
Abstract
Cysticercosis is a parasitic infection caused by larvae known as cysticercus cellulosae. Orbital cysticercosis is usually a part of generalised systemic infestation. Isolated infection of the extra-occular muscle is an extremely rare entity. Involvement of orbital adnexas are rare even if associated with brain infection. Here, we report a case of an 18-year-old boy who presented with eccentric proptosis and restriction in upward gaze and was diagnosed with cysticercosis of inferior rectus.
Introduction
Cysticercosis is a human parasitic infection common in developing countries.1,2 The common sites of infections are musculoskeletal, subcutaneous tissue and brain. Orbital cysticercosis is usually a part of generalised systemic infestation. Ocular involvement is rare. It may be intra-ocular or extra-ocular. It is a treatable condition and timely management may prevent occurrence of any complication.
Case report
An 18-year-old boy presented to our ophthalmology department with complaints of periocular swelling, right orbital pain, ocular hyperaemia and mild restriction of upward gaze in the right eye for 2 months. On clinical examination, visual acuity in both eyes was 6/6. There was lid oedema with eccentric proptosis of the right eye. The pupils were symmetrical and reaction to light was present. Fundoscopy was normal. Slit lamp examination of the anterior segment revealed mild conjunctival congestion. General physical and neurological examinations were within normal limits.
Routine blood examination and ELISA values were within normal limits. No evidence of raised ESR or eosinophilia was noted.
On account of atypical restriction of upward gaze, a B scan ultrasound (Figure 1a) of the right eye was performed, which showed a sonolucent ring with well-defined margins involving the inferior rectus muscle. There was also an intracystic, eccentric, hyperechoic, highly reflective round dot seen suggestive of a scolex. Computed tomography (CT) of the orbit (Figure 1b) confirmed these findings and excluded any brain involvement.
(a) B scan USG of right eye showing a small, well-defined, rounded, sonolucent ring with an eccentric reflective dot (scolex) in inferior rectus muscle. (b) CT orbit showing a small, round, hyperdense SOL with an eccentric dot noted in inferior rectus on right side.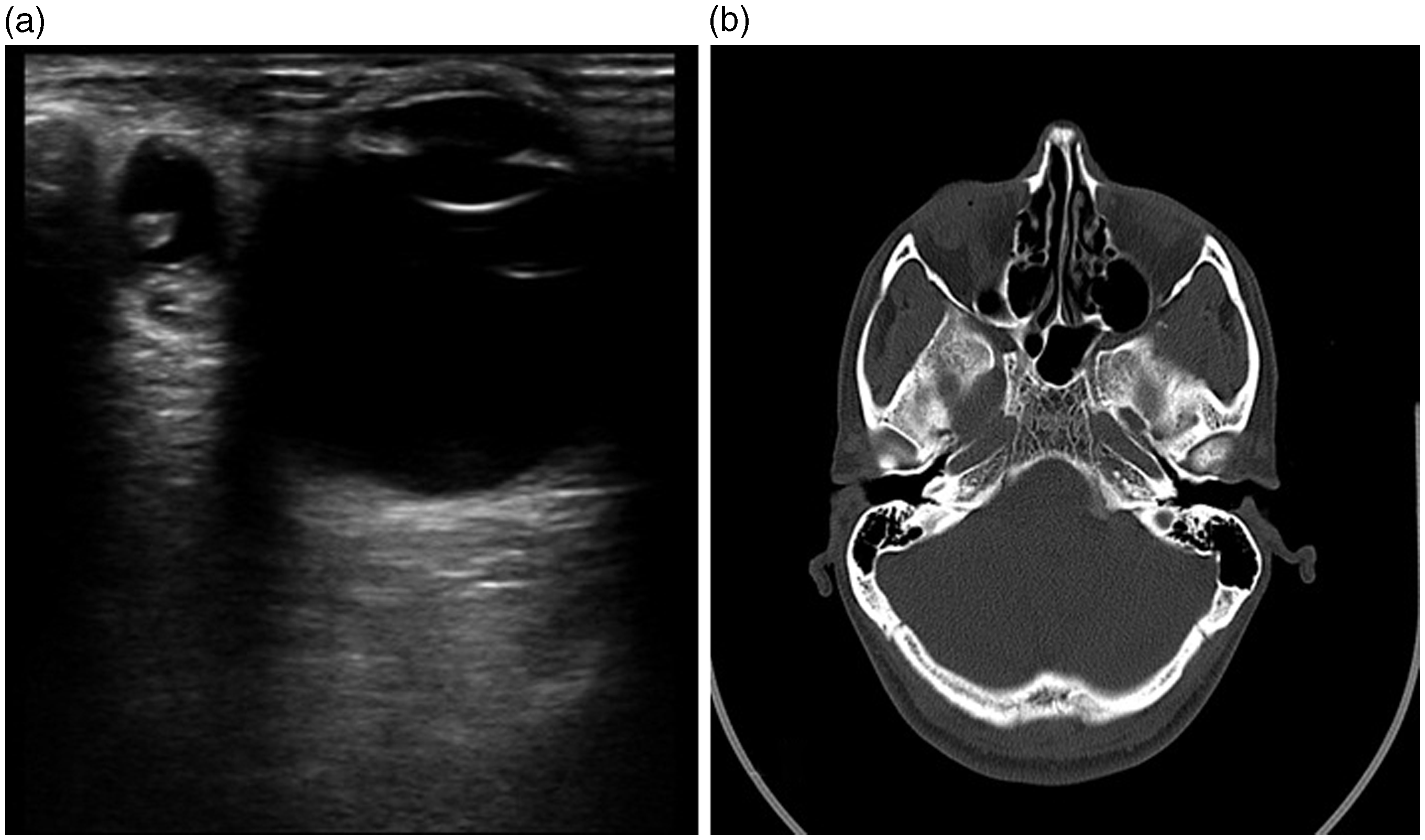
Treatment given was oral Albendazole 15 mg/kg/day along with oral steroids 1.5 mg/kg/day in a tapering dose over a period of 1 month. The cyst showed complete resolution.
Discussion
Cysticercosis is a zoonotic disease caused by the tapeworm Taenia solium. It is different from taeniasis which is caused by adult form of the parasite; cysticercosis is caused by larvae. Taeniasis is an intestinal infection, with the pig acting as an intermediate host, occurring from ingestion of undercooked pork and does not cause orbital infection. 3 In cysticercosis humans are the intermediate hosts and infection occurs through faeco-oral transmission. As the Taenia egg reaches the intestine, it hatches into a larval form which penetrates the mucosa to enter the portal vein where it then reaches other parts of the body. 4 Common sites of invasion are musculoskeletal and subcutaneous tissues and the brain. Ocular cysticercosis can be extra-occular, usually unilateral (i.e. subconjunctival or in orbital tissue) or intra-ocular (i.e. the subretinal space, vitreous chamber or anterior chamber in that order) 5 if larvae reach the choroidal circulation. Extra-ocular muscle involvement is one of the most common forms of orbital cysticercosis, but adnexal involvement is documented to be rare. 6 Any extra-ocular muscle may be involved, though the lateral and medial recti and superior oblique to a greater extent. 7
Clinical manifestation depends on the site and size of the cysts and immunity of the host. Larval cysts incite an inflammatory response that may result in compression of surrounding structures; 8 with time calcification supersedes.
The diagnosis of extra-ocular cystercosis may be made by ultrasound. Intra-ocular cystercosis can be easily diagnosed by opthalmoscopy. While the diagnosis of cysticercosis by ultrasonography is reliable, cerebral involvement warrants a CT scan.
Orbital cysticercosis without intra-ocular involvement may be treated a combination therapy of oral antihelminthics with steroids to suppress inflammation. The cyst then migrates from orbital muscle and comes to lie subconjuntivally whence it is extruded. 10 Surgical extraction is possible if the cyst is easily accessible, though it might be adherent and this may make a surgical intervention difficult or even hazardous.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.