
Abstract
In Chad, hepatitis B virus (HBV) is thought to have a high prevalence and is consequently responsible for numerous acute and long-term complications. It is often detected during screening in potential blood donors. However, no general population-based study on the prevalence of hepatitis B has been performed. The aim of this study was to gain an impression of the HBV prevalence in rural areas in south-west Chad. A total of 1309 individuals (745 boys/men, 564 girls/women) with a median age of 15 years (age range, 6–81 years) were screened for the presence of the hepatitis B antigen (HBsAG). We found an overall prevalence of 22.9%. The youngest age group (6–15 years) and the boys/men showed a significantly higher HBsAG prevalence compared to the older groups and the girls/women, respectively (P < 0.01). Vertical infection during birth and horizontal infection by sharing food, water and shelter are believed to be the main sources of infection.
Introduction
Viral hepatitis B remains a major cause of morbidity and mortality worldwide. According to the statistics of the World Health Organization (WHO), 8–20% of the population in sub-Saharan Africa are chronic carriers of the hepatitis B antigen (HBsAG), indicating acute or chronic infection with the hepatitis B virus (HBV). 1
The lifetime risk of a HBV infection in sub-Saharan Africa is considered to be above 60%. 2 The likelihood of progression to chronic infection when the patient is infected perinatally is 90%; 30% for those aged 1–4 years and less than 5% in adults, respectively.3,4 Although in some people chronic hepatitis B is inactive and does not lead to significant liver disease, longitudinal studies have shown a cumulative risk of 8–20% of developing liver cirrhosis over five years. 5 It is estimated that worldwide around 650,000 people die each year from the complications of chronic hepatitis B. 6 Also, in Chad, the main cause of liver diseases is assumed to be HBV. Reliable figures, however, are lacking.
HBV infection can occur horizontally or vertically. The virus is transmitted horizontally efficiently by both mucosal and percutaneous exposure to infected blood or various body fluids, including saliva, menstrual, vaginal and seminal fluids. 7 Vertical infection occurs in large proportions of viraemic mothers during or shortly after giving birth, especially in those who are seropositive for hepatitis B envelope antigen (HBeAG) or suffer from acute hepatitis B during the second or third trimester of pregnancy. 8
In several global hepatitis B epidemiology studies, data from Chad are either are lacking or Chad is sub-summarised in a group of sub-Saharan countries with a prevalence of greater than 8%.9–11
Methodology
Ethical approval for this study was obtained from federal and local health authorities in Chad, such as regional spiritual authorities. All participants or, in the case of minority their adult representatives, who took part in this study gave their verbal informed consent.
Statistical data analysis was performed with SPSS (IBM SPSS Statistics, Version 23).
The area of research was limited to the rural areas around Lake Léré and the western outskirts of the city of Pala in the province of Mayo-Kebbi Ouest in south-west Chad. The study was conducted in January and February 2015. The same group of healthcare professionals conducted the study visits on all the sites. Testing was performed in elementary, middle and high schools, including randomly chosen pupils from all grades and approximately equally distributed by gender and a small number of teachers. Participation was free and voluntary and included testing and post-test counselling. The participants were asked to respond to a questionnaire including their age, ethnic group and site of residence. The study population was divided into three age groups: 0–15 years; 16–25 years; and older than 25 years.
Testing was performed by using an Elisa test (Swe-Care Rapid One-step Test Strip, Manuf Date 2014 – 05 – 23, Exp Date 2017 – 05 – 22, Lot 20140523 et.).
Results
Study cohort demographics.
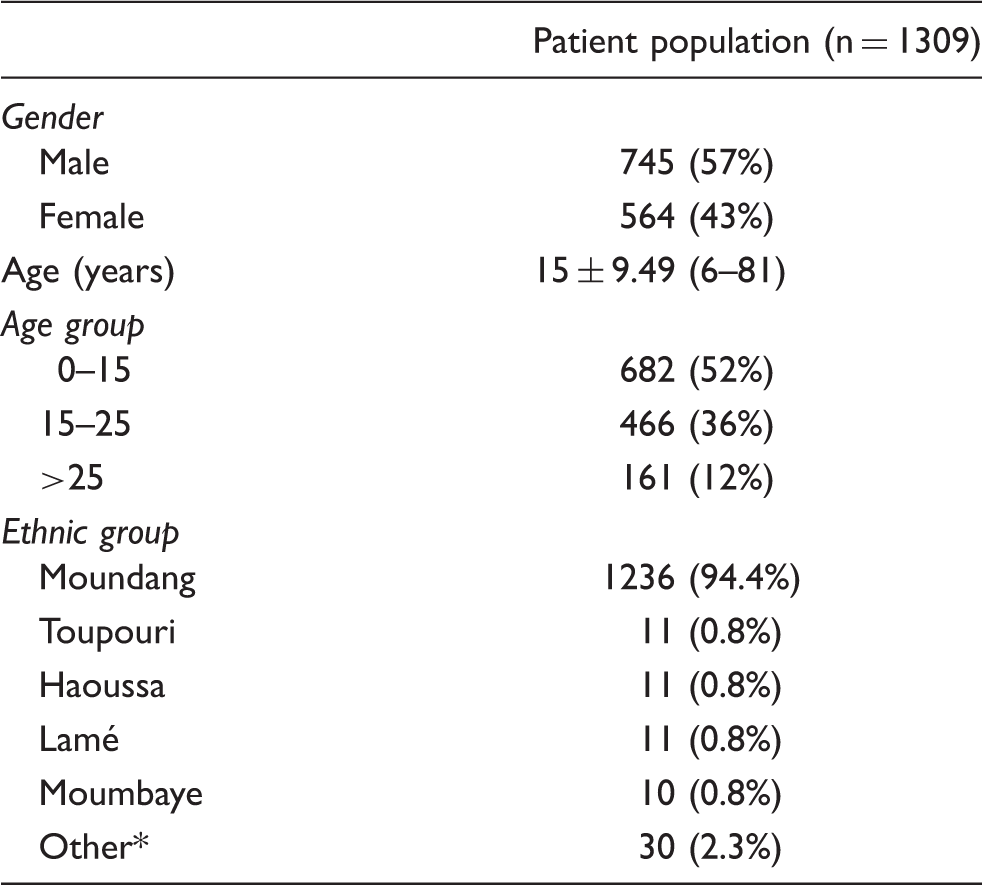
Moussey, Ngambaye, Nangtchéré, Sara Kaba, Djoukoum, Mbai, Kera, Hadjarai, Sahr, Goulaye, Kim, Arab, Langtiere.
Of the 1309 participants tested, 682 (52.1%) were aged 6–15 years, 466 (35.6%) were aged 16–25 years and 161 (12.3%) were aged > 25 years.
Of the 1309 participants, 94.4% belonged to the ethnic group of the Moundang. The other 6.4% are split up in locally less represented groups.
A total of 300 individuals (22.9%) were HBsAG positive (girls/women, 17.0%; boys/men, 27.4%; P < 0.001) with an age-adjusted odds ratio (by a Mantel–Haenszel analysis) of 0.501 (95% confidence interval [CI], 0.379–0.662). The Breslow–Day analysis for the homogeneity of the odds radio (OR) in the different age groups is P = 0.499, indicating that there is no evidence that results in gender analysis are age-linked.
HBsAG prevalence results.
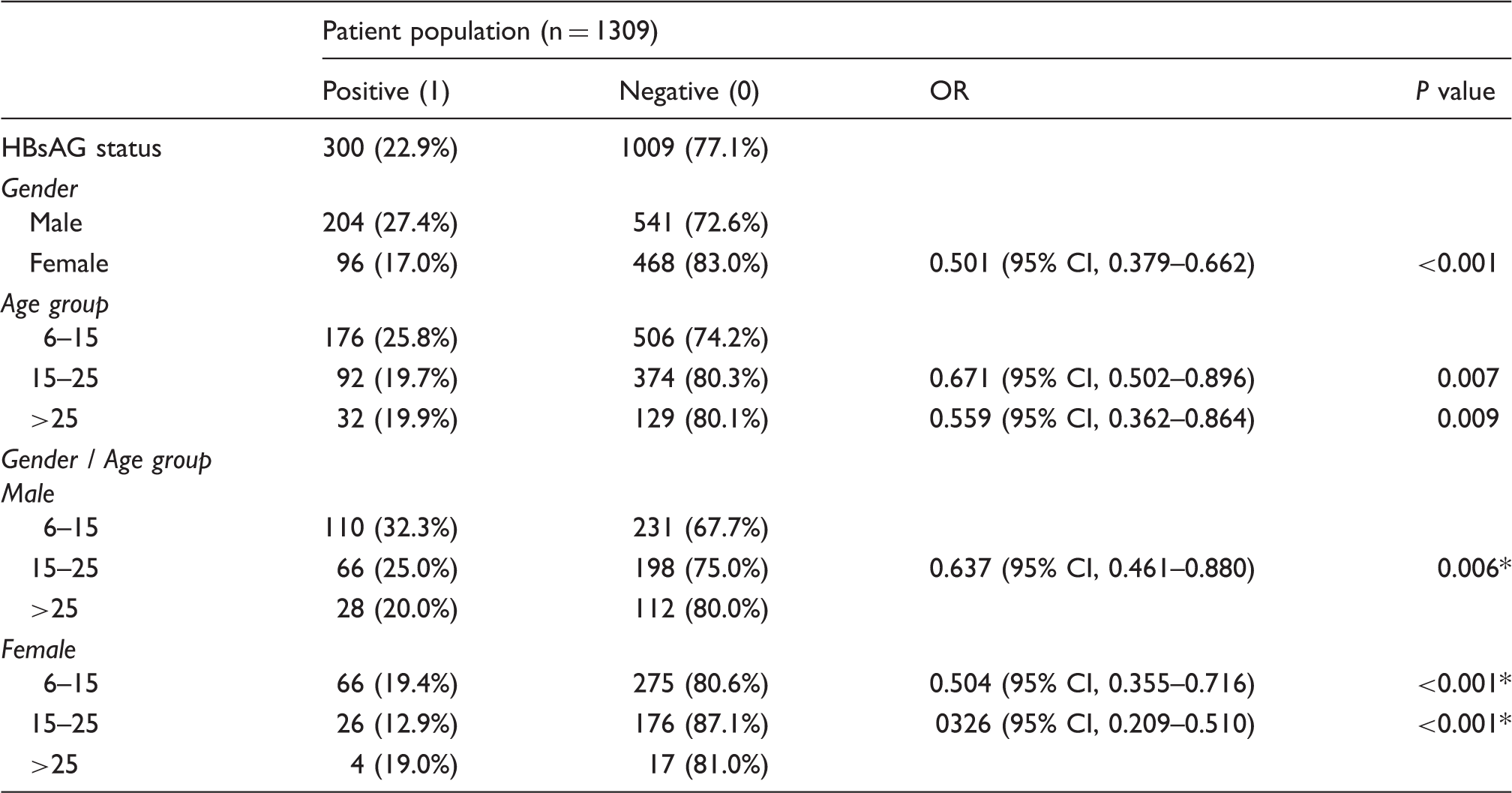
Reference category: Male, 6–15 years. The age categories 15–25 and > 25 in both genders were tied for statistical analysis.
Discussion
Studies in neighbouring countries show a HBsAG prevalence in the range of 6.7–20.6%.12–15 In our cohort involving mostly young individuals, we found a positivity rate of 22.8%. Remarkably, the group of boys aged 6–15 years were significantly more often HBsAG positive compared to girls in the same age group or the boys/men in the older age groups. One possible explanation for this could be spontaneous seroconversion during adolescence. However, this does not explain the higher incidence among boys/men compared to girls/women.
We assume that infection occurs either vertically during birth (especially when the mother is found to be HbeAG positive) or horizontally by sharing food, water and shelter very closely every day and thus transmitting the virus via saliva into a small wound in the oral cavity or on the skin. This assumption is based on the fact that many siblings of the positively tested children or teenagers were often found positive as well, when they were screened after post-test counselling. Neither the oft-suggested source of infection of sharing razor blades, towels or toothbrushes, nor the re-use of needles or syringes in healthcare institutions is believed to play a major role in rural areas. The sexual transmission of the virus is also assumed to play a minor role in these areas since the majority of the tested individuals are rather young and promiscuity in Chad is low due to strict religious and socials norms.
Limitations
The two key limitations of our study are the lack of further blood testing, such as HBeAG, transaminases or HBV DNA to indicate the level of activity of the virus and the geographical limitation to the rural areas of the province of Mayo Kebbi Ouest. Furthermore, a greater number of individuals for testing is needed for an epidemiological study, though available funds limited the area of research.
Further studies are needed to obtain an idea of the HBsAG prevalence throughout the whole country in order to grow the awareness of the disease and intensify the efforts in prevention, vaccination and treatment.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: The authors acknowledge the support of the association ‘Amitié Suisse Tchadienne’ providing the kits and logistics for this study.