
Abstract
Scrub typhus is re-emerging in India. We describe an outbreak of 45 cases from our tertiary care center in north India. This outbreak included city dwellers who had no history of travel to hilly areas. The classical feature of scrub typhus, the eschar, was also noted rarely in these patients. The changing epidemiology of scrub typhus should be kept in mind while attending patients with acute febrile illness.
Keywords
Introduction
Scrub typhus is an acute febrile syndrome caused by Orientia tsutsugamushi and transmitted by the bite of the chigger of the mite belonging to the family Trombiculidae of genus Leptotrombidium. 1 It is distributed mainly in the rural areas of the ‘tsutsugamushi triangle’ limited by northern Japan, eastern Australia, and eastern Russia that includes the Indian subcontinent, western Russia, China, and the Far East. 2 People affected are mainly those engaging in agricultural, recreational, or military activities that bring them in contact with mite infested habitats, or travelers returning from endemic regions. Scrub typhus seems to be remerging in India with several states reporting outbreaks in the last few years.3–10 Here, we describe an outbreak from our hospital and summarize the picture of scrub typhus epidemics in India in the past few years.
Short report
Acute phase sera of a total of 1,053 patients with acute febrile illness suspected to be suffering from scrub typhus were subjected to Weil Felix agglutination test. A titre of >320 was recorded in 110 patients’ sera, 51 of which were tested by a commercial IgM ELISA kit (InBios International, Seattle, WA, USA). IgM ELISA was found positive in 45 of these patients who were considered positive. A detailed clinical history of these patients was obtained. The majority of the patients were from the state of Haryana, followed by Himachal Pradesh, Chandigarh, and UP (Figure 1). Around 62.2% (28/45) were male patients and 37.8% (17/45) female patients; 55.5% (25/45) patients were from the pediatric age group. The maximum number of cases presented during the month of September (Figure 1). The commonest complaint was fever present in all the patients (45/45; 100%), followed by vomiting (27/45; 60%), hepatomegaly (22/45; 48.9%), headache (17/45; 37.8%), dyspnea (16/45; 35.5%), chills (5/45; 11.1%), altered sensorium (10/45; 22.2%), and splenomegaly (9/45; 20%). The commonest combinations of symptoms were fever with shortness of breath or vomiting or headache. Thrombocytopenia was present in 28.9% (13/45) patients, while eschar was present only in two (4.4%) patients (forearm and abdomen). Twenty-three (51%) patients developed complications, the most common of which was meningoencephalitis (27%), followed by acute respiratory distress syndrome (11%), acute renal failure (9%), and shock (4%). There was mortality in two (4.4%) patients, both in the pediatric age group.
Trend of scrub typhus outbreak and state wise distribution of cases (y-axis represents number of cases). Tricity: Chandigarh, Mohali and Panchkula.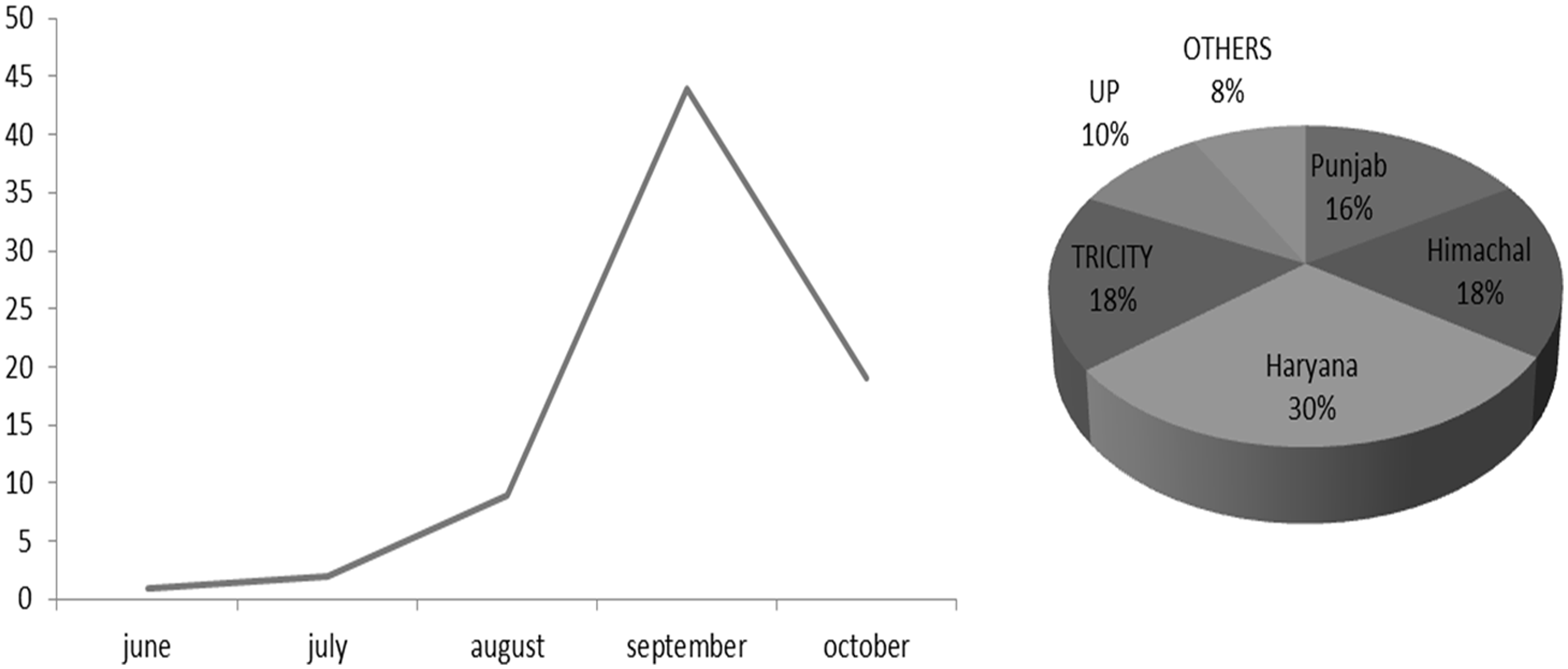
Demographic, clinical, and laboratory parameters of recent outbreaks of scrub typhus reported from India.

NA, not available.
All our patients had fever for duration of more than 1 week which helped to differentiate it from viral fever which is common during the rainy season. Many patients also had non-specific complaints pertaining to the respiratory, gastrointestinal, or central nervous system. The number of patients who presented with altered sensorium and presence of rashes were consistent with other recently reported outbreaks. Symptoms like cough and myalgia were reported in a fewer number of patients as compared to other studies. 7 Eschar, once thought to be an important sign of scrub typhus, was present only in two patients. The rarity of presentation with an eschar is increasingly being recognized in Southeast Asian patients. Hence, even in the absence of eschar in a case of undifferentiated fever, physicians should be on an alert for scrub typhus, especially in residents of/or travelers returning from south Asia. The mortality was low with only two deaths reported which could be attributed to prompt institution of doxycycline (azithromycin was used in three pregnant women).
Among the gold standard tests for the diagnosis of scrub typhus, ELISA was used in this outbreak. Other confirmatory assays like indirect immunofluorescence antibody test and indirect immunoperoxidase test are not available in our country and isolation of the organisms in animal or cell cultures is limited by lack of containment facility as well as expertise in handling these high-risk group pathogens. The most commonly used diagnostic assay in developing countries is Weil Felix agglutination test, which is a heterophile antibody test. Though less sensitive and specific, a high titre of ≥320 in a single sample is considered to be diagnostic. This test is economical and easy to perform hence useful for screening, however, should be used only in conjunction with a confirmatory test.
In conclusion, there is an increasing prevalence of scrub typhus in India and it is now occurring in areas where it was not known previously. Of particular importance is the disease occurring in residents of urban areas of the plains who have no history of travel to hilly areas. Physicians should therefore be more aware of this entity and should consider it in the differential diagnosis of acute febrile illness even when the presentation of patients is not classical of scrub typhus.
Footnotes
Declaration of conflicting interests
None declared.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.