
Abstract

Introduction
Acquired arteriovenous fistulas (AVFs) are uncommon and are usually the result of penetrating trauma or an iatrogenic percutaneous procedure. A case of acquired AVF of indeterminate origin is presented.
Case report
A 36-year-old man was referred from a remote rural district hospital to a nearby Mission Hospital with one month’s history of increasing mass in the right iliac fossa (RIF). There was a history of blunt trauma to the RIF 4 months prior to presentation.
On examination, he was a slim man, afebrile with a tachycardia of 120 bpm. A large locally tender non-pulsatile mass with a thrill was felt in the RIF (Figure 1). There were decreased pulses in the distal right leg but claudication was not reported as the patient was reluctant to walk. A continuous cardiac murmur was also present, as can be heard with a systemic AVF.
RIF mass prior to surgery.
Serologic testing was positive for human immunodeficiency virus (HIV), and the CD4 count 310 cells/mm3.
Ultrasound examination demonstrated a 12-cm diameter pseudo-aneurysm of the right external iliac artery (EIA) with thick thrombus in the wall and swirling blood in the centre. Owing to the size of the aneurysm, the veins could not be identified and a venous communication was not appreciated.
A visiting vascular surgeon was available at the time the patient presented, so no hesitation existed in recommending surgery, during which an arteriovenous fistula was found. After mobilising the colon and retracting it out of the operative field, the common, internal and external iliac arteries were dissected and vessel loops were tightened around these vessels and a vessel clamp applied to the proximal EIA, to control the aneurysm inflow (Figure 2). The right ureter was also identified and was adherent to the aneurysm sac; it was carefully preserved. The aneurysm was opened and the AVF oversewn with a prolene suture. Venous bleeding from the fistula between the back wall of the aneurysm and the iliac vein was controlled by oversewing the aneurysm and iliac vein. It was not possible to resect the aneurysm and do a primary repair to the artery as the EIA defect was too large, so a Dacron graft was used to close the arterial defect (the use of the saphenous vein to repair the injury is also possible if Dacron is not available). Following surgery, the right peripheral pulses were bounding and equal to the contralateral side. Postoperatively, there was no claudication and an ultrasound scan showed normal flow through the site of repair. There was oedema of the leg which responded to compression stockings and improved with time. The continuous cardiac murmur was no longer present.
Intraoperative image showing resection, aneurysm and vessel ties.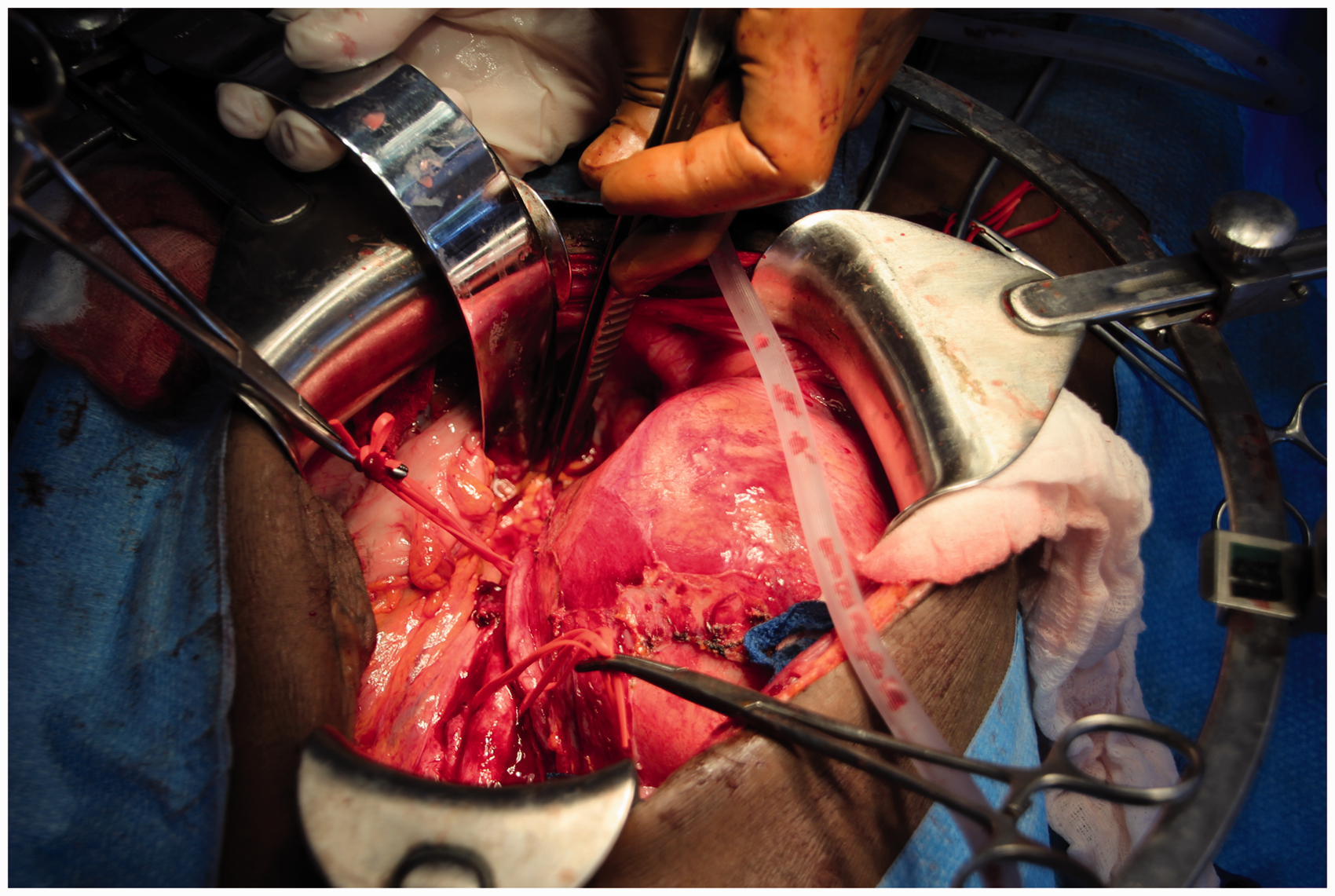
However, the postoperative course was complicated by persistent fevers to 39℃. Despite several full courses of broad spectrum antibiotics, the fevers persisted. Sputum was negative for AFB on multiple occasions. A chest radiograph demonstrated extensive right lung consolidation and right hilar lymphadenopathy, thus a diagnosis of tuberculosis was nonetheless presumed. The patient was commenced on standard treatment of rifampicin-isoniazid-pyrazinamide-ethambutol (RHZE) and rapidly became afebrile and gradually began to gain strength and weight. He was offered a full 6-month course of TB treatment and subsequently antiretroviral therapy.
Discussion
An AVF is an abnormal direct communication between an artery and a vein. William Hunter, in 1761, first described their most common physiologic effects and their usual signs. 1 The artery enlarges proximal to the AVF with a weak pulse distal to the lesion; veins in the region of the AVF become enlarged and demonstrate a hissing noise (bruit) which can be heard through a stethoscope and felt as a thrill. In our case, the swelling was not pulsatile, owing to the fact it was a fistula and the normal high resistance triphasic flow in the EIA was replaced with a low resistance flow pattern of constant forward flow. Flow in the artery proximal to a fistula can be increased up to five-fold and with such high flow, shunting will result in increasing preload on the cardiac circulation. This may lead to high output congestive cardiac failure. This patient did not have this this but had nonetheless a continuous cardiac murmur, indicating a hyperdynamic state.
AVFs may be congenital or acquired. The primary aetiologies of acquired AVFs are penetrating trauma and iatrogenic injuries (through arterial puncture) with a small number occurring spontaneously. Approximately 1% of traumatic AVFs arise from blunt trauma. Inflammatory processes may also effect pathologic changes to the arterial wall contribute to the formation of spontaneous AVFs; infectious causes include syphilis, tuberculosis and HIV disease and connective tissue disorders include Marfan’s and Ehlers-Danlos syndromes. 2
Iliac AVFs are uncommon (up to 1.4%) and are usually the result of penetrating trauma or lumbar disk surgery. 3 Our patient had developed an iliac AVF with only a history of blunt trauma. It manifested as an increasing swelling in the groin; which may also have been due to HIV disease or tuberculous emboli.
The goals of therapy for acquired AVFs are closure of the fistulous opening, restoration of normal haemodynamics and maintenance of vascular continuity. Conservative treatment was not an option in this case due to the increasing size of the aneurysm and its symptomatology. Surgical and endovascular treatments are possible; however in rural Africa, endovascular options are limited or non-existent. If a vascular surgeon and Dacron graft are not available, the following is suggested as a course of action for an iliac aneurysm or AVF:
If the AVF/aneurysm has not ruptured, refer the patient, if possible, to a larger facility which can perform vascular surgery. If the AVF/aneurysm has ruptured, ligate the proximal and distal artery (and vein in the case of an AVF) and watch for ischemia. If the patient develops ischemia, amputate at the appropriate level. Ligation of the common or external iliac artery is associated with a 40–50% rate of subsequent amputation.
4
Ligation of the common iliac artery is better tolerated than the distal external iliac artery. If the patient cannot be referred and the iliac AVF/aneurysm is greater than 4 cm, treat as for no. 2 knowing the risk of subsequent arterial insufficiency. A temporary shunt is a consideration in a traumatised artery to control bleeding and maintain flow until definitive vascular repair can be accomplished. This would not be prudent in remote hospitals where referral and a vascular surgeon are not available.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.