Ford et al. 2006, 2010). In addition, different health outcomes may be associated with specific CM domains only. For example, low childhood SES is a strong predictor for stomach and lung cancer mortality but not for other cancers (Galobardes, Lynch, and Smith 2008). Similarly, parental incarceration predicts adult mental illness but not chronic disease or obesity (Lee, Fang, and Luo 2013). As such, simply adding different CMs together and relating the sum to different outcomes can produce misleading results because the relationships between types of CM and various adult health outcomes are distinct. The empirically unfounded assumption that different adverse event/experiences carry similar weights in predicting different health outcomes calls into question the validity of summed score approaches for evaluating the cumulative effect of CM.
Further, summed score approaches, with the tenuous assumptions mentioned above, also limit inquiries into underlying mechanisms linking different CMs with later-life health outcomes (McLaughlin and Sheridan 2016). Because they fail to distinguish between types of CM, global sums assume that all adverse experiences influence outcomes through the same underlying mechanisms. In other words, CM scores assume that maltreatment, poverty, health problems, dysfunctional parenting, and parental incarceration will build up cumulative impacts on different later-life health outcomes in exactly the same way, which is highly questionable (Appleton et al. 2017). Other scholars are critical of global CM sums because they potentially confound severity and chronicity (Davis et al. 2014; Schilling, Robert, and Susan 2008). As such, summed score approaches provide few clues about what specific events/experiences are involved as potential mediators or moderators of the cumulative impact of CM on a given outcome, and worse, they impair further inquiry into underlying mechanisms.
Finally, summed score approaches may dissuade scholars from using meaningful information to construct better measures of CM or its domains. Researchers summing items within or across domains often have to measure CM items or domains dichotomously in order to add them, sometimes even dichotomizing continuous scales to do so (Barr et al. 2018). Such dichotomization in order to sum constrains scholars’ ability to maximize available data and construct the best measures possible. Dichotomizing variables is generally advised against in the methodological literature, particularly because it leaves decisions about where to set the cutoff point to the discretion of either the researcher or the research participants, a process which creates noise and inaccuracy, the loss of information (e.g., duration, intensity), and the reduction of power to detect a true relationship (i.e., type-II error). Summed score approaches are thus unable to take into account the duration and/or severity of individual CMs in estimating the cumulative CM impact or to integrate latent CM variables that could be an effective way to improve the measurement of concepts and/or reduce data dimensions. Few studies have measured specific misfortunes as latent variables, perhaps because it is inconvenient to add latent variables when constructing cumulative CM measures.
Overcoming the Limitations: A Structural Equation Modeling (SEM) Approach
We advance an SEM approach for the study of cumulative CM because it has the potential to address the aforementioned limitations, namely, the equal-weight assumptions, the concealing of potential mechanisms, and the limited measurement of constructs. The SEM framework provides a flexible tool to construct a second-order composite latent measurement model instead of a summed score measure, which represents an index of a weighted sum of conceptually distinct measures (Bollen and Bauldry 2011).
A composite latent measurement model produces a latent variable that is a special case of the formative latent variable, which stands in contrast with a reflective latent variable. Often being constructed via factor analysis models, a reflective latent variable represents a construct with conceptual unity that could be measured with multiple internally consistent indicators. A composite latent variable represents an index of a weighted sum of conceptually distinct observed/latent indicators (Bollen and Bauldry 2011). In a reflective measurement model, the causality flows from the latent construct to indicators, which could be understood as the manifestations of the underlying construct. In a composite measurement model, there need not be conceptual unity among the indicators or a causal relationship between the indicators and the latent variable, which is formed by or composed of the combination of indicators.
A composite measurement model includes several indicators (i.e., composite indicators) predicting a latent composite without an error term (or, equivalently, the variance of the error term set to zero). Although composite indicators occupy the same statistical position with covariates in a regression model and/or causal indicators in a formative latent measurement model, they have different theoretical interpretations (Bollen and Bauldry 2011). Coefficients for causal indicators may be biased in meaningful ways if there are omitted variables. Composite indicators, by definition, have no bias in that there is no error term. In other words, the theoretical latent variable is entirely defined by the (available) composite indicators. Thus, a composite latent measurement model allows us to simultaneously estimate both the cumulative impact of CM and the distinctive contribution of individual CMs or CM domains. Because it does not involve straight summation, a composite latent measurement model approach allows us to use individual CMs measured at any level such as continuous CM variables containing information on duration and severity, latent CM variables, and transformed variables to accommodate nonlinear relationships.
Additionally, the flexible SEM framework enables us to incorporate mediators to test distinct mechanisms linking individual CMs and health outcomes and the cumulative CM variable and the health outcome simultaneously. Finally, this SEM approach also can be extended to examine the offsetting impact of positive exposures such as resource accumulation. This application has an important theoretical implication because life course development is a joint product of the accumulation of risk and resources (Ferraro and Shippee 2009; Ferraro et al. 2009).
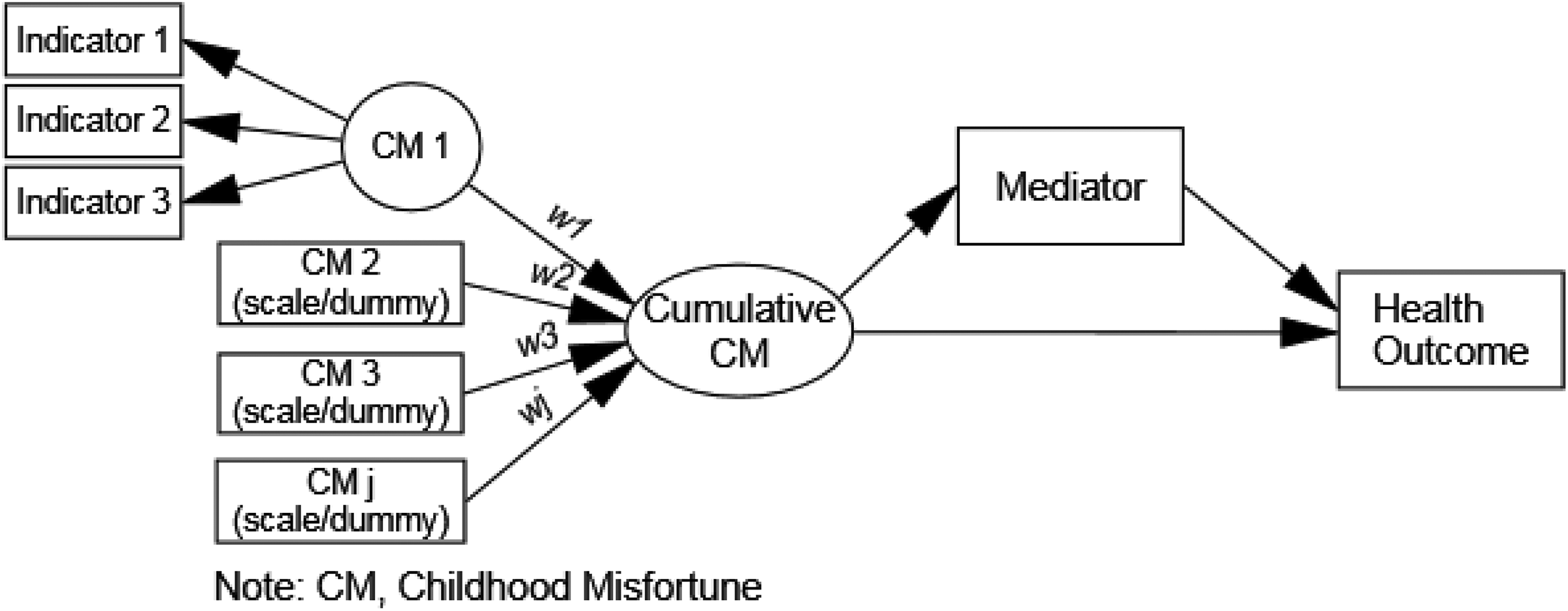
We demonstrate our method in four steps. In the first step, we estimate the impact of cumulative CM on a health outcome (i.e., depressive symptoms) using the conventional summed score approach. We refer to this model as the summed score model or model 1. In the second step, we estimate a structural equation model in which individual CM variables are summarized into a composite latent construct of cumulative CM, which in turn relates to depressive symptoms (Figure 1). We name this model the composite latent model or model 2. The major difference between models 1 and 2 is that model 2 allows different CMs to have distinct weights in the additive variable, based upon the relationship with the outcome, but it retains the dichotomous measurement of the variables. We should note that others in related fields like quality of life studies have proposed weighted indices based upon relative weights derived by citizen agreement (Hagerty and Land 2007). Our approach is empirically derived.

Formative latent model for the health impact of cumulative childhood misfortune.
In the third step, we reestimate model 2 using improved measurement for some CM variables. Specifically, we replace one dichotomous CM variable with a latent measure based on multiple effect indicators and replace a few others with continuous observed variables that include duration information. We also include a log-transformed CM variable to demonstrate that the model can take into account nonlinear relationships. We label this model the hybrid latent model or model 3 (Figure 2). We call this model the hybrid latent model because it involves a higher-order composite latent model (for the cumulative CM), a lower-order measurement model (for the latent individual CM measures that can be either reflective or composite themselves), and observed CM variables measured at different levels. This step demonstrates the flexibility of our method in dealing with various CM measures containing improved information, including duration, of different types (i.e., latent and observed) and at different levels (i.e., dichotomous, continuous).

Hybrid latent model for the health impact of cumulative childhood misfortune.
In the fourth step, we further incorporate two potential mediators linking the individual and cumulative CM variables and the health outcome. We name this model the hybrid latent mediation model or model 4 (Figure 3). This model demonstrates that our method will allow identifying distinct mediating mechanisms for distinct outcomes. The mediators examined include adult SES and functional limitations. Models estimated in the four steps are hierarchically nested, with the fourth model being the most complex. A summary of these models is presented in Table 1. We compare the goodness-of-fit indices from the summed score model, the composite latent model, and the hybrid latent model to demonstrate that our method, by freely estimating differential contributions and incorporating more sophisticated measures, will progressively explain more variance of the outcome.
Hybrid latent mediation model for the health impact of cumulative childhood misfortune.
Summary of Models.
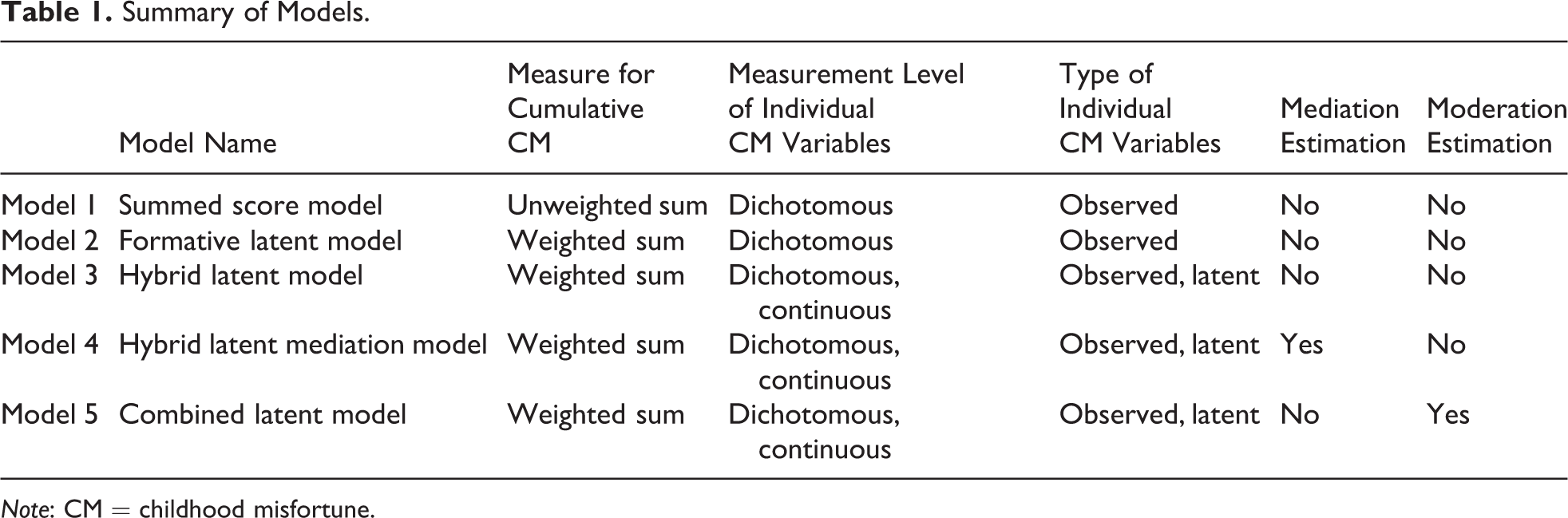
Note: CM = childhood misfortune.
In addition to the models mentioned above, we replicate steps 1–4 to estimate the impact of cumulative resources. Then, we combine the hybrid latent models for cumulative CM and cumulative resources to estimate the interaction effect of the two types of cumulative exposures (positive vs. negative) on the health outcome (i.e., the combined latent interaction model, Figure 4). These additional steps are to demonstrate the wider application of our method and its potential contributions to theoretical development. In the next section, we describe the data used for the demonstration and provide details on the specification, estimation, and interpretation of the model.
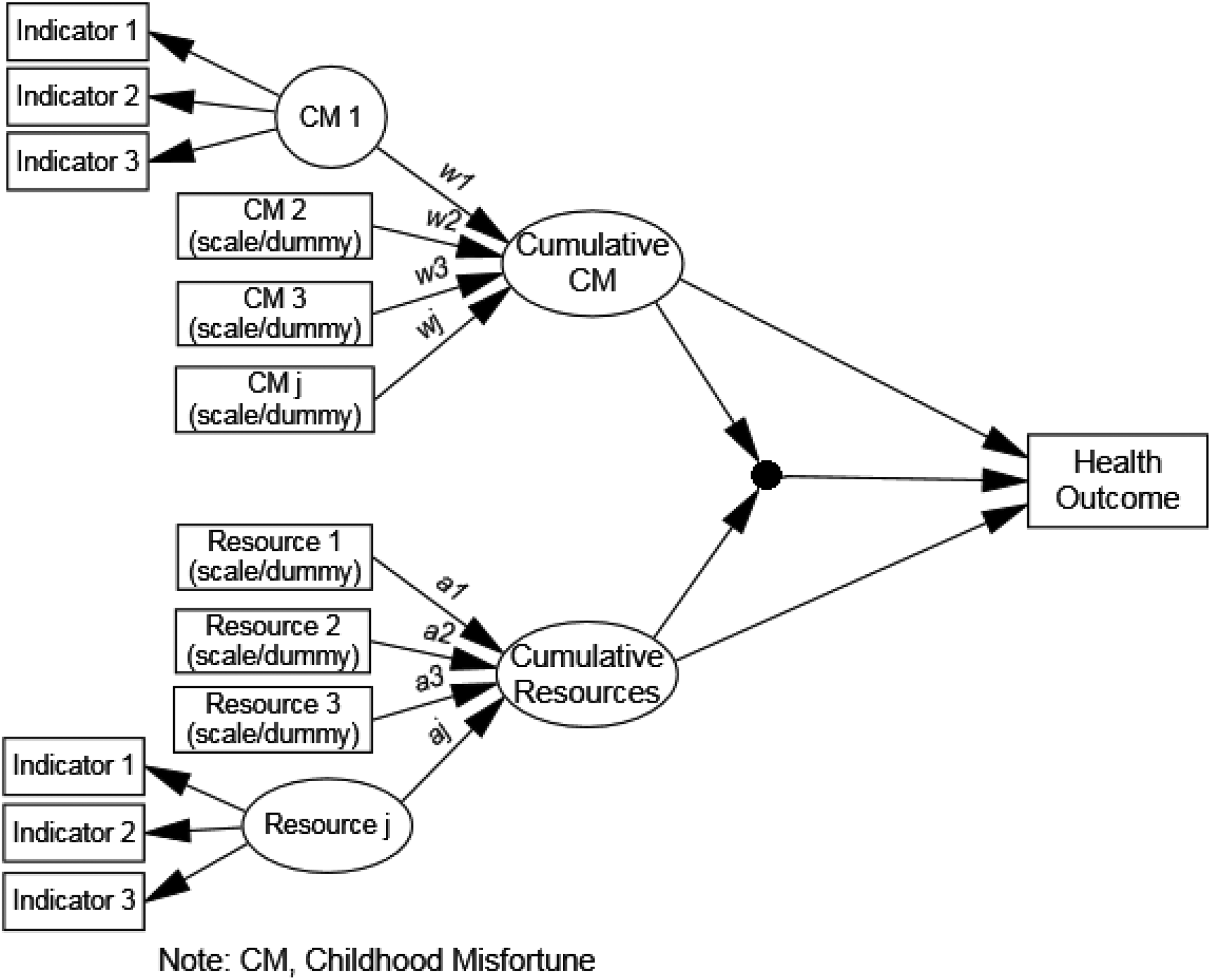
Combined latent interaction model for the health impact of cumulative childhood misfortune and cumulative resources.
Method
Data
We use data from waves 7–10 (2004–2012) of the Health and Retirement Study (HRS), a multistage area probability panel study of adults 51 years of age and older. The HRS began in 1992 and has conducted follow-up interviews every two years since that time (HRS 2015). The 2004 response rate was about 88 percent (Sonnega et al. 2014). Black and Hispanic adults, as well as residents of the state of Florida, were oversampled, making the HRS the largest and most representative panel study of adults over 50 in the United States ever. To construct our analytical sample, we focused on respondents who were alive in 2004, had no validity issues on CM reports (i.e., not reported by proxies), and had a mean total cognition score that was not two standard deviations below the mean (N = 13,921). Among these respondents, we excluded those with missing data on any CM variables and any protective factors (7,837 cases excluded, remaining sample size = 6,084). We further excluded persons with racial identification other than non-Hispanic white, black, and Hispanic from the analyses due to very small sample size. The final analytic sample size is 5,965.
Measurement
Health outcome
We used depressive symptoms as the main health outcome to demonstrate our method. In the HRS, depressive symptoms were measured in each wave between 2004 and 2012 with an eight-item Center for Epidemiological Studies Depression Scale (CES-D) measure. Because much extant literature finds that the CES-D is a multidimensional concept, we include the five items that typically load on a “depression” factor: felt depressed, felt happy (reverse coded), felt lonely, enjoyed life (reverse coded), and felt sad. 1 We used the mean score of depressive symptoms measured between 2004 and 2012.
CM
Based on a group of retrospective childhood questions in the core surveys of HRS, we identified seven CM variables that map onto the three types of adversity presented in the Introduction: low family SES and parent smoking (negative exposures); childhood poor health, childhood disability, childhood depression, and parent substance use (adversities associated with distress or harm); and parent physical abuse (trauma). Each of these variables has been found in prior research to be an adverse childhood exposure that has a negative impact on adult health.
In the equal-weight summed score model, all CM variables were coded dichotomously to be summed into an overall score of cumulative CM. Specifically, low family SES was measured as father having less than eight years of education. Childhood poor general health was measured as having “fair or poor” self-rated health. Parent physical abuse, parent substance use, parent smoking, childhood depression, and disability took the value 1 if the condition is present and 0 otherwise. The composite latent model in step 2 also used the same set of dichotomous CM variables.
In the hybrid latent model, the hybrid latent mediation model, and the combined interaction model, we measured childhood family SES as a reflective latent variable (i.e., a factor score) loading on father’s level of education (measured on five-point scale ranging from “lower than elementary school” to “above college”), mother’s level of education, and self-rated financial situation (measured on a four-point scale ranging from “poor” to “pretty well-off”). All three variables were coded in such a way that higher values indicate lower SES. We treated childhood SES indicators as effect indicators to demonstrate our method’s capacity to incorporate reflective latent measures of CM, which are typically difficult to sum into an overall CM score. To fully demonstrate our method’s capacity to incorporate other types of CM measure and because latent variables for SES are often specified with formative indicators rather than reflective, we include four supplemental tables (Online Supplemental Tables 1–4) to summarize results from alternative model specifications with childhood SES indicators being treated as composite indicators in Online Supplemental Tables 1 and 2 and as a single-item observed variables in Online Supplemental Tables 3 and 4 (father’s education). A model with causal indicators, which is an increasingly common way to model SES and the method recommended in several papers by Bollen (e.g., Bollen and Davis 2009), is not identified and thus not estimated here. Bollen and Davis (2009) mention the difficulty in identifying causal models.
We also used a more refined measure for childhood poor general health, which ranged from 1 (excellent) to 5 (poor). Finally, for childhood depression, we integrated duration information by measuring it as the years of having depression (0 represents the absence of depression, top-coded at 16). Due to a nonlinear relationship with the outcome, we log-transformed the years of childhood depression to demonstrate that our method can take into account nonlinear relationships.
Mediators for cumulative CM
In fitting the hybrid latent mediation model, we used adult SES and functional limitations as two intermediate risk factors linking cumulative CM and depressive symptoms. Adult SES was measured as a reflective latent variable based on adult years of education, income, and family net wealth modeled as effect indicators. As with childhood SES, we provide supplemental tables for models 1–3 as well as for the mediation model with adult SES measured by a single-item, family net wealth (Online Supplemental Tables 3 and 4). Functional limitations were measured in 2004 by self-reports of having difficulty with any of the following activities: walking one block; climbing one flight of stairs; lifting or carrying 10 pounds; picking a dime up off the ground; stooping, kneeling, or crouching; and pushing or pulling large objects. We treat functional limitations as a composite latent variable.
Cumulative resources
In applying our method to model cumulative resources, we focused on the following protective factors in adulthood: high SES, mastery, social support, being married, religious attendance, and being physically active.
High SES was measured as a reflective latent variable based on years of education, annual income (eight discrete categories, from “0–10 K” to “>150 K”), and family net wealth (nine discrete categories, from “≤0” to “>500 K”) modeled as effect indicators. Mastery was assessed as a reflective latent variable based on how much the individual agreed with the following statements: “I could do anything I set my mind to,” “I usually find a way to succeed,” “get what I want is in my own hands,” “the future depends on me,” and “I can do the things that I want to do.” Social support was assessed with three items regarding spouse, children, and friends: (a) “How much do they really understand the way you feel about things?” (b) “How much can you rely on them if you have a serious problem?” and (c) “How much can you open up to them if you need to talk about your worries?” Response choices for each item range from 1 (not at all) to 4 (a lot). We estimated a composite latent variable for social support. Religious attendance was measured as an observed variable with a five-point scale ranging from 1 (“less than once a month”) to 5 (“daily”). We measured physical activity as a reflective latent variable based on the frequency of vigorous, modest, and light physical activities, each of which ranged from 1 (never) to 5 (everyday).
In the summed score model and the composite latent model, all continuous protective variables were recoded dichotomously. Specifically, both the SES index and the mastery index were split into quintiles, with individuals in the fifth quintile coded 1 for having high SES or high mastery and all others coded 0. Religious attendance was dichotomized into “less than once a month” and “at least once a month.” We created a global dichotomous measure for physical activity by combining participants’ self-reported frequencies of doing light, moderate, and vigorous physical activities over the last 12 months, with 1 representing the individual having done any type of physical activity “at least once a week or more” and 0 otherwise.
Control variables
We adjust for age (in years), gender, and race (black and Hispanic) in all models.
The SEM Approach
The composite latent model (i.e., the aforementioned model 2) constitutes the core of our method. The hybrid latent model, the hybrid latent mediation model, and the combined latent interaction model are further extensions based on the composite latent model. The basic structure of the composite latent model can be written as:


where

where Xp is the vector of pth observed effect indicators for the latent CM domain construct
η could also be measured as composite latent variables:

where Xp is the vector of pth observed indicators for the latent CM domain construct
The latent cumulative CM variable (C) is an exact linear combination of the seven CM variables and can be interpreted as the weighted sum of the seven specific CMs. As an intermediate variable linking specific CMs to a specific health outcome Y, cumulative CM variable (C) represents a unique way of summarizing both the weighted sum of the distinct type of CM and the differential impact of each CM on that particular outcome. The weights (wj) represent the differential contributions of the various CM variables to a latent cumulative C, and
In the conventional summed score model, the jth CM variable
As an extension to the hybrid latent model, the hybrid latent mediation model can be summarized in these equations:




Building on equations 1 and 2 from the hybrid latent model above, in equation (4),
Finally, the combined hybrid latent model simultaneously estimates both the cumulative CM and the cumulative protective factor as two different composite latent constructs and interacts these two constructs in predicting a health outcome:
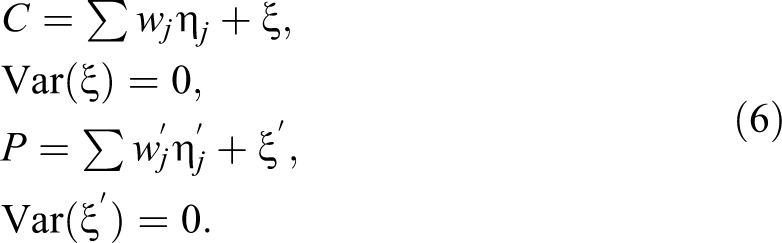

Parallel to equation (1), which estimates the latent composite construct for cumulative CM, equation (6) estimates an additional composite construct for the cumulative protective factor P. Equation (7) relates cumulative CM (C) and cumulative protective factor (P) to a health outcome Y, in which
Results
Table 2 shows the descriptive statistics for variables used in the models for the cumulative impact of CM as well as for the list of protective factors used in the models for the cumulative impact of protective factors. Childhood exposure to different types of misfortune varies considerably. For example, the majority of the sample had a parent who smoked (68 percent), a sizable portion of the sample had a father with low education (22 percent), but only a small portion of the sample reported parental physical abuse (7 percent), disability (4 percent), parent substance abuse (1.6 percent), poor health (1.1 percent), and childhood depression (1.7 percent). Notably, the dichotomous measures for the CM variables conceal much information on severity and duration of these experiences, which can otherwise be captured by observed and/or latent continuous measures. Those appear in Table 2 are the dichotomous measures. Turning to protective factors, 24 percent of the weighted sample have adult high SES, 23 percent have high levels of mastery, 13 percent have high social support, almost 70 percent are married, 75 percent attend religious services at least once per month, and about 33 percent participate in physical activity at least once per week. As with the CM variables, dichotomizing the protective factors obscures detailed information about the level and amount subjects’ possess or experience. The means and standard errors of the continuous variables, which are used in the more advanced models, appear below the dichotomous variables in Table 2.
Weighted sample characteristics, Health and Retirement Study 2004–2012.
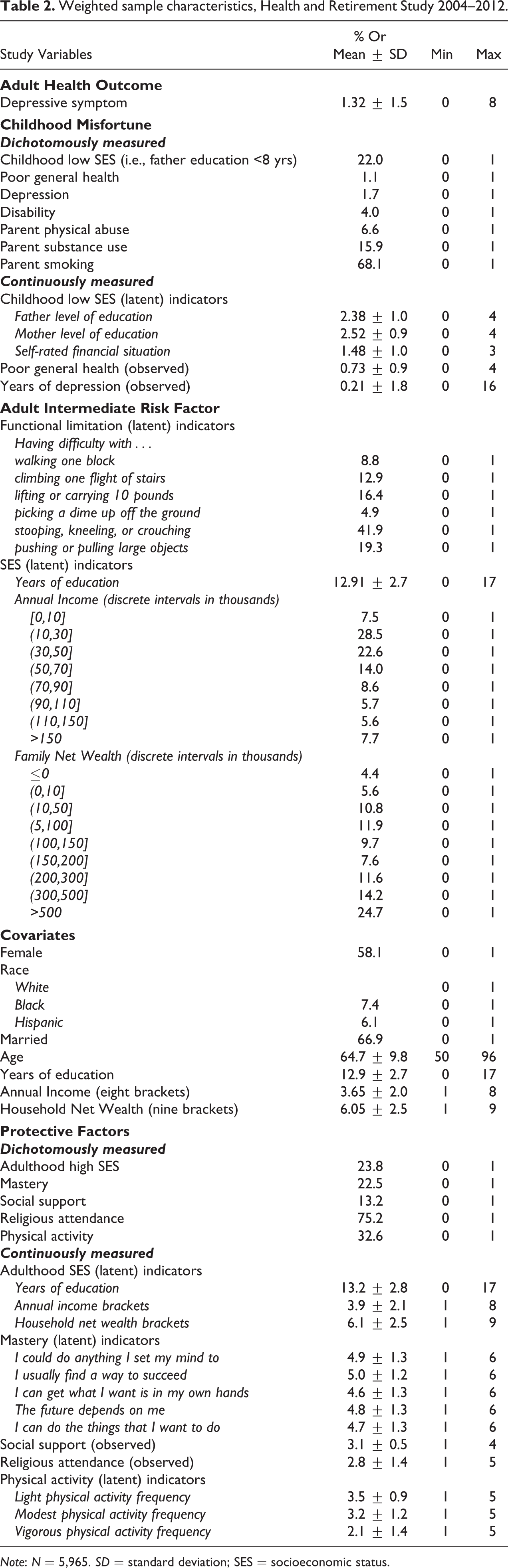
Note: N = 5,965. SD = standard deviation; SES = socioeconomic status.
Modeling Cumulative CM
Table 3 summarizes the goodness-of-fit statistics and the estimated coefficients for cumulative CM from the conventional summed score model, the composite latent model, and the hybrid latent model for depressive symptoms, respectively. From the conventional model to the hybrid latent model, the R2 increases from .08 to .10 to .12; the Akaike information criteria (AIC), Bayesian information criteria (BIC), and sample size–adjusted BIC decrease (e.g., sample-size adjusted Bayesian information criteria [SA-BIC] decreases from 14,775 to 14,644 to 14,560). This pattern indicates that our method, by allowing the individual CM variables to differentially contribute to the cumulative CM variable and by incorporating more refined measures for individual CM variables in the cumulative CM variable, improves model fit and explains an increasing amount of variance in depressive symptoms in adulthood. The improved estimation is also evident in the increased association between cumulative CM and depressive symptoms (from .12 to .18 to .21). A standard deviation change in the traditional summed score measure is associated with a .12 standard deviation increase in depressive symptoms and our measure in the hybrid latent model with a .22 standard deviation increase.
Model Fit Indices and the Standard Regression Coefficients for Cumulative Childhood Misfortune Predicting Adult Depressive Symptoms, Health and Retirement Study.
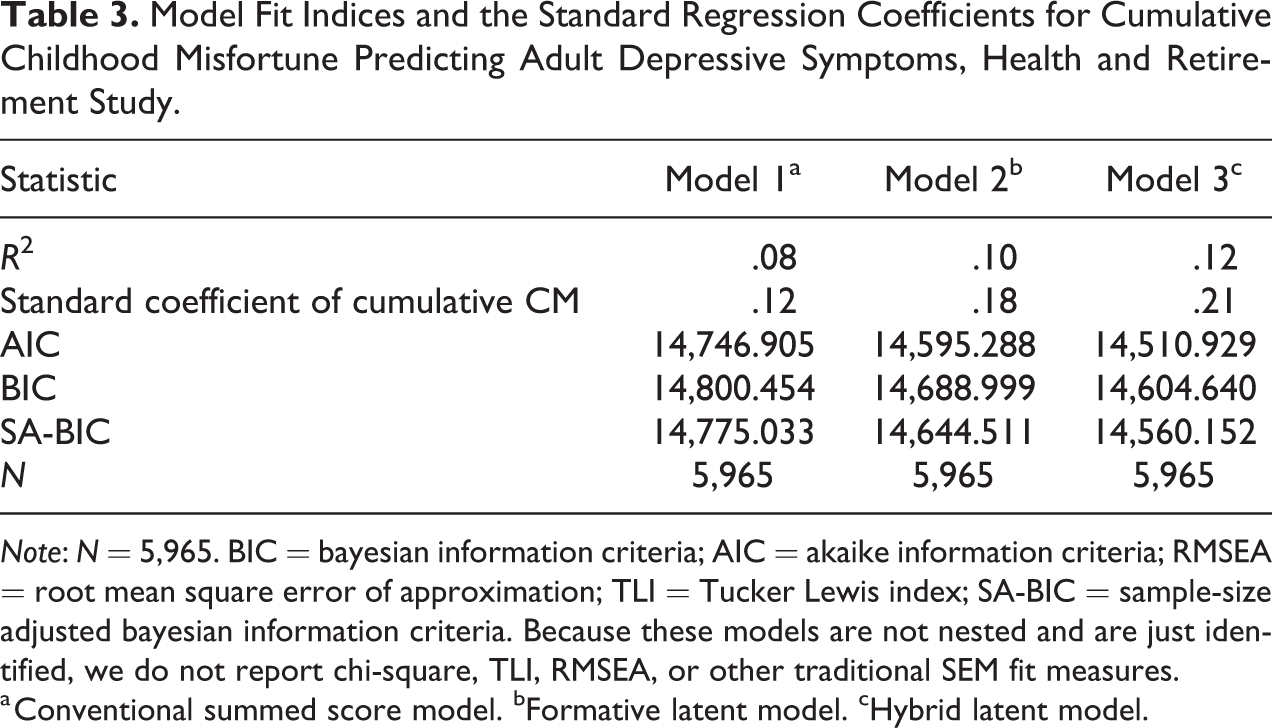
Note: N = 5,965. BIC = bayesian information criteria; AIC = akaike information criteria; RMSEA = root mean square error of approximation; TLI = Tucker Lewis index; SA-BIC = sample-size adjusted bayesian information criteria. Because these models are not nested and are just identified, we do not report chi-square, TLI, RMSEA, or other traditional SEM fit measures.
a Conventional summed score model. bFormative latent model. cHybrid latent model.
Table 4 presents standardized regression coefficients for cumulative CM from the hybrid latent model predicting depressive symptom. The left two columns in the table present the individual weights (wj in equation [1]) and associated standard errors for each CM variable in forming the cumulative CM construct. The right two columns present direct effects on depressive symptoms from the cumulative CM variable. Indirect effects from individual CM variables can be calculated as the product of the weights for individual CM (wj) and the coefficient for the cumulative CM (
To demonstrate the flexibility of this approach and because SES is often treated as a causal latent variable rather than a reflective latent variable, we present additional results treating childhood SES as a composite latent variable as well as an observed single-item variable. Online Supplemental Table 1 summarizes the coefficients of different indicators (i.e., father’s education, mother’s education, and self-rated financial situation) contributing to the composite construct. Online Supplemental Table 2 presents standardized regression coefficients for cumulative CM from a hybrid latent model that treats childhood SES as a composite latent variable. The only notable difference between the supplemental analytic results and the original results is a smaller coefficient of childhood low SES in predicting cumulative CM when treated as composite. This difference is due to childhood low SES representing different constructs in each specification. In the original model specification, childhood low SES is a reflective latent construct representing the shared cause for low father/mother education and financial difficulty, while in the supplemental model specification, the latent variable is a linear combination of the indicators, which are mainly driven by father’s education and less so by mother’s education and perceived financial situation. Online Supplemental Table 3 present results from models 1–3 with childhood SES treated as a single-item variable. The coefficient for the cumulative CM variable is smaller in this specification compared to either reflective or composite because of the reduced amount of information on childhood SES. The mediation model in Online Supplemental Table 4 shows a similar pattern of results to the main mediation model, except that adult SES does not mediate the impact of childhood SES on depressive symptoms, which is, again, not unexpected given the reduced amount of information and further demonstrative of the benefits of the latent approach. All supplementary models follow the same pattern of higher R2, higher coefficient of CM and better model fit across the successive specifications.
Results From Hybrid Latent Model for Cumulative Childhood Misfortune (CM) and Adult Depressive Symptoms, Health and Retirement Study.a
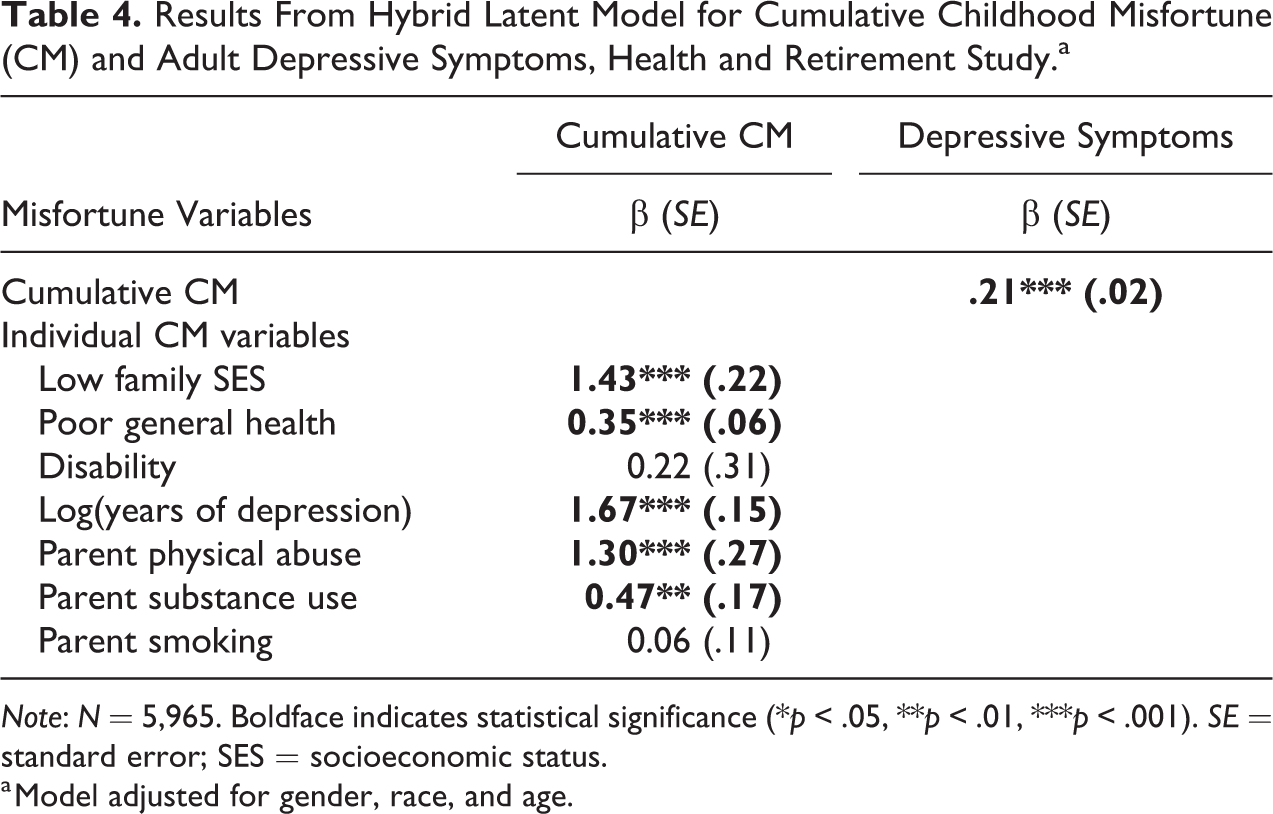
Note: N = 5,965. Boldface indicates statistical significance (*p < .05, **p < .01, ***p < .001). SE = standard error; SES = socioeconomic status.
a Model adjusted for gender, race, and age.
Modeling Cumulative Resources
We replicated the above modeling approaches on the health impact of cumulative protective factors. Table 5 summarizes goodness-of-fit statistics from the summed score model, the composite latent model, and the hybrid latent model. Similar to the pattern in the cumulative CM models, the hybrid latent model that incorporates more refined measures and allows distinct weights for different types of protective factors has the best model fit (as evidenced by the highest R2 and lowest AIC, BIC, and SA-BIC), followed by the composite latent model and the summed score model.
Model Fit Indices and the Standard Regression Coefficients for Cumulative Protective Factor Predicting Adult Depressive Symptoms, Health and Retirement Study.
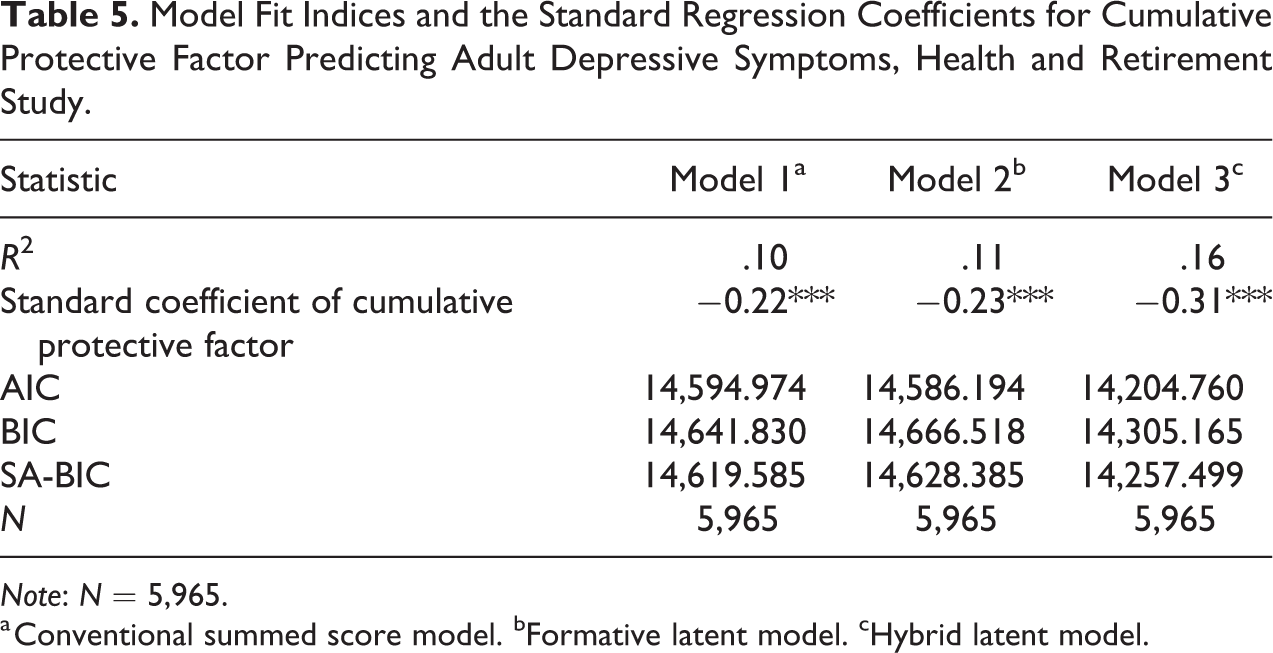
Note: N = 5,965.
a Conventional summed score model. bFormative latent model. cHybrid latent model.
Table 6 presents results from the hybrid latent model for depressive symptoms and cumulative protective factors. The left two columns in Table 6 present individual weights and associated standard errors for each protective factor in forming the cumulative protection construct as estimated by the hybrid latent model. The right two columns present the direct effects of cumulative protective factors on depressive symptoms. Indirect effects from individual protective factors can be calculated as the product of the weight for individual protective factors and the coefficient for the cumulative protective factors. While all protective factors are negatively associated with depression, the level of the associations vary from −.05 (religious attendance, calculated as .16 × −.31) to −.21 (physical activity, calculated as .69 × −.31). These results suggest that certain factors (e.g., mastery, social support, and physical activity) matter more than others (e.g., religious attendance) in the accumulation of protection against depressive symptoms.
Results From Hybrid Latent Model for Cumulative Protective Factor and Adult Depression, Health and Retirement Study, Health and Retirement Study.a
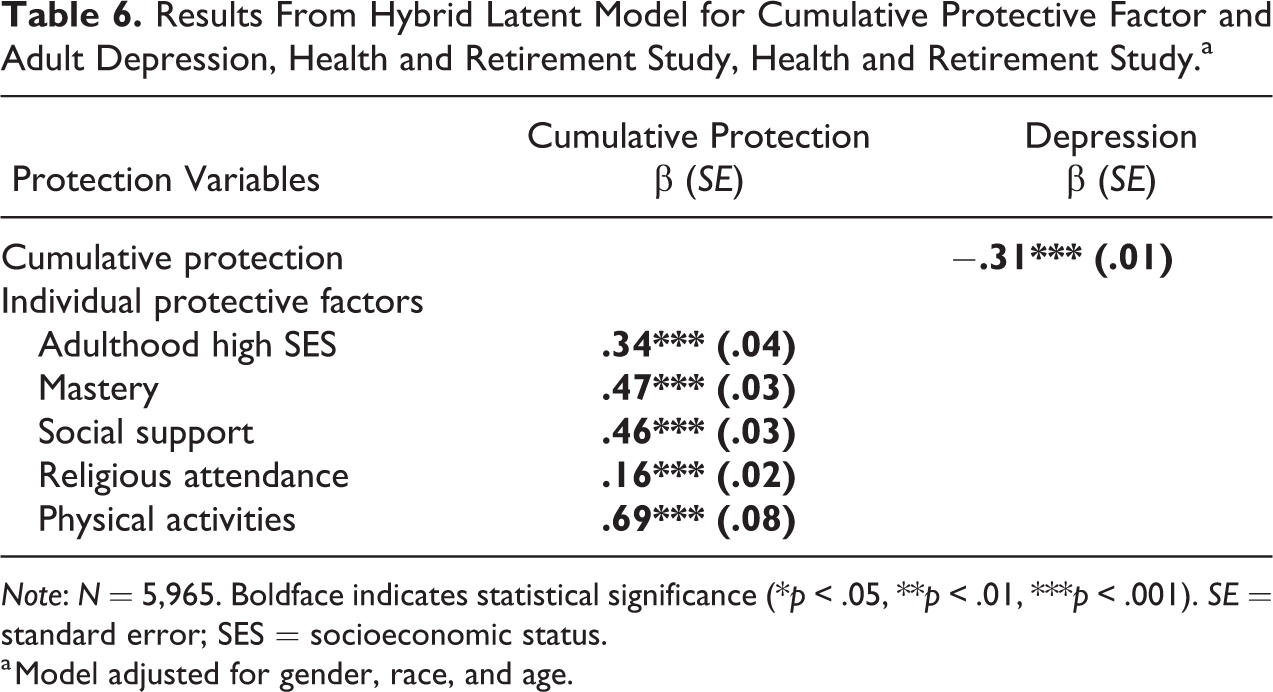
Note: N = 5,965. Boldface indicates statistical significance (*p < .05, **p < .01, ***p < .001). SE = standard error; SES = socioeconomic status.
a Model adjusted for gender, race, and age.
Hybrid Latent Mediation Model for CM
Allowing various CMs to have distinct contributions to the additive misfortunate variable paves the way to study the mechanisms linking different CMs to health outcomes as well as mechanisms linking cumulative CM to health outcomes. This task can be accomplished with a further extension of the models discussed above, that is, adding a mediator between the cumulative CM variable and the health outcome. Table 7 summarizes the total effects of the cumulative CM and the individual CM variables on depressive symptoms as well as their indirect effects through adult SES and adult functional limitations as estimated in two hybrid latent mediation models. Cumulative CM was not associated with depressive symptoms either via adult SES or adult functional limitations, but among individual CM variables, low family SES was associated with depressive symptoms via the adult SES pathway. None of the other CM variables were linked to depressive symptoms through either pathway.
Results From Hybrid Latent Mediation Model for Cumulative Childhood Misfortune (CM) and Adult
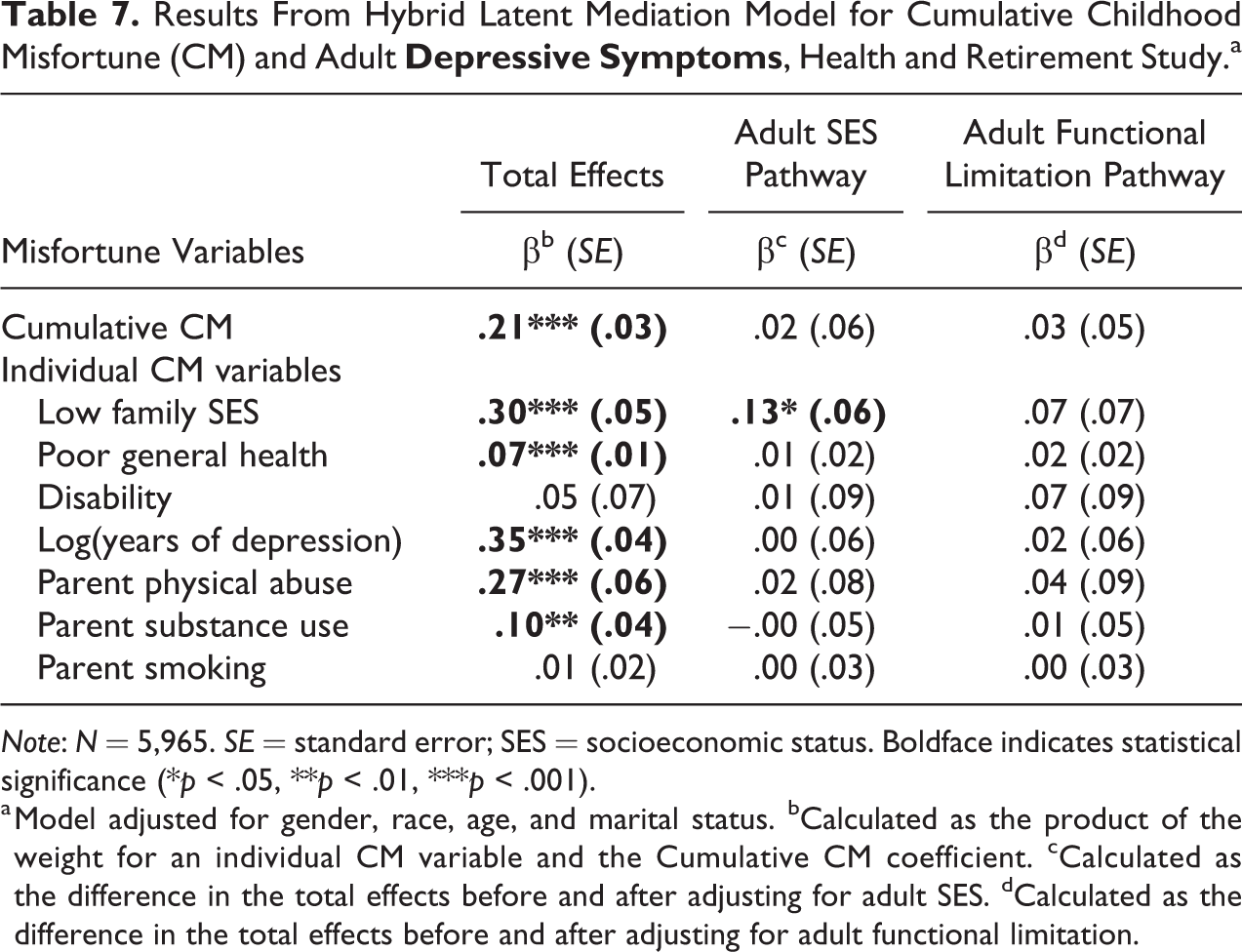
Note: N = 5,965. SE = standard error; SES = socioeconomic status. Boldface indicates statistical significance (*p < .05, **p < .01, ***p < .001).
a Model adjusted for gender, race, age, and marital status. bCalculated as the product of the weight for an individual CM variable and the Cumulative CM coefficient. cCalculated as the difference in the total effects before and after adjusting for adult SES. dCalculated as the difference in the total effects before and after adjusting for adult functional limitation.
Combined Latent Model
Lastly, we estimated a combined latent model in which we interacted a composite latent construct of cumulative CM with a composite construct of cumulative protective factors. This model provides a tool to explicitly test the hypothesis that the accumulation of resources can attenuate the negative consequences of cumulative CM. Results from the combined latent model (Table 8) show that cumulative protective factors indeed offset the negative impact of cumulative CM on adult depressive symptom, as indicated by the significant negative coefficient for the interaction term (β = −.06, p < .001). Meanwhile, the buffering effect from any individual protective factor can be represented as the product of its weight and the coefficient for the interaction term between cumulative CM and cumulative protective factors. As such, the model results enable us to see that all protective factors significantly buffer the negative health consequence of cumulative CM, which are mainly driven by five of the seven types of misfortunes. The strength of the buffering effect varies across the protective factors, with physical activity having the strongest buffering effect, followed by mastery and social support.
Interaction of the Cumulative Childhood Misfortune and Cumulative Protection in Predicting Adult
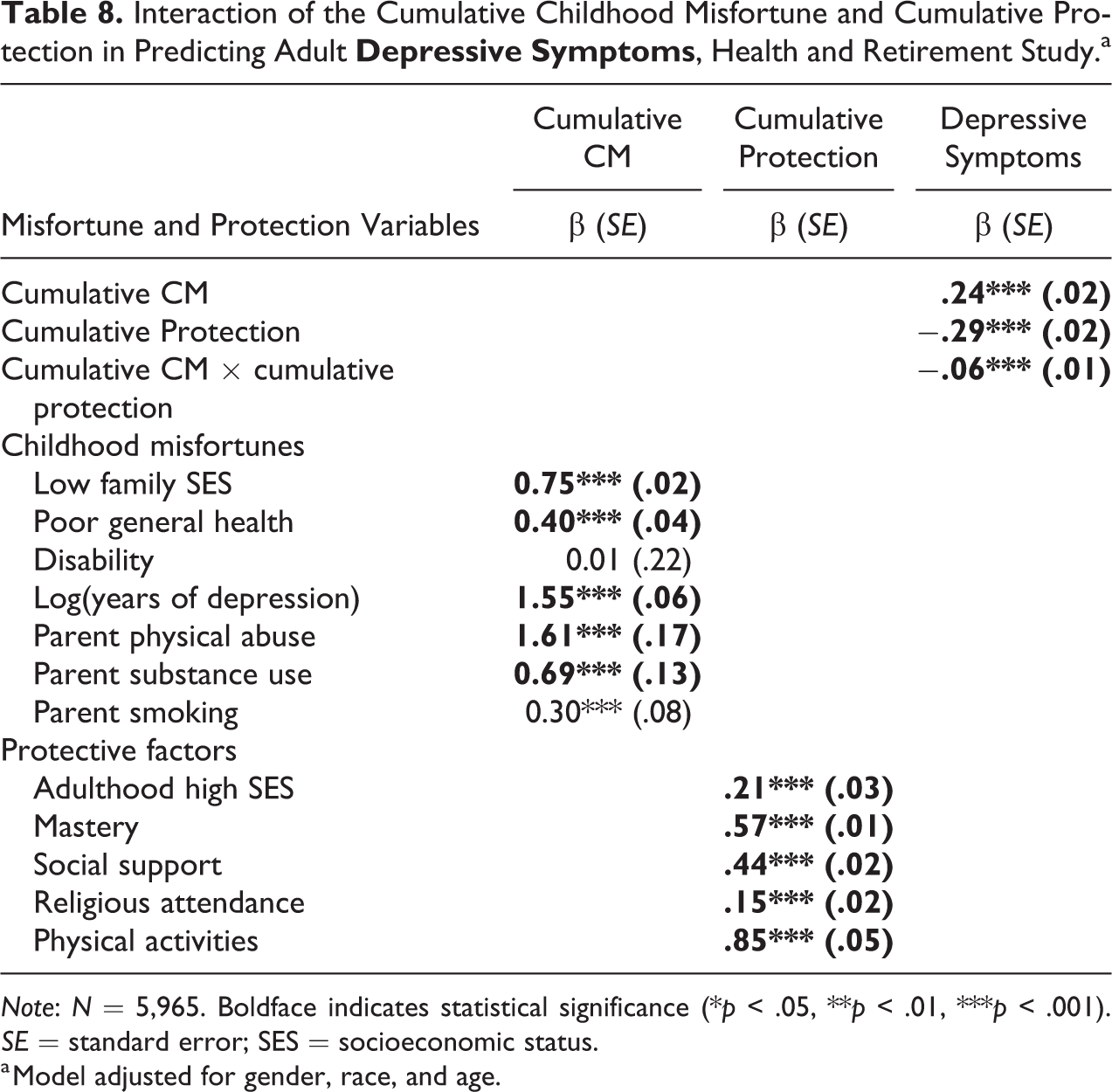
Note: N = 5,965. Boldface indicates statistical significance (*p < .05, **p < .01, ***p < .001). SE = standard error; SES = socioeconomic status.
a Model adjusted for gender, race, and age.
Discussion
Evaluating the cumulative impact of CM on health outcomes is a focal interest for life course studies on the consequences of early life exposures, but the widely practiced approaches of using a summed score of available epistemic CM indicators may be misleading because of unfounded assumptions about individual CMs carrying the same weight in contributing to later-life health risks. Drawing on the SEM framework and particularly the composite measurement model, we develop an alternative approach to estimate the health impact of cumulative CM while allowing each individual CM to be differentially weighted based on its association with the health outcome. This method can further incorporate flexible CM measures including scales, latent variables, and intermediate risk factors. It can also be applied to explicitly test hypotheses involving interactions, which paves the way for future theoretical developments.
To demonstrate the advantages of the SEM approach, we developed a composite latent model and a hybrid latent model and compared the performance of these models with that of the conventional summed score model. The composite latent model, in which the cumulative CM is measured as a latent composite construct based on seven CM variables, constitutes the core of our method. Unlike a summed score, this composite latent construct of CM represents a weighted index that allows different CM variables to have distinct weights in modeling the cumulative impact on a specific health outcome. It thus allows us to simultaneously estimate both the cumulative CM impact and the differential impact of individual CM variables. The hybrid latent model further incorporates flexibly measured CM variables including reflective and composite latent variables, continuous observed variables, a log transformed observed variable, and several dichotomous variables.
A comparison of goodness-of-fit indices from models 1 to 3 suggests that the hybrid latent model has the best model fit and explains the highest amount of variance in the health outcome (i.e., depressive symptoms), followed by the composite latent model and the summed score model last. Additional analyses (not shown here) examining the impact of cumulative CM on a different health outcome (i.e., BMI) reveal the same pattern, that is, the composite/hybrid latent models outperform the conventional summed score model in terms of model fit and explanatory power. The generally better performance of the SEM modeling approach is because we can simultaneously account for the additive impact, the differential impact, and capitalize on better measures of the individual CMs.
If each CM domain is measured dichotomously and weighted equally (as in the summed score model), the coefficient for the cumulative CM (i.e., the additive variable) is .12. For each standard deviation increase of misfortune, depressive symptoms increase by .12 standard deviations. When the domains are allowed to be measured more flexibly and weighted differentially (as in the hybrid latent model), the coefficient for the cumulative CM rises to .21. The hybrid latent model clearly illustrates a cascade of differentially weighted CM domains, with childhood depression having the strongest influence, followed by low family SES, parental physical abuse, parent substance use, and poor health last, with childhood disability and parent smoking having no impact at all. This model also illustrates that we can incorporate a nonlinear relationship into the index. In this case, childhood depression relates to depressive symptoms in a nonlinear way, with its impact gradually leveling off as the number of years of childhood depression increases. The differential contributions of distinct CM variables to the cumulative impact on the health outcome thus calls into question the interpretability and validity of the estimates of the summed CM score in the conventional model.
A further advantage of our approach is that it can be extended to include mediators in assessing the association between cumulative CM and health outcomes. In conjunction with the differential weights for individual CM variables, a mediator between cumulative CM (as a composite latent construct) and a health outcome allows us to evaluate whether different types of CM share the same mechanisms in influencing health. For example, results from the hybrid latent mediation model suggest that adult SES is a mechanism through which childhood low family SES contributes to depressive symptoms in adulthood. Yet, none of the other CM variables contribute to depressive symptoms through either the adult SES pathway or the functional limitation pathway and neither pathway mediates cumulative CM. By revealing these patterns, our approach challenges the assumption of the summed score approach that all CM variables factor into a health outcome via the same mechanisms and demonstrate that a more intricate approach to studying mediation will be rewarded with uncovering more nuanced patterns.
Finally, the SEM approach can be applied to studying the accumulation of both risks and resources, as well as the interaction of these dual accumulation processes over the life course on health outcomes. The hybrid latent model for the health impact of cumulative protective factors fits the data much better and explains more variance in depressive symptoms than the summed score model. Moreover, by combining the hybrid latent model for cumulative CM and cumulative protective factors, we explicitly evaluate the interaction between the two types of accumulation and find that cumulative protective factors attenuate the deleterious health impact of cumulative CM. In sum, based on our findings, we conclude that the summed score approach may be useful in preliminary analyses or as a screening mechanism but that there are better ways to model additive CM to advance our understanding of cumulative impact, illuminate pathways for how early negative exposures influence adult health, and elaborate the interactions between the accumulation of positive and negative exposures over the life course.
As with any method, there are limitations. It is likely that we failed to observe those who experienced the greatest amounts of misfortune because some died before entering the HRS and others were not able to be sampled because they were institutionalized or otherwise unavailable due to extremely poor health, addiction, and so on. While our model could incorporate propensity scores or instrumental variables, we cannot adjust for subjects who died before being recruited into the study or who were institutionalized. Not including these subjects means our estimates are likely underestimated, but how to adjust for that underestimation is a question for future study.
Another limitation is the retrospective nature of the data upon which this method relies. Few studies track participants from childhood through older adulthood. As such, many studies that model the accumulation of any kind of advantage or disadvantage rely on retrospective data and recall bias can be an issue. Further, due to identification issues, we were unable to include latent variables with causal indicators in this model. We will continue to work on this issue in the future with the goal of devising a way to identify such a model. Lastly, because this model is so flexible, it requires that researchers decide whether individual CMs should be treated as reflective latent variables, composite latent variables, continuous variables, dichotomies, and so forth. To guide those decisions, we recommend using as much information as is available and using extant literature and available tests as guides.
The approach developed in this study has several major advantages. First, it is based on more realistic assumptions about the relationship of various CMs to distinct health outcomes. Consistent with the recommendation of Appleton et al. (2017), it is incumbent on investigators to examine differential weighting of CM indicators when creating constructs. Although it is possible that differential weighting of indicators is not needed, the SEM approach developed here enables the investigator to test the plausibility of the equal-weighting assumption. The SEM approach also provides a tool for understanding distinct mechanisms linking different CMs and different health outcomes.
Second, it is relatively easy to implement. The basic component of the approach, namely, the composite measurement model, is an established method that has been used in multiple subfields of social sciences (Bollen and Bauldry 2011; Coltman et al. 2008; Diamantopoulos and Winklhofer 2001; Edwards and Bagozzi 2000). Similarly, second-order latent models are also well established. Commercial statistical packages for implementing this model are readily available. We used Mplus 8.2 in our analysis, but multiple equation models with latent variables are now available in other software such as Stata 16 and R 3.6 as well.
Third, the model can be extended further by incorporating various lower-order measurement models for CM constructs to capitalize on available data, deal with measurement error, or reduce data dimensions. For instance, if one has information on the reported severity and duration of negative exposures, the composite model can incorporate such information efficiently.
Fourth, this method could facilitate studies on the temporal accumulation of a single risk factor such as poverty. Studies on the cumulative exposure to childhood poverty, for instance, report that repeated poverty exposure causes more health risks than no exposure or transitory exposure (Kimberlin 2011), but the simple additive approach is often used to model cumulative economic hardship, which either sums up or averages the times/occasions children spend in poverty (Bane and Ellwood 1983; Chen, Martin, and Matthews 2007; Korenman and Miller 1997; McLeod and Shanahan 1996; Smith et al. 1997). That approach assumes that poverty exposure at different times carries the same risk for particular health outcomes and thus obscures the importance of the timing of exposure. This problem could be overcome using the methods developed here, which would allow poverty exposure at different times to differentially influence the outcome.
Fifth, this model can incorporate multiple outcomes. Although we used depressive symptoms in this exposition, one could easily model multiple outcomes simultaneously, such as heart disease, diabetes, and cancer. Lastly, this new method has wide applicability. It can facilitate the study of cumulative effects in many areas of study such as life course epidemiology, criminology, gerontology, child development, and developmental psychology, regardless of whether the accumulation is in childhood, adulthood, or over the life course. The study of cumulative CM and many other types of accumulation variables across different areas of research will benefit from conceptualization, inclusion, and measurement of new types of exposures, which will be facilitated, encouraged, and enabled by the SEM approach.
Supplemental Material
Supplemental Material, Supplemental_Tables_7062019_R2 - Evaluating the Cumulative Impact of Childhood Misfortune: A Structural Equation Modeling Approach
Supplemental Material, Supplemental_Tables_7062019_R2 for Evaluating the Cumulative Impact of Childhood Misfortune: A Structural Equation Modeling Approach by Sarah Mustillo, Miao Li and Kenneth F. Ferraro in Sociological Methods & Research
Footnotes
Acknowledgment
We thank Shawn Bauldry and the anonymous reviewers for helpful feedback on this manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This work was supported by National Institute on Aging R01AG043544 (PI:Kenneth Ferraro).
Supplemental Material
Supplemental material for this article is available online.
Note
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.