
Abstract
Clinical data of 65 histologically documented ulcerative colitis patients from January 2001 to December 2013 were prospectively recorded till June 2017 and analysed to determine the outcome of long-term maintenance treatment. Drugs used were 5-aminosalicylates, steroids and azathioprine. Primary outcome measure was relapse. Though 73.8% patients relapsed, most occurred within the first five years with mild to moderate severity and were easily controlled with the same medicines. None had progressive disease; drug discontinuation was possible in six cases. Side effects of drugs were negligible. Rates of surgery, colon cancer, complications and disease-related death were very low. Longer disease duration, azathioprine discontinuation and 5-aminosalicylate use in dose < 2.4 g/d were positively associated with relapses. Biologics were not used in any patient. We conclude that long-term effective use of low-cost drugs in India may obviate the need for newer more expensive drugs.
Introduction
Ulcerative colitis (UC) is characterised by episodes of remission and relapses. The management and course depend on clinical presentation and endoscopic findings; however, which initial and subsequent maintenance therapy will best reduce long-term relapse rate is unclear. The effectiveness of maintenance therapy is influenced by the type and duration of treatment along with the location and duration of disease. 1 Recently, newer drugs which target different cytokines involved in the pathogenesis of UC have been developed and used for its treatment. These include ‘biologics’ such as anti-tumour necrosis factor agents (infliximab, golimumab, adalimumab), anti-adhesion molecules (vedolizumab, etrolizumab) or Janus kinase inhibitor (tofacitinib). Even though a ‘top-down’ approach (i.e. early use of biologics) has been recommended in severe or fulminant disease in order to ensure early mucosal healing, it is not effective in all patients. In addition to the low incidence of severe disease (about 5%) in India, the high cost of such therapy and the high incidence of serious side effects, including flare up of endemic infections such as tuberculosis and hepatitis B, make this approach unacceptable. Most patients benefit from 5-aminosalicylates (5ASA) with or without steroids as induction and 5ASA with or without azathioprine (AZA) as maintenance therapy. However, published data on their outcome are surprisingly rare. Our aim was to determine the length of remission using conventional medication and estimate dosages appropriate to maintain long-term remission.
Methods
This was a real-life prospective cohort study with retrospective analysis of a prospectively maintained database containing all patients’ disease-related information such as detailed history, clinical examination, relevant investigations, drugs used and follow-up data. We included all patients of UC (both inpatient and outpatient), diagnosed for the first time in our hospital between January 2001 to December 2013, based on clinical, endoscopic and histologic findings with a minimum of five years of supervised follow-up. Disease activity was determined according to the Mayo score. 2 Extent (E1–3) was defined according to Montreal criteria. 3 Pregnant patients and those with hepatic or renal disease or salicylate allergy were excluded. Remission was defined as clinical improvement with bowel frequency ≤ 3/day without rectal bleeding (partial Mayo score ≤ 2). Relapse was defined as any increase in clinical severity (especially rectal bleeding) compared to a pre-existing status which entailed more aggressive treatment. Time to relapse was defined as the interval between date of enrolment and relapse.
A step-up approach to treatment was followed. Induction was achieved with 5ASA with or without steroids according to our protocol described below (see Figure 1). Rectal steroid once daily was used if urgency or bleeding was disabling. Biologics were reserved for those patients failing to respond to these measures. Drug discontinuation was attempted for patients (especially those with E1 disease) in long-term remission (minimum five years) showing complete mucosal healing and no disease extension on colonoscopy. For others, the aim was to discontinue AZA while continuing 5ASA at the lowest dose possible preventing relapse. For 5ASA, a dose ≥ 2.4 g/day was defined as high, and < 2.4 g/day as low.
All patients underwent colonoscopy at baseline, after one year of treatment or earlier if indicated. Subsequent colonoscopy depended on the number and severity of relapse because of its unacceptability for minor symptoms in the local population. It was avoided if relapse occurred only once per year, was mild in severity or related to reduction in drug dosage. It was used in E1 disease in long-term remission (to assess mucosal healing) in order to consider drug discontinuation. All patients were personally supervised by the author and followed up monthly for worsening, new symptoms, drug side effects or complications, and ensuring proper drug adherence. As our hospital provides all medicines free of cost at monthly intervals (after checking the previous month usage), follow-up and drug compliance was very good. Patients were also free to report any time if they felt so inclined. The primary outcome measure was relapse and the secondary ones were change in disease extension, rate of complications, admission, colectomy, colon cancer or death.
Descriptive statistics (mean and standard deviation for quantitative variables) and proportions (for categorical variables) were calculated. Univariate (Student’s t-test or χ 2 ) and multivariate (binary logistic regression) analysis were performed to determine the relation of relapse to demographic status, disease-related data (duration, extra-intestinal manifestations, severity, extent, length of follow-up) and treatment-related data (need of steroid for induction and 5ASA in high/low dose for maintenance, 5ASA or AZA discontinuation with or without relapse) factors. Ordinal regression was done to test their effect on the number of relapses. All tests were done with SPSS 13 statistical software and a P value < 0.05 was considered significant.
The study protocol conforms to the ethical guidelines of the 1975 Declaration of Helsinki. Ethical clearance for this study was obtained from the institutional ethics committee and informed consent was obtained from all participating patients and their families regarding obtaining information, as well as follow-up data.
Results
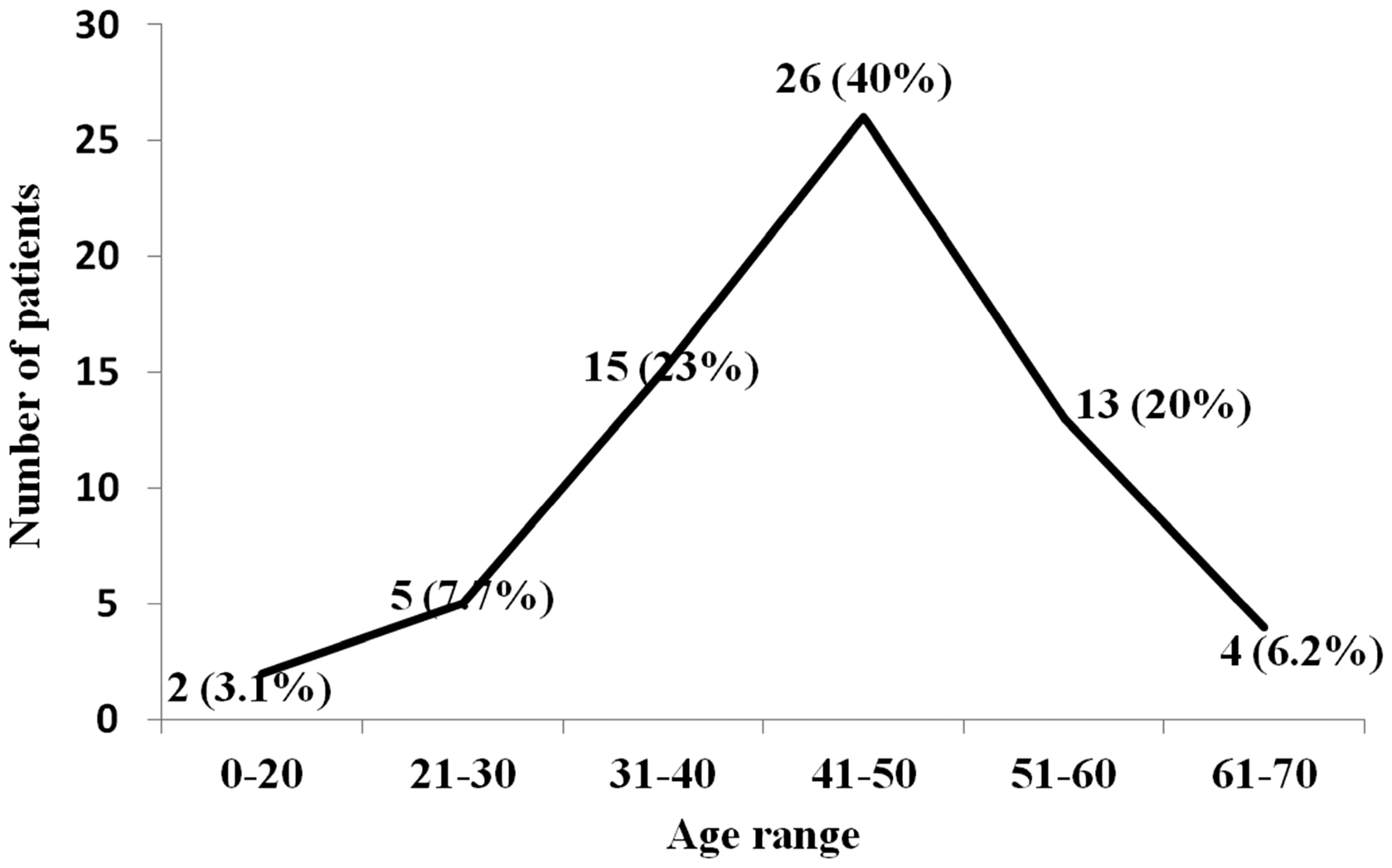
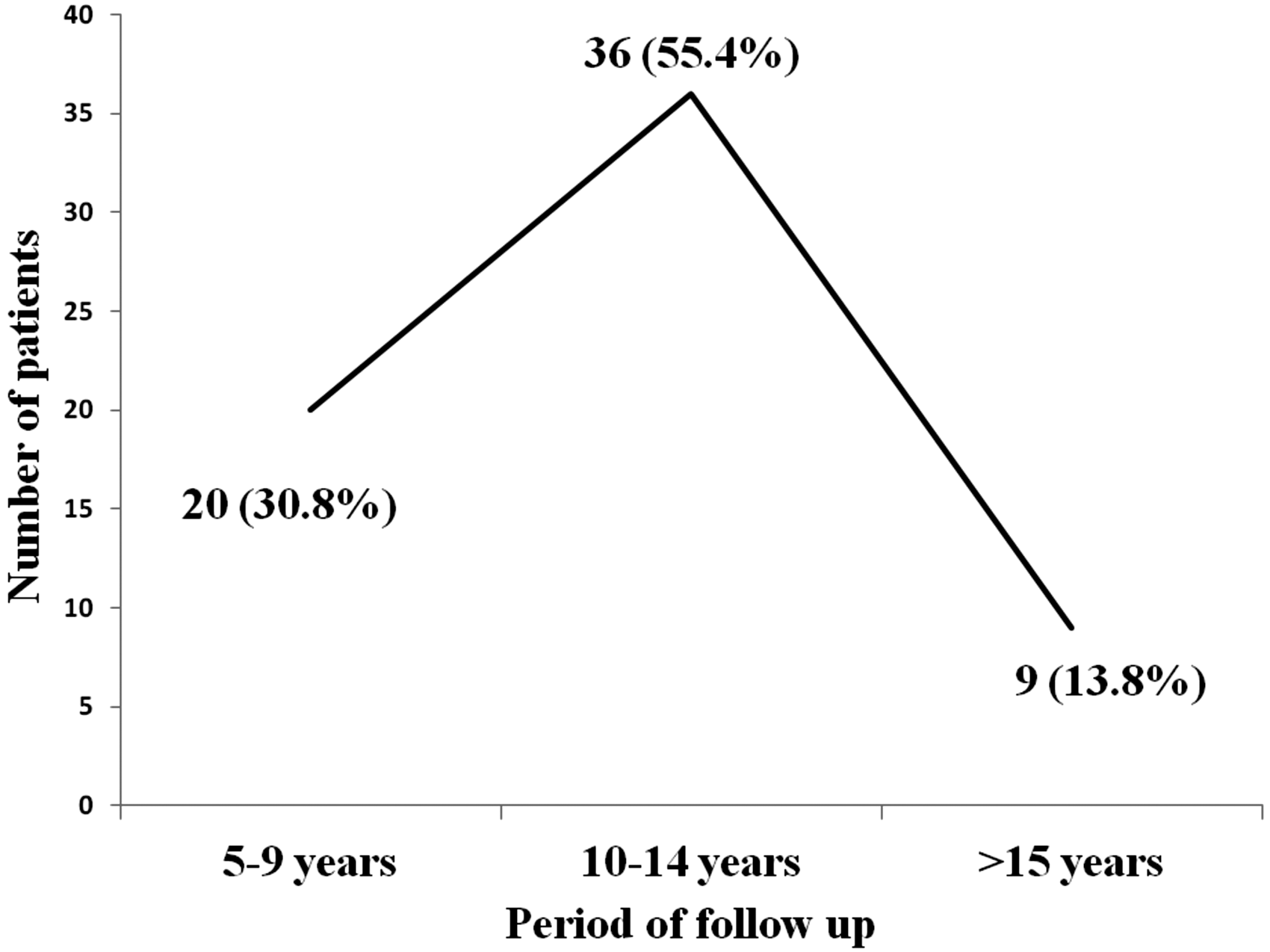
Over the study period, 65 eligible patients (41 men, 24 women; mean age at disease onset = 44.45 years; age range = 18–68 years) were included. Their baseline and follow-up clinical variables are summarised (Figures 2–7). Another 28 patients were excluded because UC was diagnosed for the first time elsewhere, there was irregular follow-up or treatment was taken elsewhere at the patient’s own discretion. Twenty-six (40%) patients were smokers and extra-intestinal manifestations were present in seven (10.8%), including uveitis and erythema nodosum in one each (1.5%) and sacroileitis in five (7.7%). There was a total of 724 person-years of follow-up with a mean of 11.14 years (range = 5–17 years). Similar mean follow-up of 10–12 years was recorded for severe, moderate and mild disease.
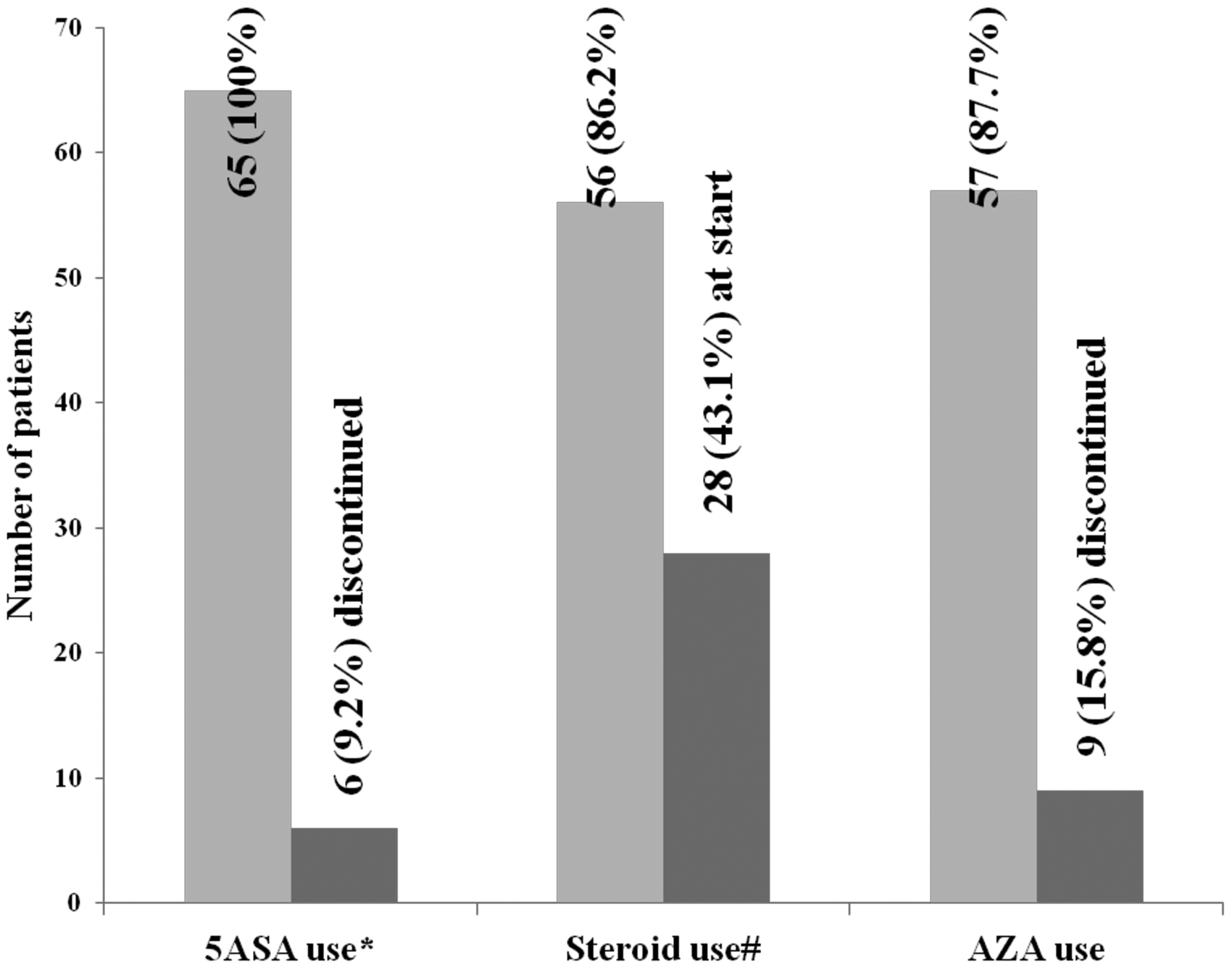
Flowchart on Treatment protocol. Unimodal peak of age of patients. Number of patients on long-term follow-up. Disease severity at presentation and relapses. Long-term drug adherence and remission rate. Number of patients on different drugs. *High dose 53 (81.5%), low dose 12 (19.5%), #Intravenous 16 (28.6%), oral 40 (71.4%). 5ASA, 5 Aminosalicylic acid; AZA, Azathioprine.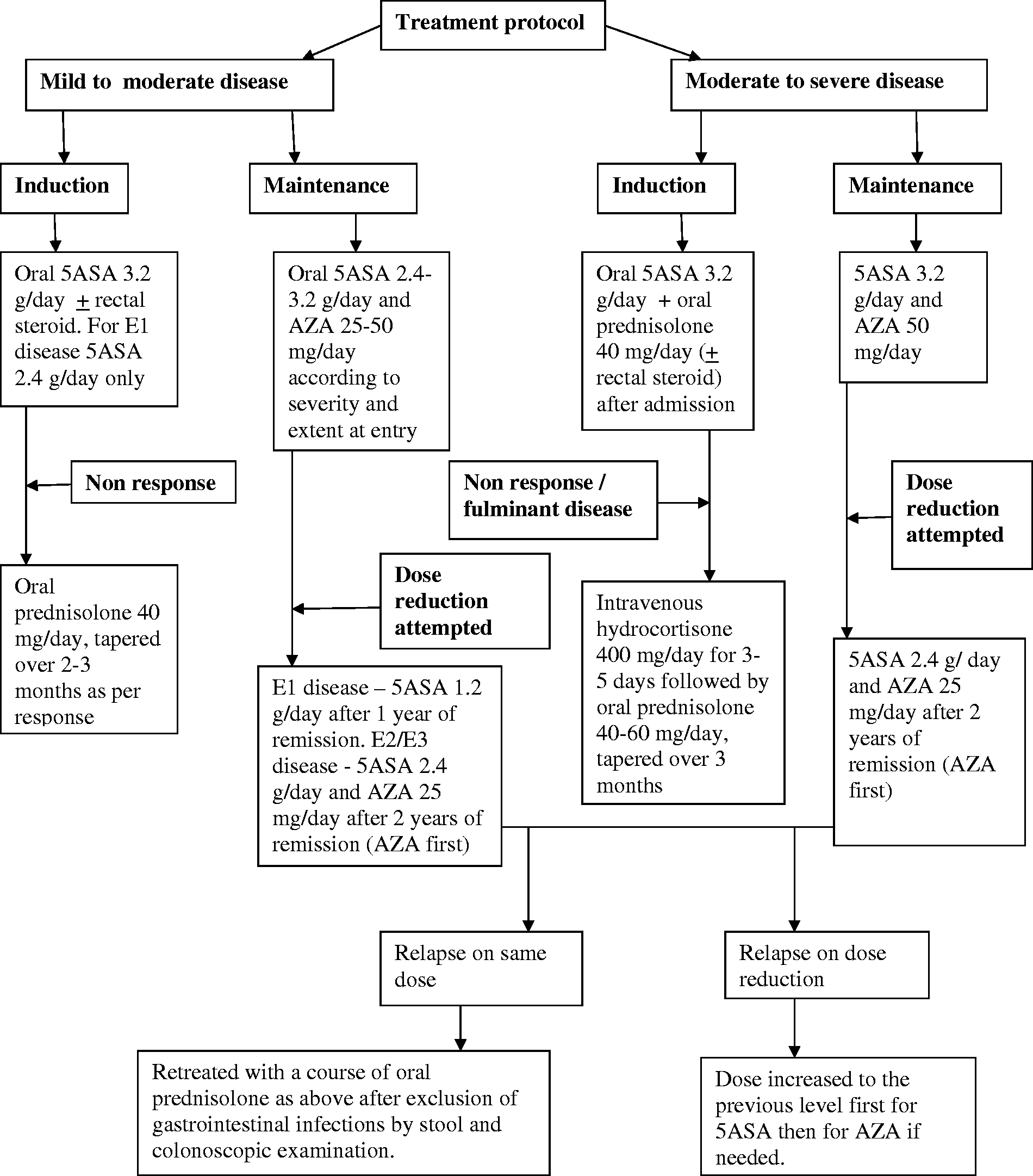
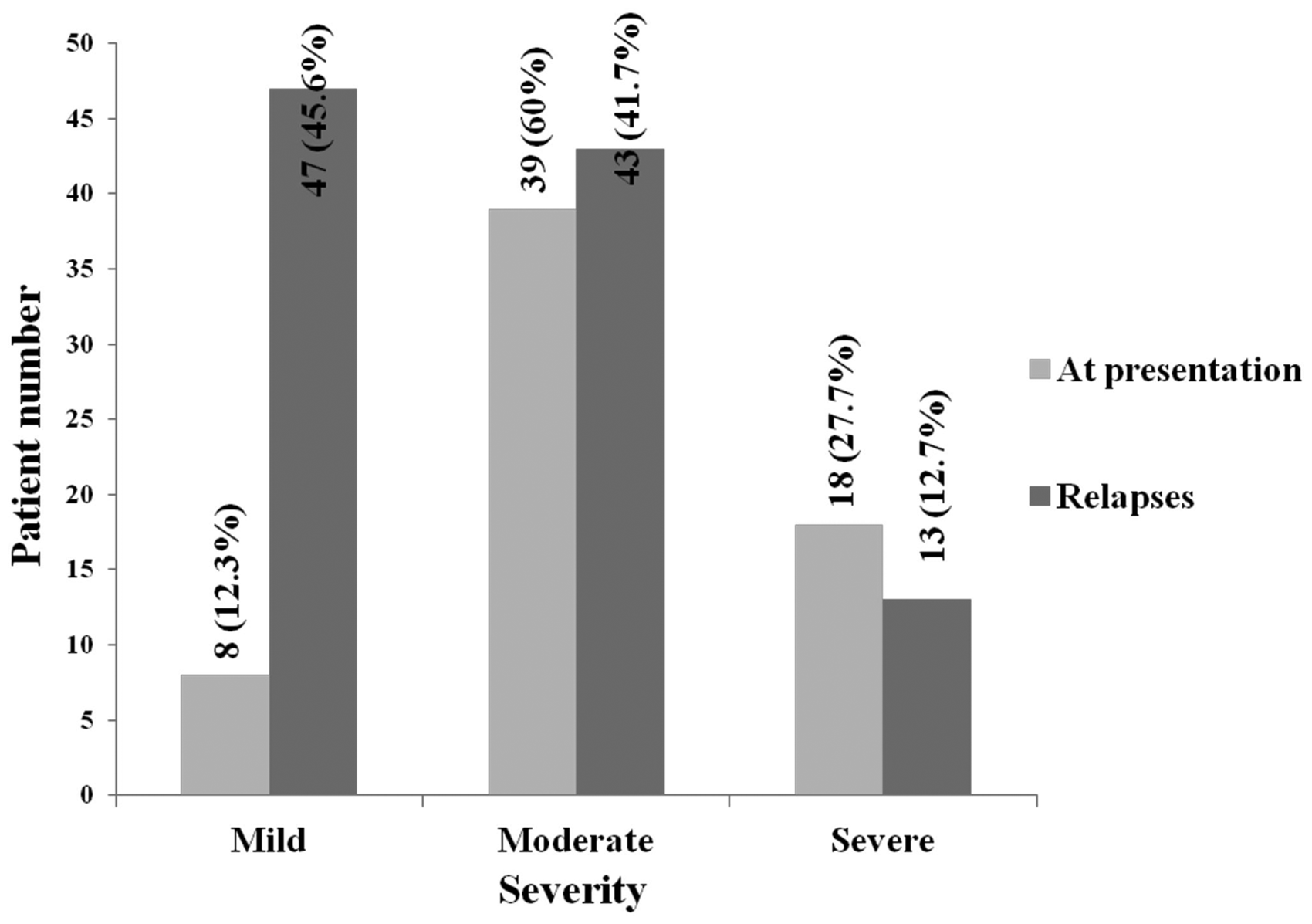
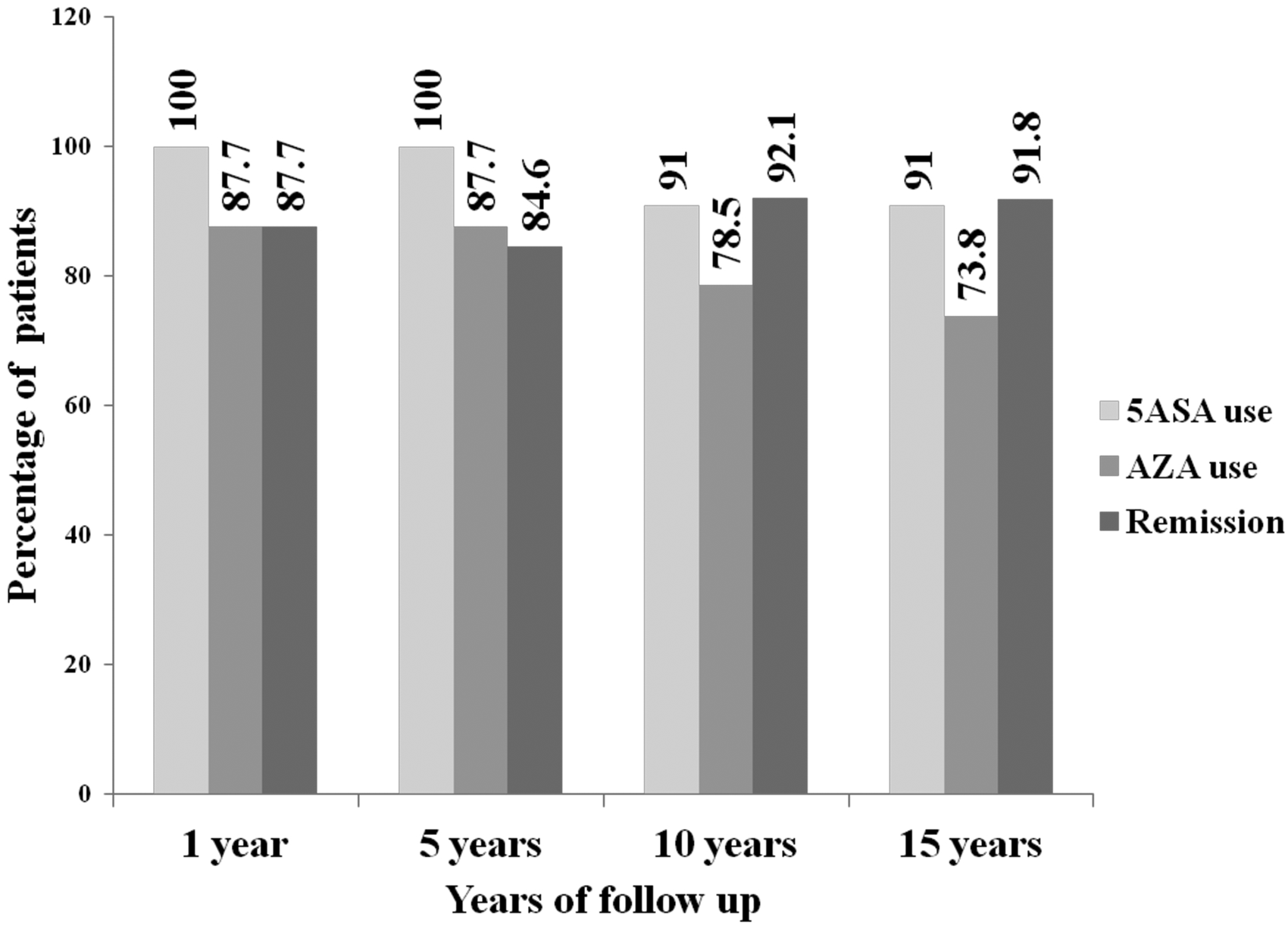
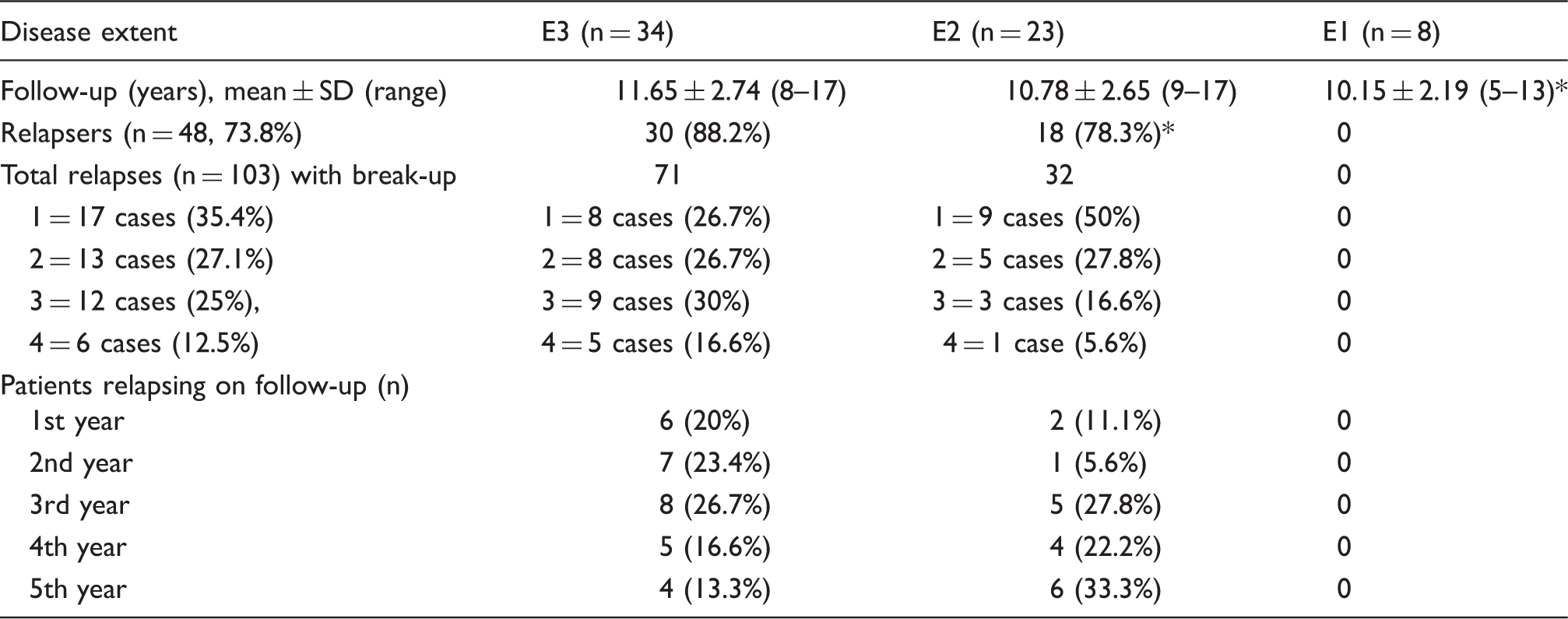
Data on relapses are represented in Table 1. A total of 17 (26.2%) did not relapse, and the first relapse occurred in all cases within the first five years. Relapses tended to decrease after the first 5–6 years (Figure 8). Haemorrhoids were present in 13 (20%) patients and bleeding from haemorrhoids labelled as ‘relapse’ could not be excluded with certainty.
Disease course according to extent. *5 Aminosalicyalte 2, Azathioprine 2. E1 disease, involvement limited to rectum only; E2 disease, involvement limited distal to splenic flexure; E3 disease, involvement proximal to splenic flexure. Data on relapse according to disease extent. P = not significant. SD, standard deviation; E1, involvement limited to rectum only; E2, involvement limited distal to splenic flexure; E3, involvement proximal to splenic flexure. Absolute number of relapses over the years according to disease extent. E1, involvement limited to rectum only; E2, involvement limited distal to splenic flexure; E3, involvement proximal to splenic flexure.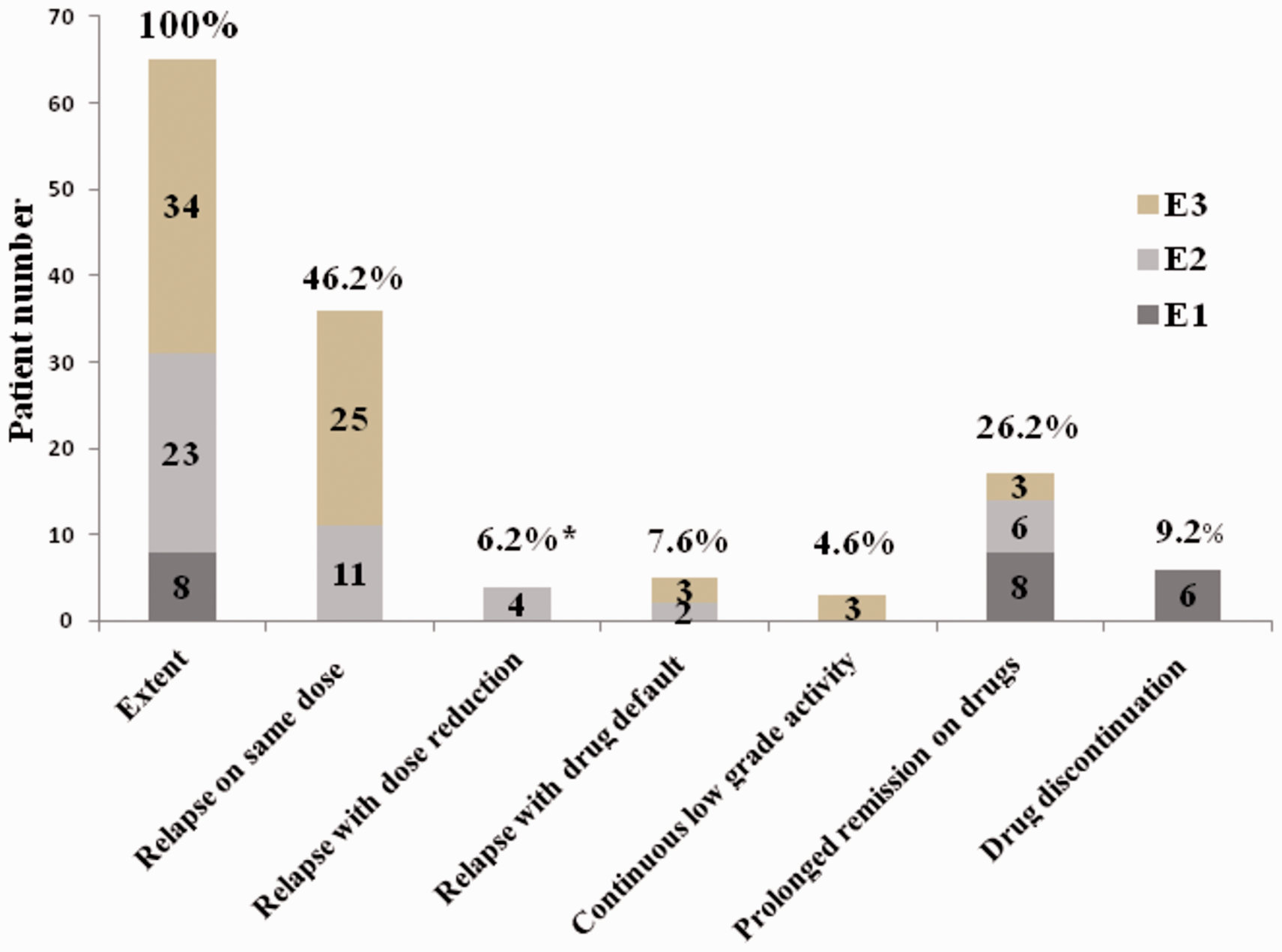

Disease progression did not occur in any patient. All eight patients with E1 disease were controlled with oral 5ASA and rectal steroids; drug discontinuation was possible in six patients owing to disease regression and complete mucosal healing after five years without any relapse up to ten years. All those with E3 and E2 disease needed 5ASA, AZA and intermittent steroids; regression occurred in two with E2 disease and none with E3 disease but without complete mucosal healing. There were no steroid-resistant cases but three had continuous low-grade activity on 5ASA and AZA which responded to increasing drug dosage or intermittent courses of oral steroid. No side effects were observed after 579 person-years of 5ASA use. Only one patient developed pancreatitis after 418 person-years of AZA use. Biologics were not required in any case, neither for induction nor for control of flare-up.
A total of ten (15.4%) patients needed admission at the start of treatment and 24 (36.9%) at different times during follow-up. Four (6.2%) patients died: one man with pancolitis developed cancer of the descending colon 12 years after disease onset, underwent total colectomy with ileorectal ananstomosis but died two years later from pneumonia; one woman, also with pancolitis, had a sudden massive haemorrhage and died during emergency operation. Two other deaths were unrelated, one from a cerebrovascular accident and the other from acute coronary syndrome. All deaths occurred above the age of 60 years. Thus, the colectomy rate was two (3.1%) and complications were cancer (n = 1, 1.5%) and massive rectal bleed (n = 1, 1.5%).
Univariate analysis of factors affecting relapse.

Pancolitis and left-sided colitis significantly more than proctitis but not different between them; moderate and severe disease significantly more than mild disease but not different between them; intravenous and oral steroid significantly more than no steroid but not different between them.
Calculated after exclusion of six cases.
Data represented as mean +/− S.D [Range].
EIM, extra-intestinal manifestations; AZA, Azathioprine; 5ASA, 5 aminosalicylate.
Discussion
The prevention of relapse and complications are the long-term goals of treatment of UC. As only naïve patients were included and treated in a similar manner, this homogeneity excluded any extraneous influence on the results. This study shows that relapses do occur, even on continuous maintenance therapy with the same dose (apart from drug default and dose reduction), but most are mild to moderate in severity and are easily controlled by increasing the dose of 5ASA or using short courses of steroids. There are inherent variations in causative immunological mechanisms of relapses and remission over time. Relapses tend to wane after the first five years of disease. The course of the disease was generally benign in the long term. Disease extension was prevented by long duration maintenance therapy in spite of a high relapse rate and the majority of patients not achieving complete mucosal healing. This was possibly owing to good drug compliance and early detection and intervention in cases of drug default. For similar reasons, relapses were negligible in E1 disease. Side effects were negligible as drugs were effective in lower dosage.
Long-term follow-up results of studies on adult UC in the pre-biologic era using 5ASA, AZA and steroids are available mostly from Asian studies. Though the studies are heterogenous with respect to disease extent at presentation and drug usage (facts which can affect outcome), the results are mostly similar to ours with earlier high relapse rate (55–100%) decreasing at later follow-up, with low rates of extra-intestinal manifestations (4.5–11%), colon cancer (0.2–3.2% after ten years of follow-up), colectomy (mostly 3–7%) and disease-related death (0.6–5.7%) except that disease extension was noted in 7–44% of patients, higher with increasing disease duration.1,4–9 Most of these studies do not mention anything about treatment adherence. A recent review of the natural history of a very large adult UC in population-based cohorts (the majority being from Europe and North America, followed up for 1–20 years) 10 showed a similar outcome.
Our study shows that AZA is an important drug for maintaining remission in dose of 50 mg/day (much lower than required in Western counterparts) along with 5ASA in doses ≥ 2.4 g/day without significant effects. For proctitis, 5ASA in doses of 1.2 g/day may suffice to maintain remission and discontinuation may be achieved after five years in some cases.
Such long therapy also tests patient compliance: this study could achieve excellent cooperation owing to personal supervision and the free and easy availability of medicines. Indeed, in a previous study on self-reported treatment adherence by 127 patients, 81% were non-compliant within a mean disease duration of 6.4 years. 11
The main limitation of this study is its low patient quota. UC in India is still much rarer than in Europe and North America and there are no data on trends over time though there is a general belief that incidence is rising.
In conclusion, our study proves importantly that low-cost drugs (steroids, 5ASA and AZA) are effective in: (1) induction and long-term maintenance of remission with control of relapse; (2) prevention of disease extension; and (3) reducing complication provided drug compliance is good. Thus, the use of biologics, even as induction therapy in severe disease, must be re-evaluated. A better clinical outcome may possibly be due to the relatively benign nature of UC in India. 12 In a resource-constrained country where biologics are very expensive and their complications are extremely difficult and costly to treat, the long-term benefit of effective low-cost medicines should not be underestimated.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.