
Abstract
Severe ulcerative colitis can be associated with bowel perforation. Bowel perforation rarely leads on to abdominal wall and scrotal wall emphysema. Bowel perforation in such cases can be spontaneous or iatrogenic (colonoscopy-related). We report a rare scenario where a patient presented with abdominal wall and scrotal emphysema after topical corticosteroid enema-induced traumatic rectal perforation. Topical corticosteroids were stopped immediately after identification of rectal perforation. The patient was managed conservatively with intravenous antibiotics. With this report we intend to sensitise clinicians and topical enema manufacturers regarding this rare complication.
Case report
A 51-year-old man, recently diagnosed with severe ulcerative pancolitis on 5 amino salicylic acid (mesalamine 3 g daily), oral prednisolone (80 mg daily) and prednisolone retention enema (20 mg daily, prednisolone Sodium phosphate) presented to the Emergency Department with a sudden onset of swelling in the scrotal area of 2 days' duration without any pain at the local site or in the abdomen. There was no history of any endoscopic procedure except for diagnostic colonoscopy done 4 weeks previously. Colonoscopy had shown loss of vascular pattern, erythema and mild friability throughout in the mucosa of colon and rectum. There was no history of fever, trauma or prior scrotal disease. He denied having diabetes or using any other medications in the past. Local examination revealed the presence of crepitus in the scrotum, which was extending up to the lower anterior abdominal wall. Abdominal examination revealed a soft and non-tender abdomen. His investigations revealed haemoglobin of 12.4 g/dl, white blood cells 8,900/cumm, platelet count 194,000/cumm and ESR 13 mm. Serum albumin was 3.9 g/dl. An X-ray of the abdomen showed air in the lower abdominal wall and scrotum (Figure 1). An urgent computed tomography (CT) scan with oral, intravenous and rectal contrast revealed multiple air pockets in the perineum extending anteriorly to inguinal region, scrotum and upwards to the ischiorectal area and lateral sides of the lower abdominal wall (Figure 2). Contrast was seen extravasating posteriorly from the lower part of rectum. There was no peritoneal contamination as the perforation was below the level of the peritoneal reflection. The rectal enema was immediately stopped. The patient was managed conservatively with intravenous antibiotics (ceftriaxone and metronidazole) and his scrotal swelling subsided. He was discharged on day 3 and continued to receive oral antibiotics for 2 weeks; oral prednisolone was tapered and 5 amino salicylic acid was continued in view of active colonic disease. After 4 weeks, he again presented with complaints of similar swelling in the scrotal area of 1 day duration. Examination confirmed recurrence of crepitus. A barium enema was done and it showed the presence of leak from the previous site of perforation in the rectum (Figure 3). Oral prednisolone was stopped completely and he was continued on 5 amino salicylic acid. The perforation had probably recurred due to the tapering dose of oral steroids. One week later his scrotal swelling subsided completely without any surgical intervention. He had no recurrence of scrotal swelling or exacerbation of ulcerative colitis at 1-year follow-up.
Abdominal X-ray of index case. (A) Presence of air in abdominal wall (large arrow). (B) Air in the scrotal wall (small arrow). CT scan of pelvis of index case. (A) Presence of air and contrast leak in the rectal wall (large arrow). (B) Air in the scrotal wall (small arrow). (A) Barium enema picture showing recurrent leak from the rectal perforation site. (B) Prednisolone rectal enema.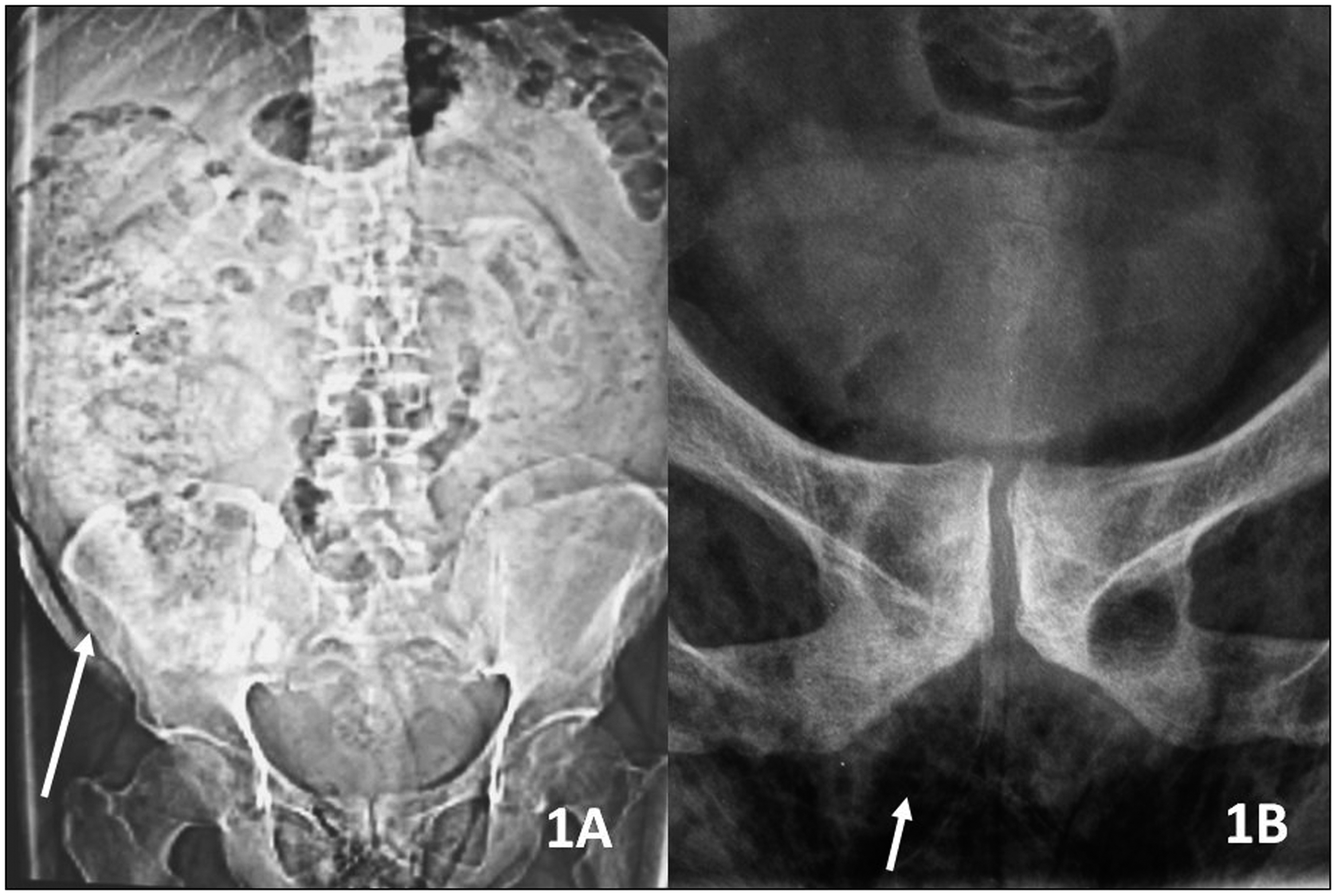


Discussion
Retention enema is an important mode of treatment for ulcerative colitis, 1 but enema-induced rectal perforation is rarely described.2,3 In the index case the patient was using a large nozzle applicator (∼9 cm long, provided with the topical steroid, Predsol Retention enema, UCB Pharma, Berkshire, UK) (Figure 3). Previous reports have discussed the complication of pneumoscrotum in the setting of iatrogenic perforation after colonoscopy or endoscopic sphincterotomy. 4 The mechanisms of development of pneumoscrotum include: the retroperitoneal air dissecting into the dartos lining of the scrotal wall; local gas production by micro-organisms resulting in scrotal gangrene; and movement of air from intraperitoneal space via patent process vaginalis. 5 The pneumoscrotum can mimic Fournier’s gangrene but generally the latter occurs in elderly patients with multiple other co-morbidities. Fournier’s gangrene presents with fever, intense genital tenderness, erythema, crepitus and gangrene. Most of these cases require urgent surgical debridement along with broad spectrum antibiotics. In comparison, patients with traumatic rectal perforation usually improve with conservative management as the retroperitoneal air gets absorbed quickly and a similar management strategy was adopted in this patient. The recurrence of scrotal emphysema was due to spontaneous perforation at the site of the previous rectal wound under the influence of use of oral steroids. Corticosteroids are known to hamper wound healing and increase short-term postoperative infections in acute colitis and in postoperative state in ulcerative colitis. 6 Occasionally surgical or laparoscopic closure with diverting colostomy may be required especially if the perforation is large or is associated with formation of pelvic abscess. 7
This case is a message, both for astute physicians and aggressive surgeons. Rectal enema should be considered as a rare cause of rectal perforation in patients receiving this modality of treatment and a conservative strategy is needed in such cases. The drug manufacturer should also remain alert about this complication and the correct method of drug application should be clearly described pictorially in the package insert.
Footnotes
Declaration of conflicting interests
None declared.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.