
Abstract
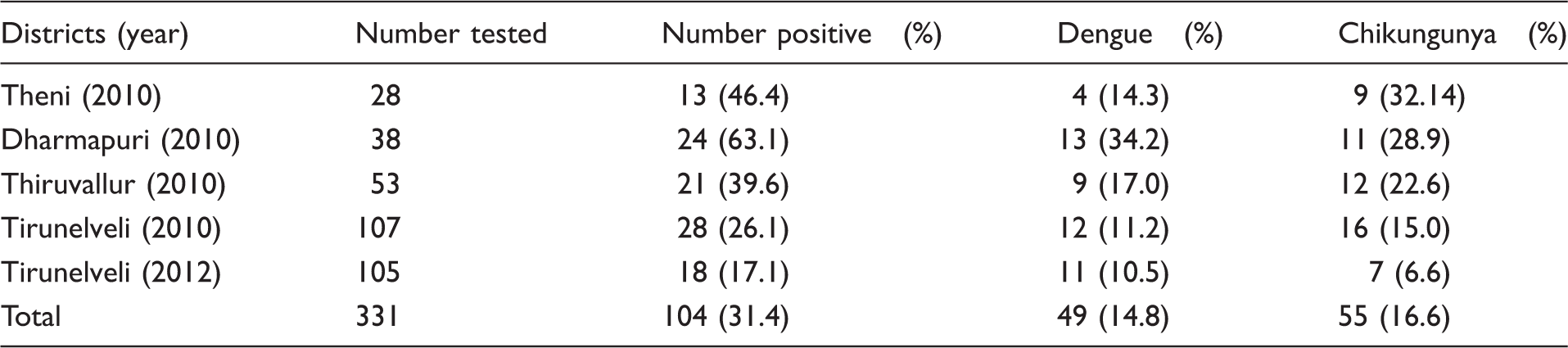
Following a report of dengue outbreak from January 2010 to 2012 in the Tirunelveli, Theni, Dharmapuri and Thiruvallur districts of Tamil Nadu state, India, an investigation was carried out. The study was to demonstrate the probable presence of Chikungunya viral antibodies in patients clinically suspected of dengue fever. Out of 331 samples analysed, dengue viral antibodies were observed in 14.8% (n = 49) of patients, while 16.6% (n = 55) were positive for Chikungunya viral specific IgM antibodies. In the four districts surveyed, patients found positive for Chikungunya were found to be higher than dengue. The clinician should consider Chikungunya in the differential diagnosis of dengue-like infection appearing in the community.
Introduction
There are 390 million dengue infections reported per year worldwide. 1 Acute infection of dengue virus (DENV) in adults may cause dengue fever (DF) characterised by biphasic fever, head ache, eye pain, myalgia, arthralgia, prostration, rash, lymphadenopathy and leukopenia. Chikungunya virus (CHIKV) causes an acute infection characterised by fever, polyarthralgia, headache and myalgia clinically. 2 Chikungunya is a self-limiting and non-fatal acute illness, whereas dengue may lead to severe complications. 3 In Asia, the CHIKV affected areas overlap with dengue fever-endemic areas, 4 providing opportunities for mosquitoes to be infected with both viruses. Mourya et al. 5 isolated CHIKV in Aedes aegypti mosquitoes and showed the maintenance of a low level of CHIKV in the Pune district. Aedes aegypti is sensitive to changes in temperature and available moisture. Their number was found to decrease during dry and cool seasons, but increased when the wet season begins. 6 The clinical signs and symptoms of Chikungunya and dengue seem to be similar and difficult to distinguish without laboratory investigations. Severe arthralgia, fever, headache and vomiting are the commonest symptoms of both. In the past 5 years, Tamil Nadu state, south India has registered a steep rise in deaths due to dengue and Chikungunya. While dengue cases increased from 707 in 2007 to 8482 in 2012, Chikungunya cases also increased from 45 to 5018 during the same period. Serology proved to be useful in confirming Chikungunya infection.
The present investigation is a prospective study to demonstrate the presence of Chikungunya antibody in samples of patients clinically suspected of having dengue fever. A suspected dengue case is defined as an acute febrile illness characterised by frontal headache, retro-ocular pain, muscle and joint pain, and rash. 7
Material and methods
The study was carried out during 2010–2012 in the Tirunelveli, Theni, Dharmapuri and Thiruvallur districts of Tamil Nadu state, south India following reports of a dengue outbreak. Suspected cases with clinical features of dengue infection (age range, 1–60 years) were enrolled in the Government hospital and primary health centres of affected areas were investigated. With the consent of the patient, 2 mL of blood was collected by the health authorities. The serum was separated and ELISA testing was carried out for dengue as well as Chikungunya virus specific IgM antibodies 8 using ELISA Kits (obtained from National Institute of Virology, Pune, India) as per the manufacturer’s instruction. Patients’ clinical histories were also collected after obtaining prior consent.
Results
District-wise dengue and Chikungunya antibody positivity during the outbreak investigation in the years 2010 and 2012.
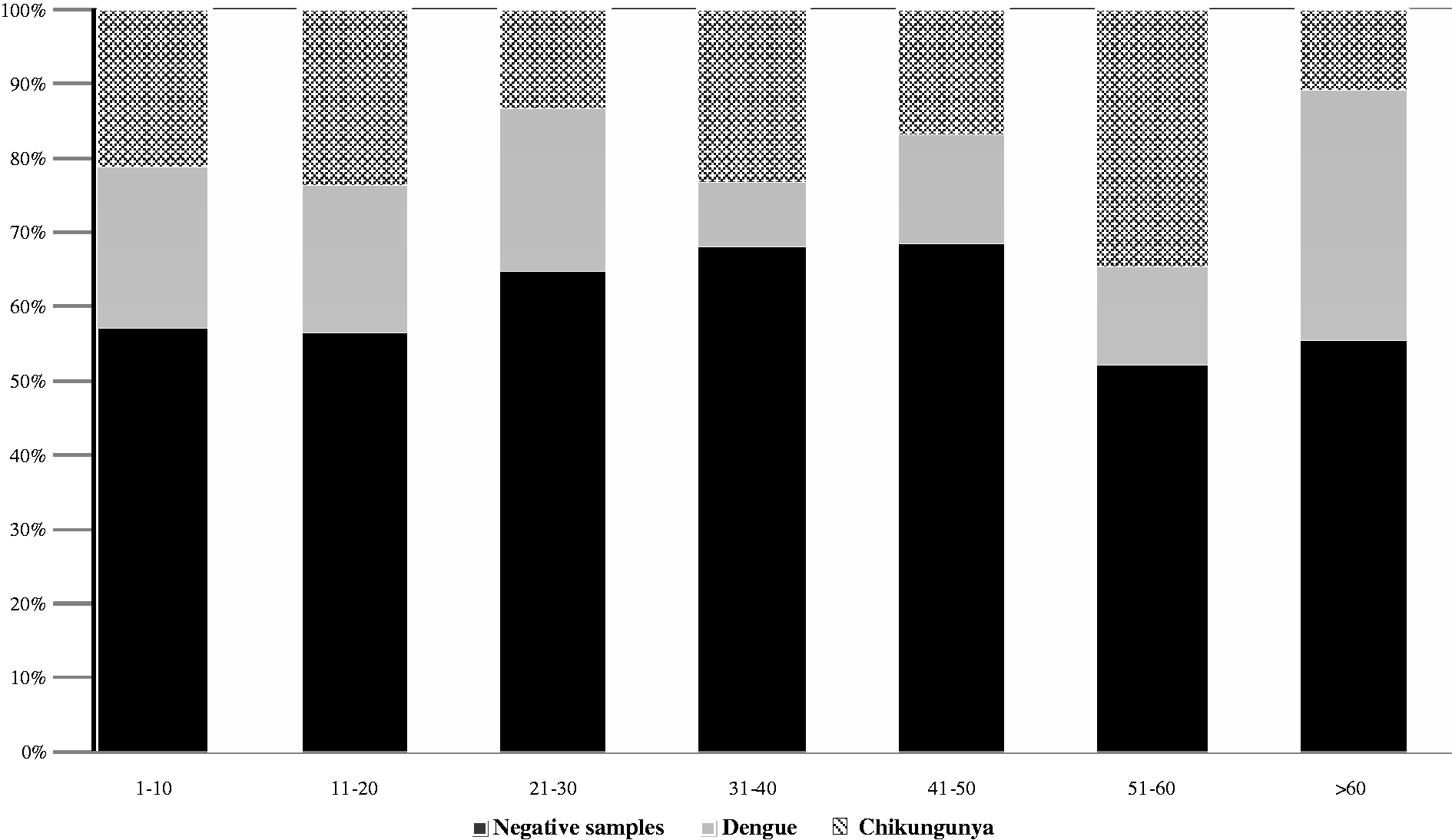
Age group-wise distribution of dengue and chikungunya antibody positivity during an outbreak in Tamil Nadu (in 2010).
The major clinical features elicited in the patients were fever, vomiting, rashes, retro-orbital puffiness, myalgia and arthralgia. Fever was elicited in all age groups invariably. The symptoms, viz, myalgia and arthralgia were noticed in 80.06% and 83.99% of adults, respectively, while these were not reported among children. Vomiting was observed in 32.02%, while purpuric rashes were observed in 3.02%. Retro-orbital puffiness was seen in 38.07%. There is no difference noticed in the symptoms among the patients who were positive for DENV/CHIKV IgM antibodies.
Discussion
Active Chikungunya virus circulation was evident in the community during the outbreaks. Laboratory diagnosis was supportive in differentiating Chikungunya from dengue virus infection, which is hyper endemic in many parts of Tamil Nadu state. As observed in the present investigation, it has been postulated that 9 many cases of dengue virus infection are misdiagnosed and the incidence of CHIKV infection is much higher than reported. In the present investigation, all four districts surveyed recorded higher number of patients with CHIKV antibodies. The symptoms of CHIKV infection are quite similar to those caused by many other infectious agents in the endemic areas. One particular difficulty in identifying CHIKV infection is its overlapping distribution with dengue viruses.
In the present study, there were no dual positives which shows there is no non-specific booster response to infection that is actually due to another virus. The IgM is specific to one virus either DENV or CHIKV. The cost of testing per sample in Indian rupees is 150 each against DENV and CHIKV.
Due to the non-availability of natural source of water there was an acute water scarcity in the study area and storage of potable water became a regular practice of the local residents. This condition could have created the proliferation of the vector (Aedes aegypti) in the outbreak area. During this investigation, a community-based approach that promoted interventions to prevent breeding of dengue vectors was explained, to the target stakeholders within the target communities. This strategy has been proved effective earlier 10 in order to reduce the density of dengue vectors substantially.
The clinician should consider CHIK fever in the differential diagnosis of dengue-like infection appearing in the community. Timely detection of DENV and CHIKV should prompt vector control measures to curtail further outbreaks, as there is no specific treatment for these infections. Utilising the recently developed diagnostic kits to detect dual infections (DEN and CHIK IgM antibodies), and the multiplex PCR diagnosis of viral RNA, could be additional tools to hasten diagnosis.
Footnotes
Acknowledgements
The authors are thankful to the Director General, Indian Council of Medical Research for facility and encouragement. They express their sincere thanks to Dr. BK Tyagi, Director, CRME, (ICMR), Madurai for his complete support and encouragement for carrying out this study successfully. They also thank Dr. IP Sunish, Scientist C, RMRC (ICMR), Andaman and Nicobar Islands, India for his valuable suggestions.
Declaration of conflicting interests
All the authors have seen the manuscript and approve it for submission. The authors have no competing interest in the publication of the manuscript to declare.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.