
Abstract
We report a 26-year-old man of neurobrucellosis who presented with intermittent fever and headache for 2 years, sensori-neural hearing loss with cerebellar ataxia. He responded well to a combination of antimicrobials with significant clinical improvement.
Introduction
Brucellosis is caused by infection in humans by some species of bacteria of genus Brucella. These infect domestic animals such as cows, sheep, goats, camels, horses, pigs, cats and dogs. The disease is transmitted to humans by direct contact with infected animals, through cuts and abrasions or inhalation of aerosols, or by ingestion of unpasteurised milk or milk products. The varied clinical manifestations make the diagnosis challenging. A high degree of clinical suspicion is required. Even though it is a rare complication, neurobrucellosis, if not recognised early and promptly treated, causes significant morbidity.
Case report
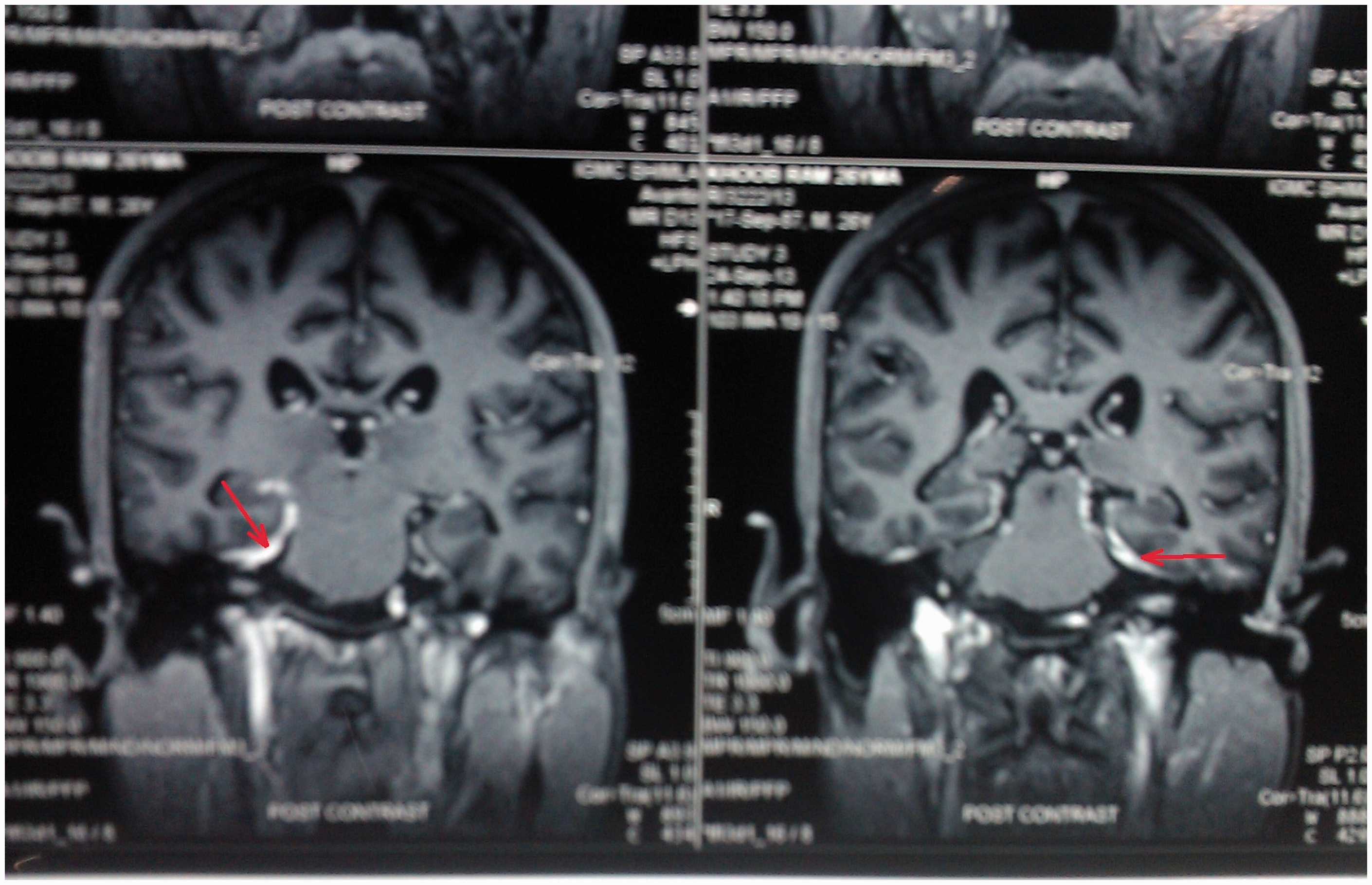
A 26-year-old shepherd presented with an intermittent mild to moderate grade fever for 2 years, associated with diffuse headache and bilateral painless progressive diminution of hearing for 9 months’ duration with significant weight loss. One year previously, he developed progressive swaying while walking, needing support for the last month. He raised domestic animals for a living and admitted to having consumed unpasteurised dairy products. He had been empirically treated twice with anti-tubercular therapy. Previous CSF examination showed a leucocyte count of 372/mm3 (lymphocytes: 92%), protein 270 mg/dl and glucose 1.94 mM. On examination he was afebrile with profound bilateral hearing loss. His central nervous system examination revealed scanned speech, impaired coordination, wide based ataxic gait, gaze evoked nystagmus but no meningeal signs. The rest of his systemic examination was non-contributory. During his hospital stay, he again developed fever. The full blood count, renal, liver and thyroid function tests were normal. Anti-nuclear antigen, HIV and VDRL were non-reactive. Standard agglutination tests on CSF revealed Brucella agglutination titres of 1:1280. The CSF analysis showed 250 white cells/mm3 (70% lymphocytes), protein 400 mg/dl, glucose 1.78 mm and adenosine deaminase 18.0 IU/L (norm <10 IU/L). No organisms were demonstrated by Zeil-Neelson, Gram or India ink stains. CSF culture for M. Tuberculosis by MGIT-960 was negative. An MRI brain scan revealed generalised atrophy of bilateral cerebral and cerebellar hemispheres (Figure 1) with enhancement of meninges along the basal cistern (inter-peduncular fossa, ambient cisterm and pre-pontine region) on injection of contrast (Figure 2).
T2-weighted brain MRI of the patient showing diffuse cerebral and cerebellar atrophy with prominence of pre-pontine cistern and supra-cerebellar cistern. Brain MRI (post contrast) of patient showing meningeal enhancement.
Treatment with doxycycline 200 mg/day, rifampicin 450 mg/day and streptomycin 1 mg/day was commenced. Streptomycin was stopped after 2 weeks but doxycycline and rifampicin were continued for 6 months. The patient began to improve over 2 weeks. On discharge after 3 weeks, he was afebrile, without headache; his gait had also improved but he still needed support walking. Apart from his deafness, which persisted, he made a good recovery at 6 months.
Discussion
Neurobrucellosis may develop at any stage of the disease and can affect any part of the nervous system with variable manifestations. Neurologic involvement of the central nervous system is detected in 3–5% of the patients with brucellosis.1,2 It may manifest as meningoencephalitis, inflammatory peripheral radiculitis/neuritis (sometimes mimicking Guillain-Barre syndrome 3 ), diffuse cerebral involvement, papilloedema or papillitis without other focal features, intracranial haemorrhage, neuropsychiatric syndromes or a combinations of these.1,4 Headache, blurred vision, loss of hearing and confusion are common smptoms. 1 Vestibulo-acoustic neuritis is the most common peripheral affectation. 5 It may manifest itself during the acute phase of the disease, possibly due to the direct effect of organisms invading nervous tissue, to the release of circulating endotoxins, or to the immunologic and inflammatory reactions of the host. 6 A hospital-based study of brucellosis in India found neurobrucellosis in 18.86% and ataxia in 0.57%. 7 In the post-antibiotic era mortality due to neurobrucellosis is in the range of 0–5%, but permanent neurological deficit especially deafness is common. 6
Footnotes
Declaration of conflicting interests
None declared.
Funding
This study received no specific grant from any funding agency in public, commercial or not-for-profit sectors.