
Abstract
Melioidosis is the disease caused by the soil and water bacterium, Burkholderia pseudomallei. Our study aimed to delineate its genitourinary manifestations. Over a 10-year period (2006–2016), 20 adults with culture-confirmed genitourinary melioidosis were identified. The patients were all men with a mean age of 45.3 ± 12.3 years. The common risk factors were diabetes mellitus (65%) and alcoholism (25%); a majority of patients (90%) had chronic melioidosis. Most had disseminated disease (n = 17) and 55% were bacteraemic. The prostate was the organ most frequently involved (60%, n = 12), followed by the kidney, bladder and seminal vesicles. Diagnosis was established by blood and urine cultures and imaging. Patients were successfully treated with ceftazidime intensive therapy followed by eradicative therapy, with surgical debridement and guided aspiration, when deemed necessary. There was one case fatality and no relapses. Melioidosis is an important differential to be considered in chronic genitourinary infections in the appropriate setting.
Keywords
Introduction
Melioidosis is the clinical disease caused by Burkholderia pseudomallei. 1 Infection is acquired by ingestion, inhalation and inoculation, and the spectrum of disease ranges from fulminant septicaemic disease, subacute infection to the indolent chronic form. 2 Clinical manifestations are protean and involvement of practically every organ system has been described. The disease is endemic to South East Asia and Northern Australia and recent studies show that India is at risk for a surge of cases. 3 The disease is often under-recognised, owing to diagnostic challenges posed by a low index of suspicion and inadequate laboratory support, even in endemic regions.
Genitourinary involvement has been previously reported with melioidosis. The prostate is the most common organ of involvement and is described in 2.5% patients and up to 18% of men with melioidosis.4,5 Other organs of involvement include the kidney, bladder and seminal vesicles, but this entity is poorly described. 6 We undertook this study to delineate the genitourinary manifestations of melioidosis.
Materials and methods
Our study was undertaken in a tertiary care referral hospital in South India between January 2006 and January 2016. We included all adult patients aged ≥18 years with culture-proven melioidosis with involvement of the genitourinary system. Data regarding patient demographics, clinical characteristics, laboratory and radiological parameters, and outcomes were retrospectively reviewed. Acute and chronic disease were defined based on disease duration of >2 months or >2 months, respectively. Patients were said to have disseminated disease if there were two or more organs of involvement or one organ involvement with positive blood culture. 2
Continuous variables were summarised using mean and standard deviation (SD) when normally distributed and median and interquartile range (IQR) when not normally distributed. Categorical variables were analysed using proportions. The study was approved by the Institutional Review Board and Ethics Committee. Data were analysed using SPSS v20. (IBM Corp Released 2011; IBM SPSS Statistics for Windows, Version 20.0; IBM Corp., Armonk, NY, USA).
Results
Baseline characteristics of patients with genitourinary melioidosis.

Mean ± SD.
†Median (IQR).
Among patient with genitourinary melioidosis, chronic disease was observed more frequently than acute (18 vs. 2). Patients were symptomatic for a median duration of six months (IQR = 3–7 months) and fever was the most common presenting symptom. Symptoms specific to the genitourinary system included dysuria, frequency, flank pain and retention. Most patients (85%) had disseminated disease. In three patients, the diagnosis was established by obtaining pus cultures from a non-genitourinary source.
Organ involvement and outcomes of patients with genitourinary melioidosis.
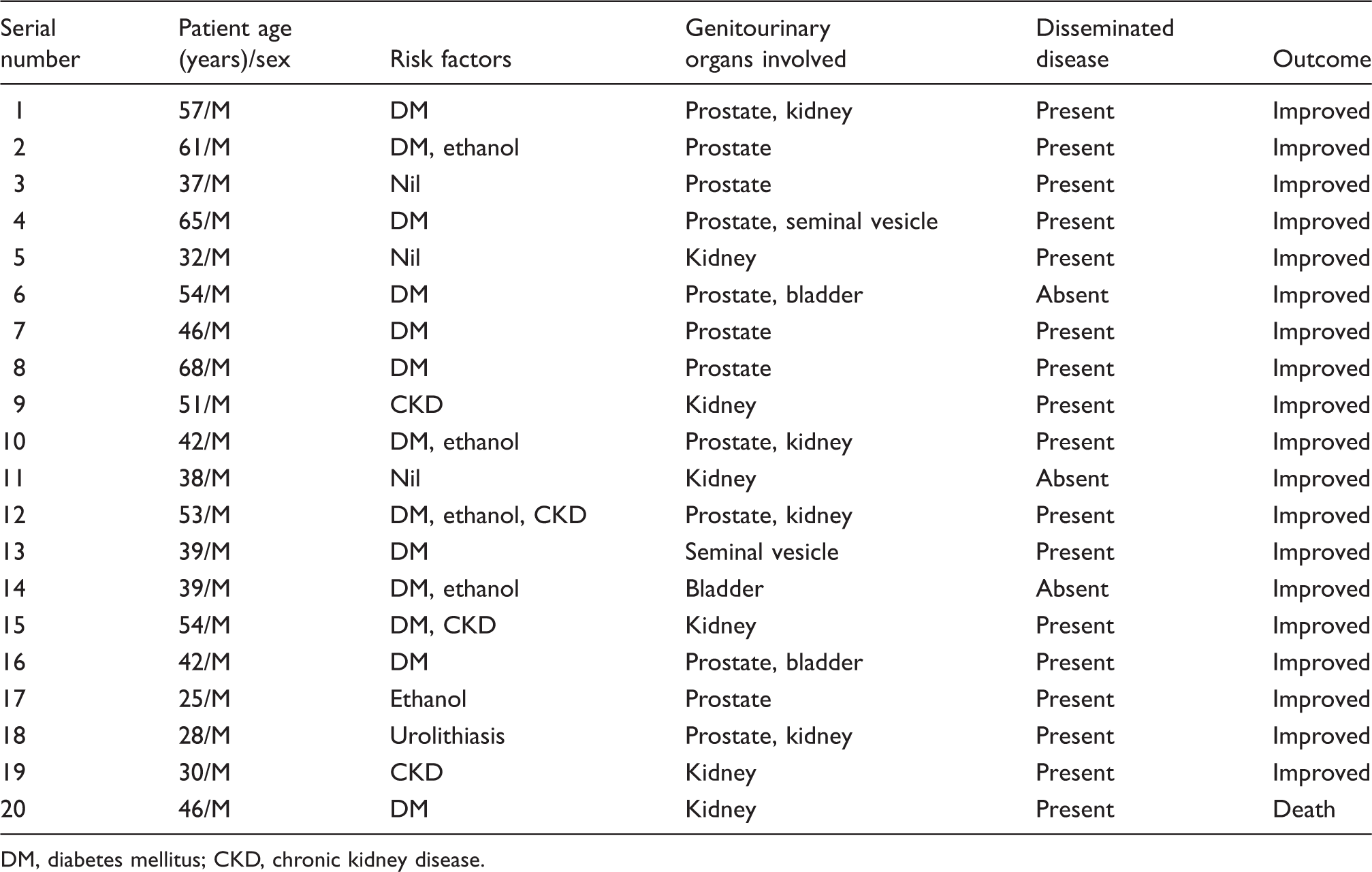
DM, diabetes mellitus; CKD, chronic kidney disease.
Patients were hospitalised for a median duration of 21 days (IQR = 11.3–29.3 days). Most received standard intensive treatment with ceftazidime for a median duration of 21 days (IQR = 14–42 days) followed by eradicative therapy with doxycycline and trimethoprim-sulfamethoxazole for 90 days (IQR = 90–140 days). Eleven patients (55%) required a diagnostic or therapeutic interventional procedure. One death occurred in the group, in a patient with disseminated blood involvement. All other patients had a favourable outcome. Follow-up data were available for 50% of the group at three months and 25% at one year. During this period, there were no cases of relapse.
Discussion
This study highlights that genitourinary disease, though under-recognised, contributes significantly to the burden of melioidosis. Our hospital treats an average of 15–20 patients with melioidosis each year. As in other studies, men were mostly affected with a predilection for the middle-aged population. 4 The large proportion of patients from East and North East India could reflect endemicity in these areas or referral bias. While diabetes and harmful ethanol consumption were observed to be the most common, interestingly, in a small proportion of patients (20%), we failed to identify any risk factors. Hence, this differential should be considered even in the absence of traditional risk factors.
Genitourinary melioidosis was commonly seen in the setting of chronic disease. In keeping with other studies, the prostate was the most common organ of involvement, followed by the kidney, bladder and seminal vesicles.4,7 While recent studies cite E. coli to be the commonest causative organism of chronic bacterial prostatitis, melioidosis should also be considered in the appropriate setting. 8 Along with classical urinary tract symptoms, symptoms of obstruction and retention should alert the clinician to this diagnosis.
Most patients (85%) had evidence of disseminated melioidosis and 55% were bacteraemic. However, in the absence of the above, obtaining urine and pus cultures and appropriate clinical imaging is imperative in establishing the diagnosis. Surgical debridement and image guided aspiration of pus should be attempted, whenever feasible.
The retrospective nature of the study and lack of occupational details of a proportion of patients are some limitations that merit mention.
In our country, the most common infectious agent causing chronic genitourinary disease is mycobacterium tuberculosis. Melioidosis has often been referred to as a great mimicker and the same holds true for genitourinary melioidosis. 9 There is significant overlap in the pathogenetic mechanisms and risk factors of both diseases. 10 In our series, two patients had received prior antitubercular therapy before the diagnosis of melioidosis was made. Lack of awareness and inadequate laboratory facilities are impediments to the establishment of a correct diagnosis. 11
Our study highlights the importance of considering melioidosis as a differential in patients with chronic genitourinary infection.
Footnotes
Acknowledgements
The authors thank Dr. Ramya Iyadurai, Dr. Alice J Mathuram, Dr. Vignesh Kumar Chandiraseharan and Dr. Angel Miraclin Jebakumari T for their valuable contribution to the article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.