
Abstract

Introduction
Ocular surface squamous neoplasia (OSSN) includes a spectrum of diseases which ranges from mild dysplasia to conjunctival or corneal intraepithelial neoplasia (CIN) and invasive squamous cell carcinoma (SCC). If the lesions are limited to epithelium only, they are considered in situ. OSSN usually presents as a sharply demarcated, gelatinous-appearing, reddish-grey growth in the palpebral fissure, which is usually seen in elderly men in their sixth or seventh decade.1,2 On the other hand, peripheral ulcerative keratitis (PUK) is characterized by unilateral crescentric sectorial thinning of the peripheral cornea associated with stromal inflammation in the affected eye, the latter being frequently associated with overlying epithelial defect which can lead to corneal perforation. 3
OSSN has often been misdiagnosed as corneal ulcer, 4 pterygium, 5 sclerokeratitis 6 and blepharoconjunctivitis. 7 To the best of our knowledge, however, OSSN masquerading as PUK has never been reported previously.
Case report
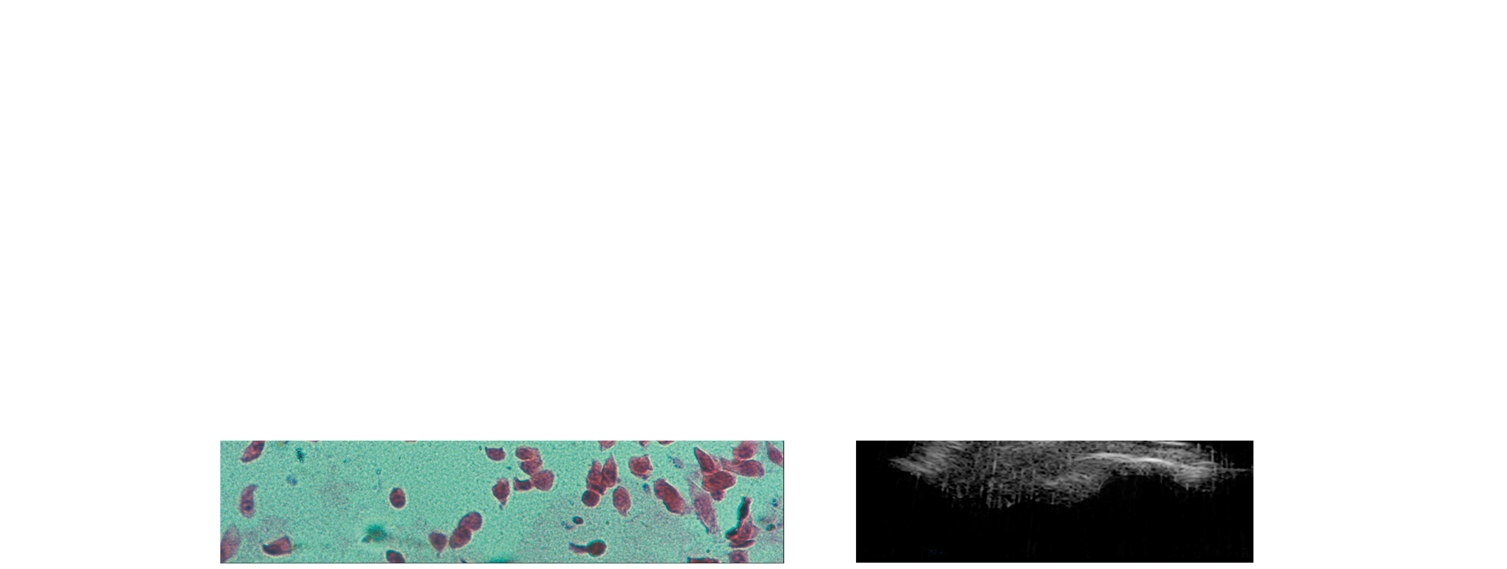
A 55-year-old male farmer from Rajasthan, India presented to the Cornea Clinic of our tertiary eye care hospital, with complaints of gradual, painful diminution of vision in the left eye, associated with redness and watering for the previous three months. He was being treated as a case of PUK with topical antibiotics, steroid and cycloplegic drops at another hospital. On ophthalmic examination, best corrected visual acuity in the right and left eye was 6/9 and 6/24, respectively. The left eye demonstrated circumcorneal congestion with an associated peripheral crescentric epithelial defect measuring 5 × 3 mm, located at the 3 o’clock position, with deep stromal involvement (Figure 1a). On careful examination, the bulbar conjunctiva nasal to the epithelial defect was elevated, bulbous with abundant intrinsic vascularity and dilated episcleral feeder vessels (Figure 1b). A greyish-white membranous growth was observed covering the nasal iris and pupillary margin suggestive of intraocular spread of the tumour. Immature senile cataract was noted bilaterally. Fundal examination and intraocular pressure were found to be normal. Corneal scrapings from the region of the peripheral ulcer did not reveal any growth. On strong suspicion of OSSN, impression cytology was taken, demonstrating inflammatory cells along with hyperkeratosis and moderate to severe dysplasia of epithelial cells, confirming this diagnosis (Figure 2a). Systemic evaluation was within normal limits and no metastasis was found on whole-body scans. Ultra-high resolution ocular coherence tomography of the elevated lesion revealed a thickened, hyper-reflective epithelium and an abrupt transition zone from abnormal to normal epithelium. Intraocular invasion and full thickness sclera infiltration with invasion of the angle was documented on ultrasonic biomicroscopy (Figure 2b). An enucleation was advised in view of intra ocular invasion, but the patient refused owing to persisting good vision in the affected eye. He was started on topical interferon alpha 2B (1 million IU/mL), four times a day and kept under observation. At 2-month follow-up visit, the visual acuity had dropped to 6/60, the surface lesion had decreased in size and severity, but the intraocular spread had progressed. The patient was again counseled for enucleation and made to understand the invasive nature of the disease and this time, he gave consent.
(a) Showing circum-corneal congestion in left eye with an associated peripheral crescentric epithelial defect measuring 5 × 3 mm located at the 3 o’clock position, with deep stromal involvement. (b) Showing elevation of the bulbar conjunctiva nasal to the epithelial defect and dilated episcleral feeder vessels. (a) Histology of the conjunctival lesion on impression cytology demonstrating atypical epithelial cells with nuclear enlargement, hyperchromasia and prominent nucleoli. Haematoxylin & eosin × 2000. (b) On ultrasonic biomicroscopy, intraocular invasion and full thickness sclera infiltration was documented as shown. 13 × 8 mm (300 × 300 DPI).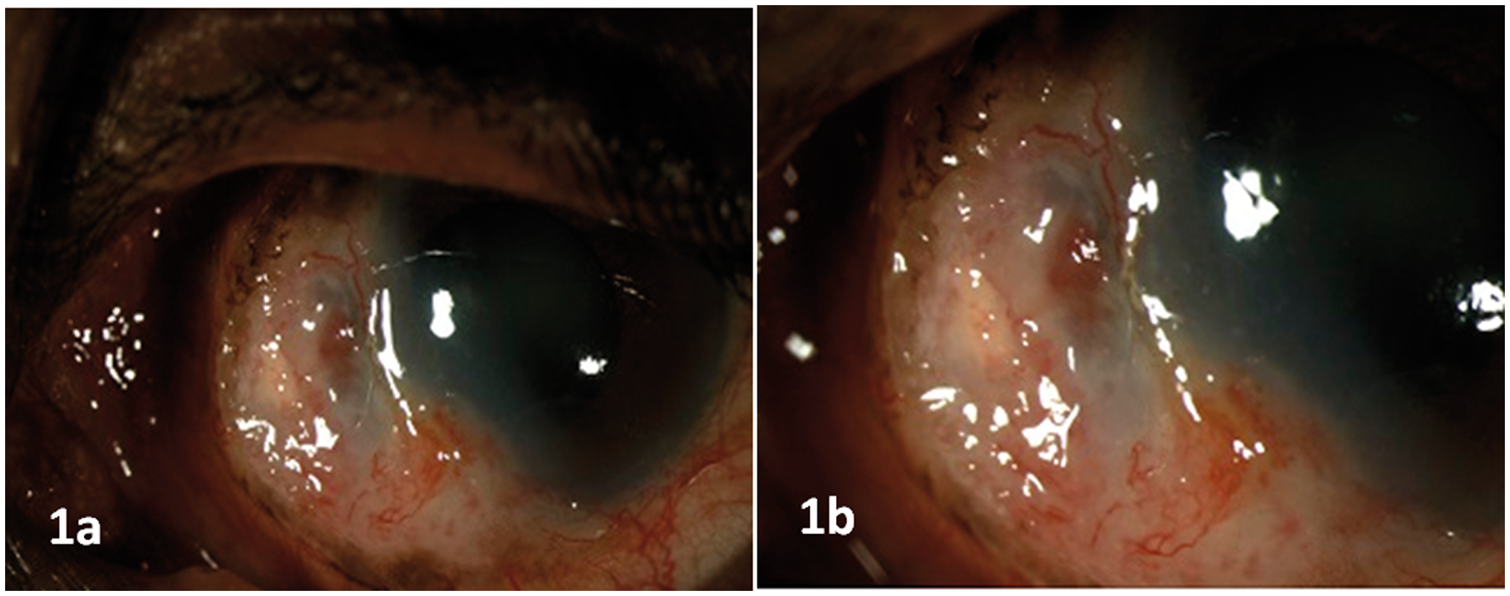
Discussion
Patients with OSSN usually present with an elevated mass on the ocular surface, commonly affecting the bulbar conjunctiva that is exposed to ultraviolet radiation. 8 However, occasionally, in the diffuse variety of OSSN, a well-circumscribed growth is not evident and corneal involvement may be seen. Ulceration of the peripheral cornea is rare with these lesions and may be a manifestation of an invasive carcinoma, as in our case with intraocular extension. The presumed mechanism of the epithelial defect and thinning could be secondary to the dellen formation and local ocular surface involvement which can result in breakdown of peripheral corneal epithelium and its progression to keratitis. 9
However, our patient was initially diagnosed as a case of PUK, based on clinical evaluation and symptomatology, but the subtle peripheral conjunctival lesion and dilated vessels were missed or thought to be due to peripheral extension of PUK. It is possible that the treating ophthalmologist mistook the clinical picture for associated scleritis or made a diagnosis of Mooren’s peripheral ulcer as the patient was in the elderly age group. Hence, limbal lesions in such settings should be carefully monitored and the line of management should be reconsidered in cases of non-responsive and progressive lesions, despite standard medical therapy. The ophthalmologist should assess such subtle lesions with high index of suspicion and scrutinize them with investigations such as impression cytology to facilitate accurate diagnosis and management in order to avoid fatal systemic as well as other ocular complications.
Impression cytology has been reported to have a high predictability in cases of OSSN and does not yield any false positive results. In previous studies, it has been shown to be accurate in the majority of cases of OSSN and correlates well with tissue histology, except in cases with abundant surface keratinisation or inflammation. 10 Although impression cytology cannot replace tissue histology, it has an important role in the diagnosis and management of patients with OSSN, being less invasive. It is useful in elderly patients unfit for surgical biopsy and relevant in cases where the diagnosis can be supplemented by anterior segment ocular coherence tomography and ultrasonic biomicroscopy, as in our case.
To conclude, the presence of OSSN is not always associated with a distinct ocular mass lesion and can masquerade a number of corneal conditions, especially PUK. In cases of diffuse OSSN, intraocular spread due to perforation of ocular tissues can occur, attributed to ongoing inflammation and vascular invasion. Hence, OSSN should be kept in mind in patients with atypical PUK presentation, especially if older male patients residing in a tropical or sub-tropical regions.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.