
Abstract

Introduction
Scrub typhus (ST), a mite-borne rickettsial disease, has increased in frequency in India, among other countries, in recent years.1,2 It is most commonly characterised as a febrile disease with a range of varying symptoms. This disseminated multi-organ disease may be life-threatening if not treated early during the illness and relapses with early cessation of treatment are common. 3 Approximately 1 million ST cases occur annually, although surveillance statistics are poor in many countries. However, potentially > 1 billion people are at the risk of infection. 4 The chigger vectors themselves act as the disease reservoirs and man is an accidental host. Agriculturalists residing in and travellers visiting the endemic area (the tsutsugamushi triangle) during activities such as rafting, hiking and trekking are at the greatest risk of the disease. 5 Outbreaks of ST in military units are common, 6 such as a recent outbreak during the Cowley beach exercise in Australia. 7 Mortality rates were high in the pre-antibiotic era; decreasing mortality has been seen in recent years.8,9 Broad antigenic heterogeneity is observed in Orientia tsutsugamushi (OT), 8 and thus vaccines have not yet been successfully developed. Newer endemic areas have been identified in China. 10 New evidence from Kenya and Chile indicates a larger endemic zone of ST than was previously believed to have existed, although this may be due to unrecognised species.11,12 Unresolved problems associated with ST include: pathogenesis; diagnosis and prognosis; and the role of immunity. Research progress in reducing the burden of this disease has been slow. 13 Early vaccine trials have shown that resistance to reinfection with homologous strains may occur up to three years and immunity to heterologous strains seem to dissipate within two years. 14 It is believed that reinfection with OT is relatively common in high endemic areas, although cell-mediated immunity may play an important role in recovery.15,16 Because of this, reinfections are rarely detected. Here we report a patient with ST who was infected twice in consecutive years confirmed by both laboratory tests and positive clinical recovery with anti-rickettsial antibiotics during both episodes. Our report also emphasises the possibility of reinfection in ST which may present with different clinical manifestations between episodes, including the possible absence of an eschar.
Case report
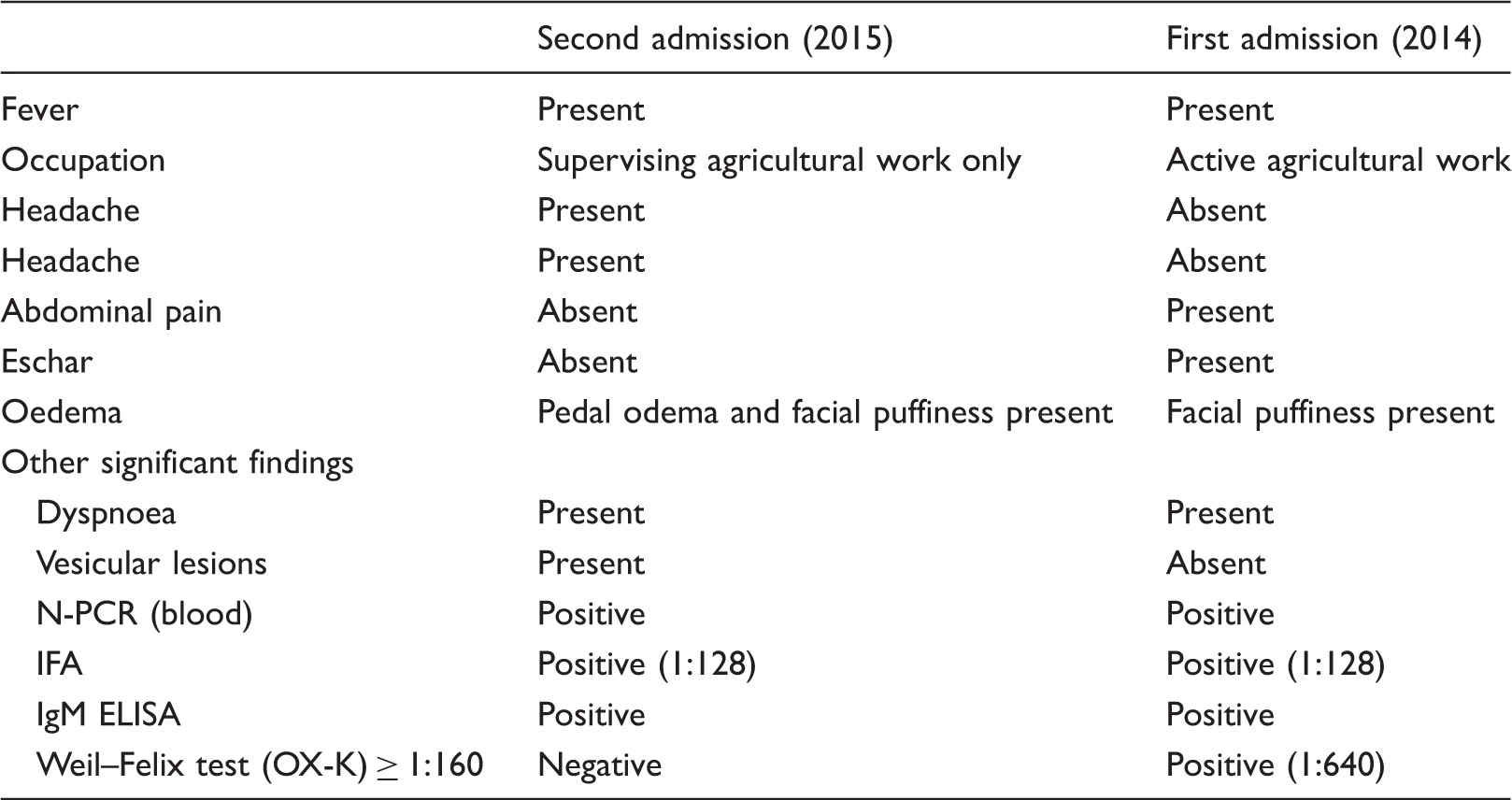
In September 2015, a 58-year-old agriculturalist presented to Kasturba Hospital, Manipal, Karnataka with high-grade continuous fever associated with rigors of eight days’ duration and frontal headache for seven days. On examination, his vital parameters were normal and systemic examination was unremarkable. Mild bilateral pitting pedal oedema with facial puffiness was noticeable. A thorough physical examination failed to identify an eschar. Vesicular lesions were incidentally noticed over the right angle of the mouth, for which the patient was successfully treated with topical acyclovir. He had not travelled elsewhere, but had been admitted and treated for a ST infection in the previous year and had refrained from active agricultural activity since then. Laboratory results showed a normal white cell count (8.1 × 109/L), a high erythrocyte sedimentation rate (ESR; 48 mm/h) and thrombocytopenia (115 × 109/L). Dengue, Weil–Felix test (OX-K, OX-2 and OX19) and malaria testing were negative. An ultrasound scan of the abdomen was normal. Serum antibodies to OT were positive by M-IFA and ST IgM ELISA. 17 The nested polymerase chain reaction (N-PCR) performed on DNA from the buffy coat was positive with a 483-bp product after amplifying with primers specific for the 56-kDa TSA. 18 Doxycycline 100 mg twice daily on the day of admission was administered. Platelet counts steadily normalised and the patient was discharged six days after admission as he was asymptomatic. Incidentally, during admission, he had complained of dyspnoea on exertion; an ECG showed T-wave inversion, which was treated solely with aspirin.
During late July 2014, the same patient was admitted with the chief complaint of dyspnoea on exertion for a period of two weeks. He had mild bilateral pitting oedema with facial puffiness, an eschar with a scab that had fallen off in the left lumbar region, and with mild tenderness in both right and left lumbar regions. Laboratory results showed leucocytosis (15.6 × 109/L), an elevated ESR level (52 mm/h), normal platelet counts (280 × 109/L) and an elevated creatinine level (129.6 µmol/L). The Weil–Felix test for (OX-K) antigen (1:640), ST IgM Micro immunofluorescence assay (M-IFA) and ST IgM ELISA were positive. N-PCR with STA56 gene primers with DNA from the buffy coat was also positive confirming the diagnosis as ST. 18 Doxycycline 100 mg twice daily was administered empirically as ST was suspected on the first day of admission. Improvement was seen and the patient was discharged after five days, being asymptomatic again.
Comparison of symptoms and laboratory results from the two episodes of ST infection.
Discussion
ST is primarily a rural disease and those exposed to infective chiggers are at the greatest risk. ST reinfections are known to occur in endemic regions, but are rarely reported.15,16 The present case was an agriculturalist by occupation and was more active during the initial episode rather than the latter. Following the initial episode, he only supervised the work undertaken when he visited agricultural farms. Recently, large numbers of ST cases have been observed from the area where our patient was working; ST is more common during the cooler months of the year. Human immunity from the first infection may last for one to three years against the homologous strain but is short-lived (less than one year) against the heterologous strains. 19 In our case, reinfection occurred 14 months later, during which time the immunity generated had waned, especially if the infecting strain was of heterologous type. Interestingly, during the second episode, our patient did not present with an eschar. Experimental studies suggested that an eschar was more closely associated with primary infection than reinfection. 14 Thus, immunity from the primary infection may only be sufficient to prevent the formation of an eschar but not avoid active infection. Phylogenetic analysis of infective strains may provide more information on this point.
Footnotes
Acknowledgement
The authors thank Dr. Gregory A Dasch, Rickettsial Zoonoses Branch, DVBD, NCEZID, CDC, Atlanta, USA for critically reviewing the case report and suggestions.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The present case (first episode) was observed during the large hospital-based cross-sectional study on scrub typhus funded by the Indian Council of Medical Research (ICMR).