
Abstract
Leptospirosis, Q fever, scrub typhus, and murine typhus are endemic zoonotic diseases in southern Taiwan that often present as acute undifferentiated febrile illness. We retrospectively compared epidemiological, clinical, laboratory, and outcome characteristics of leptospirosis (n = 41) and rickettsial infections, including Q fever, scrub typhus, and murine typhus (QSM; n = 103), in Kaohsiung City from 2013 to 2024. Leptospirosis occurred mainly during rainy and typhoon seasons and was associated with myalgia, gastrointestinal symptoms, jaundice, conjunctival suffusion, hepatic and renal dysfunction, leukocytosis, elevated C-reactive protein, and higher rates of acute kidney injury and shock. QSM occurred year-round, with eschar characteristic of scrub typhus, while prolonged activated partial thromboplastin time and relative bradycardia were more common in QSM. QSM generally showed a milder clinical course, particularly Q fever. Distinct clinical and seasonal patterns may facilitate early differentiation and risk stratification in endemic areas.
Introduction
Zoonotic febrile illnesses remain a major public health and clinical challenge in tropical and subtropical regions, where multiple pathogens co-exist and present with overlapping clinical manifestations. In southern Taiwan, leptospirosis, Q fever, scrub typhus, and murine typhus are endemic and frequently encountered.1,2 Early differentiation between these infections is crucial, as disease severity, complication profiles, and management strategies differ substantially.
Most previous studies have focused on pathogen-specific characteristics or pairwise comparisons between individual zoonotic infections.3,4 However, in real-world clinical practice, Q fever, scrub typhus, and murine typhus are often considered together because of their similar exposure histories, 2 early non-specific symptoms, and shared diagnostic challenges. During the initial stage of illness, clinicians in endemic regions frequently rely on clinical judgment and limited laboratory data while awaiting confirmatory microbiological results.
To reflect this clinical reality better, we conceptualized Q fever, scrub typhus, and murine typhus as a unified clinical syndrome (QSM) and compared this syndrome with leptospirosis. Using this syndrome-based framework, we aimed to (1) compare the epidemiological, clinical, laboratory, and outcome profiles of leptospirosis and QSM; (2) examine whether these zoonotic infections represent a spectrum of disease severity; and (3) identify practical clinical features that may assist frontline clinicians in early differentiation in endemic settings. We sought to provide clinically relevant insights applicable to tropical and subtropical regions where these infections are prevalent.
Materials and methods
We conducted a retrospective observational study of hospitalized patients diagnosed with leptospirosis or Q fever, Scrub typhus, and murine typhus (collectively referred to as QSM) at Kaohsiung Medical University Hospital and Kaohsiung Municipal Siaogang Hospital, in Kaohsiung, Taiwan, during the period 2013–2024.
Eligible cases were defined as patients aged >18 years with a confirmed diagnosis based on compatible clinical manifestations and laboratory confirmation through serological assays.
Clinical data were retrieved from the electronic medical record system and included demographic characteristics (age, sex), clinical features (viz. fever, myalgia, nausea, diarrhoea, relative bradycardia), laboratory parameters (e.g., leucocyte and neutrophil counts, activated partial thromboplastin time [aPTT], serum creatinine, blood urea nitrogen), and major complications (e.g., acute kidney injury, jaundice, shock).
The study protocol was reviewed and approved by the Institutional Review Board of Kaohsiung Medical University Hospital, Kaohsiung, Taiwan (approval number: KMUHIRB-E(I)-20250249). Given the retrospective nature of the study, the Institutional Ethics Committee of Kaohsiung Medical University Hospital waived the requirement for written informed consent.
A confirmed case of leptospirosis was defined as either a fourfold rise in microscopic agglutination test (MAT) titres between acute and convalescent serum samples or a MAT titre ≥1:400 in a single serum specimen. 5
Q fever was diagnosed in patients with fever and compatible serological evidence, including either a fourfold rise in Phase II IgG titres between acute and convalescent samples or the presence of significant Phase II IgM titre (≥1:50) by indirect immunofluorescence assay, as confirmed by the Taiwan Centers for Disease Control.
Scrub typhus was diagnosed using PCR analysis of blood samples or an IFA (indirect immunofluorescene assay) detecting antibodies against Orientia tsutsugamushi. Diagnostic criteria required either a fourfold increase in total antibody titres to O. tsutsugamushi strains (Karp, Kato, Gilliam) in paired sera or a significant IgM titre ≥1:80.
Murine typhus was diagnosed based on compatible clinical features (e.g., acute febrile illness) and serologic evidence, defined as either a fourfold rise in IgG titres between paired sera or an IFA IgM titre ≥1:80 against Rickettsia typhi. 2 All diagnostic methods were performed at the laboratories of the Center for Disease Control and Prevention, Taiwan.
Thrombocytopenia was defined as a platelet count of <14 × 109/L. Acute hepatitis was characterized by serum aminotransferase levels ≥1.5 times the upper limit of normal (AST ≥60 IU/L or ALT ≥78 IU/L), and hyperbilirubinemia was defined as a total bilirubin (bilirubin-T) concentration ≥23.9µmol/L. 6 Jaundice (icterus) was defined as a bilirubin-T level ≥34.2 µmol/L. Severe hepatitis was defined as markedly elevated aminotransferases, with AST or ALT ≥1000 IU/L. 7 Gastrointestinal bleeding was identified by the presence of melaena or haematochezia. Acute kidney injury (AKI) was diagnosed according to the KDIGO criteria: an increase in serum creatinine ≥ 26.5µmol/L within 48 h; an increase of ≥1.5-fold from baseline within 7 days; or urine output <0.5 mL/kg/h for more than 6 consecutive hours. 8
Categorical variables were compared using the chi-square test or Fisher's exact test, while continuous variables were analyzed with the independent-samples t test or Mann–Whitney U test. Multivariate logistic regression analysis was performed to identify independent predictors differentiating leptospirosis from QSM infections. A two-tailed p value <0.05 was considered statistically significant. All analyses were conducted using SPSS version 25 software (IBM Corp., Armonk, NY, USA).
Results
From 2013 to 2024, 41 leptospirosis cases and 103 QSM cases (13 Q fever, 65 scrub typhus, and 25 murine typhus) were reported in Kaohsiung City. As illustrated in Figure 1, leptospirosis cases were predominantly concentrated in the rainy and typhoon seasons (July to September), whereas QSM cases mainly occurred from May to December.

Monthly distribution of the 103 cases of Rickettsial infection (scrub typhus, murine typhus) and Q fever, and the 41 cases of leptospirosis, 2013–2024.
Comparison of clinical symptoms is summarized in Table 1. Male sex was more prevalent in the leptospirosis group. Fever was universal in both groups. Leptospirosis patients more frequently presented with myalgia, diarrhoea, nausea, vomiting, general weakness, and conjunctival suffusion. Petechiae were also observed only in leptospirosis. In the QSM group, relative bradycardia was more frequent. All eschars were observed exclusively in patients with scrub typhus.
Comparison of clinical characteristics between leptospirosis and QSM (Q fever, scrub typhus, & murine typhus) in Kaohsiung city, 2013–2024.

*Fisher's exact test.
Laboratory findings
Laboratory data comparison is shown in Table 2. Microscopic haematuria was more prevalent in leptospirosis, which demonstrated significantly higher levels of AST and leucocyte counts. Moreover, neutrophil predominance and lymphopenia were also characteristic findings. However, QSM cases exhibited a significantly higher frequency of prolonged activated partial thromboplastin time than leptospirosis. In multivariate logistic regression analysis, no variables were found to differentiate leptospirosis significantly from QSM.
Comparison of clinical laboratory data between the leptospirosis and the QSM in Kaohsiung city, 2013–2024.
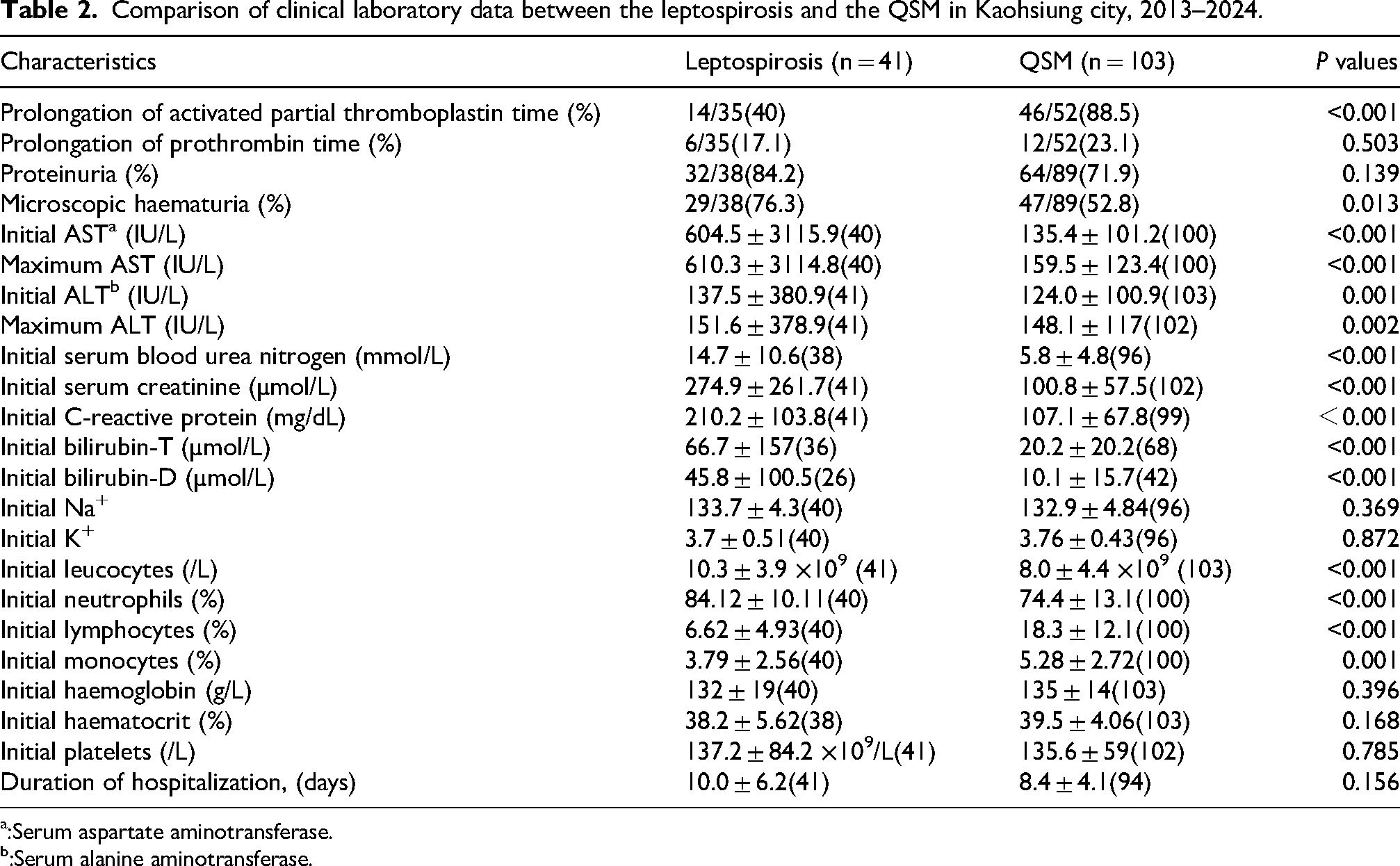
:Serum aspartate aminotransferase.
:Serum alanine aminotransferase.
Complications
As shown in Table 3, leptospirosis was associated with significantly higher rates of complications compared with QSM. Likewise, acute kidney injury, shock, jaundice, and gastrointestinal bleeding were all significantly more common. Hepatitis was common in both groups but slightly higher in QSM. Among QSM subgroups, scrub typhus patients showed the highest complication rates, followed by murine typhus, whereas Q fever patients generally exhibited the mildest disease manifestations.
Comparison of the complications between leptospirosis and QSM in Kaohsiung, 2013–2024.
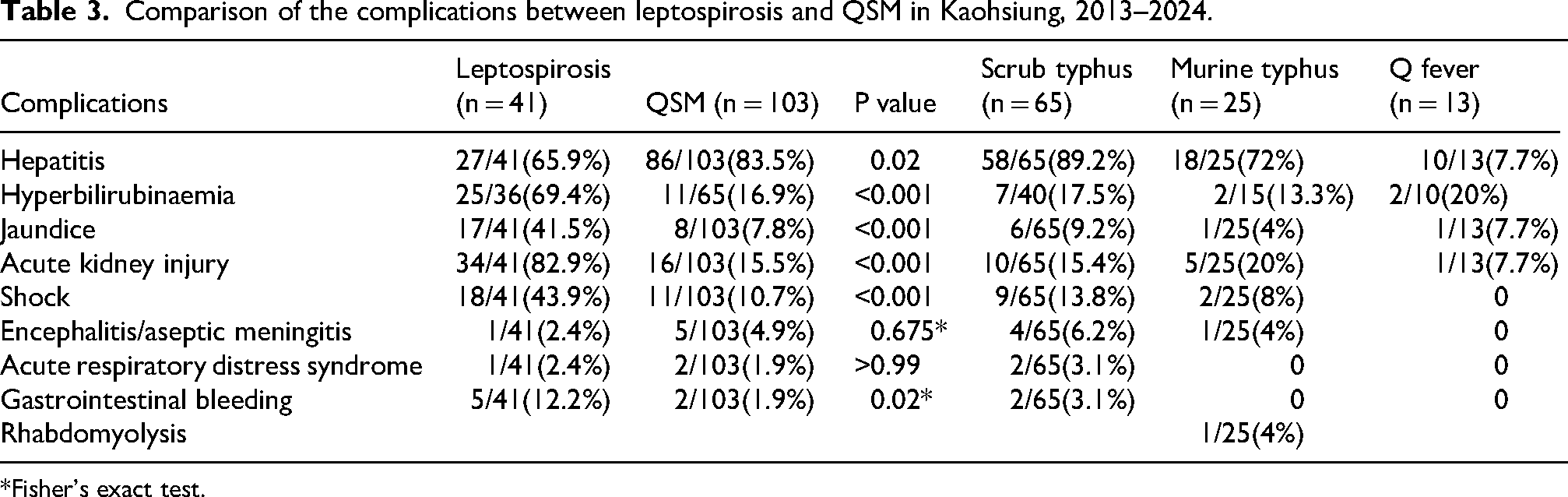
*Fisher's exact test.
Co-infections
Co-infections were observed in both groups but differed in spectrum. Among patients with scrub typhus, various concurrent infections were identified, including two cases of Escherichia coli urinary tract infection, one of Streptococcus group G bacteraemia, one of Candida albicans urinary tract infection, one of cytomegalovirus (CMV) IgM, one with Epstein–Barr virus (EBV) IgM, and one with Mycoplasma pneumoniae IgM positivity. One patient with Q fever presented with methicillin-resistant Staphylococcus aureus (MRSA) bacteraemia. Among patients with murine typhus, one case of Escherichia coli urinary tract infection was observed. Among patients with leptospirosis, one case of Neisseria gonorrhoeae bacteremia was identified. Other concurrent infections were nosocomial in origin, including Candida albicans, Enterococcus faecalis urinary tract infection, and Acinetobacter baumannii infection.
Discussion
In our study, we found distinct differences between leptospirosis and QSM in terms of disease severity, laboratory abnormalities, complication profiles, and seasonal distribution.
Leptospirosis consistently represented the severe end of the spectrum, with higher rates of organ dysfunction, complications, and intensive care utilization. In contrast, Q fever was associated with milder clinical courses, while scrub typhus and murine typhus showed intermediate severity. This gradient highlights the heterogeneous nature of zoonotic infections and underlines the importance of early risk stratification in endemic settings.
Distinct differences in clinical manifestations were observed between the two diseases. Myalgia, nausea, vomiting, diarrhoea, conjunctival suffusion, and petechiae were significantly more common in leptospirosis, whereas eschar remained the hallmark clinical feature of scrub typhus. 9 Nevertheless, a substantial overlap in non-specific symptoms, including fever, headache, and general weakness, highlights the diagnostic challenges encountered in regions where these pathogens are endemic.
Laboratory findings further supported this distinction. While non-specific abnormalities such as thrombocytopenia were observed across all groups, prolonged activated partial thromboplastin time (aPTT) was more frequently associated with QSM, as was relative bradycardia. Their combined presence may serve as a useful bedside clue favouring QSM over leptospirosis, particularly during the early stage of illness when confirmatory testing is not yet available.10,11 Such pattern recognition may assist clinicians in guiding initial diagnostic considerations and empirical management.
Co-infections were identified3,9,12 and distinct patterns were observed between the two groups. In QSM, Mycoplasma pneumoniae and Epstein–Barr virus (EBV) IgM positivity were predominantly heterogeneous and mainly identified through serologic testing, suggesting background exposure or immune modulation rather than true concurrent acute infection. In contrast, co-infections observed in leptospirosis, such as Neisseria gonorrhoeae or Acinetobacter baumannii infection, were more frequently associated with severe illness and healthcare-related infections. These findings indicate that the clinical significance of co-infections may vary according to the underlying zoonotic disease and should therefore be interpreted within a broader clinical context.
Seasonal variation further distinguished the two groups. Leptospirosis showed a strong association with the rainy season,1,13,14 consistent with environmental exposure to contaminated water sources, whereas QSM exhibited a more evenly distributed temporal pattern.
The treatment of leptospirosis and QSM differs mainly by disease severity. Doxycycline is the first-line therapy for Q fever, scrub typhus, and murine typhus, with good efficacy and rapid clinical response, although prolonged treatment may be needed in chronic Q fever. 6 In contrast, leptospirosis requires a severity-based approach: mild cases may be treated with doxycycline or amoxicillin, whereas severe cases often need intravenous penicillin G or ceftriaxone. 15 Supportive care, including renal replacement therapy and intensive care, is crucial in severe leptospirosis. 1 Overall, while doxycycline is generally sufficient for QSM, leptospirosis often requires both antimicrobial treatment and aggressive supportive management because of its more severe systemic involvement.
Our study has several limitations. First, the relatively small sample size, especially within the leptospirosis and Q fever subgroups, limited the statistical power to detect subtle differences and may restrict the generalizability of the findings. Second, not all patients with leptospirosis were tested for Q fever, scrub typhus, or murine typhus. Third, long-term outcomes and treatment responses were not systematically evaluated, precluding conclusions regarding prognosis or therapeutic effectiveness.
Overall, we emphasize the value of a syndrome-based approach to zoonotic febrile illnesses in endemic areas. By framing Q fever, scrub typhus, and murine typhus as a unified clinical syndrome and contrasting it with leptospirosis, we provide a pragmatic framework for early differentiation and risk assessment. This approach may be especially useful for frontline clinicians practicing in tropical and subtropical regions, where rapid clinical decision-making is required before definitive microbiological confirmation.
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.